
Abstract
This article argues for a more rigorous engagement with intersectionality within political ecologies of health. Building on the work of feminist scholars who explore the co-production of social and ecological differences, I examine how health improvement schemes that target practices of natural resource use concentrate value (economic and ecological) and health dividends in particular bodies at the expense of others. As part of this intervention, I draw on long-term and ongoing ethnographic research in north-central Sri Lanka. This region is an endemic zone for a mysterious and deadly form of kidney disease (CKDu) as well as the site of frenzied health improvement intervention. Specifically, and in response to scientific studies that link kidney disease to agrochemical use and drinking water, an increasingly diverse range of actors, from different branches of the state apparatus to private industries and civil society organizations, have invested heavily in reconfiguring the region’s water supply infrastructure and agrarian landscapes. Through an analysis of resident testimonies, I demonstrate that the burden of subsidizing these new “healthful” practices of water provision and agricultural production is unevenly experienced, as are residents’ abilities to adopt and maintain them over time and space. More crucially, I illustrate how schemes designed to heal turn on the production of differentiated harms, including new gendered labor burdens for poor women, and intensified agrochemical use for ecologically and economically resource-poor farmers. Developing these narratives toward a feminist political ecology of health, I demonstrate how social, ecological, and bodily differences intersect to constitute new patterns of health and harm in the dry zone. I conclude by reflecting on how this approach can explain the paradoxical effects of well-intentioned disease mitigation strategies.
Introduction
On a hot June morning, I, like many other residents of the agrarian settlement scheme of Padaviya made the daily walk to a nearby Buddhist temple which now doubles as the home of what residents call “RO” (Reverse Osmosis) water filters. The filter was built within the temple complex in 2016 and is one of twenty-seven RO plants constructed across the settlement scheme in a bid to improve residents’ kidney health by increasing the quality and quantity of their water consumption. According to its attendant, the filter purifies groundwater pumped from two deep tube wells that sit adjacent to it.
On average, it distributes 2000 liters of filtered water per day, mostly to residents who live nearby. An additional 5000 liters of water “are sold to local bowsers” (water tankers) which then transport the water to other areas, local businesses, and private residents. At the time of my visit, water was sold for 50 c/l. “We used to sell for Rs. 1/l” 1 the attendant explained, but “because of the failed cultivation last season, we have reduced the price.” However, as I had discovered through my ethnographic fieldwork in the area, the cost of filtered water varied, and some residents continue to pay up to Rs. 2.50/l for the convenience of having water delivered to their homes.
This RO plant is run by the civil defense authority and is staffed by men in their late thirties with crew cuts and navy-blue shirts. It, like almost every filter I have visited during my fieldwork in the north-central dry zone of Sri Lanka, is the culmination of a unique set of actors and interests. The plaque on the side of the small building which houses the filtration equipment lists a collaboration between five groups: The Chemistry Department of a local university, a prominent Buddhist organization, a prominent national TV station, a Radio Broadcasting Company, and the Civil Defense Force. This filter is also one of several within a mile radius: the attendant lists three administered by the armed forces in close proximity, and another filter down the road constructed by a prominent businessman based in the country’s capital, Colombo. Over the course of the morning, I watch people collect purified water from two small taps on the side of the RO plant. They come with plastic containers varying in colors and sizes. On average, the attendant tells me that “when a person comes to purchase water, they bring a 20–25 liter can and they come every 2–3 days.” This water, he explains, “is meant for drinking and cooking, but a lot of people can’t afford to do both. Whatever quantity [of water that] they take home, is rationed very carefully.” Some come on bikes, others in trishaws or vehicles. Like all the filters that I visited during my fieldwork, most who come by foot are women. And as I watch these women walk away their bodies form strange silhouettes, weighed down and distended at odd angles by the containers of water that they carry with them.
As my tour of the small facility winds down, we end up at a small concrete tank overflowing with the byproducts of the filtration process. I had discovered earlier that morning that for every 3 liters of water pumped from temple’s wells, 1 liter becomes wastewater. The discharge is white and has the appearance, though not the smell or texture of diluted milk. “Don’t touch it!” the attendant says, when I follow a stream of wastewater diverted to a nearby field. “It will burn your hands.”
This encounter provides a window onto how health improvement interventions reconfigure patterns of natural resource use and herald new socially and ecologically differentiated relationships between water and health in north-central Sri Lanka. Since the first cases of mystery kidney disease (CKDu) were discovered in the early 1990s, there have been myriad government and civil society schemes designed to improve kidney health in this region. These programs have included the construction of community-scale RO water filters, but also the distribution of indigenous rice varieties to farming households, and the promotion of “toxic-free” or organic agriculture. While there is still no scientific consensus on the etiology of CKDu, these interventions draw strength from clusters of research that suggest the geochemical composition of the groundwater, chronic dehydration, and agrochemical exposures are crucial factors that shape the pathogenesis of this disease (Bandara et al., 2010; Chandrajith et al., 2011a; Jayatilake et al., 2013). While most research on CKDu is preoccupied with discovering the etiology, mapping the prevalence, or quantifying the economic costs of this disease, very little work has examined how schemes to manage CKDu transform possibilities for health and rework the long-term sustainability of socioecological relationships in the dry zone.
Against the backdrop of ongoing and intense speculation about mysterious kidney disease, this article documents how health improvement interventions materially transform dry zone environments, social relations, as well as health opportunities and exclusions. As part of this intervention, I examine how schemes to improve kidney health create unexpected health-environment relationships as well as new social, bodily, and ecological differences. Specifically, I utilize the feminist concept of intersectionality to demonstrate why it is important to analyze the production of these social, ecological, and health differences in concert. As an approach that traditionally investigates how race, class, gender, and other dimensions of difference work as “interdependent and interlocking rather than disparate and exclusive social categories” (Mollett and Faria, 2013: 120), intersectional analysis “opens up possibilities to understand how power operates not only in two dimensions, but rather in multiple dimensions that can have lateral and unexpected consequences for bodies…, subjectivities” and indeed, health (Nightingale, 2011: 155 emphasis added). I argue that in the wake of CKDu-related intervention, intersectional analyses can help explain why some dry zone residents struggle to translate increased access to “healthful” resources like filtered water and native seed into real dividends for health and well-being. More broadly, the analytic of intersectionality sheds light on how and why health improvement schemes generate new yet unevenly experienced harms by: (i) intensifying labor burdens and labor-related health conditions among economically disadvantaged women; and (ii) intensifying debt and dependence on agrochemical use among economically and ecologically resource-poor farmers.
My central argument is that schemes to promote kidney health set in motion interdependent and recursive processes of social, ecological, and bodily differentiation that rework the distinctions between what harms and what heals, as well as who is harmed and healed. That is, I argue that the production of differentiated harms and uneven exposures to risk are in fact, central to how disease mitigation strategies unfold on the ground. By analyzing these dynamics through the concept of intersectionality, polyvalent relationships between health and environment are brought into sharp relief. I conclude by arguing that efforts to promote health in regions that are designated by the Ministry of Health as kidney disease hotspots need to engage with the intersectional dimensions of power (social, ecological, and bodily) that shape uneven health outcomes and uneven capabilities to adopt or maintain “healthy” consumption and cultivation practices. 2 Without doing so, these health improvement schemes will continue to fall short of their stated objectives and give rise to paradoxical effects as has largely been the case thus far.
