
Abstract
Background
Rapid response systems (RRSs) were developed to respond to early warnings of unexpected deterioration, but their effectiveness may be limited by factors impacting RRS activation (afferent limb) or response (efferent limb). Despite decades of RRS implementation, patients still experience unrecognized deterioration with associated worse outcomes.
Methods
This rapid review used modified search strategies to focus on the most valuable studies performed in the United States. Citations were screened by one reviewer with artificial intelligence as a second reviewer at the title/abstract review stage. The full text of eligible articles was then reviewed by a single team member to confirm eligibility. One reviewer completed the data abstraction, and a second reviewer checked the first reviewer's abstraction.
Results
Three categories of interventions were identified: implementation of a new RRS, and modifications to the afferent limb and/or efferent limb of an existing RRS. RRSs may have a large impact in reducing in-hospital mortality and an even greater impact in reducing cardiorespiratory arrest on hospital general wards in adults but the effect is unclear in children. Their impact on unanticipated intensive care unit admission is unclear. Modifications to the afferent and/or efferent limb were associated with a reduction in mortality and the incidence of cardiorespiratory arrest for adults.
Conclusions
RRS may have a large beneficial effect on hospital mortality and in-hospital cardiorespiratory arrest, but the strength of the evidence is low due to methodological weaknesses of the studies. Innovations in afferent and efferent limb structures show promise for increased benefit.
Introduction
Failure to rescue is failure or delay in recognizing and responding to a hospitalized patient's unexpected deterioration. In patients on general hospital wards, unexpected deterioration may result in cardiorespiratory arrest (CA) or other life-threatening complications. 1 These events may be heralded by premonitory signs and symptoms that create opportunities to recognize the deterioration in a timely manner, intervene to stabilize the patient, and halt the deterioration.2–11 Rapid response systems (RRSs) were developed to respond to early warnings of unexpected deterioration,12–18 but their effectiveness may be limited by factors impacting RRS activation or response.12,19–21
Activation criteria were generated from studies defining premonitory signs and symptoms of CA.2–11 General ward staff were educated on the importance of early recognition of clinical deterioration, and how to activate the response team if and when patients met activation criteria (i.e. the afferent limb of rapid response). The response team (i.e. the efferent limb) would then rapidly come to the patient's bedside to assess, intervene if necessary, and potentially triage patients to a higher level of care. Despite decades of implementation of RRSs, patients still experience unrecognized deterioration on general hospital wards and RRS activation is often delayed or does not occur. The previous Making Healthcare Safer III report found moderate evidence that RRSs are effective in reducing CA but inconclusive evidence for their effect on hospital mortality and intensive care unit (ICU) transfers. 3 That report also found that partial or complete failures of the afferent and efferent limbs impact the effectiveness of RRSs.
We report here the findings of the Making Healthcare Safer IV rapid review of the recent literature on the overall effectiveness of RRSs and effectiveness of efforts to optimize the afferent and efferent limbs of RRSs.
Methods
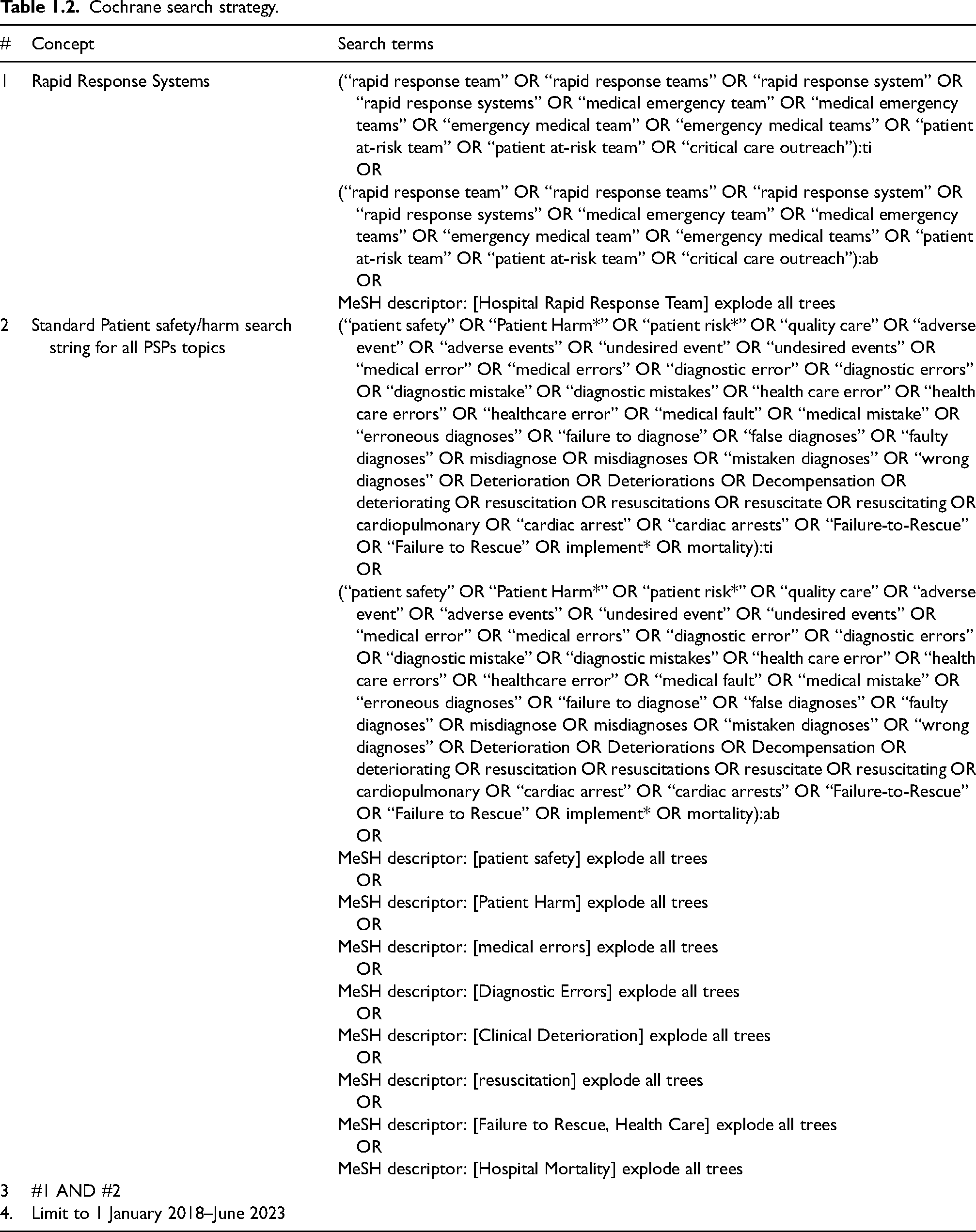
For this rapid review, strategic adjustments were made to streamline traditional systematic review processes as proposed by the Agency for Healthcare Research and Quality (AHRQ) Evidence-based Practice Center (EPC) Program. 22 The protocol for this rapid review is posted on the AHRQ website. 23 Adjustments included highly specific questions, modifying search strategies to focus on the most valuable studies, restricting the search to studies published in English and performed in the United States, and limiting the databases searched (PubMed and Cochrane supplemented by a narrowly focused grey literature search). The search strategy is presented in Table 1. We searched for systematic reviews and primary research studies. The title and abstract of each citation were screened by a team member based on predefined eligibility criteria (Table 2), and then the AI Classifier Manager feature of DistillerSR served as a second reviewer of each citation at the title and abstract review stage. The full text of each remaining potentially eligible article was reviewed by a single team member to confirm eligibility. A second team member checked a 10% sample of the full text reviews to verify that important studies were not excluded. Details of these methods are in the final report. 24
Search strategies for published literature.

