
Abstract
Responding to the 2016 Council on Education for Public Health foundational competency requirement that students demonstrate the ability to “perform effectively in interprofessional teams,” the distance-based executive master’s program at Emory University developed an innovative interprofessional education (IPE) experience for geographically dispersed mid-career professionals. Because executive students are mid-career professionals from a variety of disciplines, they participated in this experience representing their professional roles and titles. IPE student groups represented at least three distinct disciplines. The executive program created a four-part online experience consisting of (1) a self-paced didactic module, (2) a synchronous case study group discussion, (3) small (three to five students) group development of a video solution to the case study, and (4) peer review of other groups’ case study solutions. The first-year pilot program was evaluated via standard online course evaluations and a separate evaluation survey sent immediately after completion of the complete experience. Of those responding to the standard course evaluation, 61.1% reported that they learned a great deal in the course and, of those responding to the immediate evaluation survey, 87.5% reported being very satisfied or satisfied with the experience. During the second iteration of the program, an additional survey, the Nebraska Inter-Professional Education Attitudes Survey identified improvement on 9 out of 19 attitudes toward interprofessional education. Overall, this IPE experience offered a unique way to employ the strengths of executive students and provide a meaningful IPE encounter for students in geographically diverse locations.
Interprofessional education (IPE) helps improve health outcomes by preparing health professional students to work collaboratively in team-based care (Gilbert et al., 2010). Since the 2009 founding of the Interprofessional Education Collaborative (IPEC) by six national health professional school associations, there has been significant growth and acceptance of the need for health professional students, including those in public health, to participate in interprofessional education and training (IPEC, 2016). There are now 21 national associations of health professions in IPEC, more than 550 citations of the IPEC Core Competency report (Barzansky & Etzel, 2015) and numerous effective implementations of interprofessional education (IPE) experiences. Many health professional accrediting organizations now require or recommend that IPE competencies be included in the curriculum (Health Professions Accreditors Collaborative, 2019; Zorek & Raehl, 2013). In 2016, the Council on Education for Public Health (CEPH), which is the accrediting body for schools and programs of public health, released a new set of foundational competencies for all students at accredited schools and programs of public health. Among these competencies is one on interprofessional practice, where students must demonstrate that they can “perform effectively in interprofessional teams” (CEPH, 2016).
The need for students to demonstrate interprofessional skills (Gilbert et al., 2010; IPEC, 2016) and the associated accreditation requirements have prompted schools and programs of public health to implement IPE curricula. However, there is not a “one-size-fits-all” approach that works for all disciplines or educational models.
Challenges for Public Health Students
Despite public health being one of the founding disciplines for IPEC, public health students continue to face challenges in identifying IPE experiences that meet their needs (Singh et al., 2019) because IPE activities have traditionally focused on patient care in a clinical setting. While health professional students are increasingly expressing interest in public health and prevention, many IPE activities continue to underrepresent public health either by not including public health students or focusing exclusively on clinical scenarios. IPE programs that do include public health perspectives, tend to focus on cultural competency, patient-centered medical history taking, and use of language and translation services (Aelion et al., 2015; Anderson et al., 2019; McCloskey et al., 2011), rather than scenarios that fully encompass the social determinants of health and other public health principles (Fulmer & Gaines, 2014). The narrow focus on clinical settings prompted IPEC to expand the IPE framework to be more inclusive of public health (Interprofessional Education Collaborative, 2016). Other organizations such as the Institute for Healthcare Improvement developed the “triple aim” framework, which includes a public health focus (Earnest & Brandt, 2014). Despite these approaches, public health concepts are still not fully integrated in student IPE experiences.
Challenges for Distance-Learning Students
Research on IPE for distance-learning students lags behind research for traditional, face-to-face students. For example, McCutcheon et al.’s literature review from 1971 to 2015 revealed 478 IPE studies, with only 16 conducted in the distance learning arena (McCutcheon et al., 2017). One reason may be that many of the features that attract distance learners (flexibility, asynchronous learning, lack of travel) may not be ideal for traditional IPE offerings. In particular, the ability to collaborate in the same physical space, as may be required for a clinical simulation, is difficult when learners are geographically dispersed. Even synchronous case study collaborations may be difficult if learners are located across time zones. As interest in online learning continues to grow at a rapid pace, it is not surprising that some public health academic programs have initiated online IPE opportunities for their students. These IPE opportunities remain limited in number and scope, such as the program for undergraduate public health students at the University of Michigan, which introduces IPE concepts but does not facilitate collaboration with other health sciences students (Anderson et al., 2019).
