
Abstract
Graduate public health education is evolving rapidly as a function of complex and interrelated factors including rising student debt, a changing economy and job market, varied perceptions of the value of higher education, and new educational technologies affecting how courses and programs are delivered. At the same time, employers are seeking more highly trained public health professionals across a broader range of industries including, but not limited to, government, health care, pharmaceutical, consulting, and education. We redesigned the Boston University Master of Public Health (BU MPH) curriculum to provide students with integrated foundational knowledge; specialized skills and training in key areas sought after by employers across industries and functions; and activities to build student’s professional capabilities and confidence. The BU MPH, detailed in this article, provides an illustration of an MPH that is interdisciplinary, flexible, and adaptable to meet the changing needs of the workforce.
Several evolving issues are shaping graduate education worldwide during the first quarter of this century. A burgeoning literature on the science of pedagogy has been nudging graduate educational practices from teaching to learning, from content coverage to competency mastery, from faculty-centered to student-centered practices (Frenk, Hunter, & Lapp, 2015; Valladares & Ávila, 2015). In addition, increasing accountability from within and outside colleges and universities, shifts in student demographics, and growing student debt contribute to a rapidly changing landscape of graduate public health education. An explosion of undergraduate public health offerings has coupled, incongruously, with increasing demands on the parts of employers for more highly skilled and specialized graduates. These evolving issues suggest that it may be an appropriate time to ask: How do we most effectively train the next generation of public health practitioners?
Academic public health in the United States has engaged this question on several levels. In October 2012, the Association of Schools and Programs of Public Health (ASPPH) formed the Framing the Future Task Force to “re-vision the role of education for public health 100 years after the Welch-Rose Report” (ASPPH, n.d.-a). This latter report outlined recommendations for the establishment of professional schools of public health in the United States. The Framing the Future Task Force was convened to address a number of challenges, including the following:
A growing interest in undergraduate courses, programs, and degrees
An increase in Doctor of Public Health (DrPH) programs (which vary widely in terms of their focus and goals) calling for more explicit articulation with the Master of Public Health (MPH) training
Competency-based educational models that are not new but have not been consistently applied or evaluated in public health
An increase in the number of accredited schools and programs in public health with new and different concentrations and subspecializations to address changes in the field and in the demands of the workforce
An expansion of the sectors in which public health professionals work, given that the majority of public health professionals now work outside of local public health (Explorehealthcareers.org, n.d.; Kennedy, 2009)
To inform the Framing the Future Task Force, ASPPH conducted a survey of employers from the public, private, and nonprofit sectors to collect data on emerging trends, critical components, and capabilities that should be considered in 21st-century public health curricula (ASPPH, 2013). The report included recommendations for essential elements of public health educational programs. It emerged clearly that employers are increasingly looking for graduates with an understanding of how the health system works and skills in problem solving, leadership, management and teamwork, global health, policy, analytic methods, technology and information, budgeting and finance, and communications. However, these recommendations were not listed by priority and are essentially a wish-list not constrained by credits or program hours, raising the question about how we may best structure graduate public health training to reflect these preferred attributes.
The Framing the Future Task Force convened several expert panels to develop frameworks for undergraduate public health education, public health education at community colleges, the MPH, and the DrPH. The MPH Expert Panel Report outlined several design features for the MPH of the 21st century (ASPPH, 2014). Specifically, the MPH degree should be based on a rigorous, structured, and carefully sequenced curriculum that may require prerequisites. A common element of all MPH degrees should be a well-designed core that covers critical and interdisciplinary content in foundational areas of public health. Each MPH degree should offer in-depth education in concentration or specialty areas that are responsive to the interests of students, the strengths of the college or university, and the needs of employers. The practicum and culminating experience in the MPH degree should be considered primarily as elements of the concentration rather than as elements of the core. The MPH degree should have distinct and defined learning objectives for each of its major elements, including core, concentration, practicum, and culminating experience.
Building on this work and other educational reports, several schools of public health have innovated specific aspects of their curriculum (ASPPH, 2016). In the fall of 2012, the Mailman School of Public Health at Columbia University launched a new MPH curriculum replacing their traditional core courses with a new comprehensive core composed of 18 distinct modules organized into five studios of foundational knowledge, adding new course requirements that offered students the opportunities to learn leadership skills and to delve into case studies, expanding the practicum experience to be more interdisciplinary rather than discipline-based, and offering the option for students to earn certificates beyond their selected discipline (Begg, Galea, Bayer, Walker, & Fried, 2014). The Tulane School of Public Health examined its MPH curriculum and integrated independent core offerings through case studies and cross-cutting examples and offered options to students for a second area of specialization, beyond their selected concentration, through graduate certificates (White, 2015). The University at Albany, State University of New York, integrated their independent core courses around a common cross-cutting issue, diabetes (Dewar, Bloom, Choi, Gensburg, & Hosler, 2015). Many other schools have launched integrated cores that range from a combined epidemiology and biostatistics course to one fully integrated core curriculum (ASPPH, n.d.-b; UNC Gillings School of Global Public Health, n.d.).
