
Abstract
Background
As China's population ages, the burden on caregivers of individuals with Alzheimer's disease and related dementias (ADRD) is increasing. Comprehensive nationwide studies on caregiver burden, particularly emotional experiences, however, remain limited.
Objective
To investigate the multidimensional aspects of caregiving burden associated with ADRD patients through a nationwide survey.
Methods
This cross-sectional study included 1221 ADRD patient-caregiver pairs from 29 province-level administrative divisions in mainland China, recruited through dementia-dedicated online forums. The multidimensional aspect of caregiver burden, including physical, mental, familial, emotional, and quality-of-life impact, as well as attitudes toward caregiving and needed supports, was measured using a self-reported assessment.
Results
Patients had a median age of 66 years, with 33% classified as young-onset dementia (YOD). Caregivers were predominantly younger (median age: 30), employed (96.6%), and male (59.8%). Most reported moderate-to-severe physical (24.2%), mental (31.0%), family life (29.2%), and quality-of-life (47.2%) burden, with high emotional strain (ambivalence: 66.7%; grief: 59.8%; guilt: 57.7%). Independent predictors of burden included patient mood, caregiver emotional states, and caregiving extent, while financial stability and positive caregiving attitudes were identified as protective factors. Caregivers prioritized financial aid (25.1%), additional helpers (19.7%), and psychological support (16.7%).
Conclusions
This nationwide study highlights the multidimensional burden faced by ADRD caregivers in China. Predominantly younger, employed, and male caregivers reflect shifting sociocultural dynamics. The high prevalence of YOD adds complexity to caregiving demands. Our findings underscore the need for evidence-based individualized support mechanisms, such as psychosocial and workplace interventions, to alleviate caregiver burden in China.
Introduction
Dementia is an umbrella term for several neurodegenerative diseases that impair memory, thinking, and the ability to perform daily activities. An estimated 57 million people worldwide were living with dementia in 2021. 1 The most common forms of dementia are Alzheimer's disease and related dementias (ADRD), including vascular dementia, Lewy body dementia, frontotemporal dementia, and mixed dementia. Alzheimer's disease (AD) alone accounts for 60–70% of all cases. 1 While ADRD share many cognitive and pathological features, they are often clinically indistinguishable. 2 The absence of effective prevention and treatment strategies has imposed a tremendous burden on people living with dementia (PLWD) and their caregivers worldwide. 3 This burden is especially pronounced in China, where dementia prevalence is the highest globally and continues to rise rapidly.4–6
Understanding caregiver burden has profound implications for both caregivers and care recipients. Studies have shown that high caregiver burden could lead to poor outcomes in care recipients, i.e., diminished quality of life, an increased risk of unmet care needs, and a higher likelihood of institutionalization.7,8 Caregivers are also subject to the negative impacts of caregiving, such as poor sleep quality, chronic fatigue, poorer quality of life, behavioral disturbances, accelerated functional decline, immune dysfunction, increased cardiovascular risk, depression, and anxiety.9–12 Strained caregiving relationships may lead to interpersonal tensions, reduced communication, resentment, and a greater risk of elder mistreatment.13–15
Caregiver burden is shaped by the characteristics of care recipients, caregivers, and the caregiving context. 16 Factors related to care recipients, such as the type of dementia, extent of personality change, presence of behavioral disturbances, behavioral and psychological symptoms of dementia (BPSD), or severe cognitive impairment, and functional dependence, can consistently increase caregiver stress and workload.9,17,18
Caregiver factors, including age, gender, education level, socioeconomic status, physical health, coping resources, and relationship to the care recipients, also play a central role; for example, women, older spouses, and low-income caregivers experience disproportionately higher burden. 19
The caregiving context, defined as the environment and circumstances in which care occurs, includes cultural expectations (e.g., filial piety), availability of formal services, financial strain, living arrangements, and social support networks. 16 Caregiving context affects the caregiver's ability to provide effective care. 19
A range of interventions, such as psychosocial, lifestyle, and multicomponent interventions, respite care, and skills-training programs, have been shown to mitigate the burden caregivers face, although their effectiveness varies across settings.20–22 In China, access to these interventions remains limited due to regional disparities, shortages of trained personnel, and low public awareness. 19 Moreover, caregiver needs in China are highly heterogeneous because of geographic and cultural differences, socioeconomic inequities, and uneven development of dementia-care services across provinces. 19 Existing evidence on dementia caregiver burden in China largely comes from studies with narrow geographic coverage, small sample sizes, or a primary focus on psychological symptoms, such as anxiety and depression,23–25 thus leaving evidence-based interventions lagging behind the diverse and evolving needs of caregivers.