Existing Models of Online Education for IPE
Models of online education used for IPE include both synchronous (real time) and asynchronous (teaching and learning not simultaneous) delivery (Sanborn, 2016), as well as a variety of modalities including online simulations and case-based discussions (McCutcheon et al., 2017; Moote et al., 2019; Packard et al., 2018). To date, these models of online education have focused largely on clinical health sciences, with little or no inclusion of public health students or scenarios.
With no robust online model that included public health content, the Executive MPH (EMPH) program at an accredited school of public health in the U.S. Southeast needed to develop a model that allowed its working professional students in a distance-education program to participate in IPE training. Therefore, the EMPH program developed an online, asynchronous didactic module built into the university’s learning management system (LMS) and a remote synchronous case study experience that leveraged the diverse experience of the working professional students in the executive program. In this article, we describe the program and discuss potential applications for other distance-learning programs and disciplines across the health sciences.
Executive Master of Public Health Program Description
The EMPH program described herein offers an MPH degree with three majors: Applied Epidemiology, Applied Public Health Informatics, and Prevention Science. Students come from a variety of professional and disciplinary backgrounds and must have a bachelor’s degree and a minimum of 3 years of professional work experience. The EMPH is a hybrid-online program in which working professionals attend classes in person for two weekends each semester (first and last weekend of the semester) and in the intervening weeks, the curriculum is offered online via the university’s LMS. Courses are offered in an asynchronous format because our students are spread across time zones throughout the United States and, in some cases, internationally.
Given the realities of geography and competing professional responsibilities for our student population, participation in a traditional “Interprofessional Education Day,” where students from a variety of health sciences disciplines come together in person to address various scenarios or case studies, was not feasible. This limitation is common for distance-based and executive students. Nonetheless, students in these programs still need to complete interprofessional practice training for their own growth and to meet accreditation standards.
The EMPH IPE Program
While we have mentioned the challenges of participation in the existing IPE training formats, our EMPH students also presented unique advantages to the development of an IPE experience. Most notably, our EMPH students bring an average of 7 years of professional experience from a diverse range of fields and disciplines. Building on this diversity, we realized that while our students are all studying to obtain an MPH degree, they are a group of professionals from varied disciplines in their daily work lives. Therefore, with guidance from our accrediting agency, CEPH, we asked the EMPH students to participate in the IPE experience while representing the disciplines of their “day jobs” rather than the discipline of public health. With this “day job” approach, students participated in all the components of our IPE experience from the perspective of their employed discipline. A sampling of the disciplines included in the 2018–2019 cohorts is shown in Figure 1.