Cochrane search strategy.
Inclusion and exclusion criteria.
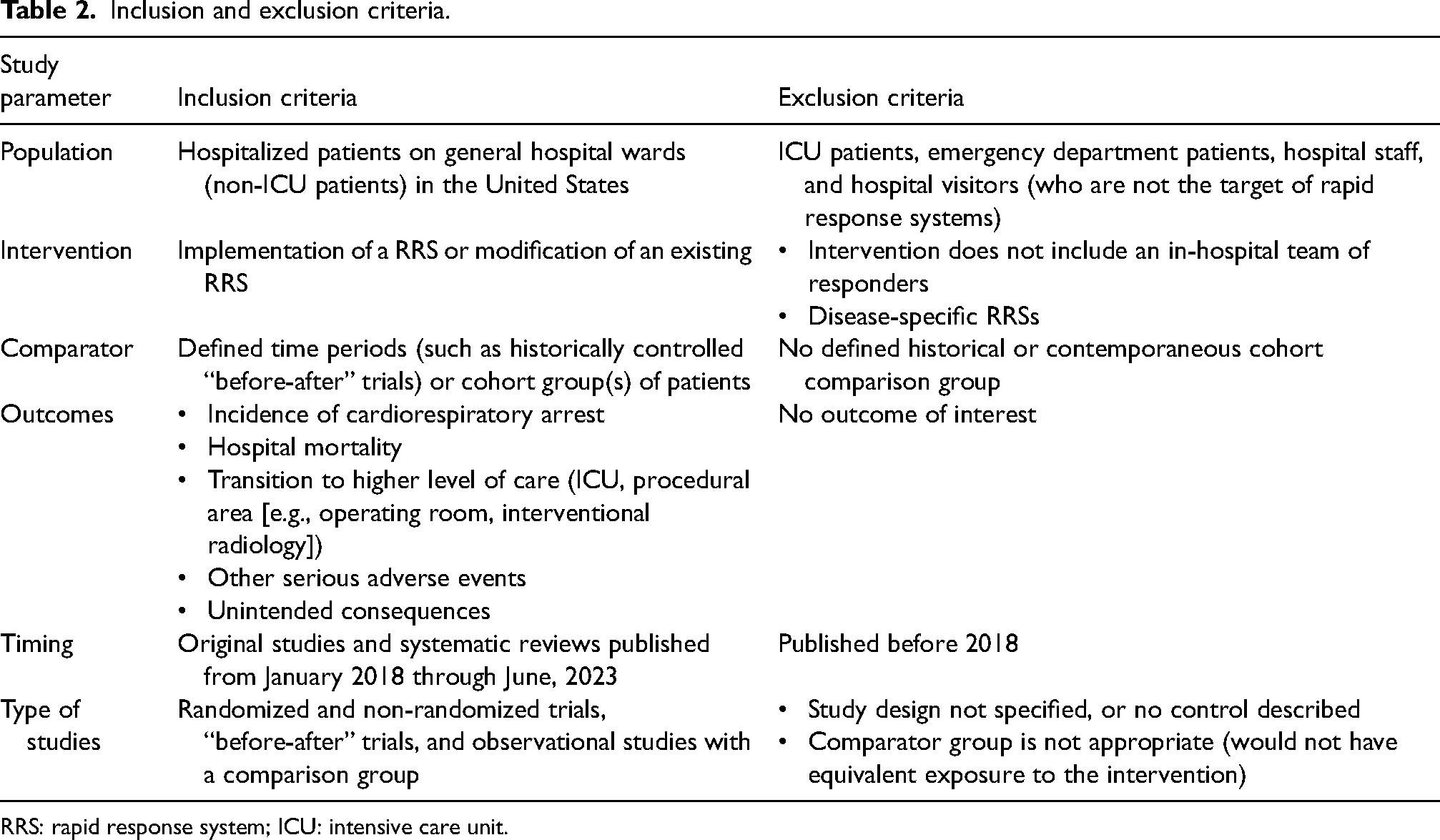
RRS: rapid response system; ICU: intensive care unit.
Reviewers extracted information and organized it according to the review questions and included author, year, study design, frequency and severity of the harms, measures of harm, characteristics of the RRS, outcomes, implementation barriers and facilitators, resources needed for implementation, and any description of toolkits used for implementation. One reviewer completed the data abstraction, and a second reviewer checked the first reviewer's abstraction for completeness and accuracy.
For primary studies, we used the ROBINS-I tool for assessing the Risk of Bias in Non-randomized Studies (all included studies were non-randomized). Our risk of bias assessments focused on the main outcome of interest in each study. 25 For included systematic reviews, the primary reviewer used the criteria developed by the United States Preventive Services Task Force Methods Workgroup for assessing the quality of systematic reviews. 26 We graded the strength of evidence (SOE) for systematic reviews using the methods outlined in the AHRQ Effective Health Care Program Methods Guide for Effectiveness and Comparative Effectiveness Reviews (Table 3). 27
Strength of evidence for each outcome by intervention and population.