To address this evidence gap, the present study investigated dementia caregivers across China through the QQ platform (a leading multipurpose social media and communication application in China) to describe caregivers, their care recipients, and caregiving context, and assess multidimensional (physical, mental, family life, quality of life, and emotional) burden, the determining factors, and support needs.
Methods
Study design and population
This study was a cross-sectional, self-administered, anonymized online survey with caregivers of ADRD in China and reported in accordance with the CROSS (A Consensus-Based Checklist for Reporting of Survey Studies). 26
Survey instrument development
A survey questionnaire with 57 question items across four domains—ADRD patient characteristics, caregiver characteristics, caregiving context, and caregiver burden—was self-developed based on the current literature and focus group interviews with ADRD patients and their caregivers from a local community hospital. The caregiver burden domain was designed as a multidimensional construct—physical health, mental health, family life, and overall quality of life (QoL), and evaluated using a single 5-point Likert scale (1 = none to 5 = severe) for each construct. Emotional experiences, adapted from “The Emotional Side of Caregiving” by Family Caregiver Alliance, 27 were evaluated with Yes/No questions accompanied by descriptive examples (e.g., “Guilty: You feel guilty for not being able to help or prevent the patient`s condition? [Yes/No]”) (See the Supplemental Material for details).
The content of the survey was developed in English; validated for the content (content validity) by two experts; translated into Chinese using forward-backward method and validated for translation accuracy and cultural appropriateness (translation validity), and the wording, layout, clarity of instructions, answerability, and response latency (face validity) by two bilingual investigators and a small group of college students (n = 6); and revised as needed. A group of volunteer caregivers (n = 17), identified through one local hospital, was invited to a pilot test for the functionality of the instrument, the accuracy and pattern of responses, and the cause of missing data before finalizing the instrument (see the Supplemental Material for the English version of the survey).
Participant recruitment
ADRD patient/caregiver pairs across mainland China were recruited by distributing a survey poster containing a QR code to four caregiver forums (each with 200–500 members) hosted on the popular social media platform QQ. These forums are specifically designed to support caregivers of individuals with ADRD.
Survey administration
The survey was available on the Chinese survey hosting website, Sojump (www.wjx.cn), from August to September 2022. To incentivize participation, we offered a small monetary reward (5 RMB or 0.7 US$ per questionnaire) along with self-designed educational e-brochures (https://mp.weixin.qq.com/s/r3sgDG7Ci5TPOEq9S_0k8Q; https://mp.weixin.qq.com/s/wK5RiUoAbRoBT2mtrd7nmQ; and https://mp.weixin.qq.com/s/wbEYTeuFgP-2xDkqhN6MZg) accessible via a WeChat official account for valid surveys. Reminders were sent to the QQ groups to improve response rates.
Data management and analysis
The survey data were imported from the survey hosting site into an Excel database. A total of 1409 submitted surveys were screened, and 188 were excluded for repeated IP addresses. Missing data, such as the duration of the caring period or inconsistent responses (e.g., full-time administrative staff claiming to provide daytime patient care), were assumed to be “missing completely at random (MCAR)” and recorded as NA (not available). Only valid questionnaires (N = 1221) were included for data analysis.
SPSS (version 30.0) was used for data analysis. Normally distributed continuous variables, such as caregiving time, and Likert items, such as burden on physical and mental health, family life, and the overall QoL, which were treated as continuous variables, were analyzed by the T-test for two groups and ANOVA for more than two groups, and reported as mean (SD). Non-normally distributed continuous variables, such as the ages of caregivers and their care recipients, were analyzed using the Mann-Whitney U test for two groups and the Kruskal-Wallis test for more than two groups and reported as median (IQR). Categorical variables, such as sex, family structure, financial status, roles and responsibilities, and emotional experiences, were analyzed using the Chi-square test and reported as n (%). Multiple linear regression was conducted to identify factors associated with multidimensional caregiving burden. Only variables with statistically significant association or correlation in preliminary analyses were included in the final regression models.
Two-tailed p-values < 0.05 were considered statistically significant.
