
Abstract
Background
Atherosclerotic cardiovascular disease (ASCVD) risk factors in mid-life are associated with cognitive decline and late-life dementia. However, the role of these risk factors in Alzheimer's disease (AD) pathology remains elusive.
Objective
We investigated the association of mid-life 10-year ASCVD risk with late-life amyloid, tau, neurodegeneration [AT(N)] measures and white matter hyperintensities (WMHs).
Methods
Participants enrolled in the Heart Strategies Concentrating on Risk Evaluation (Heart SCORE) study between 2003–2005 (mid-life) and underwent brain MRI and PET scans in 2018–2022 (age >65 years, late-life) to detect and quantify amyloid (A, PiB-PET) and tau (T, Flortaucipir (FTP) PET) deposition, cortical thickness (N) and WMHs. Mid-life ASCVD risk was categorized as; borderline (5%–7.4%), intermediate (7.5%-<15%), or high (≥15%). Association of mid-life ASCVD risk HR (95% CI) was assessed using logistic and linear regressions with A, T, or N and chi square beta coefficients for WMH in late life.
Results
Over a ∼16 years follow up, in 135 participants (mean age 73 years), mid-life ASCVD risk categories had a graded association with neurodegeneration (ORASCVD high vs low risk% 6.98 [2.44–19.95]; p < 0.05) driven primarily by self-identified Black race and age, while none with A and T. ASCVD risk score was also associated with WMHs ((β=0.42 ± 0.22; p = 0.05).
Conclusions
In this asymptomatic, diverse cohort, 10-year ASCVD risk was predictive of late-life neurodegeneration and WMHs but not amyloid or tau. Further mechanistic studies can elucidate whether midlife ASCVD risk factors associated neurodegeneration initiates brain vulnerability leading to AD in late life.
Introduction
Alzheimer's disease (AD) and AD-related dementias are a major public health challenge in the United States with projected increases to 9.3 million by 2060. 1 Development of disease-modifying therapies are challenging due, in part, by the long preclinical window of AD. The preclinical window of AD can begin in mid-life, providing a critical window for identification and optimization of AD risk factors.
In the National Institute on Aging and Alzheimer's Association Research Framework, AD is defined by its underlying pathologic processes that can be documented by postmortem examination or in vivo by biomarkers. The diagnosis is not based on the clinical consequences of the disease (i.e., symptoms/signs) in this research framework, which shifts the definition of AD in living people from a syndrome to a biological construct. The research framework focuses on the diagnosis of AD with biomarkers in living persons. Biomarkers are grouped into those of amyloid-β (A) and tau (T) deposition, and neurodegeneration (N) or collectively identified as AT(N). This classification system groups different biomarkers (imaging and biofluids) by the pathologic process underlying each measure.
Neurodegenerative changes (N) in the absence of amyloid and tau, in addition to white matter hyperintensities (WMHs) are suggested to be linked with various forms of cognitive decline—though their involvement in AD onset remains elusive. Both WMHs and neurodegenerative changes, like atherosclerotic cardiovascular disease (ASCVD), can present years before cognitive decline.2,3 Hypertension, inflammation, and dyslipidemias, risk factors for ASCVD, have been linked with neurodegeneration and WMHs in individuals with cerebrovascular pathology and without.4–7
In the United States, 10-year ASCVD risk assessed calculated by the pooled cohort equations (PCE) is used as a guiding tool to identify individuals are risk for ASCVD events. 8 In the 2013 and 2018 American Heart Association and American College of Cardiology's cholesterol guidelines, the PCE derived 10-year risk was recommended to guide the use of statin therapy in primary prevention. Although the PCE predicts ASCVD events, its risk prediction for dementia or AD pathology has not yet been assessed. This study investigated the association of PCE based ASCVD risk score with cerebrovascular white matter damage as WMHs, neurodegeneration and brain biomarkers of AD in a biracial cohort of community dwellers with preserved cognition over a ∼16-year follow up period.