We were interested in developing a new model for graduate public health education that both reflected the national reports and built on prior innovation by other schools of public health. In particular, we were interested in taking a big picture look at the foundations of graduate public health education and attempting to design an entirely new curriculum that would enable higher levels of learning, be fully integrated across disciplines, align with the needs of the workforce, and provide enhanced opportunities for a diverse body of students to develop practical and professional skills and confidence. We describe here our vision of an innovative, adaptable, competitive, and effective MPH program within the evolving environment of public health and how we put this vision into practice through a redesigned MPH.
The Boston University (BU) MPH
Formative Work
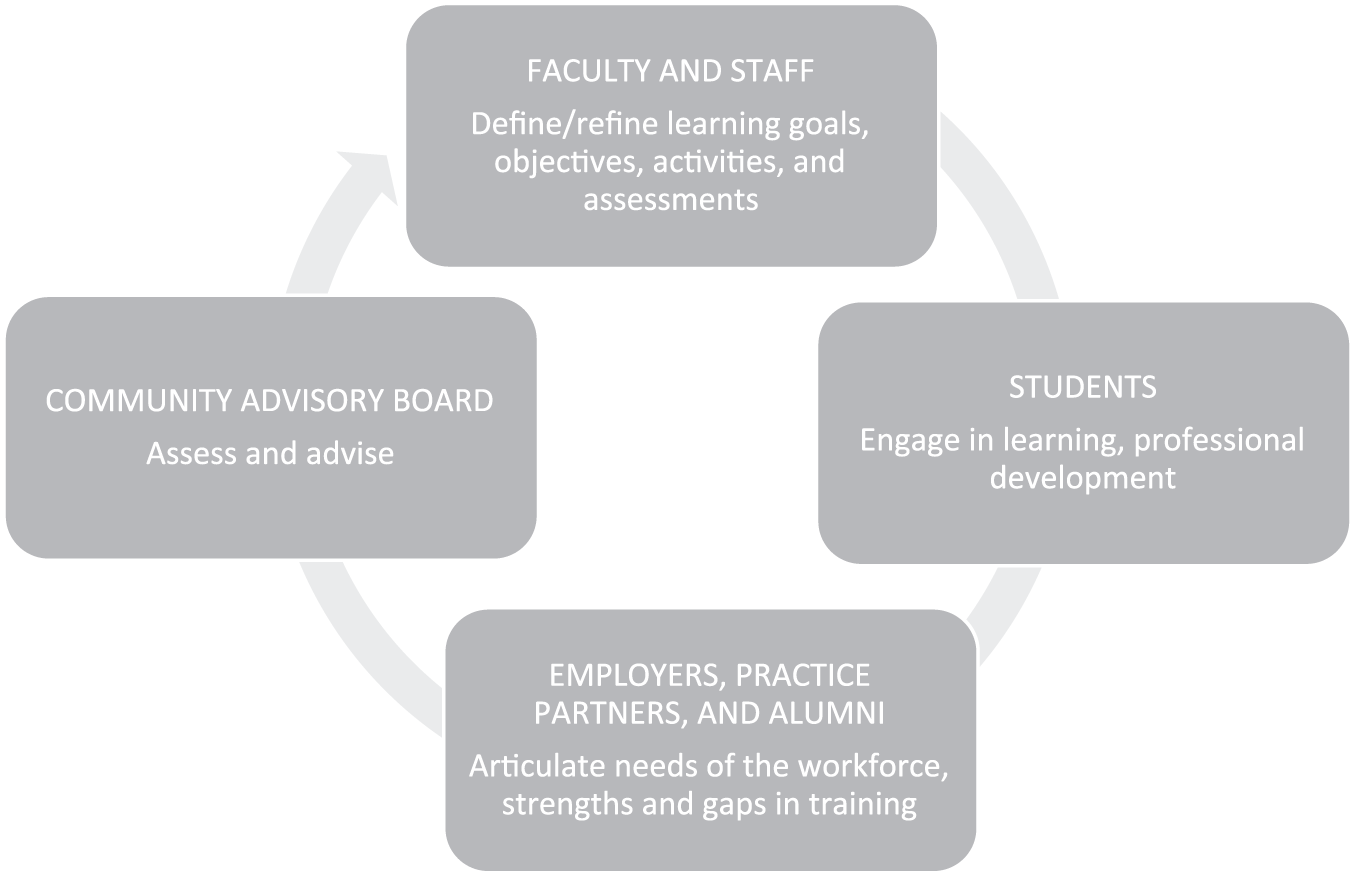
Bringing this new vision to life was years in the making. We collected data using comprehensive surveys and in-person interviews from key stakeholders including students (n = 320), alumni (n = 425), employers and practicum supervisors (n = 88; see Figure 1). We organized a task force of 10 faculty and 4 staff who represented each department and major administrative function of the school who met biweekly for 2 years. Two retreats of school leadership were convened to review data and to develop parameters for the redesign. Five working groups, composed of 36 faculty and 14 staff, were organized to tackle specific areas—the core curriculum, concentrations, the practicum, culminating experience, and effective teaching and assessment. We held four open town hall meetings for the entire school community to discuss progress and to solicit additional input and ideas. All faculty and staff were contacted and invited to submit proposals on any aspect of the redesign. Regular updates were provided to the school community at student meetings with the dean (three per semester over 2 years), curriculum coordinator meetings (10 presentations given to educational staff), monthly departmental faculty meetings, monthly faculty senate meetings, and at school-wide assemblies (four presentations given). All of the task force documents including proposals and meeting minutes were also posted on a password-protected website so that all members of the school community could access the latest developments. After extensive consultation with faculty, staff, students, alumni, and community partners, the task force articulated an MPH that was endorsed by the Governing Council, the senior governance body for the school.
The BU MPH.
The resulting BU MPH (Figure 2) has three components: (a) an integrated core curriculum, (b) specialization in the form of interdisciplinary certificates, and (c) a professional development and practical experience component that includes the practicum, integrated learning experience, and a newly designed Career PREP (Prepare|Reach|Emerge|Propel) program. We describe each below, focusing on key elements and resources to maximize success.

Meeting the needs of the workforce.
Foundation: The Integrated Core Curriculum
Key Elements
The integrated core curriculum includes four interdisciplinary courses. The rationale and goals of each are outlined below.
