
Abstract
Introduction
Pitt-Hopkins syndrome (PTHS) is an autosomal dominant disorder caused by a mutation in the transcription factor 4 (TCF4) gene.1–3 Common characteristics of PTHS include dysmorphic facial features (e.g., gap between the two front teeth, broad nasal bridge, wide mouth, “cupid’s bow” upper lip), epilepsy, microcephaly, hypotonia, stereotypic movements, breathing difficulties (e.g., hyperventilation), and gastrointestinal issues. 4 The phenotypic presentation has also been characterized by severe intellectual disability, profound language impairment, severe motor impairments, and autism spectrum disorder (ASD). 4 The current clinical consensus criteria of PTHS is defined by cardinal features such as facial abnormalities, severe intellectual disability, and breathing regulation anomalies. 5
As suggested by the clinical criterion, TCF4 mutations alone do not determine whether someone has PTHS. In mice models, TCF4 abnormalities are associated with an array of neurodevelopmental disabilities, including PTHS, mild intellectual disability, developmental delay, ASD, and schizophrenia. 6 Across a case report on a familial variant on exon 18 of TCF4 and another family case report on disruptions and deletions to the proximal part of the TCF4 gene did not result in a PTHS diagnosis in part because individuals with the disruptions had mild intellectual disability and facial dysmorphologies not specific to PTHS.7,8 A group of non-related individuals with a recurrent TCF4 missense variant p (Arg389Cys) was found to have varying levels of intellectual disability and varied facial abnormalities that were non-specific to PTHS and did not result in a an PTHS diagnosis. 9
Although milder PTHS case presentations have been identified in the literature, these individuals have exhibited mild intellectual disability and been placed in self-contained special education classrooms as children.10,11 Since PTHS has fewer than 500 individuals diagnosed worldwide, 12 it is vital that the literature characterizes the full spectrum of clinical presentation.
Case history
The current case report describes a 14-year-old White male who participated in a larger survey study of individuals with PTHS in 2015 that was approved by the University of Alabama at Birmingham’s Institutional Review Board (IRB: X140626005) and conformed with The Code of Ethics of the World Medical Association. Demographic information was collected over multiple phone calls and a follow up standardized questionnaires for the original study. For the case report analysis, the family was contacted for consent and subsequently participated in a follow-up interview in June 2021. This information is consolidated and summarized below. With parental consent, the research team was able to obtain a brief genetic report from their medical records. The child was not available for a comprehensive physical examination, so all physical descriptions are from the child’s mother unless otherwise stated.
PTHS diagnosis
When the child was around 3 years of age, physicians ordered genetic testing to address concerns for possible genetic causes of hypotonia via a neuromuscular disorders panel. At that time, there were no significant genetic findings. At 6.5 years of age, the family enrolled the child in an ASD study in which participants received broad genetic testing, and the results were positive for PTHS. The participant was referred to a children’s hospital for further genetic testing and the child was formally diagnosed with PTHS at 8 years of age, shortly before his participation in the original PTHS study.
The child’s genetic profile was ascertained from a review of his medical records. In 2015, a chromosomal microarray identified a deletion at 18q21.2. Specifically, the deletion was found from 53,039,033 to 53,265,496, which resulted in a partial deletion in the first part of the TCF4 gene.
A physical examination in 2015 from the child’s home hospital revealed the following characterizations: a normally formed head, pupils are equal, round and reactive to light and accommodation, extra-ocular eye movements intact, mildly deep-set eyes, ears were normally placed and formed, normal teeth and lips, broad palate, large mouth, normally formed neck, no heart murmur, strong peripheral pulses, clear lungs, chest normally formed, no scoliosis appreciated, soft abdomen, no organomegaly, bilateral transverse palmar creases, normally formed hands and feet, 2 cm cafe-au-lait macules on left lower back, intermittently anxious, mildly uncoordinated run, slightly brisk reflexes bilaterally, no clonus at ankles, normal gait, can stand on one foot for about 5 s, no dysmetria with reaching.
As a result of the TCF4 deletion and a physical examination, the child was formally diagnosed with PTHS. According to the mother’s notes from a phone consultation following this genetic evaluation, the geneticist attributed the child’s mild PTHS presentation to his partial deletion and explained that he likely still “uses” parts of the TCF4 gene, and he can retain some of the gene function by making shorter versions of the transcription factor protein.
Early medical history
Related to his birth history, the child was conceived through in vitro fertilization and was born at 38 weeks gestation via Cesarean section. He weighed 3.289 kg and was 53.3 cm long at birth. He had reflux after his second feeding and was diagnosed with laryngomalacia, but this resolved spontaneously at 8 years of age. As of 2015, his medical history was significant for hypoglycemia, chronic constipation, and chronic ear infections. Medical history was insignificant for seizures, scoliosis, vision problems, hyperventilation, hypotonia, and dental problems. He carried diagnoses of ASD and attention-deficit/hyperactivity disorder (ADHD).