Toward a feminist political ecology of health
In recent years, the field of feminist political ecology has directed attention to “the multiple kinds of oppressions and privileges people face” in struggles over resource access and control (Mollett, 2017: 150). Central to this analytical shift is the concept of intersectionality which at its core investigates how social relationships and subjectivities are “produced through the ways axes of power (gender, race, ethnicity, class, sexual orientation, age (dis)ability) intersect and emerge in relation to one another, rather than being based on stable or given understandings of social difference” (Elmhirst, 2015: 523). Anchored in a long-standing tradition of black feminist thought (Gines, 2011), and coined by Kimberle Crenshaw in 1989, the theory of intersectionality responded to blind spots in existing activism for civil rights and women's empowerment in the United States. As Crenshaw (1990) takes pains to point out, while these movements were motivated by important social justice goals, they all failed to grapple with the complex discrimination experienced by African American women. As a consequence, intersectional frameworks arose to better account for the particular constellation of oppression African American women faced as simultaneously black and workers and women (Collins, 1998; Collins and Bilge, 2016; also see: Crenshaw, 1989, 1990; Guy-Sheftall, 1995; Hooks, 2000).
Owing significant debts to this history of black feminism, intersectional approaches have taken scholarship in the field of political ecology in new directions, extending studies of water access and control (Sultana, 2009, 2011, 2012; Truelove, 2011), sanitation infrastructures (Truelove and O’Reilly, 2021) migration and development (Bastia, 2014; Mollett and Faria, 2013), agrarian environments (Nightingale and Harcourt, 2021), climate change and nutrition (Nichols, 2016; Nyantakyi-Frimpong, 2021), and community forestry programs (Nightingale, 2011). Cutting across this work is a focus on how embodied practices of resource use and engagements with the physical environment variously reproduce and disrupt “the boundaries that keep distinctions between ethnic groups, [gender hierarchies], and castes clear” (Nightingale, 2011: 154, 2012). More recent interventions draw on the concept of intersectionality to theorize the emergence of “racialized genders” in the wake of national and international development practice as well as how gender relations emerge within local hierarchies of race and religion (Mollett, 2017; Mollett and Faria, 2013). As a consequence, an important review of feminist political ecology by Rebecca Elmhirst (2015: 63) concludes that among the greatest strengths of intersectional approaches is that they pay “attention not only to how … patriarchy and racism are imbued in shaping human-environment relationships … but also to the role of nature in producing particular identities and bodies.” Stated simply, this kind of work draws our attention to how categories of social difference such as gender, race, caste, and class operate and are at times challenged, through interactions with material environments.
In dialogue with this work, political ecologists who study water insecurity and agrarian landscapes provide important scaffolding for re-theorizing intersectionality to more explicitly address “eco-social relations” (Nightingale and Harcourt, 2021; Thompson, 2016; Thompson et al., 2017). By attending to the “causal powers” of differentiated ecologies, this work illuminates how patterns of environmental dis/advantage are enrolled in creating social difference. Through his analysis of pesticide use, agrarian capitalism, and agri-food system governance in Costa Rica, for instance, Ryan Galt (2014) documents how ecological gradients of climate, soil fertility, elevation and pest-pressures, and specifically the environmental advantages that accrue from access to land with favorable ecological characteristics, increase the profit margins of resource-rich farmers while reducing their pesticide exposures. At the same time, the uneven ability to relocate production and to access “environmental advantages” locks most resource-poor farmers into a “faster and more powerful pesticide treadmill” (Galt, 2014: 87). Highlighting how the materiality of water can deepen intersectionality theory and method, Thompson (2016, 2017) and Sultana (2020) pluralize the forms of difference that count in struggles over water, with a specific focus on how ecological processes of differentiation intersect with social complexities to determine patterns of access and insecurity as well as differentiated experiences of citizenship.
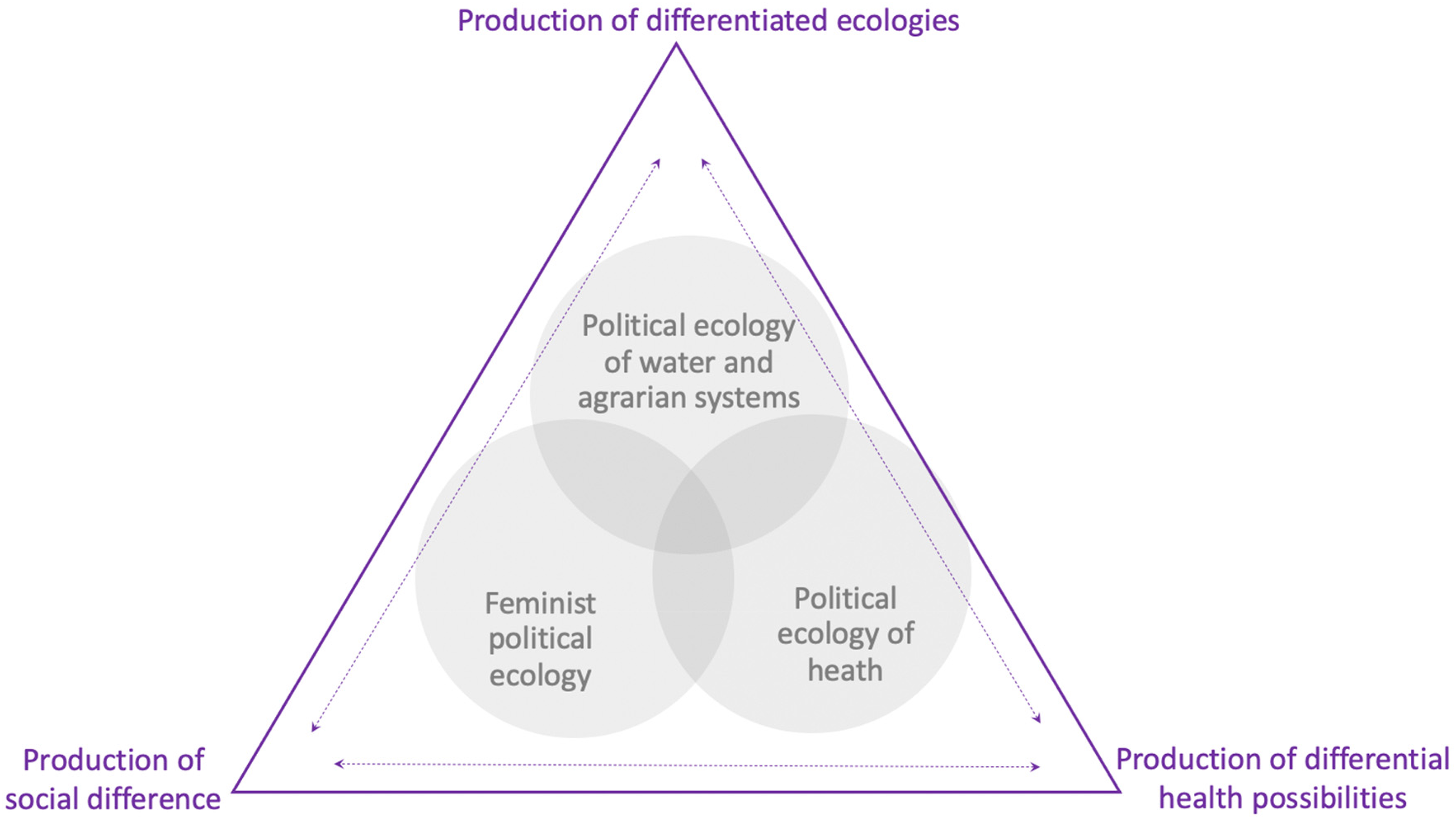
Crucially, this work displaces the assumption that nature is “outside of” or irrelevant to the production of identity and embodied difference. Instead, scholars across different domains of political ecology demonstrate that struggles over natural resources, and “changing environmental conditions bring into existence categories of social difference… In other words, [difference]… itself is re-inscribed in and through practices, policies and responses associated with changing environments and shifting modes of resource governance” (Elmhirst, 2015: 523; Figure 1).