Health Systems, Law, and Policy: Laws and policies have a major impact on the shape, operation, and outcomes of health and health care systems. This course provides students with the information and tools they need to analyze how public health and medical care systems are organized, regulated, and financed and how well or poorly they meet policy goals of equitable access, high quality, and reasonable cost. Cases are drawn from the United States and other countries.
Individual, Community, and Population Health: Understanding health and the determinants of health at multiple levels is critical to improve the health of individuals, communities, and populations. This course provides students with an understanding of complex health problems and the tools to develop strategies for improving health at the individual, community, social, environmental, and structural levels.
Leadership and Management for Public Health: Public health professionals rarely work alone to make things happen. This course provides students with skills to effectively and ethically communicate with, engage, and organize others in the pursuit of specific projects and change efforts, and to understand the complex organizational contexts in which change is sought.
Quantitative Methods in Public Health: The ability to evaluate information and make evidence-based decisions is essential for today’s public health professionals, regardless of their specialty area or career path. This course provides students with the fundamental concepts and skills to organize, analyze, and present data for decision making, and to critically evaluate the validity of conclusions presented by others.
Resources to Maximize Success
Because we do not require prerequisite coursework in public health, students come to the school from diverse academic backgrounds. To fill gaps, we developed a library of online resources to ensure that all students are prepared to handle the integrated core. These have proven extremely valuable for faculty and students alike and allow for the new integrated cores to move all students further along. For example, faculty can refer students with limited statistical experience to online modules which provide more background.
We also recognized that students needed more formal training in writing for the profession. We devised a public health writing program that includes faculty and staff who provide instruction in writing as part of the integrated core. The faculty writing director met with faculty teaching each of the integrated cores to review writing assignments, expectations, and grading rubrics. She then developed writing instruction sessions, open to all students in the integrated core, which were delivered as students were working on specific assignments. Staff assisted in the writing sessions and also coordinated a peer coaching program that offers one-on-one or group-based appointments with peer writing coaches trained to answer questions, provide feedback, and assist students in all aspects of the writing process. We developed a detailed public health writing guide and extensive online resources to support effective writing. These include general writing strategies, techniques for providing and utilizing feedback, techniques specific to different types of public health writing, and finding and using references.