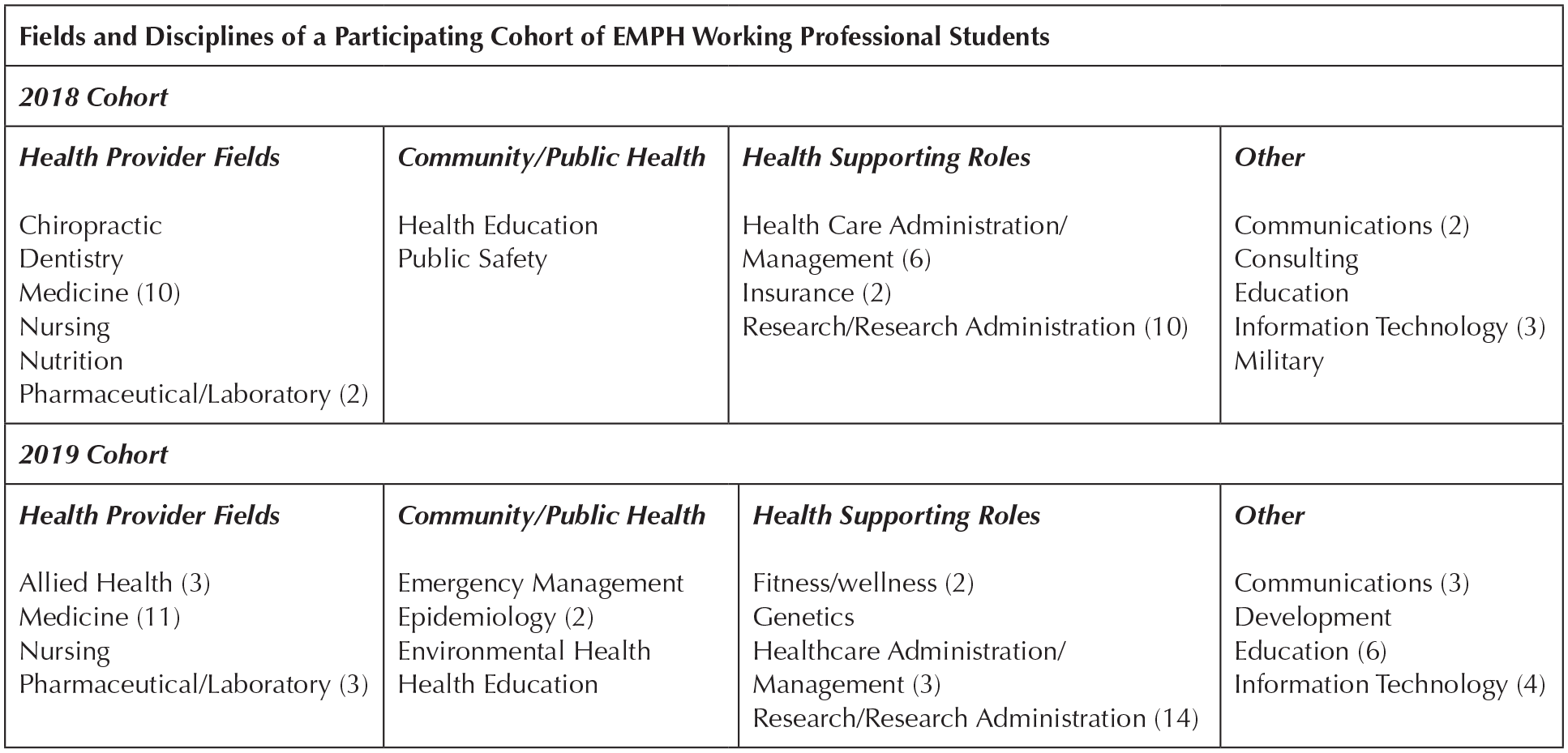
Fields and disciplines of Executive MPH (EMPH) working professional students.
We piloted this EMPH IPE program in 2018 and revised it for the 2019 cohort. The development of our IPE program began with a review of the four key interprofessional practice competencies from the 2016 IPEC Report and consideration of both the special needs and opportunities our specific student population presented. The key interprofessional competencies from IPEC (Interprofessional Education Collaborative, 2016), can be seen in Figure 2.
