
Abstract
Intimate partner abuse is a major public health driver of mental and physical morbidity in Palestine. This qualitative study examines how domestic violence becomes biologically embedded through chronic stress and cardiometabolic risk. We thematically analyzed 30 testimonies posted by Palestinian women in two large Facebook groups between January and March 2023, purposively sampling accounts that described health sequelae. Texts were coded in MAXQDA using Braun and Clarke’s framework, with deidentification, moderator permission, and institutional ethical approval (Braun and Clarke, 2006). Six interlinked themes traced a stress-to-illness cascade: persistent strain that pervades daily life; physiological pathways involving sleep disruption, palpitations, tremors, and elevated blood pressure; emotional trauma with somatic pain; intergenerational effects on children’s fear, school performance, and caregiving roles; scarcity of support and escalating harm; and breaking points that compel help seeking. The findings suggest that abuse in the West Bank functions as a chronic stress condition that reorganizes family life and accelerates cardiometabolic vulnerability. Integrated trauma-informed primary care, confidential referral pathways, childcare supports, and school-based buffers are required.
Introduction
Intimate partner violence (IPV) is a pervasive public-health problem with consistent links to women’s mental and physical morbidity across settings (Beydoun et al., 2012; Campbell, 2002; Coker et al., 2002; Pico-Alfonso et al., 2006; Roberts et al., 1998). The WHO Multi-Country Study documents substantial lifetime exposure to physical, sexual, and emotional abuse, together with injuries and reproductive harms, grounding IPV in gendered power relations that normalize control over women (Garcia-Moreno et al., 2005). Within Palestinian and neighboring Arab contexts, community and school-based research shows that marital coercion, humiliation, and threats co-occur with psychological distress and constrained help-seeking, while social surveillance and family pressure often silence disclosure (Haj-Yahia, 1999, 2001; Haj-Yahia and Clark, 2013; Oweis et al., 2009; Hamamra et al., 2025). Family-systems evidence demonstrates that children’s exposure to interparental violence is associated with internalizing and externalizing symptoms and school difficulties (Edleson, 1999; Evans et al., 2008; Graham-Bermann et al., 2006; Gewirtz et al., 2011; Herrenkohl et al., 2008; Holt et al., 2008; Salameh et al., 2025). Cross-cultural and longitudinal findings converge on continuity of risk: early maltreatment and family violence forecast later mental-health burden and relationship problems into adulthood (Evans et al., 2008; Roberts et al., 1998). In Palestinian settings specifically, witnessing or experiencing violence in the home predicts anxiety, depressive affect, and trauma-related symptoms among adolescents and young adults, reflecting local norms that can tacitly authorize male authority and limit women’s agency (Haj-Yahia, 1999, 2001; Haj-Yahia and Clark, 2013). These patterns do not end at the point of injury; they generate a sustained physiological load and anticipate chronic dysregulation—developed next under the lens of chronic stress (Campbell, 2002; Lightman, 2008; Veronese et al., 2026).
Chronic stress is the principal pathway that biologically and socially embeds IPV-related harm. Recurrent coercion, threats, and assaults sustain hyperarousal, anticipatory fear, insomnia, and cognitive strain between incidents, producing persistent dysregulation rather than transient reactions (Campbell, 2002; Coker et al., 2002). Longitudinal and meta-analytic research shows a bidirectional IPV–depression loop: violence increases depressive symptoms and suicide attempts, while depression elevates vulnerability to subsequent victimization, locking survivors into chronic stress states (Beydoun et al., 2012; Devries et al., 2013; Kim and Lee, 2013). Neuroendocrinology explains the biological embedding: prolonged activation of the Hypothalamic-Pituitary-Adrenal (HPA) axis and autonomic imbalance culminate in allostatic load—the cumulative “wear and tear” that heightens risk for mental and physical disease (Lightman, 2008). In Palestinian households, IPV-related strain is layered onto economic precarity, family obligations, and social surveillance, narrowing coping options and prolonging exposure (Haj-Yahia, 1999; Haj-Yahia and Clark, 2013; Oweis et al., 2009). Children living in these ecologies show parallel stress signatures—anxiety, aggression, and school adjustment problems—that heighten caregiving burdens and feed back into maternal strain (Edleson, 1999; Evans et al., 2008; Graham-Bermann et al., 2006; Gewirtz et al., 2011; Herrenkohl et al., 2008; Holt et al., 2008). Evidence from diverse contexts, including Korea and Bolivia, indicates that cultural differences do not negate shared stress pathways or their functional impacts (Kim and Lee, 2013; Meekers et al., 2013). In short, chronic stress under IPV represents a sustained condition with biological plausibility and cross-setting reproducibility, setting the stage for the cumulative emotional depletion described next as psychological exhaustion (Lightman, 2008; Campbell, 2002).
