
Abstract
Objective
To find out the determinants of patient safety culture among healthcare providers in the Upper East Region of Ghana.
Design
This was a cross-sectional survey of three hospitals. The Hospital Survey on Patient Safety Culture questionnaire was adapted for data collection.
Setting
The setting was three selected hospitals (mission, public, and private) from the Upper East Region of Ghana.
Participants
A total of 393 healthcare providers were invited to participate, but 384 (98%) honored the invitation.
Results
It was found that only 7% of the respondents thought that overall patient safety culture was excellent, while close to 14% of the respondents thought that overall patient safety culture was poor. The significant predictors of overall patient safety culture were teamwork across units (β = 126, p = .04), organizational learning (β = .112, p = .05), and management support for patient safety (β = .172, p = .00).
Conclusions
Generally, patient safety culture in the selected hospitals was below expectation. In the quest to promote a culture of safety, healthcare managers of the hospitals must invest resources in promoting teamwork, organizational learning, and management support among other factors.
Introduction
Adverse event poses a threat to patient safety and is gaining attention worldwide.1,2 Adverse events are “unintended injuries or complications that are caused by health care management rather than by the patient’s underlying disease and can lead to death, disability at the time of discharge and prolonged hospital stay.”3,4 Adverse events kill more people than motor-accident, breast cancer, and acquired immune deficiency syndrome. 5
A positive patient safety culture has been found to be a viable tool that can help reduce the occurrence of adverse events in healthcare facilities.6,7 Patient safety culture is the set of shared values, attitudes, perceptions, beliefs, and behaviors that support safe practices among individuals in healthcare organizations. Promoting safety culture among healthcare providers has enormous benefits, such as increasing provider and patient satisfaction with care. 8
In Ghana, patient safety culture is an emerging area. However, adverse events and concerns about safety have existed,9–11 only recently has research started to address patient safety culture in Ghana and only for a few adverse events.12–14 Since promoting a culture of safety across the care continuum is a key to reducing the occurrence of adverse events, there is an urgent and compelling need to find out the factors that influence patient safety culture in Ghana’s hospitals. Understanding the factors can inform patient safety interventions and policies. To fill this gap in knowledge, the main objective of this study was to identify the salient factors that influence patient safety culture among healthcare providers in the Upper East Region of Ghana.
Methods and materials
The study was a cross-sectional survey of three hospitals in the Bawku enclave. 15 Bawku is in the Upper East Region of Ghana, one of the most deprived regions in the country. For instance, the region has the lowest doctor–population ratio (1:25,878) coupled with inadequate healthcare facilities. According to the 2010 Population and Housing Census, Bawku has a total population of 322,575 representing 19.6% (1,046,545) of the total population of the Upper East Region. 16 The area has three hospitals comprising of a mission hospital, a public hospital, and a private hospital. In addition, the study area has health centers, clinics, and community-based health planning and services that augment the hospitals in the delivery of healthcare. The mission hospital has a bed capacity of 388 and a staff strength of 304. The private hospital has a bed capacity of 80 with a staff of 97, and the public hospital has a bed capacity of 110 and a staff strength of 224. The total staff capacity of the three hospitals adds up to 625 healthcare providers.
Using a population of 625 healthcare providers and a design effect of 1.5 and an outcome of 50%, the sample size was 393 (see Appendix 1). Based on the staff strength of the hospitals, a ratio of 3:2:1 was used to recruit respondents from the mission, public, and private hospitals respectively. The three hospitals were purposely selected since they are the only hospitals in the study area. Respondents were recruited using convenience sampling technique. This technique was appropriate because of the rotation and shift system operated by the hospitals.
The English version of Hospital Survey on Patient Safety Culture (HSOPSC) questionnaire, developed by the Agency of Health Research and Quality (AHRQ) was adapted for data collection. 17 The questionnaire has a Cronbach alpha ranging from 0.63 to 0.84 18 and has been either adopted or adapted worldwide to assess patient safety culture.17,19 The HSOPSC tool is a 42-item structured questionnaire, excluding socio-demographic variables.
Ten dimensions of the HSOPSC questionnaire that are more applicable to the context of the study were adopted to assess healthcare providers’ perceptions of patient safety culture. The dimensions include teamwork within units (four items), supervisor expectations and actions promoting patient safety (four items), organizational learning–continuous improvement (three items), management support for patient safety (three items), feedback and communication about error (three items), communication openness (three items), teamwork across unit (four items), staffing (four items), handoffs and transitions (four items), and non-punitive response to error (three items). The items were a five-point Likert scale ranging from “1= strongly disagree” to “5= strongly agree” or “1 = never” to “5= always.”