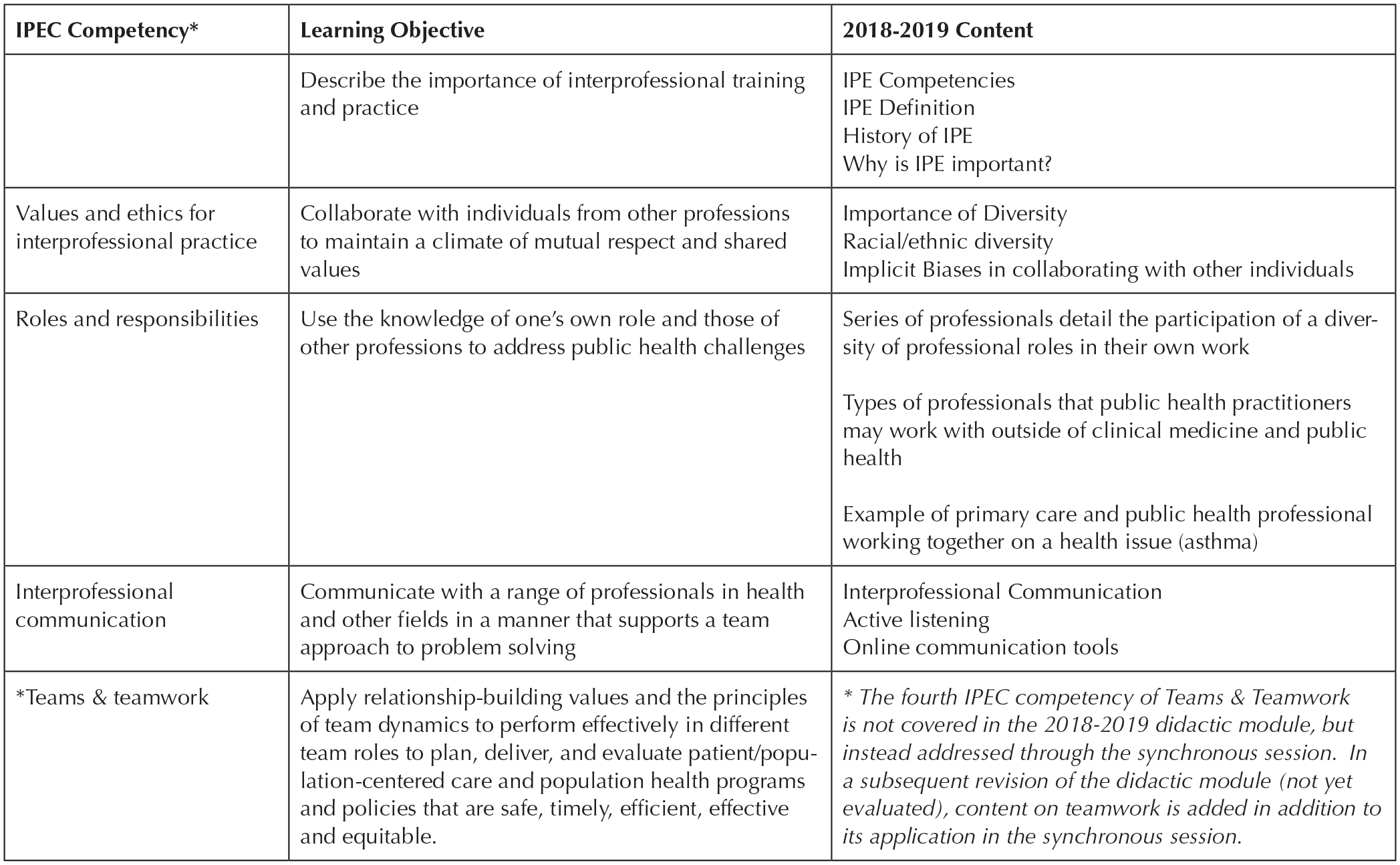
Interprofessional Education Collaborative (IPEC) competency and corresponding learning objectives and content for the didactic module.
Using these key interprofessional competencies as the foundation for our IPE program, we curated a collection of materials and exercises that could be used to create a rich, interactive experience for executive students. We created a four-part online experience consisting of (1) an asynchronous, self-paced didactic module; (2) a synchronous case study group discussion; (3) group development of a video solution to the case study; and (4) peer review of other groups’ case study solutions.
Asynchronous, Self-Paced Didactic Module, and Quiz
Based on the key interprofessional competencies, we created a self-paced didactic module delivered through the university’s LMS. The didactic module included an introduction to the importance of interprofessional education, as well as a detailed introduction to each of the first three competencies listed above. The didactic materials included web pages, originally-developed videos, secondary videos selected from reputable sources, and links to reports and programs, such as Project Implicit of Harvard University (Project Implicit, n.d.), which works to educate the public about hidden biases. Notably, Competency 4, regarding teams and teamwork, was addressed through practice in the synchronous session discussed below. Students were given 3 weeks to complete the didactic module individually, which took approximately 2 to 3 hours to complete. At the end of the didactic module, students were asked to complete a short quiz that included a mix of short answer questions regarding the application of what they had learned to their own professional lives and multiple choice questions on the presented topics. Figure 2 details the learning objectives and content for each section of the didactic module.