Psychological exhaustion names the cumulative depletion—hopelessness, demoralization, slowed cognitive processing, and loss of motivation—that undermines agency and help-seeking in abusive relationships. Empirical studies tie IPV to major depressive disorder, generalized anxiety, and suicidality, indicating sustained emotional drain rather than episodic distress (Beydoun et al., 2012; Coker et al., 2002; Pico-Alfonso et al., 2006). In Palestinian and neighboring Arab communities, humiliation, coercive control, and fear of reputational damage suppress disclosure, prolonging exposure, and compounding exhaustion (Haj-Yahia, 1999, 2001; Haj-Yahia and Clark, 2013; Oweis et al., 2009). Exhaustion is often misread when assessments prioritize event-based Post-Traumatic Stress Disorder (PTSD) checklists over prevalent common disorders and daily stressors (Campbell, 2002; Beydoun et al., 2012). Family research shows that caregiver depletion reshapes parent–child interactions—reduced warmth and more inconsistent or harsh discipline—thereby magnifying children’s emotional and behavioral problems and feeding back into maternal burden (Graham-Bermann et al., 2006; Gewirtz et al., 2011; Herrenkohl et al., 2008; Holt et al., 2008; Edleson, 1999; Evans et al., 2008). In Palestinian settings, where mobility, income, and privacy are constrained, these relational spirals can be especially entrenched (Haj-Yahia and Clark, 2013; Oweis et al., 2009). To avoid repeating earlier points about the IPV–depression loop, we note simply that the longitudinal evidence already summarized under chronic stress clarifies how exhaustion becomes self-perpetuating (Beydoun et al., 2012; Devries et al., 2013; Kim and Lee, 2013). The next section follows this depletion as it converts into bodily syndromes in healthcare.
Somatic illness is a frequent clinical face of IPV-related stress. Primary-care research documents clusters of persistent, “medically unexplained” symptoms—chronic pain, headaches, dizziness, fatigue, and gastrointestinal distress—that map closely onto psychosocial strain and rarely resolve without addressing underlying violence (Rosendal et al., 2017). IPV survivors report elevated neurological and gastrointestinal complaints and chronic pain syndromes, mirroring patterns across populations (Coker et al., 2002; Beydoun et al., 2012; Pico-Alfonso et al., 2006). Biologically, sustained autonomic arousal and dysregulated cortisol rhythms amplify pain sensitivity, disturb sleep, and disrupt gut–brain signaling, converting chronic stress into entrenched bodily illness (Lightman, 2008). In Palestinian and Arab contexts, stigma surrounding marital disclosure and fears of family censure often channel women toward somatic idioms—“nerves,” headaches, stomach problems—shaping help-seeking through general practice rather than protection services (Haj-Yahia, 1999; Oweis et al., 2009). Parallel processes are seen in children: exposure to interparental violence is associated with recurrent abdominal pain, headaches, and fatigue, plus school absence and functional impairment (Edleson, 1999; Evans et al., 2008; Graham-Bermann et al., 2006; Gewirtz et al., 2011; Holt et al., 2008). Evidence from Bolivia shows a similar coupling of IPV and mental-somatic clusters, underscoring generalizability beyond the Middle East (Meekers et al., 2013). Clinically, persistent somatic symptoms should trigger safe, trauma-informed inquiry about IPV and coordinated referral; this step also matters because the same stress biology that drives somatic syndromes contributes to longer-term cardiometabolic risk, discussed next (Rosendal et al., 2017).
A growing body of evidence implicates IPV in women’s cardiometabolic disease. In a population-based cohort, women with IPV histories had higher cardiovascular risk profiles, suggesting pathways to incident hypertension and ischemic disease (Stene et al., 2013). Mechanistic plausibility is strong: chronic sympathetic activation, HPA dysregulation, and inflammatory cascades promote endothelial injury, atherogenesis, and adverse lipid and glucose regulation (Lightman, 2008; Campbell, 2002). Behavioral sequelae compound risk—sleep disruption, reduced physical activity, and stress-related eating patterns contribute to weight gain and metabolic strain (Coker et al., 2002; Beydoun et al., 2012). Clinical work further associates IPV histories with obesity, and conceptual/metabolic scholarship describes reciprocal links between stress and adiposity, reinforcing cardiometabolic vulnerability (Alhalal, 2018; Foss and Dyrstad, 2011). Affective comorbidity may mediate part of this association, but even without full mediation, chronic stress alone plausibly accelerates cardiometabolic wear. In Palestinian households facing economic pressure and social surveillance, opportunities for recovery (sleep regularity, exercise, stress buffering) are constrained, potentially intensifying risk accumulation (Haj-Yahia and Clark, 2013; Oweis et al., 2009). Accordingly, primary-care and cardiology pathways should integrate IPV inquiry, brief stress-reduction supports, and cardiometabolic prevention (blood pressure, lipids, weight, glucose) for at-risk women, using trauma-informed safety protocols during screening (Stene et al., 2013; Campbell, 2002; Alhalal, 2018).
The same stress and exhaustion documented above reorganize family life across time, shaping children’s development and later relationship patterns. A systematic review of historical trauma distinguishes collective, historically rooted harms from family-level transmission, yet emphasizes clinically relevant continuities in emotional, behavioral, and health sequelae (Mutuyimana and Maercker, 2023). Family-violence scholarship identifies mechanisms: modeling of aggression and fear, disruptions to attachment and emotion regulation, and role inversions such as parentification (Edleson, 1999; Evans et al., 2008; Herrenkohl et al., 2008; Holt et al., 2008). Following IPV exposure, changes in parent–child interactions—less warmth, more inconsistency or harshness—predict school-age adjustment problems (Graham-Bermann et al., 2006; Gewirtz et al., 2011). Regionally relevant evidence shows that Arab adolescents who witness interparental violence report anxiety, depressive affect, and trauma-related symptoms, reflecting early internalization of coercive dynamics (Haj-Yahia, 2001). Over the life course, childhood maltreatment increases risks of later IPV victimization and perpetration, which then affects the next parenting generation (Evans et al., 2008). In Palestinian families, where social pressures can discourage disclosure and constrain exits, these mechanisms likely intensify. Interrupting transmission therefore requires combined strategies: protecting women from ongoing abuse, treating caregiver depression and anxiety, restoring supportive parenting, and strengthening school-based buffers—so that clinical gains are reinforced by stable, predictable relational environments (Haj-Yahia and Clark, 2013; Oweis et al., 2009; Mutuyimana and Maercker, 2023).