Methods
The Heart Strategies Concentrating on Risk Evaluation (Heart SCORE) study originally enrolled 1949 participants aged 45–75 years at baseline entry between 2003–2005 (∼44% racialized as Black, ∼66% women) to examine racial disparities in the prevalence and outcome of ASCVD (NCT00143923).9,10 The cohort underwent a baseline evaluation of demographic and psychosocial characteristics and serologic markers including all the variables of the PCE derived ASCVD risk (i.e., age, sex, self-reported race, total cholesterol, high density lipoprotein cholesterol, triglycerides, diabetes, hypertension medications, systolic blood pressure, and smoking history). From the original Heart SCORE study, a subset of participants who are currently undergoing late-life neuroimaging and neurocognitive testing (Heart SCORE Brain Study), were recruited for this analysis. All participants underwent a baseline Montreal Cognitive Assessment prior to inclusion; those who met criteria for dementia at a Consensus Diagnostic Conference were excluded from the current study.
Brain magnetic resonance imaging (MRI) scans
The MR scanning was completed on a Siemens Prisma 3-T scanner, equipped with 64-channel systems with Connectome level gradients operating at 80 mT/m. 11 Briefly, the following sequences were obtained from all participants: MP-RAGE (Magnetization Prepared - Rapid Gradient Echo), axial gradient recalled echo T2-weighted imaging, axial T2 fluid-attenuated inversion recovery (FLAIR).
We processed T1 images with FreeSurfer version 7.1 to define regions-of-interest (ROIs) and total intracranial volume. 12 We applied the Imperial College London Clinical Imaging Center (CIC) atlas to better delineate functional subdivisions of the striatum. 13 All parcellations were visually inspected prior to analysis. We calculated a composite measure of medial temporal lobe cortical thickness (mm) as the surface area-weighted average of FreeSurfer ROI-derived cortical thickness in the fusiform gyrus, entorhinal cortex, inferior and middle temporal gyri. 12 Participants were categorized as N + if their medial temporal lobe cortical thickness </= 2.8 OR 2.7. 14 WMH volume was derived from T2 FLAIR images using a quantitative computer-aided segmentation program to measure the volumetric burden (cm3) of WMH volume. 15
Prior to the positron emission tomography (PET) imaging session, a T1-weighted structural MR series (MPRAGE) was acquired using a 3T Siemens PRISMA scanner with a 1 mm isotropic voxel size. Each participant's MR image was parcellated into a set of ROIs using the default FreeSurfer v5.3 12 pipeline and Desikan-Killiany atlas with the exception of striatal subregions, which were substituted by components from the CIC atlas 13 as previously described. 16 All FreeSurfer ROIs were visually inspected and manually edited where appropriate.
An AD-signature composite cortical thickness index was derived based on a surface-area weighted average of the mean cortical thickness of four FreeSurfer ROIs: entorhinal, inferior temporal, middle temporal, and fusiform. Abnormal composite cortical thickness indicating neurodegeneration (N+) in the ATN framework was defined as <2.7 mm based on a sensitivity threshold.14,17
PET imaging with Pittsburgh Compound B
Detailed methods for [11C]Pittsburgh Compound-B (PiB) PET have been published.18–20 Brain Aβ burden was measured via PiB 21 on either a Siemens Biograph mCT PET/CT scanner (Siemens Healthcare GmbH, Erlagen, Germany) or a Siemens ECAT Exact HR + scanner (Siemens Healthcare GmbH). We measured brain tau load using [18F] Flortaucipir (FTP) on the same Siemens Biograph mCT PET/CT described above. Briefly, at separate PET visits, participants received slow bolus injections of either PiB (∼15 mCi) or FTP (∼10 mCi). After a tracer-appropriate delay (PiB: 25 min; FTP: 75 min), participants were positioned in the scanner for a transmission scan for attenuation correction. PiB PET studies were then acquired 50–70 min post-injection; FTP PET studies were acquired 75–105 min post-injection.
Each PiB and FTP scan was visually examined and, if necessary, corrected for interframe motion prior to analysis. We created a single PET frame by averaging the images over tracer-specific post-injection intervals (PiB: 50–70 min; FTP: 80–100 min). Using PMOD version 4.1 (http://www.pmod.com), we co-registered each single-frame PET image to its corresponding MRI in native space and sampled the images with FreeSurfer and CIC atlas ROIs.