Synchronous Case-Study Group Discussion
The synchronous session was intended to address the fourth IPEC competency, to “apply relationship-building values and the principles of team dynamics to perform effectively in different team roles to plan, deliver, and evaluate patient/population-centered care and population health programs and policies that are safe, timely, efficient, effective and equitable.”
Following completion of the didactic module, students were intentionally grouped with three to four other student-professionals such that a minimum of three “day job” disciplines were represented in each interprofessional group. These groups were brought together in one synchronous session via webinar technology to work through a public health case study on the opioid epidemic. Prior to the session, students were provided information on case study discussions and how to prepare for case-based learning, the learning objectives for the case study, the case study writeup and discussion questions (Figure 3), and information on presenting their group findings. The synchronous case-study session was designed to last for 2 hours and was facilitated by an interdisciplinary group of faculty members affiliated with the EMPH program.
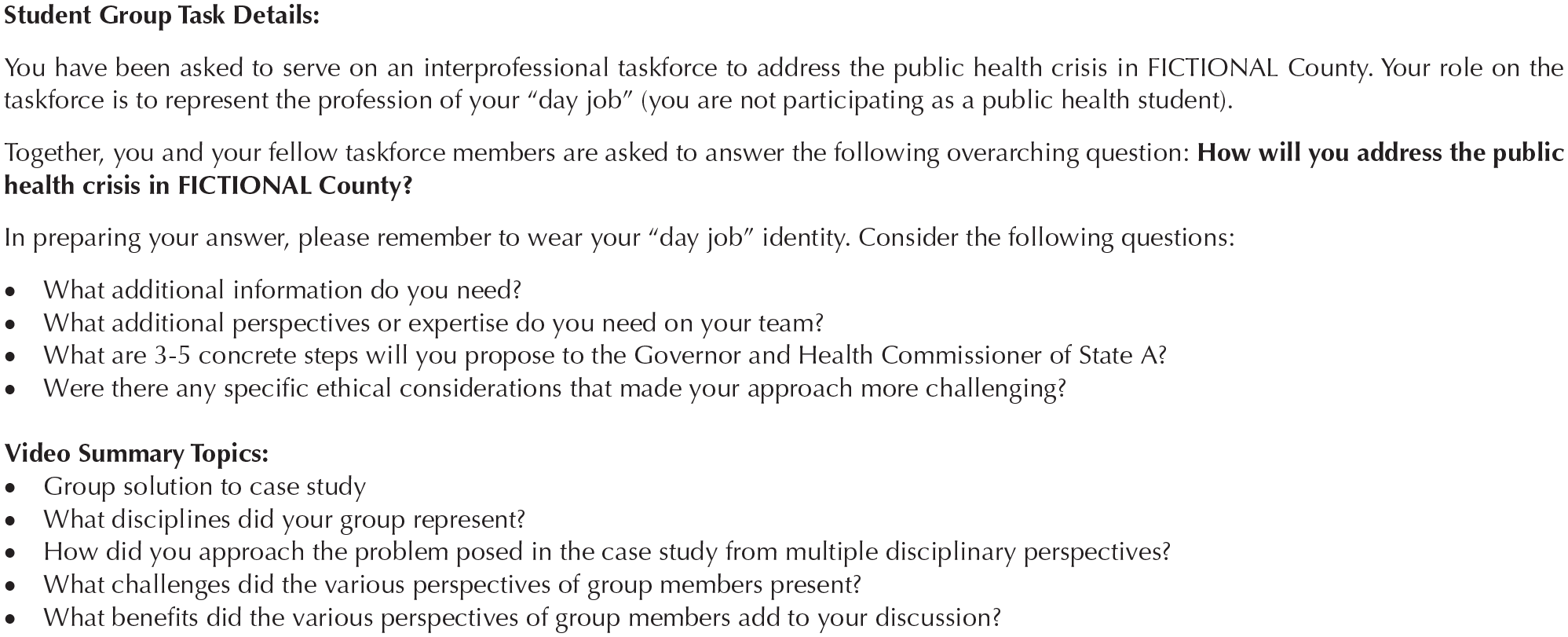
Synchronous case study session discussion questions and video summary instructions.
