
Abstract
Alzheimer's disease (AD) research increasingly emphasizes accessible biomarkers for early detection. Lactoferrin, an iron-binding glycoprotein present in saliva, has been associated with AD pathology with mixed results. In this pilot study, saliva samples from 17 middle-to-older-aged Black and non-Hispanic White adults at risk for AD were measured. After adjusting for demographic variables, salivary lactoferrin (sLF) concentrations correlated significantly with Digit Span Memory Test scores (p = 0.013) and modestly with visuospatial performance (p = 0.194), with no racial differences observed. These preliminary results support further large-scale studies to assess sLF as a potential noninvasive biomarker for AD.
Keywords
Introduction
Alzheimer's disease (AD) is the 7th leading cause of death in the United States, and assessing risk and developing preventive measures are a top priority for healthcare research.1,2 Neuropathological changes linked to AD emerge many years before cognitive symptoms emerge. 3 Therefore, the presymptomatic disease stage provides a crucial window of opportunity both to understand the mechanisms through which AD evolves from pathogenesis to clinical symptoms and to potentially implement interventions before symptom onset.
Imaging technologies such as positron emission tomography and magnetic resonance imaging and biomarkers in cerebrospinal fluid (CSF) and plasma, specifically amyloid-β (Aβ42) and phosphorylated tau (p-tau), are used to diagnose AD and guide clinical decisions throughout disease progression. 4 Currently, imaging equipment, blood draws, and lumbar punctures require trained staff, timely processing, and expensive equipment. 5
Saliva represents a cost-effective, non-invasive, and easily collected by non-specialized research staff alternative that is likely more attractive to patients, research participants and clinical investigators. 6 Traditional AD biomarkers (total tau, neurofilamentlight chain, and Aβ) have been studied with conflicting results as potential salivary biomarkers.7–9 However, other AD risk factors, including oxidative stress and inflammation, and as we report here, lactoferrin (Lf), may hold promise as reliable salivary biomarkers.10,11
Lf is an iron-binding antimicrobial glycoprotein that can be found in most biological fluids. 12 It was first isolated from bovine milk in 1939 and, more recently, it was described as a key nutrient for neurodevelopment and cognitive function during early periods of rapid brain growth.13,14 Animal studies show that Lf can ameliorate mitochondrial dysfunction and reduce neuroinflammation.15,16 Moreover, Lf administration significantly improved spatial cognition in aged mice and reduced amyloid burden, including Aβ40 and Aβ42 in brain homogenates.17–19 In saliva, Antequera et al. reported a significant early and robust decrease in salivary lactoferrin (sLF) in six- and twelve-month-old APP/PS1 mice that was not seen in their age-matched wild-type counterparts. 20
Lf is highly expressed in cortical tissue affected by AD pathology, specifically in senile plaques composed of aggregated Aβ, extra- and intracellular neurofibrillary tangles, and glial cells of AD patients. 21 Five clinical studies have investigated sLF in relation to AD, with mixed results. In an observational study among 116 patients with mild cognitive impairment or AD, Carro et al. described that sLF correlated with Mini-Mental State Examination scores and AD CSF biomarkers Aβ42 and total tau. Moreover, sLF levels were able to differentiate healthy controls from participants with mild cognitive impairment/AD.22,23 Another observational study by the same group showed a negative correlation between sLF and cortical Aβ load and middle temporal cortex thickness. 24 To date, one pilot clinical trial with sLF in 50 AD patients showed improvements in serum Aβ42, p-tau181, and inflammatory markers interleukin-6 and interleukin-10, after daily intranasal administration of Lf for three months. 25 While these studies describe promising results, Gleerup et al. found no relationship between sLF and AD biomarkers in CSF and described no difference in sLF between subjects with AD and controls. 26 Potential reasons for conflicting results include indiscriminate participant selection, exclusion criteria, and fasting versus non-fasting sample collection, which we further explain in the discussion. No previous study has investigated sLF in a population of cognitively healthy participants at an increased risk of AD, which could highlight whether sLF is dysregulated preclinically.