Results
A total of 1221 ADRD patient/caregiver pairs from 29 province-level administrative divisions, including 25 provinces and 4 direct-administered municipalities, of mainland China were included in the study.
Demographics of patients with ADRD
As shown in Table 1, females accounted for 51.8% (632/1221) of patients. The median (range) age of patients was 65 (40–98) years. Age group distribution was 40–54 years (8.2%), 55–59 years (11.2%), and 60–64 years (13.6%); alternatively, 40–64 years (33.0%) and 65–98 years (57.7%), with age data missing in 9.3% (data not shown). The duration since diagnosis of dementia varied widely, with a median of 30 months (IQR: 18–44 months).
The characteristics of patients with Alzheimer's disease and related dementias (ADRD)a (N = 1221).
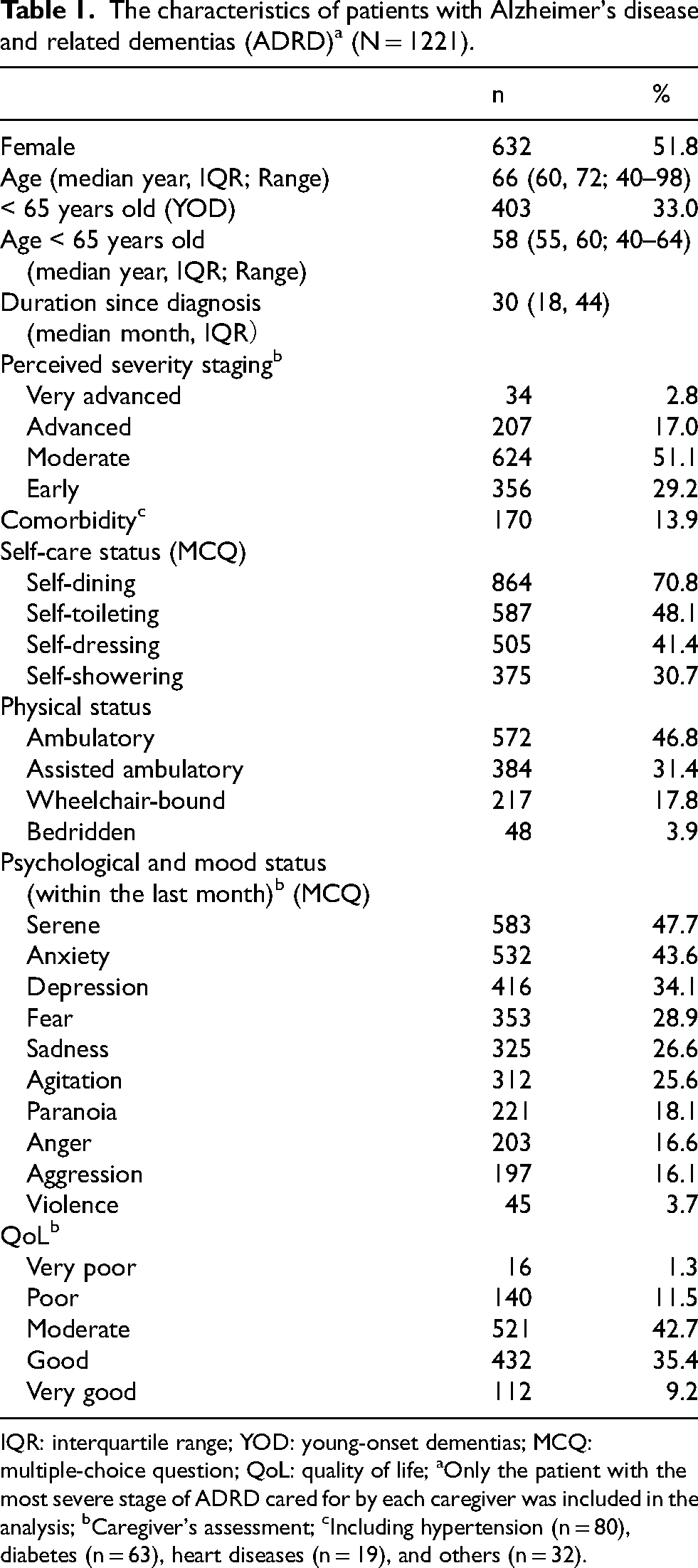
IQR: interquartile range; YOD: young-onset dementias; MCQ: multiple-choice question; QoL: quality of life; aOnly the patient with the most severe stage of ADRD cared for by each caregiver was included in the analysis; bCaregiver's assessment; cIncluding hypertension (n = 80), diabetes (n = 63), heart diseases (n = 19), and others (n = 32).