Because these harms persist within unsupportive ecologies, clinical fixes alone are insufficient. Multilevel analyses link community and societal gender inequality to women’s acceptance of wife-beating, signaling that norms can normalize harm and suppress help-seeking (Uthman et al., 2009). In Jordan and Palestinian settings, practical barriers—financial dependence, family pressure to endure, and fear of reputational damage—trap women in violent marriages and isolate them from services (Oweis et al., 2009; Haj-Yahia, 1999; Haj-Yahia and Clark, 2013). Health systems are critical entry points yet often miss IPV because survivors present with somatic complaints and clinicians lack established pathways for safe inquiry and referral (Rosendal et al., 2017; Campbell, 2002; Coker et al., 2002). Global syntheses therefore recommend survivor-centered, multilevel strategies that combine immediate safety planning and economic supports with coordinated services and stigma reduction (Garcia-Moreno et al., 2005; Meekers et al., 2013). For Palestinian families, this means integrating routine IPV screening into primary care, building confidential referral networks, providing childcare and transport supports that make attendance feasible, and partnering with schools to reinforce protective routines for children exposed to violence (Edleson, 1999; Evans et al., 2008; Holt et al., 2008; Gewirtz et al., 2011). Such reforms link back to earlier sections: reducing chronic stress, preventing psychological exhaustion, limiting somatic and cardiometabolic sequelae, and interrupting intergenerational transmission. Building on the theoretical framework outlined above, linking IPV to chronic stress, psychological exhaustion, somatic illness, cardiometabolic risk, intergenerational transmission, and structural neglect, this study is guided by the following research questions: First, how do Palestinian women narrate the experience of chronic stress and emotional exhaustion within abusive intimate relationships? Second, how do women describe the physiological and health-related consequences of sustained abuse, including somatic and cardiometabolic symptoms? Third, how is stress experienced and transmitted within family systems, particularly in relation to children’s well-being? Fourth, how do women describe the role of familial, social, and institutional responses in shaping the escalation or mitigation of harm, and what constitutes a breaking point requiring urgent intervention?
Methods
Study context
This qualitative study examines Palestinian women’s experiences of domestic abuse in the occupied West Bank, a space administered by the Palestinian Authority while remaining under Israeli military control since 1967, where everyday life is shaped by legal fragmentation, mobility restrictions, and social surveillance that together condition how harm is named, concealed, or disclosed. In this article, “Palestine” refers specifically to the West Bank and is intentionally distinguished from the Gaza Strip and from Palestinian citizens of Israel, since each context carries distinct juridical systems, infrastructures of care, and opportunities for help-seeking that bear directly on how women can report violence and access support. The testimonies analyzed were authored by women who identify residence in Hebron, Nablus, Jenin, Bethlehem, and Salfit, grounding interpretation in concrete places where domestic abuse is narrated as continuous strain that overwhelms coping resources and spills into bodily illness. This geographic focus does not deny related experiences elsewhere; rather, it enables analytic precision about how the West Bank’s sociopolitical conditions inflect the pathways from abuse to chronic stress, psychological exhaustion, and medical presentation. In keeping with the article’s health orientation, the design treats these testimonies not as isolated disclosures but as situated accounts that render private suffering legible as a claim to care and protection.
Forums and settings
Data derived from two moderated, women-only Facebook groups—Ask the Girls of Palestine (approximately 137,000 members) and Strong Independent Women (approximately 46,800 members)—that function as semi-anonymous spaces where Palestinian women solicit advice, exchange solidarity, and convert personal experiences into public text. Within these forums, women describe cycles of shouting, humiliation, and physical assault, and they give those experiences a health vocabulary that includes “nerves,” trembling, sleeplessness, collapse, and stroke, thus translating fear and hypervigilance into recognizable markers of illness. Membership is restricted and posts are moderated, which lowers the interpersonal cost of disclosure and creates a communicative environment where women can document harm that might otherwise be silenced by family pressure, reputational fears, or practical dependence. These groups therefore operate as discursive sites where domestic abuse is not only reported but interpreted, as speakers and respondents connect violent events to persistent stress, deteriorating mental health, somatic complaints, and the burdens borne by children who witness abuse. Treating the forums as research settings acknowledges that digital spaces are now critical venues of testimony and collective sense-making in Palestinian society, especially when offline routes to care are uncertain or obstructed.
Data collection and sampling
Data were collected between January 2, 2023, and March 18, 2023 using a bilingual Arabic–English search strategy designed to capture both abusive acts and their health consequences. Keywords included terms such as “violence,” “beating,” “insults,” “shouting,” “fear,” “trembling,” “collapse,” “stroke,” and phrases women commonly use to signal psychological exhaustion and bodily decline. All posts retrieved during the study period were screened in two stages using predefined inclusion and exclusion criteria. Posts were included when they offered first-person narratives that explicitly described domestic abuse and provided sufficient contextual detail to trace consequences for psychological well-being, daily functioning, somatic symptoms, cardiometabolic events, and the experiences of children who witness violence. Inclusion required that the abuse be described as occurring within an intimate partner or family relationship. Exclusion criteria removed third-party reports, general advice-seeking without personal testimony, duplicated posts, and posts too brief or vague to support analysis. The initial corpus contained 215 posts; after systematic screening for eligibility, all qualifying posts were compiled into a preliminary dataset. In a second stage, purposive maximum-variation sampling was employed to select testimonies reflecting diversity in types of abuse (verbal, physical, psychological), severity, reported health consequences, and references to children’s exposure. Posts were reviewed comparatively and coded iteratively, and selection continued until thematic saturation was achieved, defined as the point at which additional posts did not generate substantively new categories or pathways linking abuse to health outcomes. The final analytic sample consisted of 30 testimonies comprising 102 unique statements. This sampling strategy privileges depth, variability, and the capacity to map recurrent patterns that women themselves mark as consequential for mind, body, and family life.
