
Abstract
Background
This study examines the prevalence and incidence of dementia in Ecuador, with a focus on understanding demographic and social factors associated with increased risk. Data were obtained from the Institute of Neurosciences of Guayaquil, covering patient records from 2010 to 2022.
Objective
The purpose was to identify prevalence trends and key risk factors to inform targeted prevention and early intervention efforts in high-risk groups.
Methods
This observational, correlational study analyzed patient data to estimate dementia prevalence and incidence. Statistical analyses included descriptive statistics to calculate overall and age-specific prevalence rates, while incidence was calculated per 1000 person-years. Correlations and chi-square analyses were used to evaluate associations between dementia and potential risk factors, including age, gender, education level, and marital status.
Results
The overall prevalence of dementia was 3.1%, with higher rates among women (1.8%) compared to men (1.3%). Dementia incidence was calculated at 2.4 per 1000 person-years. Prevalence increased significantly with age, from 1.2% in individuals aged 65–69 to 54.8% in those aged 95 and older. Advanced age, female gender, lower education levels, and lack of a marital partner were associated with higher dementia prevalence.
Conclusions
These findings highlight a rising dementia prevalence in Ecuador, particularly among women and older individuals, with social and educational factors contributing to increased risk. The results underscore the need for tailored dementia prevention and early intervention strategies, especially as prevalence rates continue to rise across Latin America.
Introduction
Dementia is a chronic and progressive syndrome that affects various higher cognitive functions, such as memory, thinking, orientation, comprehension, calculation, learning, language, and judgement. These impairments may be accompanied or preceded by issues in emotional control, social behavior, or motivation, worsening the prognosis due to the increased level of disability. 1
Dementias present diverse manifestations but share an etiology rooted in brain disease that leads to dysfunction. This can be primary, as in diseases, injuries, and trauma that directly affect the brain, or secondary, as in systemic disorders impacting multiple organs, including the brain. 1 Over the past decade, significant advancements have been made in understanding the clinicopathological correlation and in the development of new biomarkers. 2
Dementia is very common in the elderly population. The disease prevalence doubles every five years among individuals over 65 years of age. 3 Numerous epidemiological studies have demonstrated the variability in dementia prevalence rates.4–6
This variability may be related to age differences, the instruments used for cognitive and functional assessments, the diagnostic criteria applied, rural or urban residency, and the representativeness of the studied samples. 7 People with mild cognitive impairment have a 10 to 15% chance of developing dementia compared to healthy individuals, in whom the annual likelihood is 1 to 2%. 8 Compared to women, men have a higher incidence of dementia diagnosis before the age of 70 but a lower incidence after 70. 9
It is estimated that more than 55 million people worldwide live with dementia, the most common type being Alzheimer's disease, accounting for approximately 60% to 70% of cases. The remaining percentage includes other types, such as vascular dementia, dementia with Lewy bodies, and frontotemporal dementia, though dementia can also result from stroke, HIV infection, harmful alcohol consumption, repeated brain injuries, or nutritional deficiencies.10–12
Population ageing, initially occurring in high-income countries, is now happening in low- and middle-income countries. By 2050, two-thirds of the world's population over 60 years will live in these countries. 13 The World Health Organization estimates that between 2015 and 2050, the percentage of people aged 60 or older will nearly double, from 12% to 22%, and the number of people aged 80 or older will triple, reaching 426 million. By 2050, 80% of older adults will live in low- and middle-income countries, which will place a heavy burden on healthcare systems due to the rise in chronic diseases. 14
The latest descriptive epidemiological research on dementia allows for the investigation of changes in prevalence and incidence over time. A review of 14 studies examining trends in dementia prevalence and incidence in Sweden, Spain, the United Kingdom, the Netherlands, France, the United States, Japan, and Nigeria indicates stable or declining dementia rates, with some studies providing evidence of sex-specific changes with a multifactorial etiology, considering significant social changes and improvements in living conditions, education, and healthcare. 15