Video Solution to the Case Study and Peer Review of Other Groups’ Case Study Solutions
Finally, on completion of the synchronous case study session, each student group was given 2 weeks to create a 5- to 7-minute video summary of their case study findings and post the video to the LMS. Students were asked to discuss the impact of working with professionals from other disciplines and answer discussion questions (Figure 3). The video presentations were added on the course discussion board so that they were available for all students to review.
Once group videos were submitted, each individual student had 2 weeks to comment on a minimum of two group videos that they were not involved in creating. This created a dialog about the differences in both recommendations and perspectives for the case study under consideration.
Preliminary Evaluation
Based on guidance from the CEPH, the school of public health, which houses the EMPH program, was advised that participation in interprofessional team training activities as described herein was sufficient to meet the IPE competency. Process evaluation measures were implemented to ensure that all students (1) participated in the group synchronous session and (2) created/presented a video response to the case study with their multidisciplinary team.
Immediately after the pilot IPE program was completed, students were asked to participate in a short evaluation survey. Although only eight of 46 students in 2018 completed the evaluation, 87.5% reported being satisfied or very satisfied with the program and all but one student agreed with the statement that “The IPE module developed my ability to collaborate with individuals from other professional backgrounds.” Qualitative comments were generally positive, with students expressing appreciation for the course as a whole and the thoughtful solutions prepared by fellow students and groups.
The IPE pilot program also included the standard online course evaluation that is used for all courses in the school of public health. Notably, this evaluation was not available for students until the end of the semester, nearly 2 months after the program was completed. Therefore, recall bias and lack of participation may have affected responses. Nonetheless, 18 students (40.9%) completed the course evaluation. Of students completing the evaluation, 61.1% agreed or strongly agreed that they learned a great deal from the IPE program, 11.1% were neutral, and 28.3% disagreed. Our team also debriefed with faculty facilitators for the IPE program and found similar themes to those reported in the course evaluations. All feedback was considered and incorporated into the revised second iteration of the program for the 2019 cohort, for which the feedback continued to be similarly positive.
Students in the 2019 cohort also completed the Nebraska Inter-Professional Education Attitudes Survey (NIPEAS; Beck Dallaghan et al., 2016) before and after completing the online and synchronous didactic modules. The NIPEAS asks a series of 19 IPE attitude questions for which respondents use a 5-point Likert-type scale (strongly agree, agree, neither agree nor disagree, disagree, strongly disagree). Variables in the scale are broken out into the following constructs: Team Approach to Health Care (eight items), Receptivity to Teammates (five items), Self-Efficacy as a Team Member (four items), and Ethics in Health Care (two items). Table 1 shows the 19 items covered in the NIPEAS (Beck Dallaghan et al., 2016) and pre- and postparticipation means for each scale construct. Of the 42 students completing the pretest, 22 also completed the postsurvey demonstrating improvement on a number of the attitudes measured in the scale. Significance is measured by paired-sample T tests. Due to a data collection error, one of the self-efficacy questions (S1) was left off of the data collection instrument for the pretest. Therefore, we have imputed the mean of all the other self-efficacy variables for each absent student response to the missing self-efficacy question. The mean difference between the imputed value for the missing variable preintervention and the true postintervention value was .41 on a 5-point scale. In contrast, the mean difference between the pre- and postvalues on the other three self-efficacy measures was .38 (range .32–.41), suggesting that imputation was appropriate. Results indicate relatively high means for self-assessed attitudes toward IPE even among the PRE cohort. However, improvement was seen on many of the NIPEAS constructs after participation in the IPE module. In particular, statistically significant improvement was seen on three out of eight of the Team Approach to Healthcare variables; four out of five of the Receptivity to Teammates variables; three out of four of the Self-Efficacy as a Team Member variables; and one out of two of the Ethics in Health Care variables.
Descriptive Statistics for NIPEAS Means Pre- and Postintervention (n = 22).