Updated medical history
By the time of the follow-up call in 2021, the child had also experienced anemia, exotropia, and cavities. In the interim his parents also recognized a gap between his two front teeth that is common in PTHS. A rectal prolapse surgery led to the discovery that he had excess sigmoid colon. He no longer experiences chronic ear infections. He has been subsequently diagnosed with generalized anxiety disorder (GAD) and postural orthostatic tachycardia syndrome (POTS). His mother reported he continues to exhibit hypoglycemia and chronic constipation and still carries diagnoses of ASD and ADHD. His medical history remains negative for seizures, scoliosis, hypotonia, and hyperventilation.
Currently, the child does not have daytime bladder or bowel accidents. During the 2015 interview, he had been wearing a pull-up at night to prevent bedtime wetting, but accidents stopped when they discontinued his Sertraline prescription shortly before the interview. He was described as urinating frequently, and the mother reported the family is unsure if this is related to his POTS symptoms or to escape anxiety-invoking situations. He does not have a history of pain when urinating or urinary tract infections.
Regarding medication history, he is currently prescribed a twice daily dose of Mirtazapine 22.5 mg for anxiety, a twice daily dose of Amitriptyline 75 mg for anxiety, Hydroxyzine 10 mg as needed for sleeping difficulties, and iron infusions for anemia (he cannot tolerate iron supplements). He also takes an assortment of supplements (e.g., probiotics, mitochondrial supplements, multivitamins, salt). His diet is gluten-free to reduce constipation. He was previously prescribed Sertraline 50 mg for anxiety, Clonidine 0.1 mg for sleeping difficulties, and Methylphenidate Hydrochloride Extended Release 36 mg for hyperactivity. After beginning Sertraline, he struggled with sleep (e.g., bedwetting, nighttime awakenings, early rising), so the prescription was discontinued.
Developmental profile
No history of language or motor regression was reported. The child is fully mobile but he has a history of motor coordination difficulties and is clumsy while running. Recently, his clumsiness has improved but he still struggles with bilateral motor movements (e.g., skipping, throwing a ball, bike riding). He has a large vocabulary and was reported to “speak like an adult”, such as when he reflected on graduating from the 8th grade “Mom I know it’s a big deal that I’m graduating from this school, but I’m sad to leave because it’s a safe space for me.” He has a history of correcting others’ grammar, but this behavior has reduced with age. His conversations were described as tangential or one-sided in the past, but his conversations have become more reciprocal over time.
The child’s mother completed a Vineland-II when he was 8 years old. He had an overall Adaptive Behavior Composite standard score of 79, which is in the below average range. He had domain standard scores of 86 for Communication and 83 for Daily Living Skills, falling in the low average range. His Social domain standard score was a 73, which is in the below average range. His Motor Skills domain standard score was a 100, which is in the average range. His mother estimated that his adaptive behaviors are relatively the same today. His mother believes his socialization abilities have slightly improved but that he is still delayed compared to his peers across most adaptive skills domains.
Education
The child is currently in 8th grade at a performing arts charter school. He is in a general education setting for most subjects and in a special education classroom for reading and mathematics. He shows a weakness in executive functions and receives educational supports, such as his homework being read aloud to him and fill in the blank notes). He also has access to verbal assessments if he is experiencing testing anxiety. He struggles with changes in routine at school. His mother reported that he has exhibited a few disruptive behavior incidents, such as swiping at an iPad and purposely dropping water bottles. At the time of 2015 interview, the child attended a general education classroom for all classes, and he had a behavioral aide from kindergarten to 3rd grade to support inattention. As he transitions to high school, the following accommodations will be provided: verbal assessments in place of written work when needed, extra time on assessments, decreased homework, sensory breaks from noisy classroom when needed, audio books to supplement or replace written text (an accommodation for exotropia), and specialized classroom settings for mathematics and literature (e.g., smaller class sizes, general education/special education teachers, slowed pace).
Strengths
The child’s mother described notable strengths in reading and musical abilities during the interview at 8 years of age that were revisited in the follow up interview. At age 8 years and in 3rd grade, he was described as having a strength in reading, with reading fluency at a 5th–6th grade level and his reading comprehension was at a 4th grade level. Today, his reading abilities are slightly delayed. As an 8th grader, his current reading fluency is at a 7th grade level and his reading comprehension remains between a 5th to 7th grade level. His mother believes that his autism-related cognitive style has negatively impacted his reading abilities as he has grown, such that he struggles with perspective taking and making social inferences between characters in stories. At age 8 years, he was reported to have perfect pitch for singing, could duplicate songs after hearing them one time, and played music on the piano by ear. Musical skills described in the recent interview include that he can read music, transpose music, and change keys. At his performing arts school, he plays piano, bass, cello, and harp and he sings. When asked about other areas of strength he was described as having a strong memory, such that he can cite a classical song that was played in a Baby Einstein video he watched as a toddler.