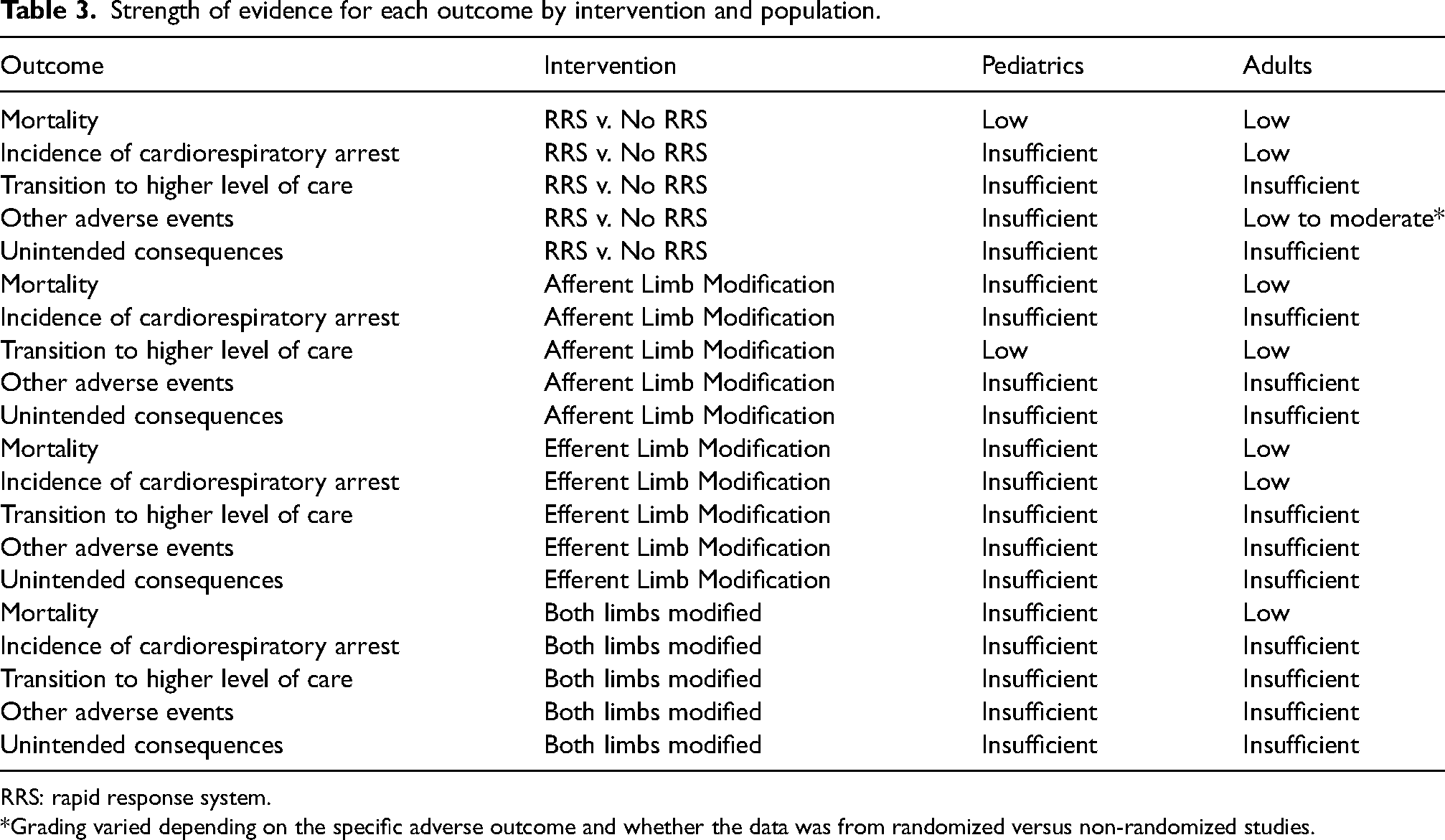
RRS: rapid response system.
*Grading varied depending on the specific adverse outcome and whether the data was from randomized versus non-randomized studies.
Results
We found 23 studies (4 systematic reviews28–31 and 19 primary studies)32–50 that met our eligibility criteria (Figure 1). Eleven studies compared outcomes with and without an RRS. One study examined the unintended consequences of the most common RRS staffing model that relies on critical care providers being the efferent limb. Ten studies compared outcomes after implementing changes to the afferent limb and six studies examined outcomes after implementing changes to the efferent limb. Two studies implemented changes to both the afferent and efferent limb. Results, in terms of the impact on outcomes, are provided in Table 4, and Table 5 outlines which studies examined which outcomes.