By the caregivers’ assessment of dementia staging, most patients had the moderately severe stage (51.1%, 624/1221), followed by the early stage (29.2%, 356/1221), advanced stage (17.0%, 207/1221), and very advanced stage (2.8%, 34/1221). Comorbidities were present in 13.9% (170/1221) of the patients, with hypertension (n = 80), diabetes (n = 63), and heart diseases (n = 19) being the most commonly reported.
Patients’ self-care abilities were generally compromised, requiring assistance for dining (29.2%, 357/1221), toileting (51.9%, 634/1221), dressing (58.6%, 716/1221), and showering (69.3%, 846/1221). Mobility was also affected, with 17.8% (217/1221) of patients using wheelchairs and 3.9% (48/1221) being bedridden. A wide range of psychological and mood issues were reported, with serene (47.7%, 583/1221), anxiety (43.6%, 532/1221), and depression (34.1%, 416/1221) being the most common moods.
QoL assessed by the caregivers revealed that most patients had a moderate (42.7%, 521/1221) or good QoL (35.4%, 432/1221). Only 12.8% of patients (156/1221) were reported as having very poor to poor QoL.
Demographics of caregivers
As shown in Table 2, males accounted for 59.8% (730/1221) of caregivers, with a median age of 30 years (range: 16∼68). Although respondents were from all over China, the majority were residents of Guangdong (40.6%, 496/1221), Beijing (9.7%, 118/1221), Tianjin (9.6%, 117/1221), and Hebei (8.2%, 100/1221). The remaining 31.9% (390/1221) were from 23 other provinces and two direct-administered municipalities. Most (96.6%, 1180/1221) were employed, with 84.6% (1033/1221) working full time. Most were married (59.2%, 723/1221), and 16.5% (202/723) had children. Nearly half of them reported their financial status as good to very good (44%, 537/1221).
The characteristics of caregivers of patients with Alzheimer's disease and related dementias (ADRD) (N = 1221).