Analysis
All texts were imported into MAXQDA 2022 and analyzed following Braun and Clarke’s six-phase thematic approach: familiarization with the data, generation of initial codes, searching for candidate themes, reviewing thematic coherence against the corpus, defining and naming themes, and producing the analytic account (Braun and Clarke, 2006). Coding proceeded inductively, with attention to both semantic content—how women describe shouting, beating, humiliation, fear, exhaustion, and bodily symptoms—and latent structures that link these descriptions to chronic stress, psychological depletion, and medicalized language. Theme development was iterative and comparative, moving between individual testimonies and the full dataset to refine boundaries among the six domains that organize the article’s Results: the burden of chronic stress, physiological pathways from stress to illness, emotional trauma and somatic manifestations, intergenerational stress and family health, the absence of support and escalation of stress, and breaking points that signal urgent need for intervention. Throughout, memo-writing documented analytic decisions and safeguarded the connection between women’s wording and the interpretive claims advanced in the report.
Positioning participants and citation scheme
The presentation of findings resists narrowing speakers to familial labels such as “wife” or “mother,” even when these appear in self-description, because such roles can obscure agency and collapse complex subjectivities into relational categories. Instead, participants are treated as narrating subjects who interpret their experiences and assign meaning to signs of distress, including the idioms by which psychological strain is rendered as bodily illness. To preserve confidentiality while maintaining geographic context, testimonies are cited with an alphanumeric code that pairs order and city (e.g., P1_Nablus, P2_Hebron). This citation scheme sustains the link between place and experience, which is central to understanding exposure, recognition, and the feasibility of care in the West Bank. The approach also supports transparency, allowing readers to track how particular quotations situate within the broader thematic architecture without risking identification.
Translation
All posts were authored in Arabic and translated into English by the researcher, who is fluent in both languages and attentive to sociocultural nuance. Translation sought to conserve the idiomatic force of the original, including expressions such as “my nerves are shattered,” “my heart will stop,” or “I collapsed,” which function as culturally meaningful articulations of distress that bridge emotional pain and physical vulnerability. Draft translations were repeatedly checked against the source to avoid inadvertent softening of urgency, erasure of religious or moral registers, or misreading of terms that carry diagnostic weight in everyday speech. This approach treats translation as an analytic step rather than a purely technical transfer, since the phrasing women choose is central to how abuse becomes legible as illness and as a demand for protection.
Researcher positionality
The primary researcher identifies as a Palestinian, fluent in both Arabic and English, with lived experience of the cultural, social, and political realities of the West Bank. This positionality shapes access to, interpretation of, and engagement with the online testimonies: shared language and cultural knowledge facilitate nuanced understanding of idioms, metaphors, and moral-religious registers in women’s narratives. At the same time, the researcher’s proximity to the sociopolitical context requires reflexivity to mitigate potential assumptions, biases, or over-identification with participants’ experiences. Analytical decisions, including the coding of psychosomatic expressions, assessment of stress pathways, and interpretation of intergenerational impacts, were regularly cross-checked through memo-writing and discussion with co-researchers to ensure credibility, transparency, and rigorous separation of interpretation from projection of personal perspective.
Ethics
Given the sensitivity of domestic abuse, stringent safeguards were applied at every stage. All potentially identifying details were removed, and permission to use anonymized posts was obtained from group moderators prior to analysis. No personal identifiers are reported, and testimonies are presented in ways that minimize risk of recognition while preserving the integrity of the narrative. The study adhered to the ethical principles articulated by the American Psychological Association (2010), including respect for persons, beneficence, and justice, and received prior approval from the Institutional Review Board of An-Najah National University (American Pyscholgical Association, 2010), and the Declaration of Helsinki (World Medical Association, 2013). Ethical reflexivity continued during analysis and writing, with special care to keep women’s voices central, avoid voyeuristic reproduction of harm, and frame findings within pathways that point toward care and intervention rather than sensational detail.
Results
The thematic analysis of women’s posts led to the identification of six themes: First theme: The burden of chronic stress in abusive relationships; Second theme: Physiological pathways from stress to illness; Third theme: Emotional trauma and somatic manifestations; Fourth theme: Intergenerational stress and family health; Fifth theme: The absence of support and the escalation of stress; Sixth theme: Breaking points and the urgency of intervention.
First theme: The burden of chronic stress in abusive relationships
Chronic stress represents one of the most destructive consequences of domestic abuse, particularly for Palestinian women whose lives are marked by both familial pressures and limited access to mental health resources. Their testimonies expose how cycles of shouting, humiliation, and physical abuse erode psychological well-being and generate cardiovascular risks. One Palestinian woman described, “He constantly insults me and curses me in front of my children; he also curses and abuses them verbally, and very often he beats them. His whole life is shouting. My psychological state has become very exhausted because of him, and this has also started to affect my children.” Her repetition of “constantly” and “very often” semantically emphasizes the endlessness of violence, while the phrase “my psychological state has become very exhausted” transforms emotional despair into a medicalized condition. Another echoed this deterioration, noting, “I am very tired psychologically, not just a little! In short, there is no hope that he will ever change. I know I should not stay with him, but I cannot find the courage.” The expressions “very tired psychologically” and “no hope” mark the semantic collapse of resilience, signaling how exhaustion becomes both psychological despair and existential illness. A third revealed the most dangerous effect of such constant strain, explaining, “I became so afraid of him, and his family said he was sick. But this life has made me ill too—I suffered a stroke.” The phrase “this life has made me ill too” semantically bridges family conflict with medical consequence, while “I suffered a stroke” provides embodied testimony that transforms abuse into a cardiovascular crisis.