Specialization: Interdisciplinary Certificates
Key Elements
In designing the specialization component of the BU MPH, we replaced departmentally based concentrations with interdisciplinary certificates. Certificates are composed of a cluster of sequenced courses (two levels beyond the core) that build competencies in a defined area. Certificates are embedded within the BU MPH and not considered as add-ons to a concentration or specialty, as is the case in some other programs. We organized certificates into two distinct categories: functional certificates, which represent specific skills bases, and context certificates, which represent key populations or areas of focus. Students are required to choose one functional certificate and have the option to choose a context certificate, a second functional certificate, or to choose electives that best prepare them for their professional goals. Functional certificates include 16 credits of coursework, context certificates include 12 credits of coursework, and students are allowed to double count up to 4 credits in two certificates. To develop knowledge, skills, and attributes in certificate-specific competencies, students engage in a focused, sequential set of courses that build on the integrated core designed to provide the skills, training, tools, and techniques needed to become a successful professional in that specialty area. Course requirements for each certificate were purposefully designed to develop higher levels of learning in students from application to creation. Application involves students analyzing and applying knowledge, skills, and techniques to practical situations, as assessed through assignments that require them to apply concepts to broad questions about unstructured problems such as cases or data sets. Creation involves students extending and applying their knowledge and skills in a professional setting, as assessed through assignments in which they work on a public health problem by evaluating relevant content and delivering a professional work product or solution. The certificate offerings available in the BU MPH along with the competencies for each are outlined in Table 1.
Certificate Options and Competencies in the Boston University MPH.

Note. MPH = Master of Public Health; CDC = Centers for Disease Prevention and Control; MCH = maternal and child health.
Resources to Maximize Success
Our interdisciplinary certificates were designed to be adaptable to evolving changes in the workforce and thus, they were intentionally not aligned with departments. That shift required some additional investments to ensure that both faculty and students felt supported. First faculty leads were identified for each certificate to provide protected time to engage in certificate oversight and administration. We also enhanced our advising and support to students through the creation of the BU Advising Network. All students have open-door access to professional staff advisors and are assigned faculty advisors in their certificate area(s). Career services professionals are available for consultations to any student or alumnus and all incoming students are invited to join our newly developed student–alumni mentoring program (STAMP; Figure 3). To further assist students in choosing the certificate(s) that best prepare them for their professional goals, we created an interactive web-based tool where students choose functional and context certificate options and based on their specific choices they see potential career pathways. Professional staff from our Career Services Office mapped out career pathways for each certificate combination including examples of organizations, roles, and job titles that might be accessible on completion of each certificate or combination of certificates. A sample of options is shown in Table 2.
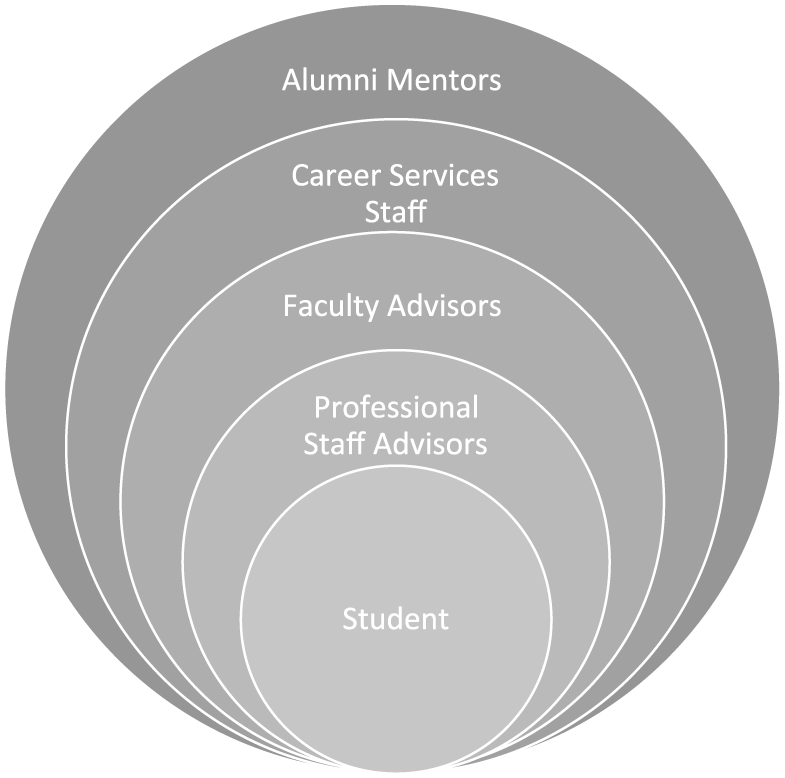
The BU advising network.