Global Aβ burden for each participant was measured as a single, global standardized uptake value ratio (SUVR), calculated as the volume-weighted average of PiB radioactivity in nine FreeSurfer-defined ROIs, normalized to cerebellar gray matter. 22 We considered participants to be A + if their global PiB SUVR >/= 1.3. 22
We used meta-temporal SUVR as a measure of tau burden by calculating the volume-weighted average of FTP radioactivity in FreeSurfer-defined entorhinal cortex, hippocampal gyrus, fusiform, inferior temporal gyrus, and middle temporal gyrus, normalized to cerebellar gray matter. 22 Participants were considered T + if their meta-temporal FTP SUVR >/= 1.18.
All PET and MR scans were quality controlled twice at the time of the MRI and PET scan by a coordinator, and MR sequences with excess motion are repeated, after scanning an expert analyst, hand quality controlled all FreeSurfer parcellations and rates, all of the images from the study passed quality control. FreeSurfer 5.3 is utilized for all PET and cortical thickness analyses and FreeSurfer 7.1 is utilized for WMH.
Covariates and PCE 10-year ASCVD risk
Baseline characteristics of the study population were defined using data at the entry into the Heart SCORE cohort. These included sociodemographic data (age, sex, and race/ethnicity, low-density lipoprotein cholesterol, and the remaining PCE variables including total cholesterol, high-density lipoprotein cholesterol, treatment for hypertension, systolic blood pressure, current smoking status, and diabetes. The cohort was divided into four categories of PCE-derived 10-year risk8,23 – low-risk (<5%); borderline risk (5%–7.4%); intermediate risk (7.5%–<15%), and high risk (≥15%).
Detailed methods for Heart SCORE lab and biomarker assessments have been described elsewhere. 9 Briefly, lipid measurements were performed on fasting plasma samples that were stored at −70°C with ethylenediaminetetraacetic acid as the anticoagulant. Plasma total cholesterol, high-density lipoprotein cholesterol, and triglycerides were measured using enzymatic measures. 10 Low-density lipoprotein cholesterol was calculated using the Friedewald equation. 24 Diabetes mellitus was defined as a fasting glucose level ≥126 mg/dL, a self-reported physician diagnosis of diabetes, or use of diabetes medications. Hypertension in the Heart SCORE study is defined as systolic blood pressure ≥140 mm Hg or diastolic blood pressure ≥90 mm Hg or use of blood pressure–lowering therapies. Consistent with the PCE, smoking history was categorized as current or not current (a composite of never and former smoking). Inflammatory burden at baseline was assessed by measuring high sensitivity C reactive protein (hsCRP).
Arterial stiffness
Arterial stiffness and wave reflection were measured at Heart SCORE study entry (mid-life) using the Endo-PAT device and expressed as heart rate-adjusted augmentation index (AI75). 25 Higher AI75 denoted higher arterial stiffness and wave reflection.
Statistical analysis
Baseline descriptive statistics of the study sample, such as the minimum, maximum, median, and mean for each continuous variable and frequency table for each categorical variable, were initially analyzed to summarize the data and detect outliers and missing values. Missing data were uncommon. Descriptive characteristics are presented as mean and SD for continuous variables, and frequencies and proportions for categorical variables. The difference of mean across the ASCVD groups is assessed by 1-way ANOVA, while the difference of frequencies is compared using the χ2 test.
WMH volume was natural log-transformed to adjust for skewness. We used linear and logistic regression models to estimate the association of the 10-year ASCVD risk score with WMH volume, brain amyloid deposition and neurodegeneration. We evaluated mid-life 10-year ASCVD risk score as a continuous and categorical variable. All models were fully adjusted for education level and hsCRP measures. Further, WMH were adjusted for total intracranial volume.
In an exploratory analysis, we also assessed association of arterial stiffness (AI75) in mid-life as a continuous variable with late-life WMHs.
Results
Baseline characteristics
Participants with PET imaging
A subset of 145 Heart SCORE participants with PET imaging were included in the current analysis out of whom 68.3% were women and ∼30% of self-identified Black race (Table 1). Overall, 35.2% of the participants had baseline hypertension and ∼38% were categorized as high risk according to the 10-year ASCVD risk in mid-life. In race-stratified baseline characteristic, more Black participants had baseline hypertension (54.8%) and diabetes (7%). Black participants (∼62%) were noted to have a higher mid-life 10-year ASCVD risk (>7.5%) compared to White (31%) counterparts (Supplemental Table 1).
Baseline characteristics of the heart SCORE participants undergoing brain PET imaging.