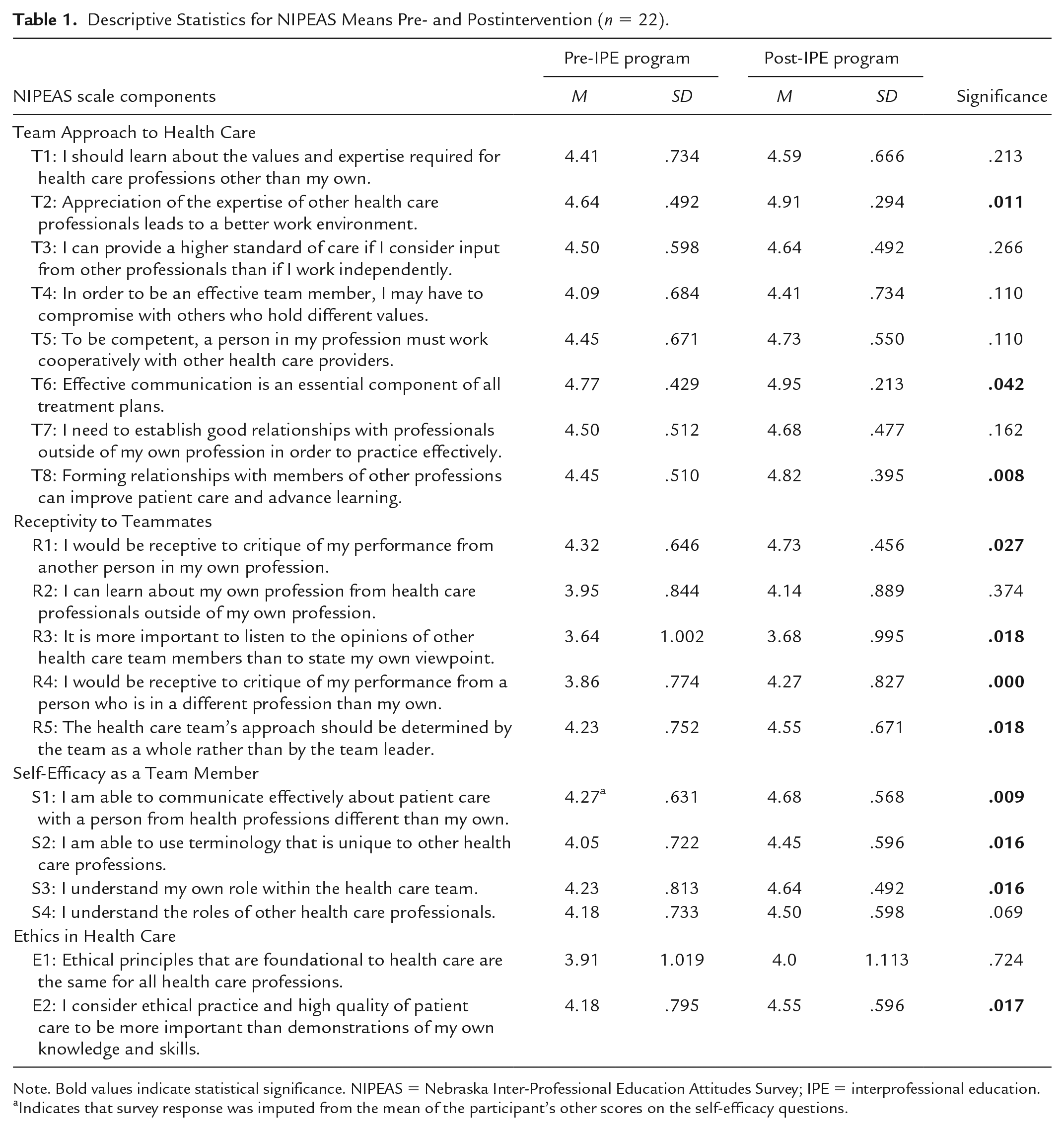
Note. Bold values indicate statistical significance. NIPEAS = Nebraska Inter-Professional Education Attitudes Survey; IPE = interprofessional education.
Indicates that survey response was imputed from the mean of the participant’s other scores on the self-efficacy questions.