The accounts of Palestinian women reveal how domestic abuse infiltrates the most intimate aspects of everyday life, forcing survivors to live in states of constant hypervigilance. Anticipating insults and violence, they describe their suffering in terms that fuse emotional and bodily collapse. One woman explained, “My husband does not fear God. I overheard him on a call speaking about me in degrading ways. The insults have increased recently, and he said if it were not for the children, he would have divorced me long ago.” The phrase “does not fear God” semantically situates her suffering in a moral-religious framework, while “if it were not for the children” reduces her worth to maternal utility. Another recounted the physical toll: “My whole body starts shaking, I cannot eat, I cannot drink, living with a man who sleeps all day and stays up all night, insulting and beating me, humiliating me in front of the children.” The phrase “my whole body starts shaking” semantically embodies terror, turning nervous collapse into a visible marker of psychosomatic illness. A third narrative illustrates the despair of entrapment: “I suffer greatly with my narcissistic husband; my life is completely stuck, nothing but depression upon depression. My children see everything, and I can no longer give them anything.” The doubling of “depression upon depression” semantically conveys suffocation, showing how despair multiplies without relief. These linguistic patterns highlight how Palestinian women translate trauma into medicalized metaphors, turning private pain into words that signify illness, collapse, and the erosion of both self and family health.
Second theme: Physiological pathways from stress to illness
Domestic abuse forces Palestinian women into cycles of chronic stress that deeply disrupt their physiological systems, especially cardiovascular health. Testimonies show how their nervous systems remain in constant fight-or-flight states, straining the body to collapse. One woman explained, “He humiliates me, insults me in front of the children, curses them, and his life is constant shouting. My nerves are shattered, my psychological state destroyed, and I no longer know peace.” The phrase “my nerves are shattered” semantically medicalizes her distress, transforming abuse into a clinical condition. Another testified, “My body trembles constantly, I cannot eat, I cannot drink, and I live in fear of him beating me or insulting me in front of my children.” The expression “trembles constantly” bridges fear and bodily dysfunction, signifying nervous system dysregulation. A third recounted, “I became sick from this life; I suffered a stroke. Even the holidays were filled with arguments and insults until my own children could not bear his behavior anymore.” The stark “I suffered a stroke” carries diagnostic weight, showing how Palestinian women’s words function as embodied evidence of violence.
Repeated cycles of abuse prevent Palestinian women from recovering emotionally or physically, each episode layering new stress onto bodies already weakened. One explained, “I live with a narcissistic husband; my life is depression upon depression. I am unable to provide for my children or even take care of myself.” The doubling of “depression upon depression” semantically conveys suffocation, an inescapable layering of despair. Another said, “He beats me and humiliates me, makes me feel worthless, and I tremble so badly that I can hardly stand. My whole body is covered in bruises from him.” The terms “worthless” and “tremble so badly” collapse identity and body, signaling abuse as both psychological degradation and somatic breakdown. A third recalled, “I am always scared, always anxious, always exhausted. He yells, curses, and blames me for everything. My nerves are destroyed, and my health is declining.” The repetition of “always” conveys permanence, while “my health is declining” linguistically documents illness. Collectively, these Palestinian testimonies show how words serve as diagnostic texts, encoding the translation of stress into bodily disease.
Third theme: Emotional trauma and somatic manifestations
The voices of Palestinian women demonstrate how emotional trauma from domestic abuse is inseparable from physical deterioration. One explained, “I live with someone who beats me, humiliates me, and curses me in front of my children. My body shakes, I cannot eat or drink, and my health is deteriorating.” The phrase “my body shakes” semantically enacts fear as somatic collapse. Another survivor shared, “I feel my life is nothing but depression upon depression, my nerves destroyed, my heart heavy, and my children witness everything.” The imagery of a “heart heavy” semantically fuses emotional grief with cardiovascular strain. A third said, “He shouted at me, cursed me, and insulted me until I collapsed. I became sick, I suffered a stroke, and now I live in constant fear that another attack will kill me.” Here, “collapsed” embodies both psychological and physical breakdown, while “I suffered a stroke” functions as medical testimony of trauma’s lethal potential.
Palestinian women’s words reveal bodies transformed into sites of illness, where humiliation becomes physical debilitation. One testified, “I swear by God my body trembles, I cannot eat or drink, and I live in terror of his voice, his insults, and his hands raised against me.” “Body trembles” semantically codes anxiety into physical disorder. Another explained, “My husband does not fear God, he humiliates me constantly, speaks about me in degrading ways to others, and I feel my heart will stop from the pressure.” The expression “my heart will stop” linguistically ties humiliation to mortality. A third confessed, “I no longer have the strength to continue; my life is unbearable, my health destroyed, my nerves shattered, and even my children are tired of him.” The words “no longer have the strength” frame collapse as both existential and medical. These linguistic choices highlight how Palestinian women turn suffering into medical metaphors that reveal the psychosomatic nature of abuse.