SD: standard deviation; HDL-C: high density lipoprotein cholesterol; BP: blood pressure; ASCVD: atherosclerotic cardiovascular disease.
Participants with WMH
A subset of 60 participants included from the Heart SCORE brain MRI study was included in the current analysis (Table 2). Mean age at baseline was 59.7 ± 4.4 years (∼60% women and 30% self-identified as Black) with ∼38% hypertensive participants. The mean ASCVD risk score for this subset was 8 ± 0.06% (Table 2).
Baseline characteristics of the heart SCORE participants undergoing brain MRI imaging.

SD: standard deviation; HDL-C: high density lipoprotein cholesterol; BP: blood pressure; ASCVD: atherosclerotic cardiovascular disease.
Association of mid-life ASCVD risk and late life brain biomarkers of neurodegeneration using cortical thickness
Neurodegenerative (N) biomarker had a graded association with increasing mid-life ASCVD risk categories (ORASCVD highVsLow risk% 6.98 [2.44–19.95]; p < 0.05) while no significant association was found with PiB uptake (A) on PET (Table 3 and 4) after a mean 16y follow up. In fully adjusted models, the association of neurodegeneration brain biomarker with the 10-year ASCVD risk was mainly driven by self-identified Black participants (RR 3.18 [1.77–5.12]), age (RR 1.84 [1.35–2.42]) and aspirin use (RR 2.10 [1.34–3.26]; all p < 0.05 (Supplemental Table 2). Baseline education level and hypertension were not associated with late-life neurodegeneration.
Mid-life 10-year ASCVD risk and association with brain biomarkers of Alzheimer's disease on PET imaging.

Bold text is to highlight significant p values.
∼p < 0.1; *p < 0.05.
ASCVD: atherosclerotic cardiovascular disease; RR: relative risk; CI: confidence interval. ^Amyloid deposition by Pittsburgh compound B uptake on imaging.
Midlife 10-year ASCVD risk and its association with neurodegeneration stratified by self-reported race.

Bold text is to highlight significant p values.
ASCVD: atherosclerotic cardiovascular disease; RR: relative risk; CI: confidence interval.
Given the significantly higher risk of neurodegeneration biomarker in Black participants, we conducted a race-stratified regression analysis (Table 3). A graded risk was observed across the ASCVD risk score amongst Black participants as well as White. However given a limited number of Black participants, we did not observe significant associations. Amongst White participants, mid-life 10-year risk of >15% had the highest risk of neurodegeneration (RR 8.46 [1.89–37.88]; p = 0.01) (Table 3).
Association of mid-life ASCVD risk and late life brain biomarkers of AD
We did not find a statistically significant association of midlife 10-year ASCVD risk with brain biomarkers of AD (A or T). Although there was a trend noted towards higher risk of amyloid (A) deposition (OR 1.14 [0.23–4.46)], it did not reach statistical significance.
Association of mid-life ASCVD risk and late life WMH on brain MRI imaging
In the continuous linear regression, late life WMH lesion burden significantly correlated with mid-life ASCVD 10-year risk (β=0.51 ± 0.21; p = 0.02). When these data were adjusted for hsCRP and education level < college, this association was attenuated (0.42 ± 0.22, p = 0.05) (Table 5). There was a significant negative association with WMH burden in late life with mid-life elevated hsCRP (β= −0.25 ± 0.11; p = 0.03) while no significance was observed with education level. We observed a graded association with risk of WMH burden in participants with intermediate to high mid-life 10-year ASCVD risk when stratified by categories of risk (Table 6). In model 2 (adjusted for hsCRP and education level), the association WMHs with mid-life ASCVD risk of >15% was no longer statistically significant; likely driven by inflammation burden (hsCRP β= −0.28 ± 0.11; p = 0.02). In the exploratory analysis, there was a signal of association between mid-life vascular stiffness and late-life WMHs in this cohort (β= 0.016 ± 0.009; p = 0.06) largely driven by presence of hypertension (β= 0.88 ± 0.39; p = 0.03).
Association of 10-year atherosclerotic cardiovascular risk score with white matter hyperintensities on brain MRI: linear regression with ASCVD as continuous variable.

* Regression coefficient was for 1SD (=0.089) increment. Model 1 = unadjusted, Model 2 = adjusted for education and hsCRP.