In addition, the HSOPSC questionnaire has an item that requires respondents to rate their overall perception of patient safety culture (dependent variable) on a five-point Likert scale (A= excellent, B= very good, C= acceptable, D= poor, E= failing). The last section of the questionnaire comprised socio-demographic variables such as age, gender among others.
The questionnaire was administered by hand to 393 healthcare providers on duty and a period agreed upon for pick-up (three to four days). This was because of the busy schedule of the respondents. Data collection was done in February and March 2018. The study received approval by the University of Ghana College of Humanities Ethics Committee (ECH 085/17-18). In addition, permission was sought from the management of the hospitals and written consent from the respondents. Healthcare providers who agreed to participate in the study were asked to sign a consent form. Participation was voluntary and participants had the free will to opt-out by not returning the questionnaire.
Retrieved questionnaires were cross-checked for errors and completeness, and entered in Statistical Package for Social Sciences software, version 23. At the univariate level, descriptive statistics were computed using frequencies and percentages. Percentage of positive response rate was computed by adding frequency percentages of strongly agree and agree or always and most of the time (for non-negatively worded items) and strongly disagree and disagree or never and rarely (for negatively worded items). The composite index for each dimension was the average of all positive response rates.
At the bivariate level, Pearson correlation was computed to explore the relationship between patient safety culture dimensions (independent variables) and overall perception of patient safety (dependent variable). In addition, one-way analysis of variance was computed to compare healthcare providers’ perceptions of patient safety culture among the three hospitals. The respondents were categorized into three groups according to hospital type (Group 1: Mission, Group 2: Private, Group 3: Public).
At the multivariate level, multiple linear regression analysis was computed to determine significant predictors of overall perception of patient safety culture (dependent variable). Using the Shapiro–Wilk test, the data were found to be normally distributed. Other assumptions underlying multiple regression such as outliers and multicollinearity were all satisfied. 20 Prior to computing the multiple linear regression, items under each independent variable (i.e. teamwork within units) were computed to generate a single composite index. At the multivariate level, all negatively worded items were reversed or recoded. Independent variables were used as linear predictors. For the dependent variable, numerical scores were created from the five-point Likert scale (A =5, B =4, C= 3, D= 2, E = 1). 21 Multiple linear regression analysis was computed by using overall perception of patient safety culture as the dependent variable and patient safety culture dimensions as independent variables controlling for socio-demographic variables such as age. All analyses were conducted at the 95% confidence level.
Results
This study recorded a response rate of 98%. Of the 384 respondents representing 100%, 56% were females, 73% were diploma holders, and 58% were married. Exactly, 53% of the respondents were young adults, 82% had less than six years of working experience in their current hospital, and 51% were nurses. Exactly, 50% of the respondents indicated that they work between 40 and 50 h/week (see Table 1).
Socio-demographic characteristics of respondents.

Note: Others (pharmacist, laboratory technicians, physician assistants, patient care assistants).