Towards a feminist political ecology of health.
Together, these scholarly contributions have far-reaching implications for imagining and practicing political ecologies of health. As a field deeply invested in theorizing the patterning of health inequalities at various scales, political ecologies of health contextualize patterns of disease incidence and virulence within social, political-economic, historical, and/or ecological settings and give conceptual weight to the dynamic ecological relationships within and between bodies and the environment (Guthman and Mansfield, 2013; King, 2010, 2015). While intersectional analysis is not new in geographic work on disease/illness (see: Craddock, 2000), political ecologies of health rarely take up the concept as part of their analytical toolkit (Carney, 2014; Jackson and Neely, 2014a; Nyantakyi-Frimpong, 2021 are important exceptions). 3
Yet, work in other domains of political ecology suggests much potential for expanding the field through theories of intersectionality. Doing so, requires situating the production of uneven health risks within multiple and intersecting power relations, where both privilege and oppression shape patterns of health exclusions and possibilities. Stated simply, intersectional theory calls on political ecologists to investigate how the synergistic and interactive effects of social, ecological, and bodily differences produce “lateral and unexpected” consequences for health, including new openings for contesting and transgressing health exclusions. At the same time, by foreground intersecting, compounding, and sometimes mutually reinforcing differences (social, ecological, and bodily), an intersectional framework can provide new insights into how and why health inequalities can be so difficult to transcend. In this article, I contribute to political ecologies of health by documenting how health inequalities can be variously produced and disrupted through the intersection of specific ecological contexts, patterns of social difference, and shifting states of health. It is precisely because of this potential to illuminate the co-production of social difference, differentiated ecological relations, and differential health possibilities that I argue intersectional approaches are germane to emerging health-environment research.
Context and methodology
To demonstrate how political ecologies of health can be sharpened by intersectional analysis, I draw on 15 months of ethnographic data collection in the north-central dry zone of Sri Lanka (2013–2017). This includes interviews with 74 residents of two kidney disease hotspots: the agrarian settlement schemes of Sri Pura and Padaviya, structured surveys of 222 households across both sites, and participant observation of rice cultivation and water procurement practices (see: Senanayake, 2020, 2022 for a detailed discussion of interview and survey methodology). Analysis of semi-structured interviews and survey data shed light on how and to what extent speculated health risks socialize new behaviors of consumption and cultivation in areas where mystery kidney disease is endemic. I also used these methods to track the mechanisms driving these changes; the emergence of new sets of relations between residents and the environment; and the perspectives of people about the disease, environmental risk, as well as disease-mitigation responses in the region. In addition to semi-structured interviews and household surveys, I conducted field transect walks (Doolittle, 2015) and on-site observation to confirm the type of seed and farming practices employed by farmers in my household surveys. As a participant observer, I documented practices of water procurement and paddy cultivation. I also accompanied women in some of their daily activities such as collecting water from filters and preparing meals. Through long-term participant observation and semi-structured interviews, I bring into sharper relief the difficult compromises of those who live in kidney disease hotspots. As a result, I demonstrate how the production of differentiated harms and uneven exposures to risk are in fact, central to how disease mitigation strategies unfold on the ground.
Empirically, the article examines government and civil society programs to promote kidney health by investing in: (1) community-scale RO filters and (2) indigenous and organic rice cultivation. Since the first cases of mystery kidney disease were identified in the early 1990s, dry zone waterscapes and agrarian systems have become sites of intense speculation about health risks as well as settings for multiple waves of disease-related intervention. Crucially—and against the backdrop of ongoing contestation and debate about CKDu’s cause—these disease mitigation strategies are pitched as “win-win” or “no regrets” health solutions. In other words, whether—or not—groundwater or agrochemicals are actually implicated in the etiology of mystery kidney disease, it is widely accepted that reducing rates of agrichemical use as well as increasing the quality and quantities of water residents consume is generally good for health (epidemiological surveys suggest that the impact of intervention in the water sector on case numbers is significant, but to date, no scientific studies correlate shifts in agrarian practices to reduced prevalence of disease). 4 So, while much of this intervention is animated by the epidemic of kidney disease, in practice health improvement schemes that target environmental behaviors shape kidney disease prevalence through diffuse, contested, and complicated pathways, if at all. In this article, I therefore focus less on the question of whether these schemes have succeeded (or failed) in reducing rates of kidney disease. Instead, I put a feminist spin on the question posed by Tania Li (2005: 391, 2007) and James Ferguson (1994): “What do these schemes do? What are their messy, contradictory, [intersectional] effects?”
Embodying multiple dimensions of difference through everyday water practices
Until very recently, residents in Padaviya and Sri Pura relied almost exclusively on dug or tube wells for drinking water. However, as numerous hydrogeological studies have shown, these wells are often rich in mineral content and fluoride (Chandrajith et al., 2011a; Dissanayake, 1996; Tennakoon, 2004). In this area, groundwater quality is primarily determined by rates of hardness (i.e. content of sodium, potassium, and calcium), fluoride, and conductivity. 5 And as many studies which link CKDu to patterns of water use are quick to point out, regions where the disease is endemic far exceed national averages and international permissible limits for these three metrics (Chandrajith et al., 2011a; Paranagama, 2013). For instance, several studies estimate that rates of fluoride in the water are so extreme that dental and skeletal fluorosis in parts of the north-central dry zone is as high as 89.9% (Chandrajith et al., 2011a: 676; see also: Dissanayake, 1996; Tennakoon, 2004). Contemporary concerns about the effects of drinking water on kidney health emerge in response to these ecologies and histories of water use. Most of these arguments link the disease to the geochemical composition of groundwater, poor access to drinking water, and the inadequate intake of water in dry climates. And it is against and in response to this backdrop, that ongoing investments in community-scale RO filters and water purification schemes unfold.