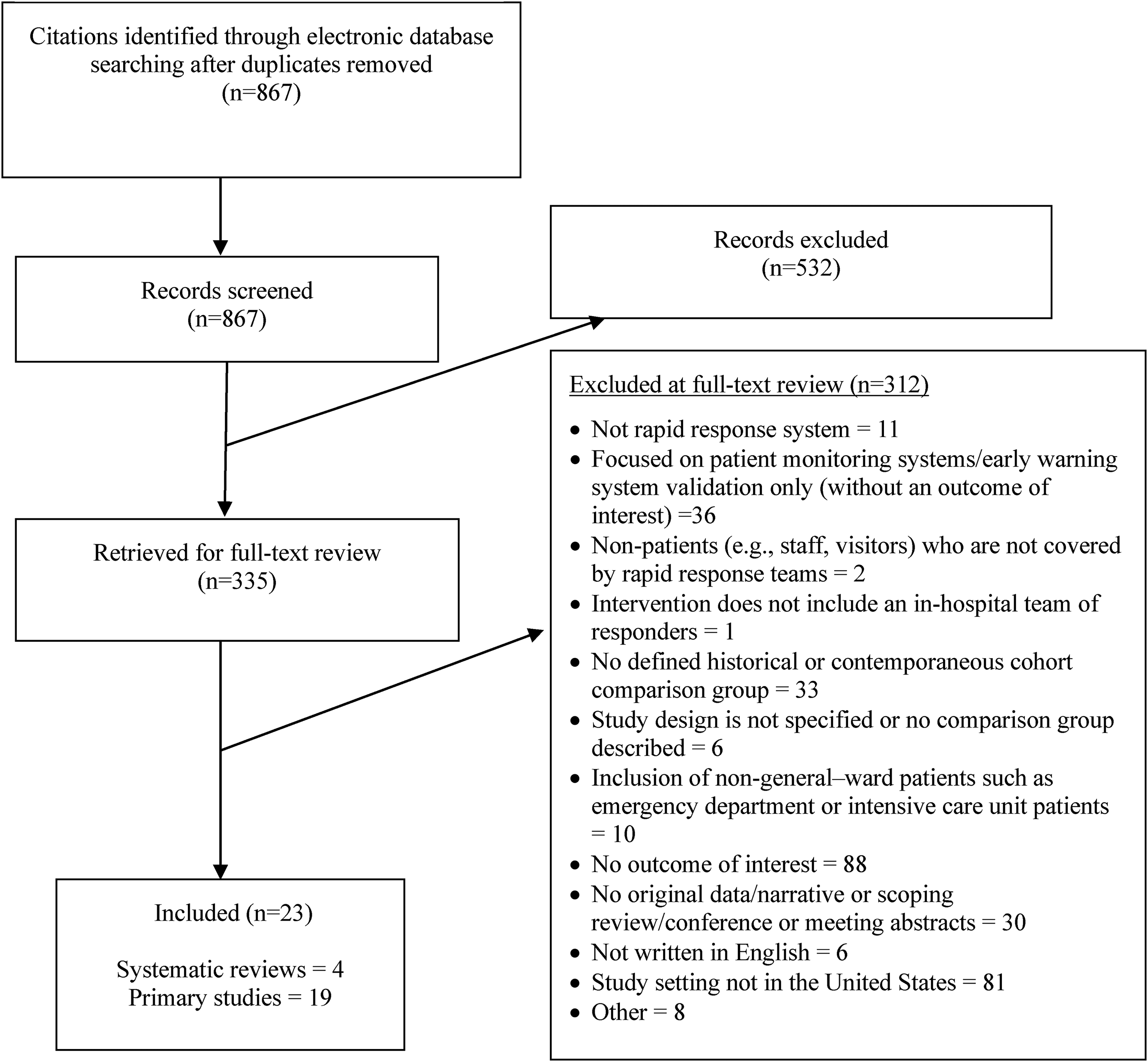
Results of the search and screening.
List of included studies by outcome.
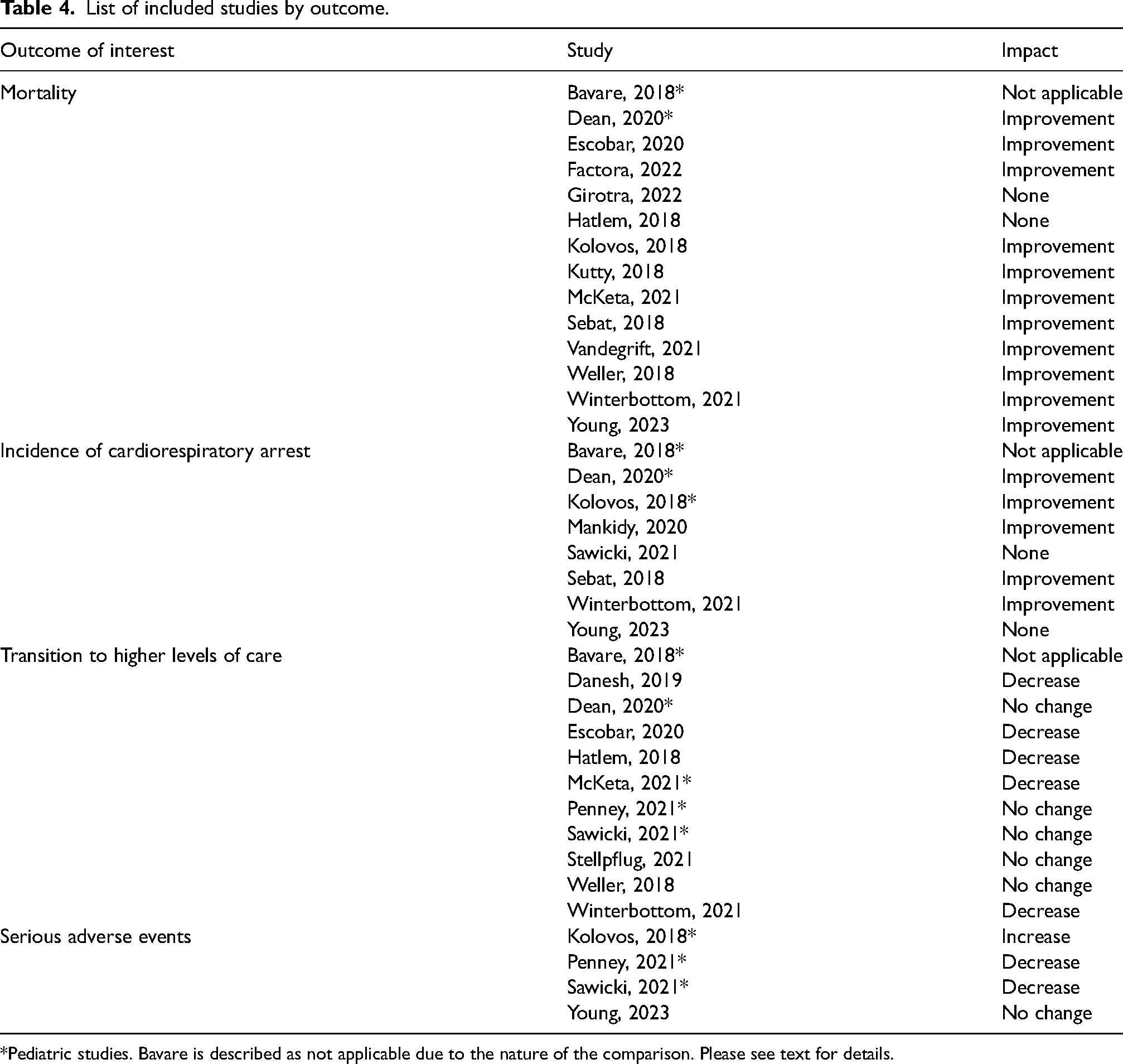
*Pediatric studies. Bavare is described as not applicable due to the nature of the comparison. Please see text for details.
List of included studies by outcomes examined.