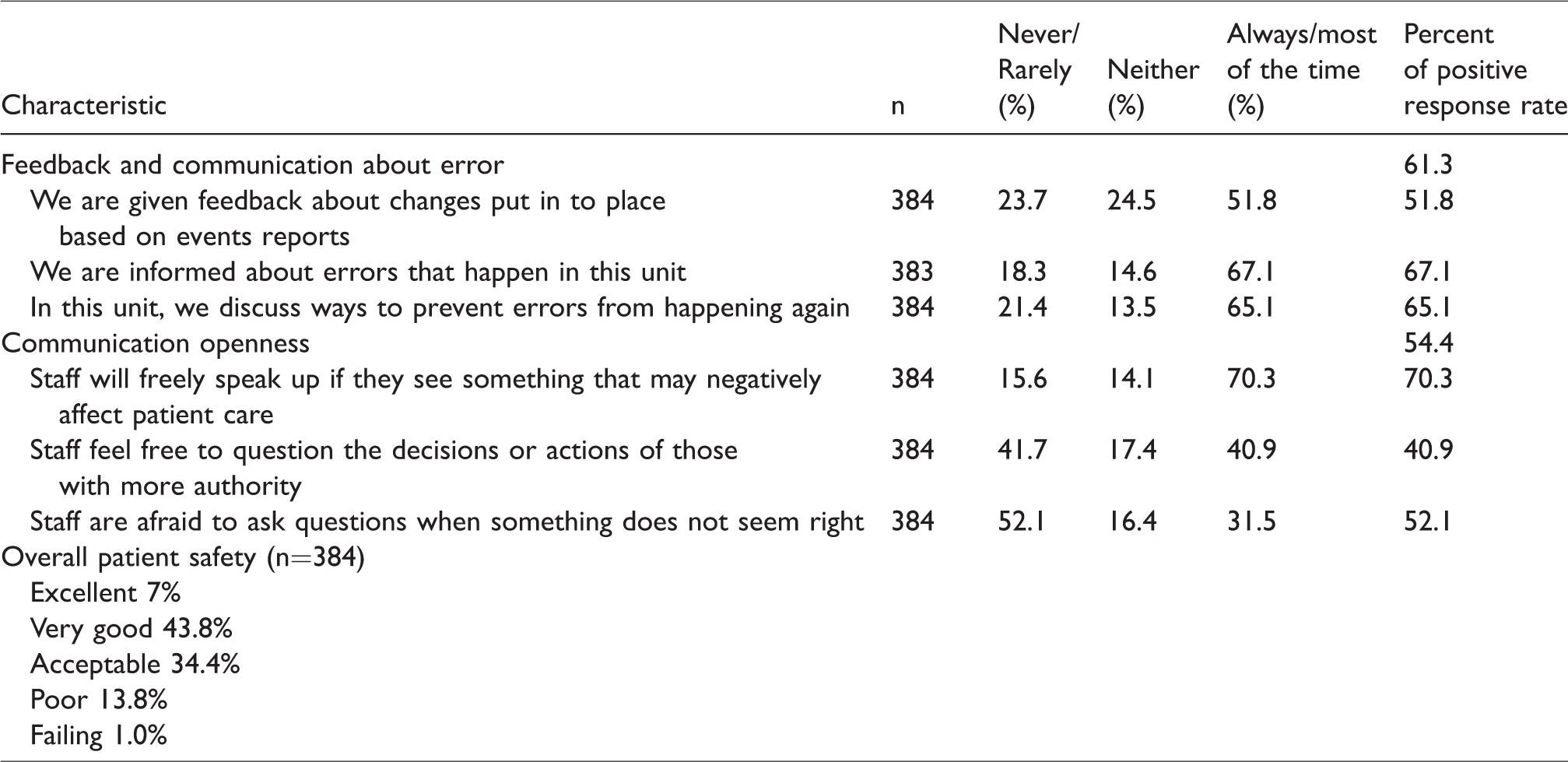
It was found that of the 10 patient safety culture dimensions, 3 dimensions recorded relatively high positive response rate, namely teamwork within units, organizational learning, and managers’ expectations and actions promoting patient safety. Regarding teamwork within units, the areas of strength were respect and support for each other. For organizational learning, areas of strength were the evaluation of patient safety interventions and continuous efforts in improving patient safety. Some of the respondents indicated that patient safety was a priority of their managers. Moreover, staff who did their work according to established patient safety procedures were commended by their managers.
The dimensions that recorded relatively low positive response rates were staffing and non-punitive response to error. Regarding staffing, many of the respondents indicated that they work for longer hours than is best for patient safety. Regarding non-punitive response to error, some of the respondents felt that their mistakes were kept in their personnel files or held against them. More than half of the respondents perceived overall patient safety culture to be good (see Tables 2 and 3).
Dimensions of patient safety culture.

Dimensions of patient safety culture (continuation….).
No statistically significant difference in overall perception of patient safety culture was found among the three hospitals: F (2, 381) = 2.155, p = .117. A weak positive significant relationship was found between teamwork within units, managers’ expectations and actions promoting patient safety, organizational learning, feedback and communication about errors, communication openness, handoffs and transitions, and non-punitive response to errors, and overall perception of patient safety culture. A moderate positive relationship was found between management support and teamwork across units and overall perception of patient safety culture. However, none of the socio-demographic variables had a significant association with overall perception of patient safety culture. Details are provided in Table 4.
Pearson correlation matrix between patient safety culture dimensions and overall perception of patient safety culture.