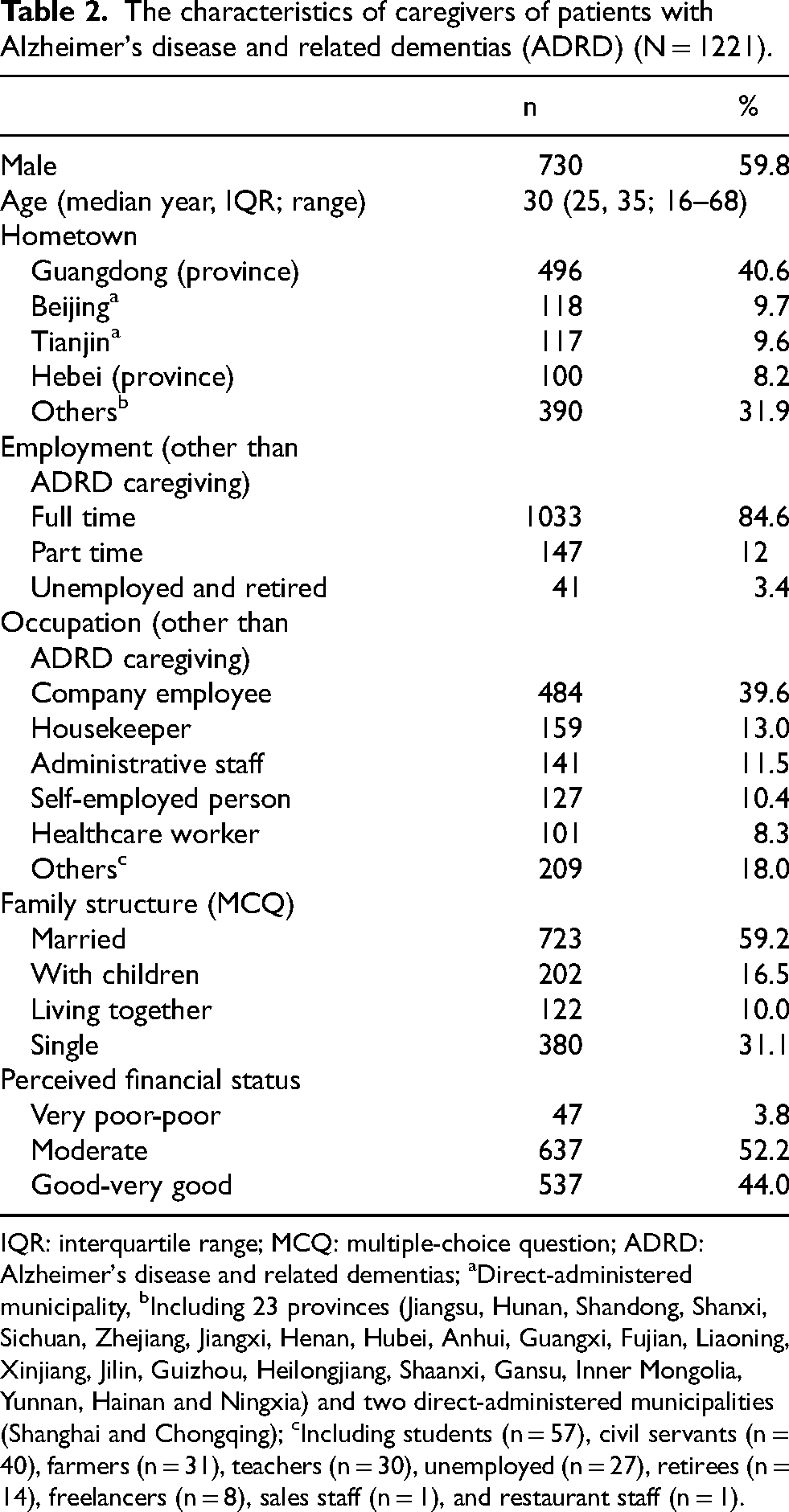
IQR: interquartile range; MCQ: multiple-choice question; ADRD: Alzheimer's disease and related dementias; aDirect-administered municipality, bIncluding 23 provinces (Jiangsu, Hunan, Shandong, Shanxi, Sichuan, Zhejiang, Jiangxi, Henan, Hubei, Anhui, Guangxi, Fujian, Liaoning, Xinjiang, Jilin, Guizhou, Heilongjiang, Shaanxi, Gansu, Inner Mongolia, Yunnan, Hainan and Ningxia) and two direct-administered municipalities (Shanghai and Chongqing); cIncluding students (n = 57), civil servants (n = 40), farmers (n = 31), teachers (n = 30), unemployed (n = 27), retirees (n = 14), freelancers (n = 8), sales staff (n = 1), and restaurant staff (n = 1).
Caregiving context
As shown in Table 3, the relationship between caregivers and their patients was mainly direct relatives (40.4%, 493/1221), followed by offspring (26.9%, 329/1221) and customers (26%, 317/1221). Most caregiving took place in the patient's home (67.6%, 825/1221), followed by care centers (37.8%, 461/1221) and hospitals (36%, 440/1221). A majority of caregivers were volunteers (68.8%, 840/1221), and many provided care on a part-time (60.4%, 737/1221) or full-time (39.6%, 483/1221) basis. Caregivers spent a median of 4 h per day on caregiving, with most providing care for over 24 days in the past month. The overall duration (median year) of caregiving was 2 years. Caregiving involved a wide range of tasks, including personal attendance (76%, 928/1221), cooking (67.4%, 823/1221), daily chores (60%, 733/1221), and house cleaning (55.4%, 676/1221). A majority of caregivers reported having received psychological (56.9%, 695/1221) and physical (47.8%, 584/1221) support, primarily from other family members (52.8%, 645/1221). A relatively small proportion (12.4%, 151/1221) of caregivers had received formal caregiving training.
Caregiving context (N = 1221).