Fourth theme: Intergenerational stress and family health
Domestic abuse harms not only Palestinian women but also their children, embedding stress into family life. One mother explained, “He constantly humiliates me and curses me in front of my children. He also curses and abuses them verbally, and very often he beats them too. My psychological state is exhausted, and this has also started to affect the children.” The phrase “started to affect the children” semantically extends trauma across generations. Another recounted, “He humiliates me in front of the children, tells them their mother is worthless, and they start to believe him. He convinces them I am a failure, while my body shakes and my heart feels like it will stop.” “Worthless” semantically erases maternal identity, showing how violence undermines authority in the eyes of children. A third declared, “I can no longer take it; my nerves are destroyed, my health is collapsing, and even my children are sick of him. They live in fear every day.” The phrase “live in fear every day” linguistically encodes the normalization of terror for Palestinian children.
Abuse disrupts maternal roles in Palestinian families, leaving children vulnerable. One woman admitted, “I suffer with my narcissistic husband, my life is all depression, and I cannot give my children anything because I am exhausted and broken.” “Exhausted and broken” semantically fuses physical collapse with maternal failure. Another explained, “He beats me in front of the children, humiliates me in front of them, and tells them I am worthless. My body trembles, and I cannot protect them.” The phrase “I cannot protect them” signifies the semantic loss of maternal agency. A third testified, “I suffered a stroke from the stress, and even my children could not stand his behavior anymore. I fear for their future because they see everything.” The declaration “they see everything” linguistically underlines children’s helpless witnessing as trauma. Palestinian women’s words thus encode abuse as both a maternal crisis and an intergenerational health emergency.
Fifth theme: The absence of support and the escalation of stress
The abuse described by Palestinian women is compounded by social neglect and lack of intervention. One said, “I went many times to my family, but in vain. His family also did nothing. He threatens me if I go back to my parents. My body is covered with bruises, my health is destroyed, and I feel I am going mad.” The phrase “going mad” semantically expresses psychological collapse in medical terms. Another recalled, “I tried to tell my family, but they did not believe me. They all said I should be patient, but I was beaten in the hospital after giving birth, and I was beaten whenever I became sick.” The words “did not believe me” encode abandonment, while “beaten in the hospital” linguistically collapses spaces of care into sites of violence. A third stated, “I swear by God my nerves are destroyed. My life has become unbearable, my body shakes constantly, and I feel my heart will collapse. No one stands with me.” “No one stands with me” semantically reveals abandonment as a second violence against Palestinian women.
Medical neglect intensifies suffering when stress-related illnesses go untreated. One testified, “I got sick from this life; I had a stroke, and even now I live in constant fear. He and his family deny everything, leaving me to collapse alone.” “Collapse alone” semantically blends isolation with medical decline. Another said, “I am always scared, my heart is heavy, my nerves shattered, and my body exhausted. I can no longer provide for my children or even for myself.” “My heart is heavy” encodes despair as cardiovascular burden. A third explained, “I no longer have the strength; my health has deteriorated, my psychological state is destroyed, and even my children cannot bear him anymore.” The phrase “no longer have the strength” linguistically conveys total collapse. These accounts show how Palestinian women’s words record both violence and systemic neglect, transforming abandonment into embodied illness.
Sixth theme: Breaking points and the urgency of intervention
Palestinian women’s testimonies reveal breaking points where psychological despair and physical illness converge. One recalled, “My husband has hit me nearly to death five times, twice choking me until I thought I would die in his hands. I have three small children, and I feel my life is finished.” The words “nearly to death” and “my life is finished” semantically equate abuse with mortality. Another stated, “I am living with constant shouting, constant insults, and constant beatings. My nerves are destroyed, my health collapsing, and my children see everything.” The repetition of “constant” linguistically encodes abuse as unending. A third expressed despair: “I no longer have the strength to go on. My body trembles, I cannot eat, I cannot drink, and I pray that death will take me so I can rest.” The phrase “pray that death will take me” semantically marks trauma’s extremity, where survival is reimagined as rest in death.