The 2017 Lancet Commission identified nine modifiable risk factors for dementia: lower educational attainment, hypertension, hearing impairment, smoking, obesity, depression, physical inactivity, diabetes, and low social contact. 16
Each year, demographic indicators in Latin American and developing countries converge, and the expected prevalence of dementia in the former now surpasses that in the latter. 17 Dementia has been declared a global challenge; however, regions worldwide show differences in both the nature and magnitude of this challenge. 18 The strategies, procedures, and tools to address ageing in general, and dementia in particular, have fallen short of the international call to tackle this medical-social issue. 19
Much remains to be done to achieve the goal of “living well with dementia” set out in the World Alzheimer Report 2016 20 because, as in many countries, Ecuador faces pronounced fragmentation in long-term healthcare, along with inadequate and poor quality of care, as well as limited coverage of basic support for individuals with dementia and their caregivers. Relatively little attention is given to systems and services that provide healthcare to people with dementia, with coverage not exceeding 10–15% of the total population. 21
Globally, diagnostic coverage is low. Only between 40% and 50% of people living with dementia have received a diagnosis. 22 In low- and middle-income countries, there are few available estimates, but current data suggest a diagnostic coverage of between 5% and 10%, 23 limiting strategies for healthcare and social planning throughout the course of the disease.
Studies conducted with samples from large cities reveal significant diversity among subjects, including individuals from rural areas with different cultural backgrounds, educational systems, and professional activities with varying levels of demand. 24 The assessment of subjects with similar backgrounds and socioeconomic, cultural, and environmental factors enables the observation of cognitive impairment prevalence and the effect of schooling, although such studies are rarely conducted. 25
The demographic structure of Latin America presents multiple unique challenges as its indicators are rapidly approaching those of developing countries; furthermore, fertility rates and their relative decline have been uneven in Latin America and the Caribbean. 26 However, the understanding of relevant factors for dementia is currently limited. 27 A high proportion of people with dementia in the region lack basic support. 28
In 2010, 10.6% of the Ecuadorian population consisted of children under five years of age, marking a 2.4% decrease in this age group compared to the previous decade. By this time, the population structure exhibited a broad-based pyramid characteristic of developing countries, with approximately 1.2 million people over the age of 60 and about 160,000 individuals aged 80 or older. Life expectancy at birth was 77.9 years for women and 72.3 years for men, with an average of 75 years. 11 Currently, Ecuador has slightly over 16 million inhabitants, and by 2050, it is expected that only 5.8% of the population will be under five years old, while 30% will be over 60 years of age. 29
The purpose of this study was to determine the epidemiological and demographic factors associated with dementia in the Ecuadorian population. Addressing this issue is essential, as understanding the epidemiology, risk factors, and socioeconomic impact will enable the design of interventions that improve the quality of life of those affected and alleviate the burden on their families and the healthcare system.
Methods
Population, sample, and type of study
This was an observational, correlational study with a quantitative approach. Anonymized data were obtained from the registry of outpatient care at the Institute of Neurosciences of Guayaquil (INSG) between January 1, 2010, and December 31, 2022. A total of 125,458 outpatients across various medical specialties and conditions were analyzed.
The study variables included demographic factors (age, gender, region of residence, level of education, and marital status) and epidemiological factors (distribution, prevalence, incidence, burden of disease, and comorbidities).
Inclusion and exclusion criteria
Patients with a diagnosis established by the International Classification of Diseases (ICD-10) of some type of dementia during their first medical care (n = 4485) were included. Cases with incomplete or inconsistent data (n = 619) were excluded, leaving a final sample consisting of 3866 records.
Procedure
This study was based on the analysis of an anonymized outpatient database from the INSG. Patients in the database were initially classified according to their primary clinical diagnosis, specifically targeting dementia, to ensure accurate categorization. Following this, subjects’ eligibility was verified against the study's predefined selection criteria. Data curation involved the removal of missing, duplicate or inconsistent entries.