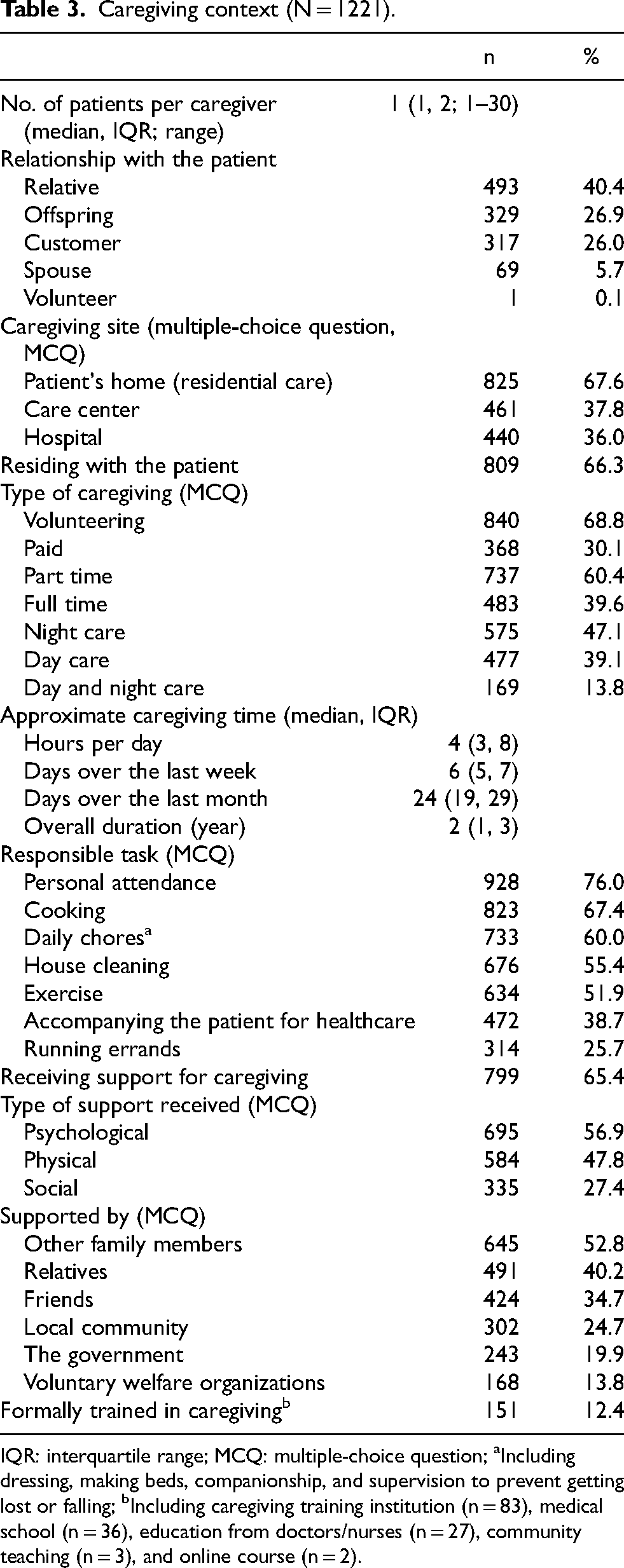
IQR: interquartile range; MCQ: multiple-choice question; aIncluding dressing, making beds, companionship, and supervision to prevent getting lost or falling; bIncluding caregiving training institution (n = 83), medical school (n = 36), education from doctors/nurses (n = 27), community teaching (n = 3), and online course (n = 2).
Multidimensional burden
In response to 5-point Likert questions, a substantial proportion of caregivers reported moderate-to-severe burden in physical health (24.2%, 296/1221), mental health (31.0%, 378/1221), family life (29.2%, 356/1221), and overall quality of life (47.2%, 576/1221) (Figure 1). Emotion-specific burden (Figure 2) revealed high rates of ambivalence (66.7%, 815/1221), grief (59.8%, 730/1221), and guilt (57.7%, 705/1221), alongside other negative emotions (54.9–32.0%), such as frustration, anxiety, tiredness, depression/sadness, loneliness, embarrassment, fear, anger, and loss, with less common emotions (31.4%–25.4%) including crankiness, irritability, disgust, impatience, resentment, boredom, and jealousy.

Caregivers’ self-perceived burden across four domains and severity levels expressed on a 5-point Likert scale. (N = 1221).