Post-filter economies and ecologies of water provision
In Padaviya and Sri Pura, investments in RO plants not only displace local dependence on groundwater but also intervene in the intimate, daily practices of water procurement and consumption in the region. At first glance, it would seem that these new water purification schemes have transformed water consumption behaviors in quite comprehensive and complete ways: 90% of households that I surveyed in 2017, supplemented at least part of their domestic water consumption with filtered water. 6 Rates of filtered water consumption are higher (96%) among households with at least one family member who is sick (suffering from any chronic illness) and also, among families with at least one member suffering from kidney disease (95%). This change occurred rapidly and reflects an overhaul of local consensus about water risk and safety. Indeed, as recently as 2013, there were no RO filters in the area and more than 97% of residents relied on wells for drinking water (Padaviya Divisional Secretariat, 2015).
Yet, my ethnographic and survey data reveal that residents’ consumption practices are differentiated through complex and uneven ecological, political-economic, and bodily relationships. Specifically, RO filters have transformed geographies of groundwater access from a resource attained via land ownership or social relations into a commodity which is accessed through centralized points of provision, in exchange for money. Over the course of my fieldwork, for example, filtered water costs residents between 50 c and Rs. 2.50/l. These fees are generally reallocated to filter maintenance and repair costs; however, in some cases, RO plants generate new revenue streams by selling and transporting filtered water to residents in the area and thus operate as for-profit ventures. Through the promise of health dividends, RO filters have thus helped to create new economies of water provision, and in turn, these economies transform health opportunities and exclusions for residents of kidney disease hotspots.
Unsurprisingly, my survey data strongly indicates that these new waterscapes are not socially or ecologically neutral. Instead, they often re-inscribe and heighten differences in ways that concentrate value and potential health dividends among some residents and not others. For instance, families receiving poverty welfare benefits,
7
who constitute almost 15% of Padaviya and Sri Pura’s population, as well as households who rely on precarious farming incomes, experienced additional burdens in procuring filtered water (Padaviya Divisional Secretariat, 2015; Sri Pura Divisional Secretariat, 2015). As a clerk attached to a local NGO explained: A lot of groups from all over the country and even sometime outside, come to this area. They encourage us to drink more water and good filtered water, to be conscious of what we eat, and as much as possible to cultivate without chemicals, even if just for our own home consumption. One group even distributed a small number of cows and asked us to drink fresh milk (instead of well water). But the problem is that our economic situation makes it difficult to follow advice like this. We know what we should do. What we can do is something different. So many people here, drink filtered water if they can afford to drink it. There are some who can’t or who are old and can’t transport it, and so they continue to drink [well] water as they have little options to do otherwise. Now we are at a point where we have to pay for water to drink! In the past, we could drink freely from tanks, from streams, canals, and our wells. But now what are the options for the people of this community? For us to follow the doctors’ advice and drink filtered water we have to spend a lot and many people can’t afford to do this, at least not in the ways that the doctors prescribe.
Together these exchanges suggest that many of my interlocutors are forced to weigh the economic burdens of maintaining access to filtered water on a day-to-day basis against the potential long-term health benefits of shifting their consumption patterns. As a consequence, most families that I surveyed, including those with members suffering from kidney disease, continue to rely on mixtures of filtered and well water on a regular basis.
Unsurprisingly, the ability to translate increased access to filtered water into potential health dividends is indexed to residents’ socioeconomic status, with potential benefits accruing to households who can absorb the additional costs of maintaining access to filtered water over longer timescales and across multiple domestic uses. One example of this can be seen in the unequal distribution of household-level RO filters. The most popular of these during my fieldwork was the Kent Filter which sold for Rs. 35,000 (not including maintenance costs and part-replacement). 8 However, this cost is prohibitive for the majority of residents in the area and only 9% of households that I surveyed could afford to install a Kent Filter within their homes.
Instead, the majority of residents that I spoke with have outstanding household debts,
9
and rely on precarious farm incomes which place household-level filters out of reach. Lasantha, a zonal education officer for the DSD division of Padaviya, explained the difficulty to me: Not every person can afford to spend Rs. 35,000 to buy a good filter. There are only very few people who can do that, someone like me, I can do it because I don’t have a lot of family responsibilities and am a government servant, but for most people in the area, it just isn’t an option.
Who bears which costs, and under what conditions?
Not only have RO filters generated new costs and created new forms of contamination, but they have also produced new and uneven labor burdens as well. In the dry zone, as in much of South Asia, the task of water procurement conventionally falls to women. While health advisories about the quality and quantity of drinking water heighten anxieties among men and women about water risk, these discourses only partially reconfigure patterns of gendered responsibility for water provision in Padaviya and Sri Pura. In fact, my survey data indicate that when shifts occur, they are by and large limited to wealthier families. For example, men with access to motorcycles or vehicles increasingly assume responsibility for purchasing and transporting drinking water from community-level RO filters to their homesteads. class status also provides some women with a means of transcending the additional labor demands placed on them by community RO filters because these women either have smaller filters installed within their homes or have water delivered to large storage tanks constructed on their homesteads (to have filtered water delivered, it costs an additional Rs. 1–1.50/l). Stated simply, in more wealthy households, women are often able to avoid the pressures that more poor women face in practices of daily water provision. Moreover, access to household-level filters or the ability to pay for water delivery services in the context of kidney disease confers status and class relations that increasingly help to distinguish dry zone residents from each other.
For most households that I surveyed, however, filters re-inscribe gender hierarchies. Specifically, my data indicate that the real brunt of compensating for the increased time, distance, and labor demands of filtered water provision falls on the bodies of women who fetch water on one to three day cycles, and who cannot afford the costs of sustaining access over larger timescales. In particular, the emergence of filters run by the armed services—which during the course of my household survey began distributing 20 liters of free water per day to residents—created new intensities of labor burden for many women in the area. The rates of filtered water procurement amongst my interlocutors are profoundly shaped by the uneven monetary costs for filtered water across Padaviya and Sri Pura. 10 In one G.N Division that I surveyed, for instance, the recent construction of a new army filter reduced the monetary costs of water provision but increased the number of trips that women made to the filter and in some cases, increased the time and distance traveled to access “free” water. These burdens are most acutely felt by households who travel to the filter daily because they cannot afford the monetary costs of reproducing access over extended time periods. Instead, for many households, access to the potential health dividends of filter water is subsidized through important but often overlooked embodied costs.
The tradeoffs that emerge between gendered labor burdens and the potential health dividends of filtered water consumption are striking. My survey of 222 households illustrates that the rates of filtered water consumption are relatively high (4.4 l/person) for those who travel to the filter daily, allowing them to capitalize on potential health dividends. These women experienced greater rates of access and security about water quality than women of similar socioeconomic status who do not live in proximity to a filter that dispenses some water to community members for free. However, their “bodies bear the brunt of subsidizing and compensating” for the daily procurement of RO filtered water (Elmhirst, 2011: 524; also see: Sultana, 2009; Truelove, 2011). To access small supplies of water for “free,” they must make more frequent trips to the filter which in turn eats into time for other domestic responsibilities and circumscribes the flexibility of their daily labor schedules. Conversely, my survey reveals that women who traveled to RO plants less frequently, on five to seven day cycles, on average consumed 1 liter of filtered water less per day. The key point is that uneven political economies of filtered water provision and intensities of gender labor burden intersect to shape opportunities and/or constraints for women to circumvent health barriers while at the same time, women’s everyday practices around water use and consumption reproduce multiple hierarchies of social and bodily difference.