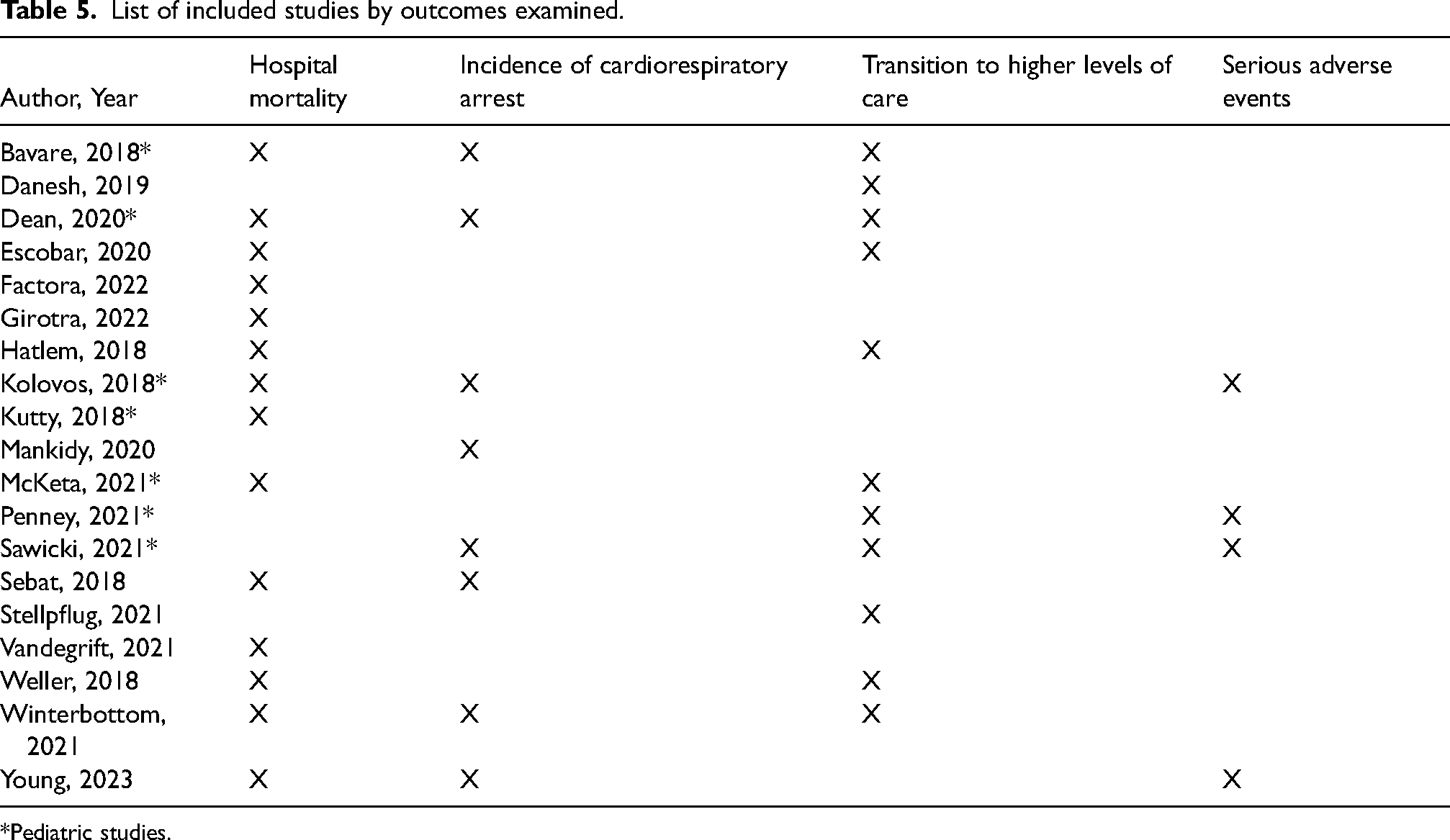
*Pediatric studies.
Impact of an RRS versus no RRS: Hospital mortality
We identified four systematic reviews28–31 comparing outcomes with and without an RRS. All primary studies examining this outcome with and without an RRS used a pre-post historical control design. Three of the reviews examined hospital mortality. Only one performed a meta-analysis of the available data. This meta-analysis pooled 15 studies published between 2000 and 2016 and found that RRSs reduced the risk of hospital mortality by 15% (relative risk (RR) 0.85; 95% confidence interval (CI), 0.76 to 0.94). 30 A second review reported that 7 of 13 studies found statistically significant reductions in hospital mortality in association with RRS implementation. 28 A third review was performed by the Cochrane collaborative and defined the intervention to include early warning system (EWS) scores and an RRS and concluded that the intervention made little to no difference in hospital mortality though the conclusion was of low certainty. 29 All three reviews rated the quality of the included studies as low due to heterogeneity and high risk of bias.
We identified seven primary studies (all using a pre-post historical control design) addressing hospital mortality.32–34,36,37,41,46 Three studies were in pediatric patients41–43 with one limited to post-cardiac surgery 43 and one being a multi-site study across 38 pediatric hospitals. 36 In adults, one primary study 32 found no improvement. A second study changed their part-time RRS to 24/7 coverage with a proactive rounding process and reported a 27% reduction in the hospital risk-adjusted mortality, but provided no statistics. 34 Another study 33 initially found a small statistically significant increase in hospital mortality in the first three years after RRS implementation. One study reported a statistically significant reduction (nearly 50%, p < 0.001) in unexpected mortality in post-cardiac surgery patients. 46 Of the pediatric studies, two reported statistically significant reductions.36,37 The third pediatric study focused on pediatric cardiac patients and showed a reduction in mortality from four deaths to one death but did not provide statistics. 41
Impact of an RRS versus no RRS: Incidence of CA
We identified three reviews that examined the incidence of CA.28–30 One review of 15 studies found that RRSs significantly reduced the risk of CA on the general hospital ward (RR 0.65; 95% CI, 0.49 to 0.87). 30 Another review reported that 8 of the 13 studies that examined CA found statistically significant reductions in this outcome but did not perform a meta-analysis. 28 A Cochrane review found that RRSs that included EWS implementation had little to no impact on the incidence of CA with a low degree of certainty. 29
We identified three primary studies34,37,46 that reported on the incidence of CA, one of which was in a pediatric population. 37 For adults, one primary study found a 65% reduction but provided no statistical analysis. 34 The other study 46 found that implementation of a RRS for post-cardiac surgery patients did not change the incidence of CA. A nonstandard metric was used in the pediatric study 37 (arrest post-arrival in the Pediatric ICU versus arrest on the general ward). This study found a significant drop in these events.