Statistical analysis
To determine the prevalence of dementias, the following formula was used: (Number of cases of the disease / Total number of cases)×100. The incidence rate (IR) was calculated by dividing the number of new cases from 2010 to 2022 (n = 3866) by the total person-time at risk (125,458 patients × 13 years) and multiplying the result by 1000 to express the IR per 1000 person-years.
The estimation of disease burden for patients with dementia was conducted using Disability-Adjusted Life Years (DALY), a measure that combines both Years of Life Lost (YLL) due to premature death and Years Lived with Disability (YLD). The YLL metric was calculated as the number of deaths (D) multiplied by life expectancy at the age of death (L), where YLL = D × L. The YLD metric was calculated as the product of the number of new cases (I), age of onset (A), duration of the condition (T), and disability weight (DW), where YLD = I × A × T × DW.
The extracted information was exported to SPSS® v.26, Jamovi® v.2.3.28, and Epidat® v3.1 statistical packages for analysis. The results are presented in tables and figures showing absolute frequency, relative frequency, and epidemiological measures. Non-parametric tests (Chi-square and Cramer's V) were used to examine the relationship between dementia, demographic variables and comorbidities.
Setting
The INSG, Ecuador, provided the data analyzed in this study. The database included outpatient records collected as part of routine care at the institution. The INSG is the largest of the three specialized psychiatric hospitals in Ecuador, with 121 hospital beds for managing mental health crises. Its outpatient clinic offers an average of 6000 visits monthly across various specialties (psychiatry, psychology, neurocognitive rehabilitation, and neurology). During the study period, 400 new cases were diagnosed annually in the coastal region, each receiving an average of 8 annual visits. Due to issues of distance and transportation costs, the Sierra and Amazonia regions use our services less, with 9 new cases annually in the former, receiving more than 90 visits per year, and 6 new cases per year in the latter, receiving psychiatric care once annually on average. The INSG uses a systematic, multidisciplinary approach to diagnosing mental illness and dementia. However, in many cases, diagnoses are based on symptom profiles and family reports due to limited service access, which restricts specific diagnostic accuracy in cases with dementia and explains why most treated patients with this pathology are classified as non-specific.