Note: * significant at 95% confidence level. Interpretation of Pearson correlation: .10–.29 =weak relationship; .30–.49 = moderate relationship; .50–1.0= strong relationship. 22
At the multivariate level, it was found that of the 10 dimensions, 3 dimensions (organizational learning (β = .112, p = .047); management support (β = .172, p = .002); and teamwork across units (β = 126, p = .037)) were found to be significant predictors of overall perception of patient safety culture (see Table 5).
Multiple linear regression analysis on predictors of overall patient safety culture.
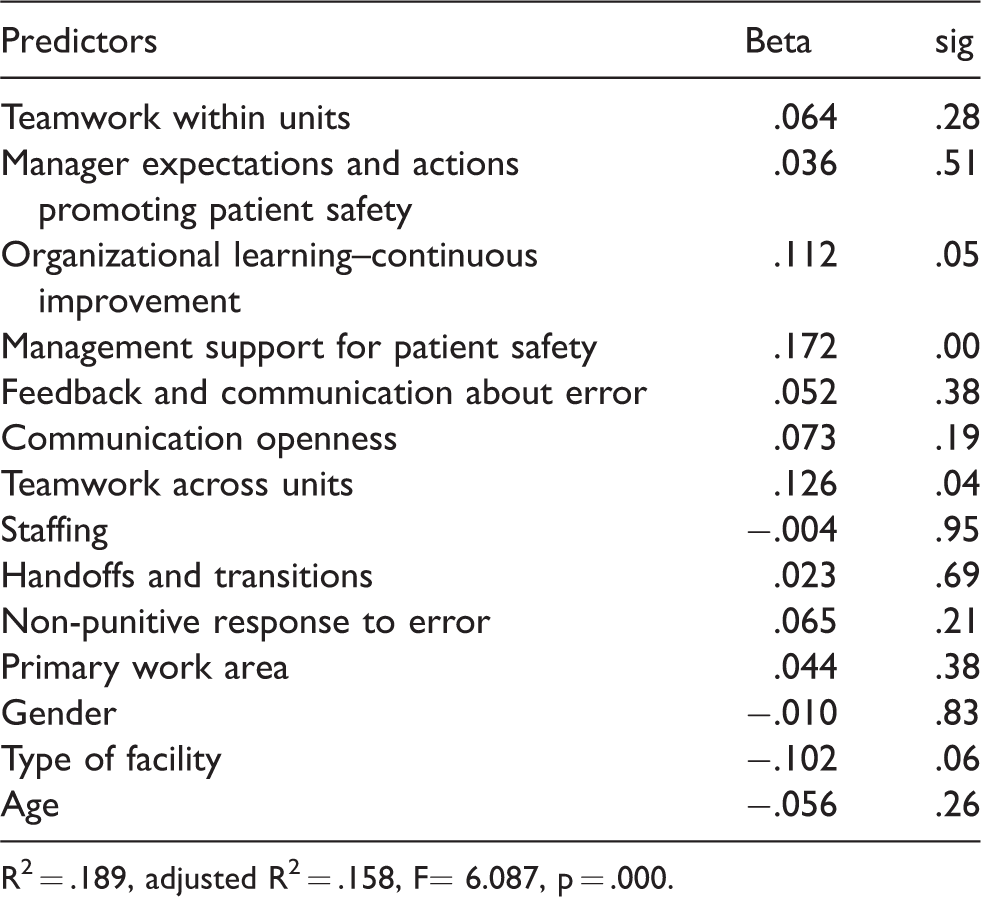
R2 = .189, adjusted R2 = .158, F= 6.087, p = .000.