Impact of an RRS versus no RRS: Transition to higher level of care
Transition to a higher level of care was defined as transfer to an ICU, intermediate care unit or an unplanned transfer to the operating room or other procedural area such as interventional radiology. Of the included reviews, only one addressed this outcome 29 and it found that an RRS with an EWS did not change transitions to a higher level of care though the certainty of the data was low to very low. We identified two primary studies34,41 that reported this outcome. One in pediatric cardiac surgery patients found a statistically significant reduction (p < 0.001) in unanticipated ICU re-admission 41 and the other, in adults, reported a reduction of 4.7% but provided no statistical analysis. 34
Impact of an RRS versus no RRS: Other serious adverse events
We identified one review that examined additional outcomes including a composite outcome that combined unanticipated ICU admission, death, and the incidence of CA, and length of stay (LOS). They found that randomized and non-randomized trials demonstrated no impact on the composite outcome or LOS with certainty levels that were moderate and low, respectively. 37
We identified two primary studies that addressed other serious adverse events.37,46 One in pediatric patients examined events subsequent to PICU admission after an RRS activation. This study found that endotracheal intubation and mechanical ventilation within an hour of arrival in the PICU nearly doubled after RRS implementation but that the need for mechanical ventilation was unchanged. This study also reported a statistically significant reduction in ICU mortality and in PICU LOS (p < 0.001). 37 A pre-post design study in adult cardiac surgical patients 46 looked at a number of adverse events (need for dialysis, re-operation, and others) and found no difference after the implementation of the RRS.
Impact of an RRS versus no RRS: Unintended consequences of RRSs
We identified one review, that included nine studies, which examined how ICU patients were affected when their nurses stepped away to respond to a RRS activation. 31 They suggested that dual ICU and rapid response team roles (a common staffing model) had negative effects on nurses’ workload and increased risk of adverse events in ICU patients. How this might apply to physicians, advanced practice providers, and other clinicians were not examined.
Impact of afferent limb modifications: Hospital mortality
We identified four primary studies addressing mortality in association with one or more afferent limb modifications, and no relevant reviews on afferent limb modifications. Two were performed in a pediatric populations38,39 while two were carried out in adults.35,42,45,47 An additional two studies 43 , 51 investigated both afferent and efferent modifications simultaneously and are discussed separately. All used a non-randomized methodology.
Most studies used multi-pronged interventions. One study35assessed stepwise modifications including real-time deterioration risk scoring with remote nurse-led monitoring of those scores. This 19-hospital study found that the risk of mortality at 30 days after meeting RRS activation thresholds was statistically lower (p < 0.001) and total hospital mortality also dropped (14.4 to 9.8%) but no statistical analysis was given. One, in pediatrics, assessed implementation of modifications including automated EWSs, huddles to identify high risk patients, learning collaboratives, workgroups, and policy changes. This study including only patients who arrested found that post-arrest mortality on the general wards fell from four during the pre-implementation period to zero. 38 No statistical analysis was given.
One study examined wearable continuous vital sign sensors to enhance recognition of deterioration and improve earlier activation. The study found nearly 40% and 30% reductions in mortality in the two populations studied (neurosurgical and neurological patients), though this was not statistically significant. 47 A second pediatrics study examined family activation of the RRS as a modification and found that the reasons for activation differed so much from clinician activation that comparisons could not be reliably made. 33
Impact of afferent limb modifications: Incidence of CA
We identified two primary studies that reported this outcome in association with modifications of the afferent limb; both were in pediatric patients.38,39 One study, 38 in a time series evaluation of a multi-pronged modification, found that the incidence of CA fell from 0.31 per 1000 patient days to 0.11 but provided no statistical analysis. The other study, 39 in comparing family activation of the RRS to clinician activation, found that clinician-initiated RRS events were statistically more likely to progress to arrest, but the underlying reasons for activation between the two groups were substantially different making comparison unreliable.
Impact of afferent limb modifications: Transition to higher level of care
We identified seven primary studies that examined this outcome after modifications to the afferent limb. One primary study 49 implemented a series of modifications to their RRS including introducing a calculated EWS, adding protocols for communication, and implementing continuous wireless vital sign monitoring among others, finding no significant change in transfers to the ICU. Similarly, another study 47 found non-significant decreases in transfer to higher levels of care after implementing a wireless continuous monitoring system.
A third study added real-time deterioration risk scoring with remote nurse-led monitoring and found a statistically significant reduction in transfers to a higher level of care. 35 A fourth study reported a statistically significant drop in transfers to the ICU after instituting a combination of EWS and a proactive critical care outreach model. 43
In pediatrics, a study using an EWS modification found no significant change in the incidence of transfer to the ICU 40 and neither did a second study 38 in response to afferent limb modifications. Finally, one study found that family activation as a modification resulted in less frequent transfers for those events but that they were not comparable to clinician-activated events, making direct comparisons unreliable.
Impact of afferent limb modifications: Other serious adverse events
One primary study in pediatrics 40 found a statistically significant reduction in the incidence of missed/delayed RRS activations after implementation of an EWS.
Impact of efferent limb modification: Hospital mortality
We identified two primary studies in adults for this association and all used non-randomized methodology, and all used multiple modifications. 33 , 50 Modifications included addition of protocols, policy changes, performance improvement strategies, and staffing changes.
One study found that the Hospital Standardized Mortality Ratio decreased by 31.2% but provided no analysis of statistical significance. 50 The other found a statistically significant downward slope trend in mortality (p < 0.001) and improved odds of hospital mortality (p = 0.0014) over the course of the multiple modification steps. 33
Impact of efferent limb modification: Incidence of CA
We identified two primary studies that reported on how efferent limb modification alone may affect the incidence of CA.42,44,48 One study found switching from a nurse staffed response team to a physician one resulted in a statistically significant drop for CA from 2.2 to 0.8 events/1000 patient days. 44 The other study, in pediatrics, 48 examined the introduction of care algorithms and found no change in the incidence of CA.