Results
A total of 3866 records of new cases of dementia treated in the outpatient clinic of the INSG during the period 2010–2022 were included. The median age was 79 years, with an interquartile range of 13, and participants’ ages ranged from 45 to 104 years. A higher number of dementia cases were found in women (n = 2285), representing 59.1% of the analyzed records (Figure 1).
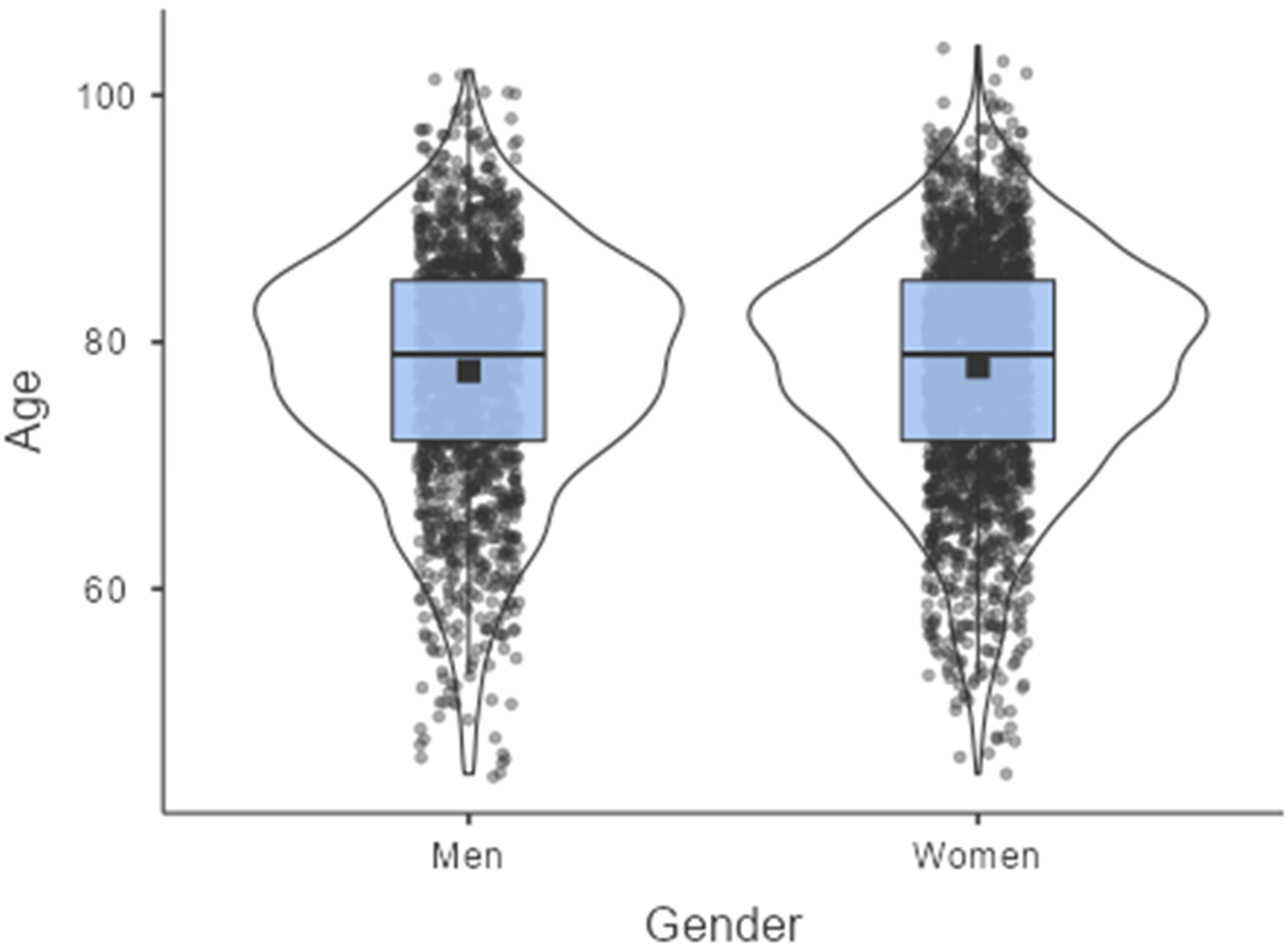
Distribution of dementias treated at the INSG by age and sex, 2010–2022. n men = 1581; Median = 79 years. n women = 2285; Median = 79 years.
Most cases attended were from the Coastal region (n = 3734; 96.5%), primarily from the province of Guayas (n = 3005; 77.7%). The educational level distribution showed a majority with primary schooling (n = 789; 46.3%), followed by secondary education (n = 714; 18.5%), with a significant percentage of illiterate individuals (n = 554; 14.3%). Marital status indicated 39.9% single (n = 1544) and 32.6% married (n = 1261). Table 1 presents the complete results of the demographic variables analyzed.
Characteristics of the population with dementia treated in the INSG 2010–2022.

f: frequency; %: percentage.
A predominance of unspecified dementias (62.6%) was observed, followed by Alzheimer's disease dementia (20.8%), vascular dementia (13.4%), and dementia linked to other diseases (3.2%). The prevalence of dementia among patients treated at INSG was 3.1% (1.3% in men, 1.8% in women), with an IR of 2.4 per 1000 person-years, varying notably over the study period. In 2014, dementia cases increased by 77.34% from 2010, coinciding with the introduction of government health policies and agreements that allowed INSG to see more patients. Higher incidences of unspecified dementia cases in 2021 and 2022 likely reflected the post-COVID-19 period, where cognitive assessment was handled online with limited access to appropriate assessment tools. Figure 2 presents the number of cases by year for each type of dementia.

Incidence of dementia 2010–2022, according to ICD-10 classification. The number of new cases for each type of dementia from 2010–2022.
The burden of disease, representing the loss of healthy life years due to death, illness, or injury, indicated that DALYs reached 242,184 years, with a greater burden on women (DALYs = 141,969 years). Table 2 presents the main indicators of the dementia burden in 2021.