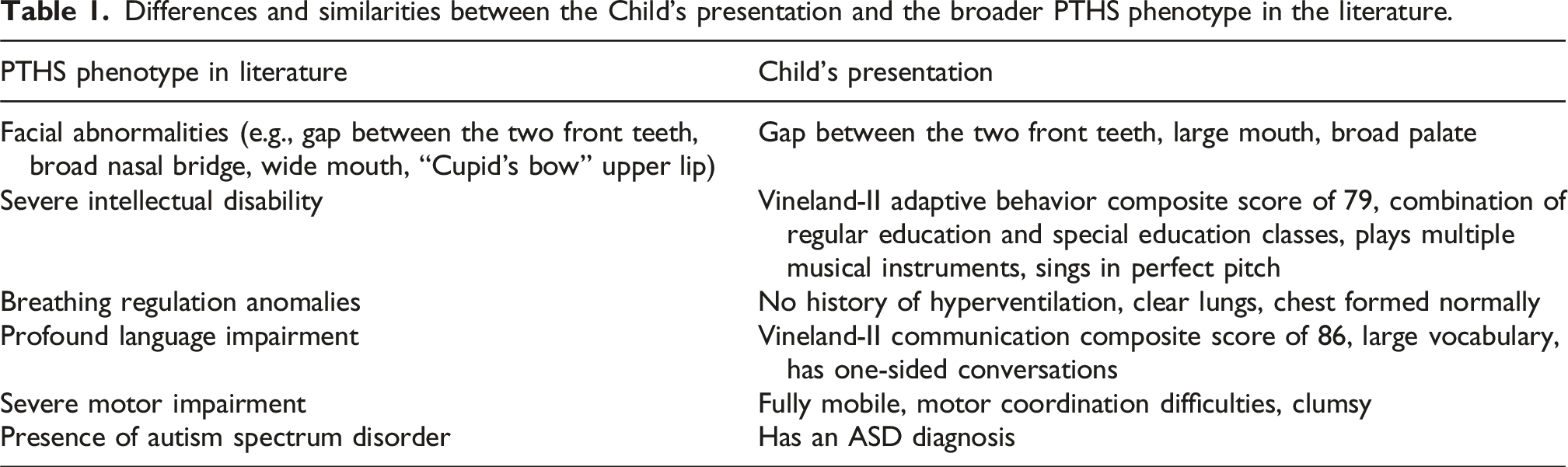
Differences and similarities between the Child's presentation and the broader PTHS phenotype in the literature.
Discussion
Given that PTHS is typically characterized by a severely impaired phenotypic presentation (e.g., severe intellectual disability, language impairments, and motor impairments) and medical complications (e.g., seizures & breathing difficulties), 4 deviations from those common characteristics provide additional understanding of the potential spectrum of this rare genetic disorder. Our study describes a child who can speak in full sentences, is mildly delayed academically, has mild motor coordination issues, and does not have seizures or breathing difficulties. He also has musical talents that have never been previously reported in PTHS. While this may or may not be related to the specific type of TCF4 mutation observed in this child, it highlights that PTHS as a diagnosis warrants consideration as a spectrum of possible presentations. This is an important point to consider when discussing prognosis and outcomes with families.
Over the course of 6 years, the child fell behind in some areas that were previously described as personal strengths (e.g., reading), and he developed additional medical complications that were not present at a younger age (i.e., anemia, rectal prolapse, convergence insufficiencies, GAD, POTS). Some of these medical complications are known to occur in PTHS, while some are not commonly observed. Given that cognitive, gastrointestinal, and vision issues are common in PTHS, 5 genetics-informed care likely bolstered this child’s medical experiences whereas if he was never diagnosed, many of these issues could have been left unexplored, unidentified, and untreated. This case further suggests that the developmental profile of PTHS could vary drastically across individuals with fluctuating impairments over the course of development. This case also suggests potential benefit of longitudinal approaches to learn more about PTHS development and progression.
Limitations
The current study did not have the child partake in additional genomic testing to provide further information about the participant’s genetic profile. However, the research team utilized a secondary genetic report from the child’s medical record. Neurocognitive assessment is currently limited to a parental report measure and the child should receive further testing to elucidate any additional deficits that are not recognizable by parental report and description. A comprehensive physical examination was not possible due to study constraints. Future research should include physical examinations on all rare genetic disorder cases, especially cases that appear to differ from well-established descriptions.
Conclusions
PTHS may have a wider functional spectrum of clinical presentations than previously understood. Such PTHS case presentations further emphasize that individuals with mild medical and neurocognitive impairments could benefit from comprehensive genetics-informed care.
Footnotes
Acknowledgements
Tremendous gratitude to the family discussed in this report for their willingness to discuss their child as a contribution to the PTHS literature. An additional thank you to Justin Schwartz for his medical expertise and review.
Author contributions
Mr. Arnold, Dr. Root, Dr. Leonczyk, and Dr. O’Kelley have made substantial contributions to study conceptualization and data acquisition. Drs. Guest and O’Kelley provided supervision for this student led research project. All authors have been involved in data interpretation, drafting, and revising the manuscript.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded in part by the Pitt Hopkins Research Foundation. This manuscript preparation was supported in part by a grant from the National Institute on Mental Health (T32MH018869, MPI: Danielson, Kilpatrick).
Data availability statement
Data is housed at The University of Alabama at Birmingham. Due to the sensitive nature of a case report, data can only be made available upon a release of information request.