Association of 10-year atherosclerotic cardiovascular risk score with white matter hyperintensities on brain MRI: linear regression with ASCVD score as categorical variable.
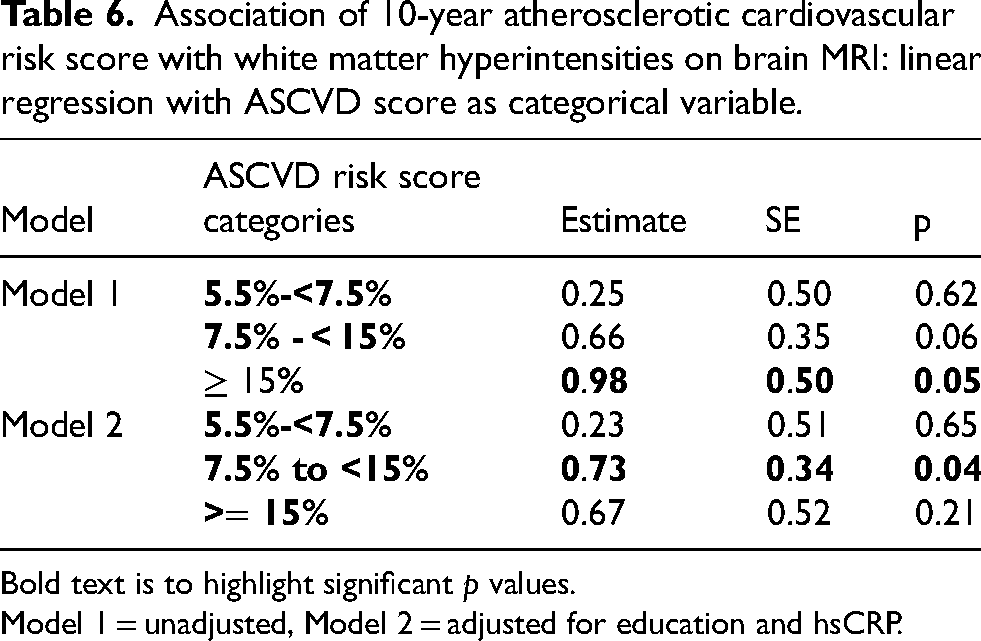
Bold text is to highlight significant p values.
Model 1 = unadjusted, Model 2 = adjusted for education and hsCRP.
Discussion
In a longitudinal cohort of community dwellers without cognitive impairment we present three key findings: 1) mid-life 10-year ASCVD risk was significantly linked to WMHs and neurodegeneration, but not to amyloid or tau, on brain imaging over 15 years later; 2) this association increased with higher ASCVD risk; and 3) the association between ASCVD risk and neurodegeneration was mainly influenced by self-reported Black race (Figure 1). To our knowledge, this is the first study evaluating mid-life ASCVD risk score and its long-term association with WMHs, neurodegeneration, and AD imaging biomarker burden in the same cohort of cognitively unimpaired adults.

Ten-year atherosclerotic cardiovascular disease (ASCVD) risk score in midlife predicts brain neurodegeneration and white matter hyperintensities in late life.
Our findings are clinically significant, suggesting that the routinely used 10-year ASCVD risk score could serve as a valuable tool for early intervention to prevent WMHs and neurodegeneration—both contributors to “brain vulnerability” and potential progression to dementia and AD. 26 The ASCVD risk score is an established predictor of ASCVD events within the Heart SCORE population10,27,28 and other cohorts across the United States.29,30 This score is routinely implemented in clinical practice by clinicians (such as primary care physicians, geriatricians, internists and cardiologists) to identify high risk individuals who will benefit from aggressive preventive interventions including statin therapy initiation. 31 Thus, to utilize a common tool for risk stratification for future ASCVD and a “vulnerable” brain state is an important advance in risk stratification and patient-physician discussion on preventive care. de Havenon et al. recently reported the association of ASCVD risk with elevated WMH burden and progression in their preliminary work. 32 Individually, hypertension and other cardiac risk factors have been associated with WMH and neurodegeneration in several cross-sectional analysis.33,34 However, longitudinal prediction of WMHs, neurodegeneration and brain AD biomarkers with a routinely used clinical tool has not been performed in a cognitively unimpaired and diverse community cohort.