Annual burden of dementia in the INSG, 2021.

YLL: years of life lost due to premature death; YLD: years lived with disability; DALY: disability-adjusted life years.
It is important to note that 6.4% of patients with dementia have one or more comorbidities. Among the main comorbidities, mental and behavioral disorders are the most frequent (54.5%), followed by hypertension (14.5%) and nervous system diseases (14.5%). Table 3 lists the top 10 comorbidities of patients with dementia seen in the INSG's outpatient clinic.
Comorbidities of dementias 2010–2022. INSG.

f: frequency; %: percentage.
The results of the bivariate analysis showed statistically significant associations between dementia and age, gender, level of education, and marital status. Additionally, a significant association was observed between dementia and some comorbidities (behavioral disorders, nervous system diseases, and hypertension). These results can be found in Table 4.
Results from the Chi-square analyses.

χ2: Chi-square; p: asymptotic significance; V: Cramer's V; *Significant association.
Discussion
Dementia represents a significant challenge for both public health and society, affecting millions of people worldwide 30 and imposing an economic, emotional, and physical burden on healthcare systems and caregivers. Due to population ageing, the number of dementia cases is rapidly increasing globally, particularly in low- and middle-income regions, where approximately 60% of cases are concentrated. 31 This phenomenon is driven mainly by rising life expectancy and an ageing population, factors that increase the incidence of dementia, especially Alzheimer's disease, which accounts for 60–70% of dementia cases.32–34
The situation in Latin America and the Caribbean is alarming, as these regions experience a faster growth in dementia prevalence compared to others. 31 In this study, based on 3866 cases seen at the INSG, most diagnosed patients had a median age of 79 years, aligning with similar population studies that indicate an increased dementia risk with advancing age. 35 Statistics reported by Custodio et al. 36 in Latin America show higher incidence rates than those found in this study, which could be related to demographic factors specific to Ecuador as well as to limitations in diagnostic access in certain parts of the country.
Research on dementia across different contexts has revealed significant variations in the incidence and prevalence of the disease based on gender, educational level, and healthcare access. Findings in European and Asian populations, for example, show a generally higher prevalence among women than men, a trend also observed in this study in Ecuador, where a higher prevalence in women is recorded. 36 These differences may be explained by women's greater longevity and by sociocultural factors that influence the risk of developing dementia. 37
Data from this study also emphasize the importance of educational level as a relevant risk factor for dementia incidence. Research indicates that individuals with lower educational levels exhibit a higher dementia prevalence compared to those with higher education. 38 This may be linked to the concept of cognitive reserve, which suggests that greater cognitive stimulation throughout life can protect against cognitive decline in old age. 39 According to Parra et al., 40 Latin American countries face specific challenges due to limitations in health infrastructure and policies, which affect effective prevention and management of dementia in the region.
Marital status and social support emerge as factors that influence the prevalence and progression of dementia. Studies in various populations have indicated that single, divorced, or widowed individuals have a higher risk of developing dementia compared to those who are married. 41 This social vulnerability, combined with a lack of family support, can impact the quality of life of individuals with dementia and their disease management. In Ecuador, a high percentage of the cases analyzed involved individuals without a partner, which could indicate a greater risk and a reduced capacity to face the challenges of the disease.
An important aspect identified in this research is the impact of comorbidities on dementia patients. 42 The presence of mental disorders, hypertension, and nervous system diseases is associated with faster functional decline and reduced quality of life in individuals with dementia. 3 Multimorbidity complicates clinical management and increases associated costs, which has significant implications for the Ecuadorian health system and underscores the need for a comprehensive approach to the care of these patients.
Globally, evidence suggests that a significant portion of the Alzheimer's disease burden could be prevented by modifying risk factors such as hypertension, obesity, physical inactivity, and low educational attainment. 43 In the Ecuadorian context, these interventions could have a notable impact on reducing the burden of dementia, especially if preventive strategies address both biological and social factors. The study by Lanctôt et al., 10 which identified a high prevalence of unspecified dementias, highlights the need to improve diagnostic precision in primary care to provide more effective and targeted care tailored to patients’ individual needs.