Certificate Matching and Career Pathways Examples.

Note. NGO = nongovernmental organization; CDC = Centers for Disease Control and Prevention; PAHO = Pan American Health Organization; WHO = World Health Organization; USAID = United States Agency for International Development.
Professional Development and Practical Experience
Key Elements
The third component of the BU MPH is professional development and practical experience. It includes an expanded field-based applied practicum experience where students have the opportunity to put what they are learning in the classroom into action in a real-world setting, the Integrated Learning Experience (ILE) where students synthesize all aspects of their program into a work product that effectively demonstrates their mastery of foundational and certificate-specific competencies, and the Career PREP program where students learn tools and techniques to conduct a job search, effectively market themselves, network, interview, and negotiate offers.
Practicum
While the school always had a practicum requirement, many of our incoming MPH students have minimal public health employment experience and need more time to develop their professional skills and confidence. Thus, we expanded the number of hours required from 112 to 240 and updated the expectations for students in the work products that demonstrate their competencies. We also invested in a new online system to allow students, field site supervisors, and faculty advisors to track progress on competencies, to conduct real-time assessments, and to ensure early identification of issues should they arise. The evaluation data collected in the system allows for outcome assessment and ongoing monitoring to ensure that the curriculum is meeting the needs of students and employers.
Integrated Learning Experience
In the ILE, students develop work products that demonstrate their capabilities and can be used in job or graduate school interviews. Work products take the form of a program plan, program evaluation, research proposal, grant application, critical review, policy paper, or research report, as appropriate. The product demonstrates the student’s ability to apply knowledge and skills from all aspects of their program. At a minimum, each student demonstrates their abilities to define a public health issue and its significance, they then acquire and use appropriate sources of information and data to critically analyze that issue. All students follow a specific process to complete their ILE including submission of a work plan and product proposal that is reviewed and approved by a faculty advisor prior to the initiation of the work. The ILE may be completed individually or by a team. However, each individual’s contribution to the work product must be clearly delineated and each student is evaluated on their specific contribution against relevant outcomes. The ILE reflects the student’s ability to make choices that consider ethics and take into account the values, practices, and priorities of relevant communities, cultural groups, and organizations. Last, as part of the experience, students demonstrate self-reflection on their own professional development and learning. Faculty review and assess the ILE based on rubrics with specific criteria to assess each student’s ability to integrate, synthesize, and apply the knowledge and skills that are relevant to their professional goals.
Career PREP
The required Career PREP program is designed to ensure that all graduates have the necessary competencies, techniques, and professional confidence to effectively market themselves during the job search process and into their public health careers. The program is developed and implemented by professional staff in the Career Services Office who integrate employers, alumni, and outside experts as needed. The program includes completion of several modules, including self-assessment to determine values, interests, and motivators; marketing strategies developed through researching sectors, industries, and employers; networking strategies and techniques, including development of a professional profile for LinkedIn; interviewing and negotiating strategies; and tools and techniques for managing a public health career, emphasizing skills not just for a first job but skills applicable throughout a career. Because we have a heterogeneous student body, we offer options to meet the needs of students with varying levels of professional public health experience.
Summary and Implications
Schools of public health need to continually review student learning and curricula to ensure that they are training graduates with the knowledge, skills, and attributes that will be required to positively impact the communities that they serve and to meet the needs of a changing workforce. This is not only a core responsibility of schools and programs of public health but required for accreditation by the Council on Education for Public Health. Fundamentally the field needs public health curricula that are adaptable and flexible but that stay true to the core of public health. Curriculum change is difficult and must be viewed as an ongoing process of continuous quality improvement rather than a onetime disruptive event. Here we outline an approach, provide some strategies, and highlight lessons learned that we hope will be useful to other schools as they update their programs in these rapidly changing times.
Footnotes
Acknowledgements
George Annas, Ann Aschengrau, Jennifer Beard, Candice Belanoff, Dan Brooks, Harold Cox, Eugene DeClercq, William DeJong, Carol Dolan, Rani Elwy, Rich Feeley, Leonard Glantz, Jacey Greece, Erin Hasselberg, Megan Healey, Tim Heeren, Wendy Heiger-Bernays, Wayne LaMorte, Mike LaValley, Jessica Leibler, Jonathan Levy, Lois McCloskey, Lisa Messersmith, Lisa Metropolis-Toby, Patricia O’Brien, Christine Paal, Victoria Parker, Mark Prashkler, Winnie Roche, Peter Rockers, Cassie Ryan, Alan Sager, Kim Shea, Michael Siegel, Jean van Seventer, and James Wolff.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.