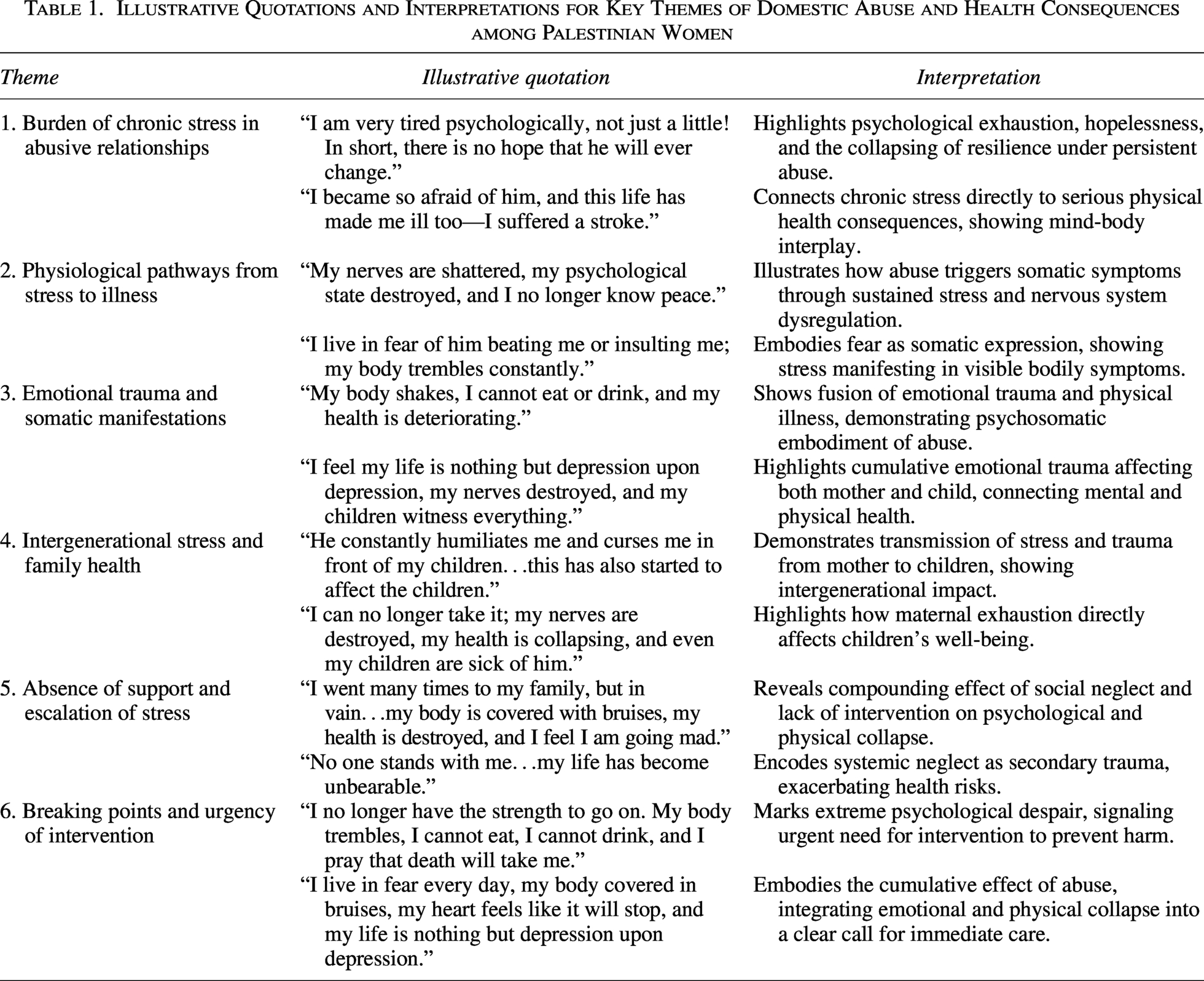
These breaking points highlight the urgency of intervention for Palestinian women, whose health and dignity collapse under sustained abuse. One explained, “I tried to be strong, but my health collapsed. I suffered a stroke, my nerves are finished, and even my children have turned away from me because of him.” “Tried to be strong” conveys resistance, while “health collapsed” semantically admits defeat under chronic stress. Another said, “I live in fear every day, my body covered in bruises, my heart feels like it will stop, and my life is nothing but depression upon depression.” The repetition “every day” linguistically signifies continuity, while “my heart feels like it will stop” embodies despair as cardiovascular risk. A third described, “I have endured all kinds of abuse, physical, and verbal, and now I feel I am losing my mind. My body is marked everywhere, and I no longer know how to survive.” The expression “losing my mind” semantically merges psychological collapse with physical scars. These Palestinian testimonies are diagnostic texts, where words encode trauma as illness, making urgent intervention a matter of survival. Table 1 presents illustrative quotations and brief interpretations for each of the six main themes identified in the thematic analysis. For reasons of clarity and space, only selected quotations are included; however, the full range of testimonies and their linguistic and psychosomatic patterns are described in the Results narrative above
Illustrative Quotations and Interpretations for Key Themes of Domestic Abuse and Health Consequences among Palestinian Women
Discussion
The findings both confirm and complicate what the introduction’s studies establish about intimate partner abuse as a stress-driven public health condition. Like Campbell’s synthesis, where repeated coercion sustains threat vigilance between incidents, participants described exhaustion, insomnia, and anticipatory fear that never fully subsided; yet they went further by showing how these states are managed inside crowded households and morally charged settings where endurance and family reputation shape choices (Bdier et al., 2025; Campbell, 2002; Haj-Yahia, 1999). Coker and colleagues reported persistent psychological burden even after episodes end; women here made that burden visible as a daily governance problem that reallocates time, attention, and care inside the home (Coker et al., 2002).
Somatic presentations in the testimonies resonate with clinical studies yet reveal practice gaps. Coker et al. found elevated pain, neurological, and gastrointestinal complaints among survivors, and Rosendal et al. showed that persistent medically unexplained symptoms often mask psychosocial strain (Coker et al., 2002; Rosendal et al., 2017). Women in this study sought help through idioms of nerves, headaches, stomach distress, and exhaustion, which the introduction’s regional literature explains as a rational response to stigma and reputational risk. In that light, symptom-only consultations without safe enquiry reproduce diagnostic drift and postpone protection.
The results also fit the bidirectional loop between distress and exposure that longitudinal work identifies. Devries et al. and Kim and Lee showed that depressive symptoms both follow and forecast later victimization, while Beydoun et al.’s review linked violence with major depression across methods (Devries et al., 2013; Kim and Lee, 2013; Beydoun et al., 2012). Accounts of hopelessness, cognitive fatigue, and social withdrawal in this study are therefore plausible mechanisms that reduce help seeking, shrink social ties, and increase dependence, raising the probability of continued abuse. The data extend this loop by showing how spiritual idioms of patience and family honor can deepen inertia even when danger is recognized.