No previous study has investigated potential racial differences in sLF levels. Black Americans (BA) are 64% more likely than non-Hispanic whites (NHW) to develop Alzheimer's disease and related dementias (ADRD). 27 However, BAs are also 35% less likely to be diagnosed with ADRD, which often results in increased disease severity and worse prognosis by the time a BA individual seeks treatment. 28 Our group and others have shown that AD and inflammatory biomarkers can significantly differ by race.29,30 These race-related disparities in AD incidence and prevalence, coupled with the demand for non-invasive and cost-efficient biomarkers to diagnose and treat AD, underscore the need to involve diverse clinical research populations.
We investigated the potential relationship between sLF and a comprehensive battery of cognitive tests in a cognitively normal cohort of NHWs and BAs at high risk for AD by virtue of parental history. Our hypothesis was that lower levels of sLF would correlate to worse cognitive performance, particularly in the domains of memory and visuospatial cognition.
Methods
This pilot project was a sub-study of a larger NIH/NIA-funded two-year observational study among cognitively normal, high risk middle-aged adults (PI: Wharton R01AG066203). Recruitment and cognitive testing were conducted by trained clinical staff, while sLF collection, processing and analysis were conducted independently (PI: Hammerschlag). Data presented here was collected between October 10, 2022 and March 24, 2023 and all procedures were approved by the Emory Institutional Review Board (IRB).
Participants taking part in the larger study were invited to participate in this optional salivary collection sub-study during their scheduled annual study visit. We enrolled 17 middle to older-aged (age = 60.29 ± 9.7 years) cognitively normal participants with a biological parent with either autopsy-confirmed or probable AD as defined by NINCDSADRDA criteria and medical records when available. 31 Demographic variables were summarized using descriptive statistics (Supplemental Table 1). Participants completed a 90-minute cognitive battery detailed in the Supplemental Material.
Results
We analyzed saliva samples and cognitive test data from 14 subjects out of the 17 subjects enrolled (reasons for exclusion in the Discussion section). Supplemental Table 1 shows sample characteristics. Participants were cognitively normal, middle to older-aged, and at risk for AD. Half of subjects enrolled in this pilot study were BAs and we analyzed race as a potential modifying variable for sLF levels. Age, sex assigned at birth, and years of education were not significantly different between BA and NHWs. Those same variables were used as controls for correlation analyses of sLF and memory.