Discussion and Recommendations
As COVID-19 pushes even more programs and disciplines to consider virtual learning, we share this model as one creative example of offering interprofessional training that may be adapted for other disciplines or student groups. There are certainly other models of IPE education available, although we were not able to identify any that specifically addressed our population of need—working-professional, distance learning public health students. As distance learning becomes increasingly pervasive in higher education generally and health sciences education specifically, it is incumbent on educators to ensure that professional students in health disciplines are able to achieve interprofessional education competencies regardless of their geographic location or modality of education.
With this in mind, we offer the following recommendations for programs seeking to establish a distance-based IPE curriculum.
Recommendations
Find creative ways to leverage the work experience of distance-learning students to support learning about interprofessional practice. Prior work experience, even when outside of health care, may provide a valuable lens through which the students can think about working with other professionals. For example, a teacher who returns to school to receive a nursing degree may have valuable insights about working with children and parents.
Use a mix of asynchronous and synchronous technology to facilitate a better interactive experience. Our IPE program built on the idea of a flipped classroom by thoughtfully mixing technology to facilitate a strong interactive experience. In a flipped classroom, students first gain exposure to new material outside class and then use class time to do the harder work of assimilating that knowledge (Akçayır & Akçayır, 2018; Al-Samarraie et al., 2019). In our program, we used a suite of specific technology, both synchronous and asynchronous in the following ways:
● Canvas learning management system is used to present an asynchronous didactic module for students to review. Within Canvas, we used a variety of teaching strategies including newly developed videos, interactive microlearning modules, links to secondary videos, readings and resources, and knowledge check quizzes.
● Zoom webinar technology is used to facilitate a synchronous case study session.
● Narrated PowerPoint technology is used by students to create a short video discussing their group’s solution to the case study.
● Canvas is again used for students to house their narrated PowerPoint videos and to participate in a discussion board commenting on the solutions by various groups.
The mix of these different types of technology lead to a rich, interactive experience.
3. Obtain regular feedback and evaluation of the IPE program with regard to content, modality and student learning. Whereas evaluation of any new program is important for ongoing quality control and improvement, the complex structure of a program such as the one described in this article requires examination of content, teaching modality and the acceptability of technologies used. In each iteration of our program, we have made revisions to both content and technology, based on feedback from participating students and faculty. We have also created a more comprehensive evaluation plan for future iterations of the program, including surveys, in-depth interviews and focus groups to better evaluate student meeting of learning objectives.
4. Include both public health and clinical perspectives in the IPE didactic module and trainings. Even though the program developed herein was targeted for public health students, there were times where it was difficult to find existing materials addressing a topic through the lens of public health. Nonetheless, it is important for all health sciences students to learn from both population and clinical perspectives.
Limitations
This descriptive article focuses on describing a unique implementation of IPE for distance-learning students. We provided limited evaluation data in the hopes that it might be instructive for other programs to consider for their own evaluation plans. However, we note that the sample sizes for evaluation are quite small and cannot be generalized. Furthermore, data collection errors potentially introduce bias into results, despite our attempts to correct for them. For future iterations of our IPE program, we have established a detailed evaluation plan that includes data collection from a variety of stakeholders (e.g., students, faculty facilitators, and university decision makers) in the form of surveys, focus groups, and document/archival review. We look forward to the opportunity to thoroughly evaluate this program.
In closing, we wish to describe the next steps of our IPE program. Following the second iteration of the program, our team received funding from an internal university grant to complete a more thorough restructuring of the didactic module and affiliated case studies. Our mandate was also to broaden the training materials to be used for all health sciences students within the university (e.g., medicine, nursing, physical therapy). To facilitate this expansion of the IPE training, we convened an expert advisory panel of faculty from across the university’s Health Sciences Center who met with our team several times to provide feedback on content and format. Preliminary evaluation data plus the feedback from the expert advisory panel, have resulted in further improvements including the creation of interactive microlearning modules, updated content and highlighting why each content area is important for students. The revised program is under development at the time of this submission and will be available for students in fall 2020. We feel we now have a good foundation to address the unique IPE needs of distance learning working professional students and share this experience so other distance-learning MPH programs can benefit from our experiences.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.