My findings also demonstrate that women’s bodies are unevenly exposed to health risks and ecological change through their daily practice of water use. In fact, as health improvement schemes that target water consumption rework one set of health-environment relationships they inadvertently give rise to others. Indeed, as many women that I interviewed pointed out, practices of water procurement in post-filter landscapes are accompanied by new risks and hazards including, an increase in the incidence of joint pain and fatigue among many women. Women’s bodies encounter differing degrees of wear and tear which are shaped by the diverse social positions that they occupy, as well as heterogeneous ecologies of groundwater quality, uneven costs of filtered water, and new anxieties about water safety. These trends in labor-related health problems were also a topic of my conversations with local doctors who noted an increase in women attending clinics for joint pain. The new harms that emerge from differing practices of filtered water procurement can help us better understand how and why health improvement strategies that target patterns of water use are experienced in contradictory ways and produce effects that undermine their stated objectives. As Yaffa Truelove (2011: 146) concludes in her work on chronic water shortages and embodied inequalities in Delhi’s public water distribution system, “only when analyses target inequalities that result from differing everyday practices does it become apparent that increased quantities of water and lower pricing may nonetheless do little to improve either water justice or the equitable distribution of [health] benefits across communities.”
The key point to emphasize here is that while interventions in the water supply sector treat residents as a homogeneous group that is uniformly affected by toxic environments, they do not have similar capabilities to adopt new “healthful” consumption behaviors. Instead, my analysis powerfully demonstrates that rural men and women are diversely positioned and engage in various strategies to procure water in post-filter landscapes. In particular, this intersectional analysis reveals who bears which costs (monetary and/or embodied) and under what conditions. Similarly, it brings to light new and important relationships between monetary, labor, and health costs by demonstrating how limited access to “free” filtered water results in greater consumption but also simultaneously increases gendered labor burdens and creates new health hazards for poor women bodies. It also draws attention to how new forms of difference are forged between residents as they respond to new anxieties about water safety and new geographies of water provision.
Deshiya rice cultivation and the social and spatial concentration of value, environmental advantage, and health
Not unlike the highly differentiated patterns of water use that I observed in post-filter landscapes, the work of Vasa Visa Nethi Ratak (Toxic-Free Nation) and other civil society actors promoting indigenous (deshiya) and organic rice cultivation as solutions to the problem of CKDu have concentrated health dividends, economic value, and environmental advantage in particular spaces and bodies (often at the expense of others). Through an analysis of (a) the current market structure for deshiya rice varieties, (b) chemically dependent agrarian ecologies, and (c) entrenched regional and class disparities, I explain how and why these social, spatial, and bodily patterns emerge. I argue that the highly uneven distribution of the economic, ecological, and health benefits of deshiya cultivation—both spatially and socially—has created legacies of economic loss that lock particular farmers into feedback cycles that reproduce their dependence on agrochemicals as well as their exposures to chemical risk.
Accumulation and loss in deshiya rice markets
In Sri Lanka, rice is cultivated by smallholders, primarily for a large national market. The overwhelming majority of farmers trade in markets for un-milled rice or “paddy,” and rely on agrichemical inputs and high-yielding rice varieties to maximize yields. 11 Very few residents in Padaviya and Sri Pura for instance, have the resources to de-husk and mill their harvests and sell polished rice grains directly to vendors or retailers. Instead, in conventional rice markets, farmers sell unprocessed paddy, often straight from their fields to large private buyers or the paddy marketing board who later thresh, dry, mill, package, and distribute rice to retailers.
Due to hypotheses that link CKDu to agrichemicals as well as the spatial and statistical correlation of this disease with rice-farming communities, dry zone agrarian systems have become sites of frenzied intervention (Chandrajith et al., 2011b; GoSL-WHO, 2012; Wanigasuriya, 2014). At the heart of the government’s disease mitigation agenda is the roll-out of a national initiative promoting deshiya and organic rice cultivation as a “long-term solution” to the problem of kidney disease. As I have discussed elsewhere, the Toxic-Free Nation Movement distributed indigenous rice seedlings, held workshops on organic cultivation techniques, and also lobbied heavily for bans on agrichemical use in the rice farming sector (see: Senanayake, 2022 for a detailed discussion).
While well intended, the Toxic-Free Nation Movement has nevertheless generated distinct patterns of accumulation and loss that rework distinctions between what harms and what heals, as well as who is harmed and healed. Central to these new patterns are processing and distribution networks in emerging markets for deshiya rice varieties, which are quite distinct from conventional rice value chains (see Figure 2). These markets are dominated by different branches of the state, local and international NGOs, and various ad hoc projects, the majority of which mediate deshiya rice markets as part of philanthropic, as opposed to, for-profit intervention. Only a very small percentage of farmers have been able to sell directly to consumers in metropolitan centers, and this was largely done by leveraging highly personalized and often ephemeral networks with health care infrastructure (i.e. stores in both western and ayurvedic hospitals), temple stores and/or via ad hoc NGO projects.