We found a significant correlation between sLF and the Digit Span Memory Test (DSMT) scores (Pearson's r = 0.607; p = 0.013; Figure 1). The measured level of significance stands after adjusting for age, sex, race, and years of education (p = 0.016). Data show that higher sLF levels were associated with better DSMT performance.

Digit Span Memory Test scores as a function of sLF concentration. We performed a bivariate Pearson's correlation and found a positive relationship (p = 0.013).
We found a positive correlation approaching significance between sLF and MRT score (Pearson's = 0.342; p = 0.194; Figs. 2 and 3). The MRT is used as an assessment of the ability to imagine spatial transformations of objects. 32 Data suggests that a lower level of sLF is related to worse spatial cognition. As expected, no relationships between other cognitive domains and sLF were observed.
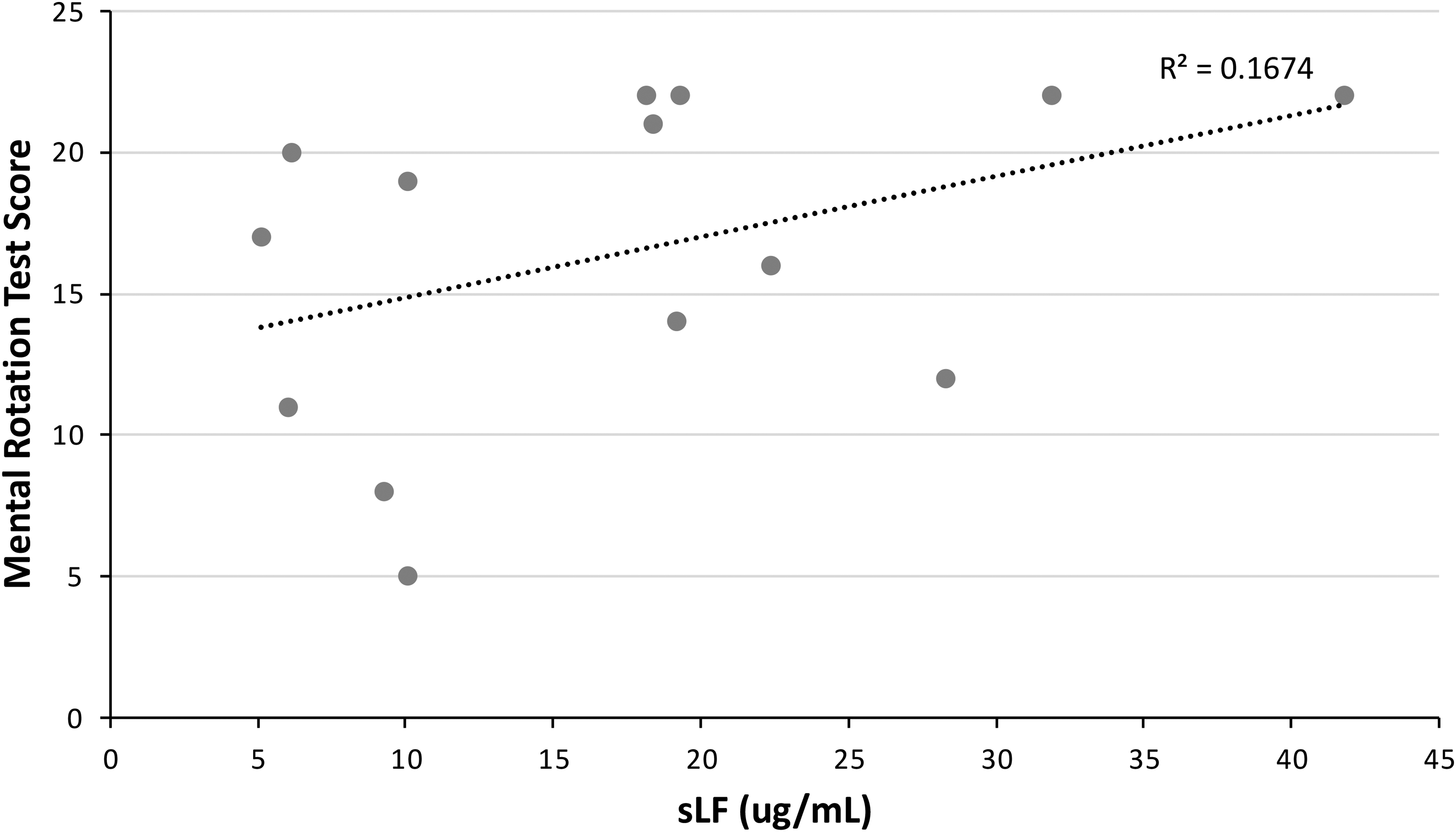
Mental Rotation Test scores as a function of sLF concentration. We performed a bivariate Pearson's correlation, and a found a trend that is approaching significance (p = 0.194).

Average sLF levels in Black American and non-Hispanic white participants. There appears to be no significant difference between both groups.
We found no significant difference in average sLF concentration between BAs and NHWs. While each group is composed of only 7 subjects, the average difference is only of ∼5%, as BAs had an average sLF concentration of 18.2 μg/mL and NHWs an average of 19.2 μg/mL.
Discussion
Conflicting results concerning the potential relationship between sLF and AD pathology and clinical symptomatology have been reported.22,23,26 The purpose of this pilot study was to assess the potential relationship between sLF and targeted cognitive test performance in a diverse cohort of cognitively normal individuals at risk for AD by virtue of parental history. Secondarily, we explored whether sLF levels differed by race.
A parental history of AD can significantly increase the risk of developing AD. 33 By identifying biological markers that are correlated with early cognitive changes in healthy but at-risk individuals, we can both increase early detection measures and potential for treatment, as well as elucidate the complex biological processes that drive cognitive decline. Enrolled participants in this study were specifically chosen because they are at increased risk due to parental history, while still cognitively normal and in their middle age—the optimal time to stage an intervention before the neuropathological cascade begins.