Intergenerational consequences in the testimonies corroborate family systems evidence while shifting attention from extreme events to daily depletion. The introduction reviewed links between caregiver strain, reduced warmth, inconsistent discipline, and children’s internalizing and externalizing problems, school absence, and functional impairment (Graham-Bermann et al., 2006; Evans et al., 2008; Gewirtz et al., 2011; Holt et al., 2008). Mothers here described guilt, sudden anger, and withdrawal that reorganized routines and emotion regulation at home. This confirms those mechanisms but challenges policy assumptions that brief parenting courses suffice; where abuse is ongoing and space and income are limited, family repair requires safety plus reliable buffers for sleep, privacy, and schooling.
The social ecology sustaining harm mirrors the global and regional evidence summarized in the introduction. Garcia-Moreno et al. documented how gendered power and community norms suppress disclosure, and studies from Jordan and Palestine described financial dependence and reputational fears that discourage separation and mute clinical conversations (Garcia-Moreno et al., 2005; Oweis et al., 2009; Haj-Yahia, 1999). Participants’ emphasis on silence within extended families confirms these barriers while pointing to missed clinical opportunities. When primary care does not ask safely about violence, the health system converts private injury into untreated illness.
Cardiometabolic risk emerges as a near-term clinical concern rather than a distant horizon. Stene et al. associated partner violence histories with elevated cardiovascular risk, and Alhalal linked exposure with obesity through stress, sleep loss, and constrained activity (Stene et al., 2013; Alhalal, 2018). Reports of collapse, palpitations, and unremitting fatigue in this study should therefore trigger integrated screening of blood pressure, glucose, and lipids alongside safety planning. The testimonies add context that cohorts cannot capture: fear-controlled mobility and surveillance within the home curtail activity and restorative sleep, accelerating risk accumulation.
Taken together, and in the light of the studies in the introduction, these results advance the field in three ways. First, they recast efficiency in coping as a survival strategy within overburdened households, not a neutral health gain, showing how symptom management without safe enquiry entrenches harm. Second, they demonstrate that risks of dependency, dishonesty, and erosion of perseverance appear early in family life through daily depletion and constrained choices, not only in clinical endpoints or rare crises. Third, they show that families negotiate safety, care, and dignity through culturally charged moral frameworks, so effective responses must pair trauma-informed primary care and confidential referral with practical supports that restore sleep, privacy, schooling, and economic margin. The implication is a shift from abstract benefit versus risk debates to a situated analysis of how violence reconfigures authority, health, and care, and of how health systems can shorten exposure, widen recovery windows, and interrupt transmission across generations.
Limitations of study
This study has several limitations. First, the testimonies come from self-selected posts in two Facebook groups, which restricts representativeness and may favor women who are more digitally connected, more willing to disclose, or seeking advice. Second, reliance on self-report introduces recall bias and strategic framing, and we could not independently verify events or health diagnoses. Third, the analysis is cross-sectional and cannot establish causal pathways from abuse to physiological outcomes; references to blood pressure, tremors, or palpitations are interpretive links rather than clinically measured endpoints. Fourth, platform norms, moderator rules, and fear of retaliation may have shaped what women shared, producing underreporting of severe violence and of sensitive topics such as sexual coercion. Fifth, the focus on the West Bank limits transferability to Gaza, Palestinian communities inside Israel, or the diaspora, where exposure, services, and stressors differ. Sixth, ethical constraints precluded follow-up, clinical screening, or inclusion of partners’ perspectives. Seventh, the sample underrepresents rural, camp, and very low-income women who lack internet access. Finally, the positionality of the researcher may have influenced analysis and interpretation. As a fluent Arabic-English speaker familiar with Palestinian sociocultural norms, the researcher’s background facilitated nuanced understanding of idiomatic expressions and psychosomatic references; however, prior experiences, perspectives, and assumptions may have shaped coding decisions and thematic emphasis. Reflexive memo-writing, iterative coding, and peer debriefing were employed to mitigate bias, but this influence remains a limitation. These constraints should be addressed in future research through mixed methods, clinic-linked recruitment, longitudinal designs, and team-based coding approaches.
Conclusions
Domestic abuse in the West Bank should be treated as a chronic stress pathology that produces cumulative biological wear and tear rather than as a private dispute or solely a psychosocial concern. The testimonies show patterned links between coercion, humiliation, sleep loss, and cardiometabolic warning signs such as palpitations and elevated blood pressure. This pattern demands a health system response that is proactive and measurable. Primary care clinics should institutionalize routine inquiry that is trauma-informed, supported by confidential referral pathways and rapid access to safe accommodation. Screening must not stop at questionnaires. It should include basic cardiometabolic checks, brief interventions for sleep and anxiety, and monitored follow-up. Ministries, NGOs, and professional associations should issue unified clinical guidance and audit compliance. Anything less allows preventable illness to take root under the cover of silence and stigma.
Yet a clini- only solution is insufficient because the drivers of chronic stress are structural. Legal gaps around protection orders, weak enforcement, economic dependence, and the constraints of occupation entrench women in violent homes. Policy must therefore combine legal reform, universal access to shelters, cash assistance, and workplace protections with school-based programs that teach nonviolent conflict resolution and emotional regulation. Digital testimonies reveal an invisible care economy where neighbors and relatives absorb unpaid labor. These informal networks deserve support through food vouchers, transport stipends, and safe communication channels. Research should move beyond cross-sectional description toward longitudinal and clinic-linked designs that measure biomarkers alongside narratives. Treating domestic abuse as a public health and public policy emergency is the only credible path to reduce preventable disease and restore dignity.
Availability of Data and Materials
The datasets generated and/or analyzed during the current study are available from the corresponding author upon request.
Authors’ Contributions
All authors contributed equally to this work.
Footnotes
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
No funding was received for this study.