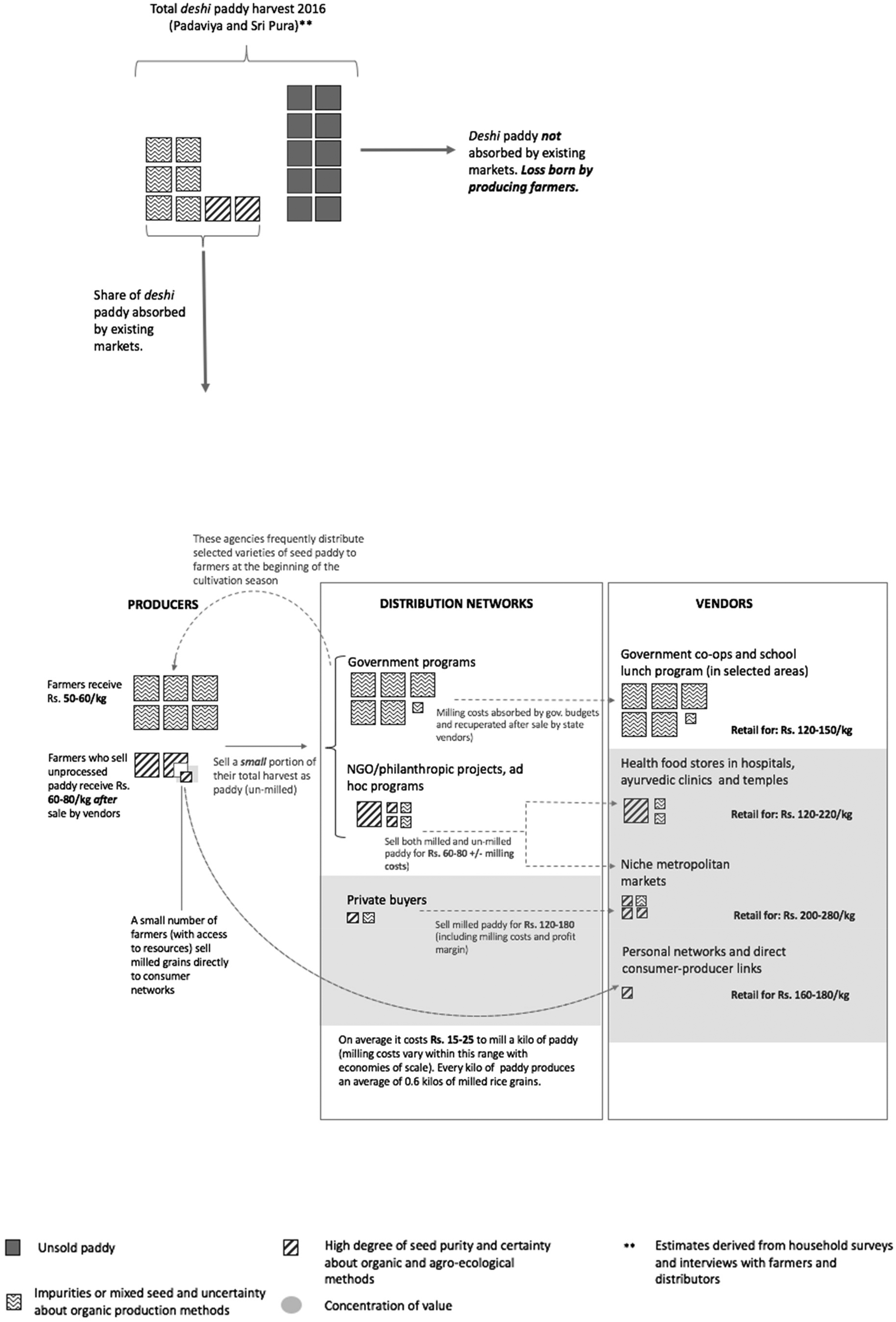
Distribution of value and loss in deshiya rice markets.
As several of my interlocutors noted, local markets (i.e. within the dry zone) capable of absorbing deshiya rice are few and far between: I’ve tried to sell our deshiya paddy to shops here [Padaviya], but there is no one willing to buy it, not even 1–2 kg. Instead, the best markets are in big cities, like Colombo, where deshiya rice grains sell for between 180–220 Rs/kg but it is so difficult for us to access them, there is no demand. But when we produce improved rice varieties, it’s not like this at all! Those varieties can always be sold in bulk, there is a huge market for them, even locally.
As this testimony suggests, despite the surge in the supply of deshiya paddy in 2016 as a direct result of heightened intervention in the agricultural sector, the demand for rice grains both locally and nationally did not increase. 12 Instead, while the price of deshiya paddy purchased from farmers dropped rapidly (from Rs. 70/kg to Rs. 50/kg), niche markets and health food stores continued to capitalize on the therapeutic value of these rice varieties by limiting the supply of milled grains in the market. The difference in revenue captured by farmers and value-added retailers is staggering (see Figure 2).
As a consequence, the current market structure for deshiya rice varieties produces key material and temporal constraints that limit the uptake and expansion of indigenous agriculture in areas where kidney disease is endemic. Consider the following testimony by Suneth, a male farmer from Sri Pura who experimented with deshiya cultivation in 2016 at great cost: When we were cultivating suwandel [a popular deshiya rice variety], we had to wait for the monk to mill it, sell the milled rice, receive money and they pay us. We can only sell it slowly, bit by bit. So, then you don’t get all the money you need in one go. But for us this is untenable, we have no idea when and if we will get paid. For some farmers, it is possible to do this because they have connections in Colombo or can mill their own paddy. But we can’t wait. We can’t have our income tied up like that. We need to get paid within a week of the harvest, that is how tight our budgets are.
Because of these temporal delays, only some residents have been able to profitably navigate markets for deshiya rice varieties. As Jayathilke, a relatively wealthy farmer, who also owns a small mill explained: “The difference between myself and most farmers is that I can store my harvest. Because of this I can process and sell [milled grains] bit by bit as prices rise and demand emerges.” Similarly, my survey data reveals that the farmers who have been able to sustain and increase profits from cultivating deshiya rice varieties own machinery or have other capital assets. This means that they are not forced to take out as many loans to cover labor costs and machine hire during the cultivation season. As a consequence, they feel less pressure to sell their harvest immediately and en-masse to recover cultivation-related debts. In fact, my data indicate that in an area where livelihood options are severely limited, deshiya cultivation has provided some farmers with new opportunities to increase their incomes. Through profitable experimentation with deshiya rice varieties, several wealthy farmers were, for instance, able to invest in more machinery or in developing small-scale milling capacity which in turn, increased the rates of profit they could generate from this type of farming.
But for most farmers in Padaviya and Sri Pura these types of profits were out of reach. Instead, more than 70% of households reported debts that curtail their ability to wait for higher prices for their harvests (whether deshiya or conventional). Instead, they are bound by debt to sell in bulk at harvest time, when supply is highest, and prices are lowest. The problem, which was explained to me time and again, is not only that most farmers in Padaviya and Sri Pura cannot afford to wait, but that the very act of waiting causes new losses that erode residents’ ability to reproduce their livelihood. Among many of my interlocutors, indigenous rice cultivation has produced significant losses in both yield and income. As Jayantha, a third-generation rice farmer from Padaviya explained: Most farmers are only able to cultivate by raising debts, they must borrow money to farm and then face immediate pressure to recover those debts. So almost as soon as the paddy is harvested, their creditors are waiting for their payment. In many cases, farmers who cultivated deshiya varieties ended up selling their harvest for a low price and couldn’t generate enough income to break even. Despite all the hype about price premiums in the market, the actual income they generated was reduced relative to cultivating improved varieties with chemical inputs. The government only purchased about Rs. 5000–6000 kg of paddy at Rs. 70/kg…So then what happened is that other private buyers came to area and were only willing to buy the rest for low prices, like Rs. 50/kg, sometimes lower. Because of that experience many farmers switched back to improved varieties and chemical inputs the next season… We can’t sustain ourselves by cultivating 100% deshiya.
The critical point is that the current market structure for deshiya rice varieties create distinct socio-spatial patterns of value and loss that compound class-specific vulnerabilities. Put differently, health improvement strategies that target the agricultural sector have thus become a force of further socioeconomic differentiation among dry zone farmers. Moreover, bitter experiences of loss have led many farmers to return en masse to chemically dependent agriculture, thereby reinforcing patterns of chemical risk among many economically disadvantaged farmers.