The significance of WMHs as an important neuroimaging characteristic has been established recently in those with autosomal dominant AD (ADAD). 35 In individuals with ADAD and cognitive impairment, Schoemaker et al. found that WMH volume was higher compared to both cognitively unimpaired ADAD and non-carriers. Conversely, cortical amyloid burden on PET and cerebrospinal fluid (CSF) phosphorylated tau levels were elevated, and CSF amyloid levels were reduced in both cognitively unimpaired and impaired mutation carriers, relative to non-carriers. Rizvi et al. have also shown that WMHs were associated with cortical thinning in the right frontal/parietal regions over a span of 4 years. 36 These patterns of atrophy align with the neurodegenerative changes commonly observed in AD including the characteristic cortical signature involving the entorhinal cortex and multiple cortical regions.
Cortes-Canteli and coworkers recently showed an association of brain hypometabolism with modifiable cardiovascular risk factors stratified by the Framingham risk score. 37 Indeed risk factors of CVD including hypertension, 38 hyperlipidemia, 39 metabolic syndrome, 40 and cigarette smoking 41 have a very strong association with dementia incidence.42,43 More recent evidence also links these risk factors for promotion of amyloid and progression of AD pathology.44–46 Although we did not observe an association of the 10-year risk score with brain amyloid and tau in the current analysis; it is plausible that long-term presence of ASCVD risk factors creates a “vulnerable” region for amyloid and tau deposition in the later years and subsequent progression to AD dementia.47–50
The 10-year atherosclerotic CVD risk score, 8 which takes into account presence of modifiable and non-modifiable clinical risk factors has an excellent predictability for ASCVD events. However, during transition from mid-to late-life, the clinical risk factors become more prevalent and are less predictive of clinical disease; thus, they likely under-quantify event “risk”. We have previously shown that in older adults, addition of biomarkers of inflammation, myocardial stretch and injury improved ASCVD event prediction (ΔAUC 0.103; continuous NRI 0.484) when added to the 10-year risk score clinical variables. 51 Thus, in the current analysis, it is also possible that the 10-year ASCVD risk score is less predictive of AD pathology on PET due to the older age of these individuals. It may be imperative to explore whether ASCVD risk score is associated with elevated plasma AD biomarkers, which can predate the tau and Aβ deposition in PET scans.52–55
Our results also signal arterial stiffness and hypertension in mid-life as likely primary drivers of WMHs in mid-life as shown previously.56–59 Whereas neurodegeneration was mainly seen in association with self-reported Black race. Thus, the likely mechanisms that lead both these pathological states in the brain may be different and necessitate exploration of racial difference in preclinical AD pathology. Furthermore, since race is a social construct, the impact of disparities in lived experiences and social determinants of health, including healthcare access inequities, need to be thoroughly assessed as the driver for not only AD but also ASCVD risk.
Limitations
Our study has some notable limitations. First, Heart SCORE is a highly educated cohort and homogeneity in terms of years of education may limit comparisons. However, we expect that high education level would not artificially increase neurodegeneration or WMHs burden. Second, more precise contributions of genetic influences, lifestyle, stress, and socioeconomic environmental exposure may influence these results, and we did not test for such interactions. Importantly, in our cohort, we also observed a low proportion of A and T positive participants thus limiting the assessment of AD pathology. Finally, we measured the 10-year ASCVD risk score one time during mid-life. Although the score may be influenced by several cardiovascular risk factors, age is the primary driver of this score and thus overtime it will increase rather than reverse in a vast majority of individuals. While our study included a good proportion of Black and White individuals, the generalizability to other racial/ethnic minorities and geographic regions may be limited due to lack of representation.
Conclusion
A key question is if the confluence of ASCVD risk factors, as measured by the 10-year risk score, can also quantify future risk of the vulnerable brain by virtue of WMHs and neurodegeneration? Our current data would point to more exploration of this question in future studies. Statin therapies and other primary preventive measures have shown risk reduction in not only ASCVD events but also dementia incidence.60,61 However, a comprehensive impact of primordial and primary prevention of ASCVD risk factors on WMHs, neurodegeneration, AD pathology and overall, cognitive decline remains to be tested in randomized and controlled studies. This will provide a more comprehensive understanding of the complex interplay between these commonly treatable risk factors in AD initiation.