Impact of efferent limb modification: Transition to higher level of care
Two studies examined this relationship.48,50 One in adults 50 found that switching from a physician-led team to a nurse-led team reduced unanticipated ICU transfers by 35.9% but no statistics were given. The other study was in pediatrics 48 and found no significant change.
Impact of efferent limb modification: Other serious adverse events
We identified one primary study, 48 in pediatrics, that examined other serious adverse events in relationship to efferent limb modifications, specifically the introduction of care algorithms and its effect on a series of adverse event outcomes. All of these events showed a positive change trajectory (p < 0.001) over time.
Combined afferent and efferent modifications: Hospital mortality
Two studies examined making afferent and efferent limb modifications simultaneously, often over a number of years. Both42,45 found statistically significant improvement (p < 0.001) in both overall hospital mortality and one also reported improved observed to expected mortality ratios. 42
Combined afferent and efferent modifications: Incidence of CA
One of the studies reporting improvement in hospital mortality with combined modifications found statistically significant improvement in the incidence of CA (p = 0.04). 42
Strength of evidence
SOE was determined to be low or insufficient for most outcomes in either adults or children. Table 2 shows the SOE for each outcome, intervention, and population. Low grades for SOE were due to methodological weaknesses and high risk of bias.
Barriers and facilitators to implement an RRS
Winterbottom et al. reported that implementation of the RRS restructuring intervention was facilitated by staff support, standardized practices, rapid penetration of clinical changes into routine patient care, and a financial return on investment. 34 Barriers to RRS implementation included variable frequency of nursing vital sign checks, 49 poor multidisciplinary collaboration, 49 and lack of nurse comfort in consulting with a physician-led team.49,50
In a review of qualitative evaluations of RRS implementation, many barriers and facilitators were identified. 53 Administrative facilitators included leadership support, shared mission, involvement of healthcare professionals, continuous quality improvement, and interprofessional training. Administrative barriers were lack of commitment, unclear protocols, lack of staff and equipment, and poorly designed monitoring systems. For the afferent limb, knowledge of the patient, clear protocols, and empowering nurses and physicians were common facilitators, whereas high staff workload, breakdowns between vital sign measurement and interpretation, hierarchy, and poor usability of the monitoring systems were barriers. For connections between afferent and efferent limbs, expertise of staff members and patient-centered teamwork were facilitators, and negative reinforcement of staff was a barrier.
Discussion
We find that RRSs may have a large impact on hospital mortality and an even greater impact on CA in adults and children. RRSs are overall associated with a 10–15% risk reduction in hospital mortality and a 35–40% risk reduction in incidence of CA. The primary studies meeting our eligibility criteria that were not included in the previous systematic reviews would not change these estimated risk reductions. One outlier is a systematic review 29 which showed no benefit from RRS implementation. That review did not perform a meta-analysis and excluded many studies that were included in other systematic reviews, which explains the divergent conclusions. A 10–15% reduction in mortality is clinically important. It means that one out of ten to one out of seven patients who would otherwise die will survive. Given that ICU mortality in the United States for adult patients is 10–29%, and the mortality rate for pediatric ICU patients ranges from 2% to 6%, 52 these reductions are clinically important. Unfortunately, the certainty of the conclusions is low due to high risk of bias in the primary studies included here and in all the systematic reviews.
We found substantial heterogeneity in outcomes across hospitals with RRS implementation. The systematic review we identified and all previous systematic reviews14–18 found substantial heterogeneity in the effect of RRSs on outcomes. Most hospitals achieved substantial reductions, but some did not experience any improvement. In our review of primary studies, one in adults found no benefit while all others, including the pediatric studies, found mortality benefit. Only two studies used a definition of CA that is consistent with previous studies and the MHS III report. One study found decreased CA while the other study, which was in a restricted patient population, found no benefit.
Many institutions are implementing modifications to their RRS programs to achieve success where they previously failed or to realize further improvement. Since 2019, studies examining the impact of RRSs in the United States have shifted to include a number of studies examining how the afferent limb or efferent limb might be improved to achieve better outcomes. The MHS III report identified only one such publication and we identified 14 that have examined changes to both the afferent and efferent limb. We conclude that implementing modifications in the afferent and efferent limbs of an RRS yields improvements in hospital mortality and incidence of CA. Most of these primary studies focused on the afferent limb and modified the afferent limb through use of EWSs but many did this in combination with other modifications. All these studies found reductions in hospital mortality. The data was more limited for CA but also found a large benefit. Modifications to the efferent limb also resulted in reductions in hospital mortality and incidence of CA in primary studies reporting these two outcomes. Efferent limb modifications often included staffing changes and the deployment of care algorithms.
Family activation of the RRS is an afferent limb modification that deserves special consideration. While this modification should be compared to clinician-based activation so that lessons learned from either type of activation can inform the other, family activation needs to be examined through a different lens. As noted in Bavare et al., 33 the reasons that trigger activations by family members are often different from why clinicians activate the efferent limb. Clinicians usually activate for physiological instability. While physiological instability is commonly found in patients who have family activations, the reasons given for the family triggering activation are primarily poor pain management and lack of communication regarding the plan of care. Comparison of family activations across hospitals might provide opportunities to learn how to better engage family members. Family activation is likely a marker for poor communication with clinical staff and may be influenced by social determinants of health. Comparison of family-initiated and clinician-initiated activations may help to explore whether families recognize subtle signs, such as cognitive or behavioral changes, better and earlier than clinicians.
RRSs may have unintended consequences. One unintended consequence is the potential risk posed to ICU patients when an efferent limb staffing model pulls critical care providers from their primary responsibility of caring for ICU patients. This was a common model in the publications we identified though it is unclear if it is the predominant model in the US. The systematic review we identified found no patient harm in any of the primary studies it reviewed but did report findings of increased nursing workload and a concern from nurses about an increased risk of adverse events for ICU patients. While we did not identify any studies focused on costs, the authors of the prior review opined that to avoid the increased nursing workload, different staffing models need to be used, and this change may incur additional costs. However, one primary study reported a financial return on investment from using a dedicated RRS nurse role. 44
The first consensus conference on RRS 54 identified four core components of an effective RRS: (1) an afferent limb focused on detection and recognition of deterioration; (2) an efferent limb of qualified clinical responders; (3) an administrative component; and (4) a data collection and quality improvement component for self-analysis. Our review suggests elements that can improve RRS implementation and patient outcomes. First, dedicated, and ideally funded, personnel should be established for data collection and analysis as well as for administrative oversight of the program. Second, staff need appropriate support, especially in terms of establishing a culture of safety that empowers clinicians to activate the efferent limb when criteria are met, rewards them rather than bringing ridicule upon them, and addresses communication failures and delays. Third, technological solutions and cultural changes are needed to improve the acquisition of physiological data and transformation of that data into triggers. Fourth, practices need to be standardized for afferent and efferent limbs. Finally, educational resources and opportunities for joint training are necessary for afferent and efferent limbs.