Chemically dependent agrarian ecologies
While deshiya rice cultivation concentrates value in high-class and urban centers, it also creates new patterns of “environmental advantage” 13 that accrue to resource-rich farmers. Critically, my interviews reveal that farmers with access to machinery and capital can take up deshiya cultivation because they can absorb the yield losses that result from transitioning away from chemically dependent production systems. In essence, they have the ability to wait two to three seasons for the biological structure of the soil to regenerate itself and are able to translate this transformation into an environmental advantage to maximize yield, rents, and profits. Through discussions with farmers and activists, I learned that, on average, it takes about three seasons to cultivate deshiya rice varieties without significant yield losses (this is on top of the natural yield difference that exists between deshiya and high-yielding seeds). As an activist attached to a local NGO explained, it can take up to “10 seasons of continuous deshiya cultivation” to really rehabilitate the fertility of the soil: “The impact is gradual, you don’t see an immediate impact. Generating microorganism numbers in the soil takes time. It is not instant. But once the fertility has increased, you only need to do some minor additions to help boost plant growth [leaves, hay, organic fertilizers] and a lot of farmers who work with us have seen their yields steadily increase,” and their costs of production steadily decrease.
Specifically, my survey data indicate that farmers who can absorb short-term losses (in terms of yield and income) and translate them into long terms gains (in terms of increased soil health, reduced costs of production, and access to niche markets) capture more value from deshiya cultivation than their peers. By making this switch, these farmers are also able to reduce their rates of agrochemical exposure (at least in their production process) and therefore, potentially, capture greater health benefits. Yet, as the testimonies above indicate, farmers in Padaviya and Sri Pura have very different abilities to wait and critically, to absorb the costs of waiting which are necessary to capture the price premiums and environmental advantages of deshiya and organic cultivation. Instead, experimentation with deshiya rice varieties produces new legacies of economic loss for many farmers because of uncertain and ephemeral markets, natural yield differences between improved and deshiya varietals, and low soil fertility. As a consequence, the temporal and ecological constraints of deshiya cultivation, together with the unequal abilities to absorb the losses of deshiya cultivation in the short term, will likely continue to drive patterns of socio-ecological differentiation in the area. These interlocking processes shed light on how environmental difference, socioeconomic differentiation, and differentiated health possibilities are dialectically produced through the work of Vasa Visa Nethi Ratak and other actors promoting a return to native seed.
Who derives the health benefits of deshiya rice cultivation? Who is this movement for?
To elaborate the benefits of an intersectional approach further, I examine how health improvement schemes in the dry zone are refracted by agrarian class relations and in particular, the historical production of an especially precarious class of sharecroppers. Among Padaviya and Sri Pura’s farming households, almost 25% are functionally landless, having no cultivable paddy land of their own (Padaviya Divisional Secretariat, 2015; Sri Pura Divisional Secretariat, 2015). This heterogeneity in tenure status is crucial to not only understanding the haphazard and uneven processes of agrarian change in the area, but also uneven patterns of exposure to, and intensities of, chemical use.
In the late colonial and early independence periods, the Sri Lankan state made multiple attempts to populate the dry zone with landless Sinhala farmers (Brohier, 1955; Peebles, 2006; Senanayake, 1935). Padaviya and Sri Pura are two outcomes of this process and as such ownership of paddy lands is largely tied to residents’ settlement histories. From the late 1950s, waves of official settlers were given land allocations of between 2-3 acres of paddy and 1-2 acres of “highland” (for their homesteads and upland cultivation). Presently, the land under paddy cultivation includes 14,000 acres of official plots and 2500 acres of “encroached” lands, usually by second- or third-generation settlers. 14 In Padaviya and Sri Pura encroached lands are classified as illegal occupations within government discourse and are often cultivated by second- or third-generation settlers who do not have legal ownership over their paddy lands and/or homestead plots (in some cases deeds have been granted post-facto, often many years after the land was originally occupied. In other cases, residents continue to occupy lands illegally). The elevation of Padaviya wewa (reservoir) has also produced a natural cap on irrigated paddy lands in these schemes. As the Senior Irrigation Engineer for the scheme explained during one of our conversations, “all of the possible lands that can be irrigated is already under paddy cultivation.” Beyond this extent, it is not possible to access the reservoir’s water supply (because of the difference in elevation). Moreover, the lands distributed under these settlement schemes are also governed by anti-fragmentation clauses (a three-acre plot of paddy land can only be legally subdivided once, and therefore, officially, the minimum size of land holdings is 1.5 acres). 15 Because of these factors, within Padaviya and Sri Pura there currently exists a scarcity of paddy lands. Under these conditions, villagers who do not own land cultivate other peoples’ fields, and in exchange pay an agreed portion of the harvest as rent. In Sri Lanka, this system of sharecropping is called a “paddy lease,” where the landless farmer has to provide a pre-agreed share of the harvest, irrespective of the final yield. In my household survey, 28% of farmers leased lands under this system the last time that they cultivated.
How do these tenure patterns restrict the spatial and social reach of health improvement schemes that target rice cultivation practices and promote indigenous and organic production? The temporal and material constraints of switching to deshiya and organic cultivation discussed above are heightened in these cases because tenant farmers only have short-term access to the land, and they have little to no incentive to bear the losses that accompany regenerating paddy soils. Even if they were to make these shifts, the environmental advantages of doing so would accrue to the owner or other farmers cultivating the land at least three seasons later. Also, because a portion of their harvest must be paid as rent, these farmers have more pressure to maximize yield and are therefore unlikely to take up deshiya cultivation because of its relatively low yields (compared to High Yielding Varieties). Consider, for example, the following statistics from my survey data which reflect key differences among farmers in the area. Among the tenant farmers that I surveyed only 24% had experimented with deshiya rice varieties or organics at some point during the past 5 years (compared to 42% across all survey respondents). Of these tenant farmers, 46% only planted native seeds on a small portion of their rice fields and 23% sustained significant losses because of this experimentation. Critically, for tenant farmers, the margin for risk is very narrow, and their ability to absorb losses is much less than many land-owning farmers. Moreover, and as has been shown in other contexts (Nyantakyi-Frimpong et al., 2016), insecure land tenure and land use rights are often correlated with chemical dependence because of the ability of agrochemicals to speed up and shorten cropping cycles as well as to maximize yield. Residents point to the compulsion to use agrochemicals due to the constrained timeframes in which they cultivate, as well as the need to produce large harvests to pay rents. Moreover, in my sample, 42% of tenant farmers also worked as seasonal wage laborers and participated in land preparation for other plots, which involves weedicide and fertilizer application. The programs implemented by Vasa Visa Nethi Ratak and other actors promoting indigenous seeds are thus layered onto these agrarian class relations and chemically dependent ecologies. The relatively low rates of experimentation with deshiya varieties among tenant farmers reveals how attempts to repatriate native seeds intersect with pre-existing patterns of social and environmental difference to (re) produce precarious livelihoods and differential possibilities for health. Stated simply, these interventions in the agricultural sector both respond to and for some residents reinforce exposures to health risks. A key finding of my work is that abilities to adopt new “healthful” practices of resource use and capture the potential health benefits of deshiya cultivation are refracted through agrarian class relations and chemically dependent ecologies, at the same time that interventions create new patterns of ecological advantage and accumulation of economic value and health dividends.