Supplemental Material
sj-docx-1-alr-10.1177_25424823241299297 - Supplemental material for Association of mid-life cardiovascular risk with biomarkers of Alzheimer's disease, neurodegeneration, and white matter hyperintensities: Heart SCORE brain study
Supplemental material, sj-docx-1-alr-10.1177_25424823241299297 for Association of mid-life cardiovascular risk with biomarkers of Alzheimer's disease, neurodegeneration, and white matter hyperintensities: Heart SCORE brain study by Anum Saeed, Yuefang Chang, Justin Swanson, Michael Vu, Mark Mapstone, Victor L. Villemagne, Beth E. Snitz, Sarah K. Royse, Hongtian Wang, Brian Lopresti, Howard J. Aizenstein, Minjie Wu, Kevin Kip, Steven E. Reis, Oscar Lopez and Ann Cohen in Journal of Alzheimer's Disease Reports
Supplemental Material
sj-docx-2-alr-10.1177_25424823241299297 - Supplemental material for Association of mid-life cardiovascular risk with biomarkers of Alzheimer's disease, neurodegeneration, and white matter hyperintensities: Heart SCORE brain study
Supplemental material, sj-docx-2-alr-10.1177_25424823241299297 for Association of mid-life cardiovascular risk with biomarkers of Alzheimer's disease, neurodegeneration, and white matter hyperintensities: Heart SCORE brain study by Anum Saeed, Yuefang Chang, Justin Swanson, Michael Vu, Mark Mapstone, Victor L. Villemagne, Beth E. Snitz, Sarah K. Royse, Hongtian Wang, Brian Lopresti, Howard J. Aizenstein, Minjie Wu, Kevin Kip, Steven E. Reis, Oscar Lopez and Ann Cohen in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgments
The authors acknowledge the contributions of Amy Beto, Janet Bonk, Mary Catherine Coast, Jowanda Green, Carol Hrtyanski, Louise Martin, Lee Ann McDowell, Jennifer Rush, and Roberta Spanos to implementation of the Heart SCORE study. The authors acknowledge all the Heart SCORE research participants for volunteering their time into the study and making research possible.
ORCID iDs
Author contributions
Anum Saeed (Conceptualization; Investigation; Supervision; Visualization; Writing – original draft; Writing – review & editing); Yuefang Chang (Formal analysis); Justin Swanson (Formal analysis); Michael Vu (Writing – review & editing); Mark Mapstone (Writing – review & editing); Victor L Villemagne (Writing – review & editing); Beth E. Snitz (Writing – review & editing); Sarah K Royse (Writing – review & editing); Hongtian Wang (Project administration); Brian Lopresti (Writing – review & editing); Howard J Aizenstein (Writing – review & editing); Minjie Wu (Writing – review & editing); Kevin Kip (Writing – review & editing); Oscar Lopez (Writing – review & editing); Steven E Reis (Funding acquisition; Writing – review & editing); Ann Cohen (Conceptualization; Data curation; Funding acquisition; Investigation; Methodology; Resources; Supervision; Validation; Writing – review & editing).
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Heart SCORE study was funded by the Pennsylvania Department of Health (ME-02-384). The department specifically disclaims responsibility for any analyses, interpretations, or conclusions. Additional funding was provided by National Institutes of Health (NIH) grant R01AG052446 (Cohen), R01HL089292 (Reis) and R01AG052446 (Steven Reis, Oscar Lopez). Anum Saeed is supported by 23CDA1055489 by the American Heart Association.
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr Saeed has no financial disclosures relevant to this manuscript but she recieves grant funding from the American Heart Association on investigating the Heart-Brain axis. Drs. Chang, Vu Wu, Mapstone, Snitz, Royse, Lopresti, Aizenstein, Kip, Reis and Cohen report no disclosures relevant to this manuscript. J. Swanson reports no financial conflicts. Dr Villemagne is and has been a consultant or paid speaker at sponsored conference sessions for Eli Lilly, Life Molecular Imaging, GE Healthcare, IXICO, Abbvie, Lundbeck, Shanghai Green Valley Pharmaceutical Co Ltd, and Hoffmann La Roche. Dr Lopez was a consultant for Novo Nordisk, Eisai, Lundbeck, and Biogen.
Data availability
The data supporting the findings of this study may be available upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.