Despite our small sample size, we observed a correlation between sLF and memory and visuospatial ability. Cognitive tests were selected based on our prior research showing that they are able to detect subtle cognitive decline in a middle-age, high risk cohort.29,34 Memory concerns and decline in visuospatial ability (i.e., spatial navigation) are signs of cognitive decline and are classic symptoms of AD.35,36 Therefore, these results suggest a possible protective effect of Lf toward cognitive areas typically affected by AD. Moreover, evidence from animal studies and Lf suggests a domain-specific relationship between visuospatial ability and Lf. 17 This study suggests a similar relationship in humans—one that, to our knowledge, has not been described before. Because deficits in visuospatial ability are common in AD patients, and our group and others have reported changes in visuospatial ability suggestive of preclinical cognitive decline, additional research is warranted.36,37
To our knowledge, no previous clinical study or trial has investigated potential racial differences in sLF levels. Our laboratory and others have reported that traditional AD and inflammatory biomarkers can differ based on race, and scientific consensus largely supports inclusion of racially diverse cohorts for this reason. 29 38–41 A validated AD biomarker that does not differ according to race could allow for better standardization and clinical implementation, and measuring it in a more accessible matrix such as saliva could mitigate significant barriers to risk assessment and diagnosis in underdiagnosed racial minorities, such as BAs. 42 In this study, we showed that there are no significant differences in sLF between BAs and NHWs, which is encouraging in the search for cost-effective and non-invasive AD biomarkers validated for use in a diverse population. Our results, which should be validated in other studies with larger sample sizes, suggest that sLF has potential as a biomarker in adults predisposed to AD regardless of race.
Our results may explain the conflicting sLF results previously reported and discussed above.22,23,26 One explanation is the reproducibility of saliva biomarkers, which can be sensitive to external stimuli and be affected by oral hygiene. 5 While this is certainly a possibility, as is the case with virtually all biomarkers, we propose a possible alternate explanation for the discordance between the two groups: Gleerup et al. measured sLF levels in non-fasted participants, whereas both Carro et al. and Gonzalez-Sanchez et al. asked participants to fast overnight.20,21,24 Lf is found in widely available food items such as meat, cheese, and milk, so food intake directly before saliva collection could alter baseline concentrations. 43
We asked the 17 enrolled participants to fast overnight prior to their study visit; however, three participants reported having eaten prior to their scheduled saliva collection and were therefore excluded from analysis. While not included in our main study results, the sLF concentrations of these three samples were surprising: they were four standard deviations higher than the average concentration measured in all other participants included in this study. These post-hoc analyses suggest the importance of fasting before sLF collection and underscore the possible impact of methodological differences on the results described by Gleerup et al. (non-fasted participants) and Carro et al. and Gonzalez-Sanchez et al. (fasted participants). Controlled studies investigating the interaction between fasting and sLF levels are needed to confirm this.
A limitation of this pilot study is its small sample size and that the data presented are correlational and not causal. While inferences can be made about the validity of the protein as a biomarker for AD, results should be taken as preliminary and should be replicated in further studies.
Our research group will continue collecting saliva samples in ongoing studies and trials, with the aim of furthering the knowledge and statistical power of the conclusions reached in this pilot study. It is imperative to have easily accessible, disease-specific biomarkers that can be clinically useful for determining risk, facilitating diagnosis, and assessing disease progression.
Supplemental Material
sj-docx-1-alr-10.1177_25424823251409391 - Supplemental material for Pilot: Salivary lactoferrin as a potential preclinical Alzheimer's disease biomarker
Supplemental material, sj-docx-1-alr-10.1177_25424823251409391 for Pilot: Salivary lactoferrin as a potential preclinical Alzheimer's disease biomarker by Bruno L Hammerschlag, Brittany Butts, Kelly DS Likos, Danielle D Verble, Nivi Nimmagadda and Whitney Wharton in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
We deeply thank all participants who volunteered to make this study possible.
Ethical considerations
All procedures were approved by the Emory University Institutional Review Board.
Consent to participate
All participants signed an informed consent form.
Consent for publication
Not applicable
Author contribution(s)
Funding
This project was supported by an Independent Research Grant provided by the Emory University URP Research Partners Program, and the National Institute of Health (NIH) National Institute on Aging, and the Alzheimer's Association. Principal Investigator: Whitney Wharton, PhD, Associate Professor, Nell Hodgson Woodruff School of Nursing & Department of Neurology, School of Medicine, Emory University, Atlanta, Georgia, USA.
Alzheimer’s Association, National Institute on Aging,
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.