This review has limitations. We restricted the review to studies from 1 January 2018, forward and for primary studies restricted eligibility to US studies because the rapid review was mainly intended to inform US policymakers and RRSs may differ widely in other countries in terms of design and resources. The systematic reviews we identified, however, did include studies from around the world. Another limitation to consider is that this analysis deconstructed systems that have interdependent components between the afferent and efferent limbs. While that distinction is important, it may have limited the ability to determine the effectiveness of the intervention as a unified whole.
Another limitation of this review is that the quality of the RRS literature is limited by significant heterogeneity and risk of bias, with no studies presenting a low risk of bias. Several types of risk of bias were present in the non-randomized studies, including concerns for bias in confounding, patient selection, missing data, measurement of outcomes, and selection of reported results. Ten of the 19 non-randomized studies had critical risk of bias (Figure 2). Also, primary studies often drew conclusions with limited or no statistical analysis. All primary studies were observational though some used cluster randomization. Therefore, we can only report associations, and these are reported with low certainty.
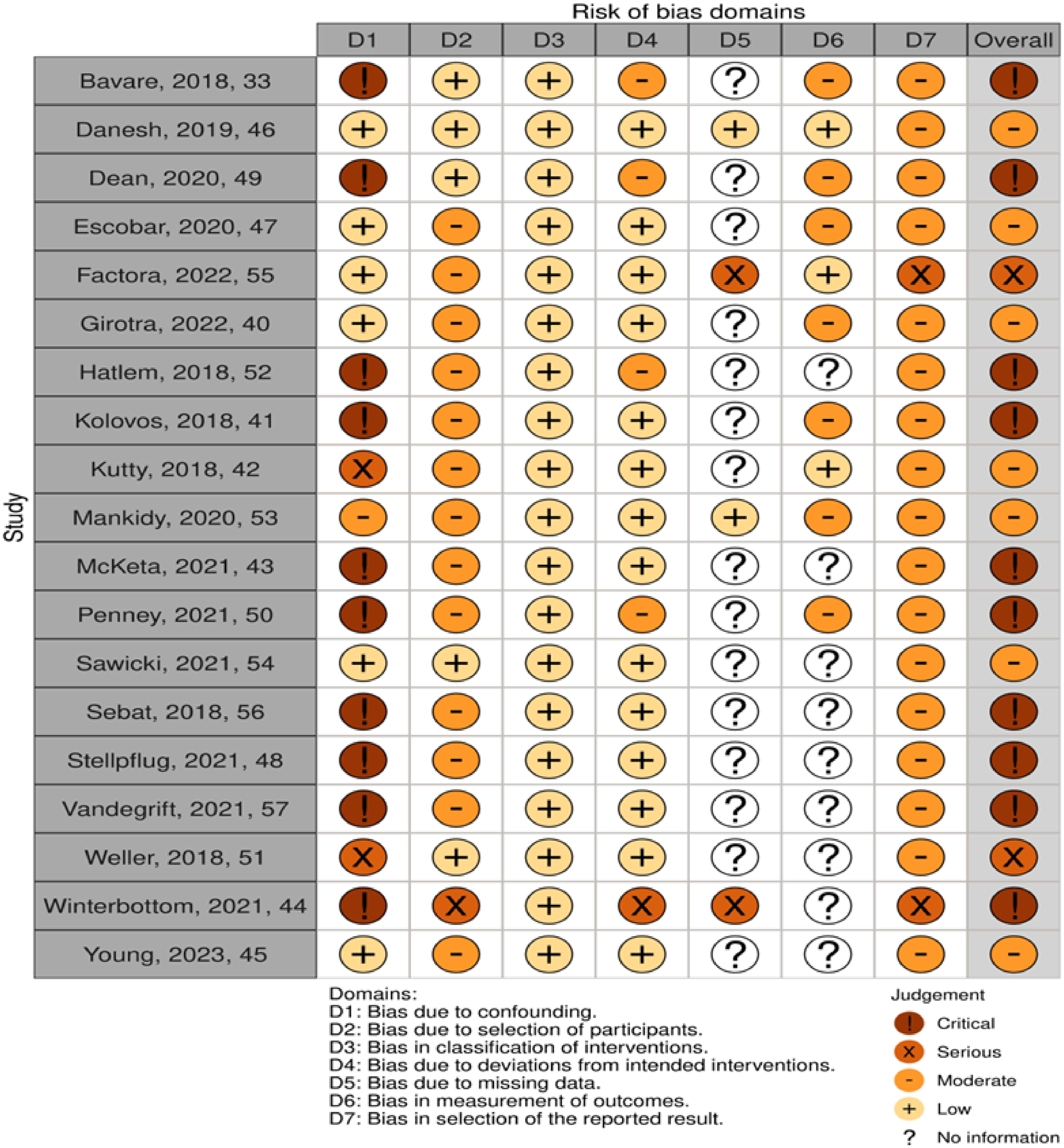
Risk of bias assessments for nonrandomized studies included in this review*.
Despite the limitations of the evidence, RRSs appear to be effective and modifications to existing RRS seem to be beneficial. The measured effect that RRSs have on outcomes has not changed over the course of time as estimated by several systematic reviews, suggesting that to achieve greater effectiveness we need to further develop and test RRS modifications. While there are no direct comparisons of an afferent limb modification against an efferent limb modification, afferent limb modifications seem to be the more robust area for future gains.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclaimer
The authors of this manuscript are responsible for its content. Statements in the manuscript do not necessarily reflect the official views of or imply endorsement by AHRQ or the U.S. Department of Health & Human Services (HHS).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The project was funded under Contract No. 75Q80120D00003 Task Order 75Q80122F32009 from the Agency for Healthcare Research and Quality (AHRQ), U.S. Department of Health and Human Services (HHS).