More broadly, key geographic differences also intersect with agrarian class relations to concentrate the economic and health benefits of deshiya consumption in higher classes and urban centers. As my interviews with distributors in deshiya markets suggest, the consumption of deshiya rice varieties increasingly confers status and re-inscribes class and regional hierarchies. As one activist argued: Eating deshiya varieties is now a hobby for many elite households in Sri Lanka. It is something done for show. These varieties are often tied to ancient traditions, a glorious past [linked to the dry zone’s ancient agrarian civilizations], these are things that appeal to people. So now there is some prestige in having these traditional artifacts or heirlooms on your dinner table…. In the very elite houses of Colombo sometimes you see them using bunches of deshiya paddy as part of decorating schemes. There is pride in that. But they don’t want to store gunny sacks of paddy in their mansions. Many of them probably don’t even eat rice everyday anymore. They only bought paddy from us for 50 rupees /kg. Then after milling, they sold our rice for 200 rupees per kilo! In some hospitals, a 35gm packet of indigenous rice is sold for 120 rupees. This rice is also distributed to the very best schools in Colombo, for the children there. But what do our children get? Isn’t this rice also for them?
This paradox was not lost on other residents in Padaviya and Sri Pura. As another of my interlocutors observed: I question the whole idea of a separate market for deshiya varieties. Actually, it is really unfair: when you have a separate market, the rice can only be consumed by people who have a lot of money [in areas like Colombo, deshiya rice products are sold at very high prices such as Rs. 200–250/kg]…. But these aren’t the areas where you have high rates of kidney disease! Also, doesn’t a poor man’s child have as much right to eat this rice?
As one of my interlocutors explained: “People don’t eat deshiya. Even if they sell their harvest for Rs. 60, they consume what they have always consumed [i.e. improved varieties]. If they can sell their deshiya harvest for upwards of Rs. 60, they are likely to sell their entire crop and then purchase hybrid varieties for Rs. 50 or less. It is not cost-effective to consume deshiya varieties if you are a producer.” Together, these quotes point to the contradictory mandates that have come to animate health improvement strategies that promote indigenous and toxic-free agriculture. Is their purpose to boost consumption of indigenous varieties outside of the dry zone or is it to promote healthful production and consumption within it? Can these mandates be reconciled in current markets for deshiya rice which marginalizes farmers’ fields as a site of profit? Or are they, as some of my interlocutors argue, fundamentally contradictory? By recognizing intersecting regional and class disparities, it is possible to explain why the speculated health dividends and environmental advantages of deshiya rice cultivation are spatially and socially concentrated in high classes and metropolitan centers. Despite the stated goals of these health improvement strategies, for the majority of residents in Padaviya and Sri Pura, experiences of deshiya and toxic-free cultivation fall woefully short in terms of promised health, as well as environmental and economic benefits.
Conclusion
This article demonstrates that the concept of intersectionality has much to offer political ecologies of health. By drawing attention to overlapping, compounding, and sometimes mutually reinforcing differences, an intersectional framework provides insights into how health inequalities are at once “constantly shifting and open to reinterpretation,” but also, often difficult to transcend. Specifically, I draw on two case examples to illustrate how residents’ abilities to derive health dividends from increased access to filtered water or native seed are mediated and crosscut by multiple axes of socioecological difference, such as health status, gender, class, geographical location, soil fertility, groundwater quality and pest pressures. My findings suggest that “successful” adoption of “healthful” consumption/production practices is not simply a matter of increased access and/or awareness—although both are important. Instead, the uneven uptake of filtered water and indigenous seed among residents is underwritten by multiple and intersecting relations of power that complicate their everyday health practices, and at times, place such practices out of reach. Indeed, as the testimonies presented above demonstrate, pre-existing differences matter to the constitution of health improvement schemes and crucially, the differences that matter are not just socio-economic, but also ecological and embodied.
At the same time, reading across these case examples also brings to light the inter-dependent and recursive processes of social, bodily, and ecological differentiation that emerge through health intervention in the dry zone. In this analysis, I illustrate how these schemes unfold in ways that simultaneously produce: differentiated costs, in terms of household labor burdens and finances; patterns of ecological difference via forms of contamination and environmental advantage/health; as well as novel social relationships because the ability to respond to anxieties about water safety and new geographies of agrarian production confers status and gendered class relations that increasingly help to distinguish dry zone residents from each other.
By means of these case examples, the article thus makes visible the ways that health improvement schemes produce new and differentiated harms in the form of intensified labor burdens for poor women, and intensified agrochemical use for ecologically and economically vulnerable farmers. In both cases, intervention has created dynamics that confer possibilities for healing to some residents while locking others into feedback cycles which either create new labor-related health problems or reproduce exposures to chemical risk. By doing so, this work zooms in on the tension between the stated goals of health improvement schemes and their uneven and frequently paradoxical effects. It is around these tensions that the distinctions between what harms and what heals are destabilized and the meaning of health, and who it is for, are transformed. Through this analysis, the article extends existing frameworks in political ecologies of health, arguing that the analytic of intersectionality helps to more fully explain how and why schemes designed to improve health through environmental transformation simultaneously produce harm and sickness.
Ultimately, efforts to produce and promote health in kidney disease hotspots (and beyond) need to take seriously uneven capabilities to adopt or maintain healthy consumption and cultivation practices, if they are serious about enacting health justice and equity. Dry zone residents are not a homogeneous group that is uniformly affected by environmental risk, they do not have similar capabilities to adopt new “healthful” consumption behaviors. Instead, health improvement schemes both unfold within, and actively produce, uneven socio-ecological landscapes. As a result, proponents of health improvement intervention could benefit from asking how residents – and their diverse, embodied, and experiential knowledge of health struggles—could shape policymaking about health improvement. This would reverse the tendency to overdetermine conceptualizations of health in ways that mask the messy, conflicting, and uneven effects of intervention. Without incorporating more diverse understandings of health, these kinds of interventions will continue to compound existing vulnerabilities and unleash new processes of differentiation that ultimately undermine their quest to enact health in the shadow of CKDu.
Highlights
Schemes to promote kidney health in dry zone Sri Lanka set in motion interdependent and recursive processes of social, ecological, and bodily differentiation that rework the distinctions between what harms and what heals, as well as who is harmed and healed.
The burden of subsidizing new “healthful” practices of water provision and agricultural production is unevenly experienced, as are residents’ abilities to adopt and maintain them over time and space.
Schemes designed to heal turn on the production of differentiated harms, including new gendered labor burdens for poor women, and intensified agrochemical use for ecologically and economically resource-poor farmers.
I demonstrate the importance of intersectional approaches to more explicitly feminist political ecologies of health.
Footnotes
Acknowledgments
The thoughtful and constructive comments of three anonymous reviewers greatly improved the focus and clarity of the manuscript. Earlier versions of this manuscript were also improved by careful and generous reads by Brian King, Aparna Parikh, and A. Marie Ranjbar. I also wish to thank Lyla Mehta for her editorial guidance during the revision of the paper. Most of all I am indebted to my participants for their time, insights, and stories.
Declaration of conflicting interests
The article is based on my original work and has not been submitted for publication elsewhere. I have no conflicts of interest to disclose.
Funding
This work was supported by the Social Science Research Council and the American Institute for Sri Lankan Studies, the Society of Woman Geographers, and the National Science Foundation (Award No. 1633991).