Discussion
A notable strength of this study is the high response rate (98%). Response rates of studies on patient safety culture using the HSOPSC questionnaire globally are mixed.22–25 Some studies report low response rates ranging from 41 to 60%.23,25,26 On the other hand, some studies report relatively high response rates ranging from 91.9 to 97.7%.22,24,27 This suggests that patient safety culture is a great source of concern in Ghana, where the prevalence of adverse events tends to be high. 9
From the univariate analysis, it was found that of the 10 patient safety culture dimensions, teamwork within units recorded the highest positive response rate (81.5%). This is a bit higher than the average rate of AHRQ (78%). 28 Prior studies using the HSOPSC questionnaire also found teamwork within units recording high positive response rate. For instance, in Iran teamwork within units recorded 65% positive response rate, in Taiwan it recorded a 94% positive response rate, and 76.5% in Nigeria.28–30 This suggests that healthcare providers in the Upper East Region of Ghana support and have respect for each other. The ability of healthcare providers to work effectively as a team contributes positively to patient safety culture. 31
On the other hand, non-punitive response to error recorded the lowest positive response rate. Previous studies have confirmed this finding.21,32,33 The rate in this study is lower than rates recorded by the AHRQ and a study in Taiwan. 28 This suggests that healthcare providers in the Upper East Region felt that their mistakes were held against them or kept in their personnel files. This is a major area of concern and therefore requires urgent attention from the management of the hospitals. To help improve patient safety culture in the hospitals, the managers will have to encourage a “blame-free” culture of error reporting and avoid holding mistakes against healthcare providers. It is important for hospital managers to consider error as a learning opportunity to decrease adverse events and not as personal failure.34,35
In addition, staffing recorded relatively low positive response rate. This finding is supported by previous studies.32,33 For instance, Boussat et al. 36 found staffing to be the most frequently reported failed patient safety culture dimension. This suggests that most of the respondents felt that staff allocation was not adequate to handle patient safety-related workload. Shortage and retention of healthcare providers is a major problem in many developing countries 37 like Ghana. The Upper East Region is one of the deprived regions in terms of healthcare workforce. For instance, it has the lowest doctor–population ratio of 1:25,878. It has been argued that the availability of adequate staff to handle the workload and work hours can improve patient safety in about two to three times. 34 On the hand, inadequate staff causes stress, anxiety, and depression which increases the incidence of adverse event. 38 The shortage of staff may be caused by the unwillingness of health professionals to accept “posting” to the northern parts of the country, partly due to poor conditions of service. To promote patient safety, improving working conditions for healthcare providers, especially those in northern Ghana should be a priority of stakeholders. 39
At the bivariate level, significant positive correlations were found between overall perception of patient safety culture and all patient safety culture dimensions, except staffing. This is confirmed by existing literature. Prior studies found that positive patient safety culture depends on effective communication, procedure compliance, leadership support, non-punitive response to error, and teamwork.37,40 Positive patient safety culture also depends on collaborative learning, replace blame culture, and motivate individuals who identify and report errors.1,41
At the multivariate level, organizational learning, management support for patient safety, and teamwork were found to be significant predictors of overall perception of patient safety culture. This suggests that improving organizational learning, management support, and teamwork across units among healthcare providers in Ghana can lead to an improvement in patient safety. Previous studies can confirm these findings.30,33 For instance, Ginsburg et al. 42 found that creating a “blame-free” environment where healthcare providers can learn from their mistakes can help reduce the occurrence of preventable adverse events and improve safe care in hospitals. Other studies have argued that organizational learning is a critical component of reliably providing safe and high-quality care. Therefore, there is the need to promote an “atmosphere” where healthcare providers can discuss adverse events with management to see the way forward.43,44
Studies have also shown that there is a positive relationship between teamwork and patient safety. For example, Manser 45 found that teamwork played a significant role in the causation and prevention of adverse events. Management support was also essential to patient safety and quality of care improvement. Since managers are in the helm of affairs and see to the day to day operation of hospitals, their role in promoting patient safety cannot be underestimated.
These findings have implications for patient safety improvement. We therefore recommended that the management of the hospitals should invest more resources in promoting organizational learning, teamwork, and management support. In addition, resources should be invested in improving the staff capacity of the hospitals and creating a “blame-free” environment where healthcare providers can freely report adverse events without fear of being punished. Such an environment can promote event reporting and consequently improve patient safety in hospitals.
Conclusion and limitations of the study
This study sought to explore the predictors of patient safety culture in three hospitals in the Upper East Region of Ghana. Teamwork, organizational learning, and management support were found to be significant predictors of patient safety culture. Even though this study provides valuable information for patient safety interventions, it is not devoid of limitations. The self-reporting nature of the HSOPSC questionnaire is prone to bias. In addition, given that the study was limited to the Upper East Region of Ghana, a generalization of the findings must be done with caution.
Footnotes
Acknowledgement
The authors would like to thank the management of Bawku Presbyterian Hospital, Vineyard Hospital, and Bawku West District Hospital for their cooperation during the data collection. We also thank all the healthcare providers who dedicated their precious time to participate in the study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.