This analysis highlights the importance of addressing dementia from a multidimensional perspective that considers both early diagnosis and clinical management, as well as public education and awareness about modifiable risk factors, particularly due to its complex etiology, progressive nature, and strong association with other chronic conditions that compound individual and societal burdens.42,44,45 In Ecuador, the prevalence of dementia at the INSG stands at 3.1%, notably lower than in countries such as Cuba, where prevalence among individuals over 65 ranges from 10.8% to 26%, and in Peru, with a prevalence of 6.85%.46–49 The variability in prevalence rates across Latin America is also observed in countries like Mexico, where rates as high as 10.88% have been reported in the metropolitan area of Monterrey for those over 65. 50 The incidence in Ecuador, at 2.4 per 1000 person-years, is also low compared to regional studies in Latin America, which report rates up to 18.4 per 1000 person-years. 36
These differences may be explained by demographic factors and disparities in healthcare access. Globally, low- and middle-income countries, where 58% of people with dementia reside, face a disproportionate burden from this condition, a situation expected to worsen in the coming decades. 11 One additional important source of difference may stem from difficulties in recognizing the need for care among family members with significant cognitive decline, particularly since diagnostic and care services are often charged to patients. In this context, it is essential for Ecuador to consider these disparities when implementing public health strategies.
Although this study does not closely analyze dementia-predisposing factors in the Ecuadorian population, the demographic and pathological description of the studied population allows us to outline a profile for this type of patient in Ecuador. Unfortunately, our data is limited to a specific region of the country, and thus, studies involving a more demographically diverse population are needed to adequately represent the situation across Ecuador's various regions, particularly given the country's rich cultural diversity and significant regional variations. Similarly, the disproportionately high number of unspecified dementia diagnoses greatly limits the identification of causes and the development of a more specific dementia profile for Ecuador. This latter situation also reveals an even more concerning aspect of the mental health system: the limited access to advanced diagnostic methods, which, in turn, impacts the ability to provide targeted treatment for this condition.
Conclusions
This study highlights the growing prevalence and incidence of dementia in Ecuador, emphasizing the need for targeted prevention and intervention strategies, particularly in high-risk groups such as older adults, women, and individuals with lower education levels or limited social support. The observed association between dementia and factors such as age, education, marital status, and comorbidities underscores the complexity of dementia as a public health issue and the necessity of a multidimensional approach in managing it. The study's findings are particularly relevant for Ecuador and similar low- and middle-income countries, where access to healthcare and diagnostic precision can be limited. By identifying demographic and social risk factors unique to the Ecuadorian population, this study provides valuable insights for policymakers and health professionals, paving the way for more effective, context-sensitive dementia diagnosis, prevention and care strategies. Given the anticipated rise in dementia cases across Latin America, addressing modifiable risk factors through public health initiatives and improving diagnostic capabilities are crucial steps towards mitigating the burden of dementia and enhancing quality of life for affected individuals and their families.
Footnotes
Ethical considerations
The study complied with the ethical principles of the International Ethical Guidelines for Health-Related Research with Human Subjects and was approved by the Human Research Ethics Committee of the Catholic University of Cuenca (CEISH-UCACUE), with code CEISH-UCACUE 2024-011.
Consent to participate
Consent to participate was waived for this retrospective study as it involved the use of anonymized data obtained from existing records, in accordance with ethical guidelines and institutional regulations.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding for the publication of this article was provided by Universidad Politécnica Salesiana, Cuenca, Ecuador.
Declaration of Conflicting Interests
The authors declare that they have no competing interests.
Data availability statement
The dataset generated during and/or analyzed during the current study are available here: https://1drv.ms/x/c/dc91ec295e860be6/EeYLhl4p7JEggNykIwAAAAABgnhItp-y-HDnfqNzdINXSQ?e = ![]()