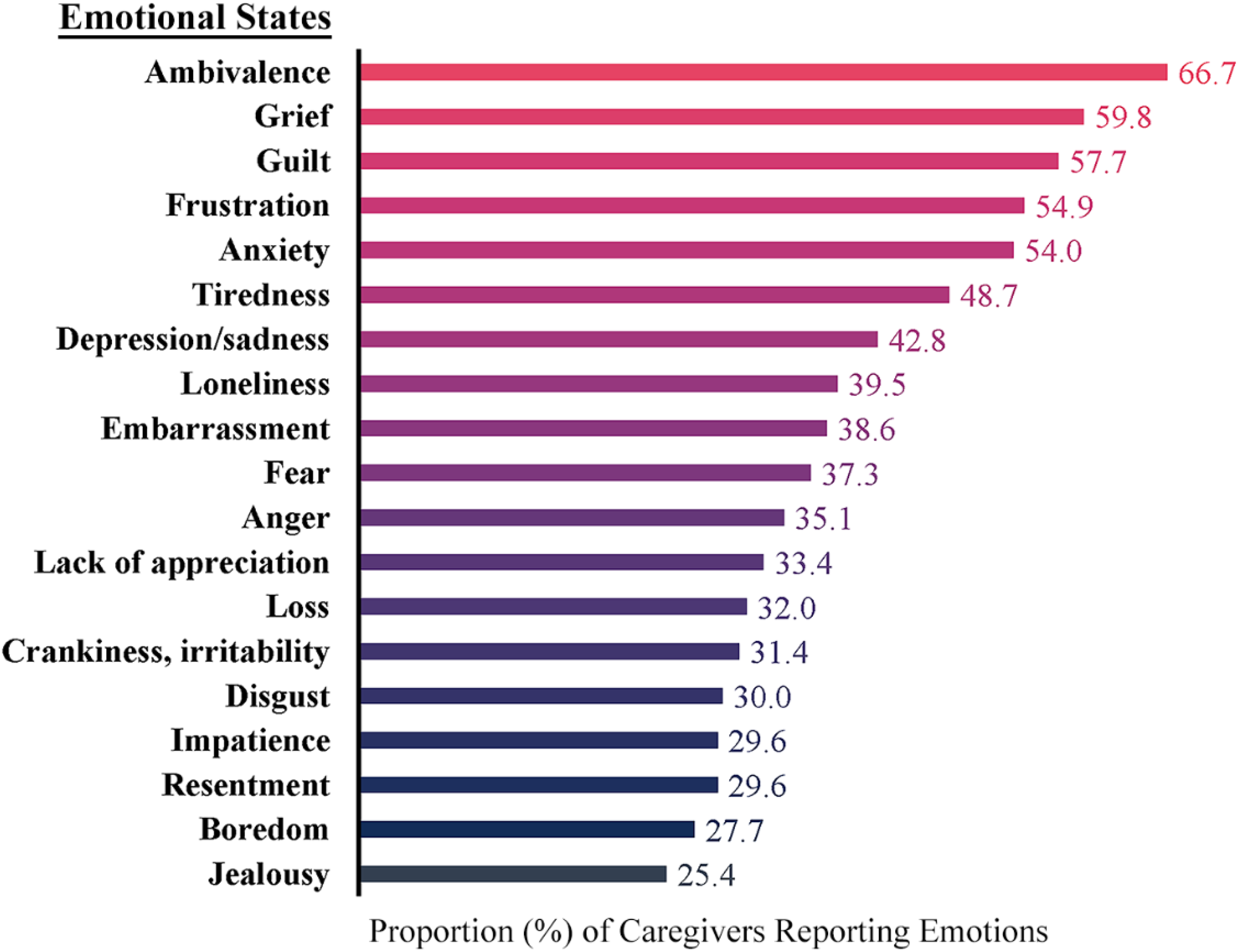
Emotional states experienced by Alzheimer's disease and related dementias (ADRD) caregivers (N = 1221).
Attitude toward caregiving (data not shown)
Despite substantial challenges, many caregivers viewed their role positively as responsible (55.2%), rewarding (55.9%), or satisfying (36.0%), although some described it as tiring (47.0%) or burdensome (37.8%).
Caregivers` concerns and needed supports
The most tiring aspects of caregiving for the caregivers were physical demands (26.9%, 329/1221), psychological strain (21.9%, 268/1221), and daily chores (18.7%, 228/1221) (Table 4). Caregivers expressed financial and material assistance (25.1%, 306/1221), helpers (19.7%, 241/1221), and psychological care (16.7%, 204/1221), among others, as the immediate caregiving supports that they wished to receive, while 16.7% (204/1221) felt manageable without support.
Caregivers’ concerns and needed supports (N = 1221).
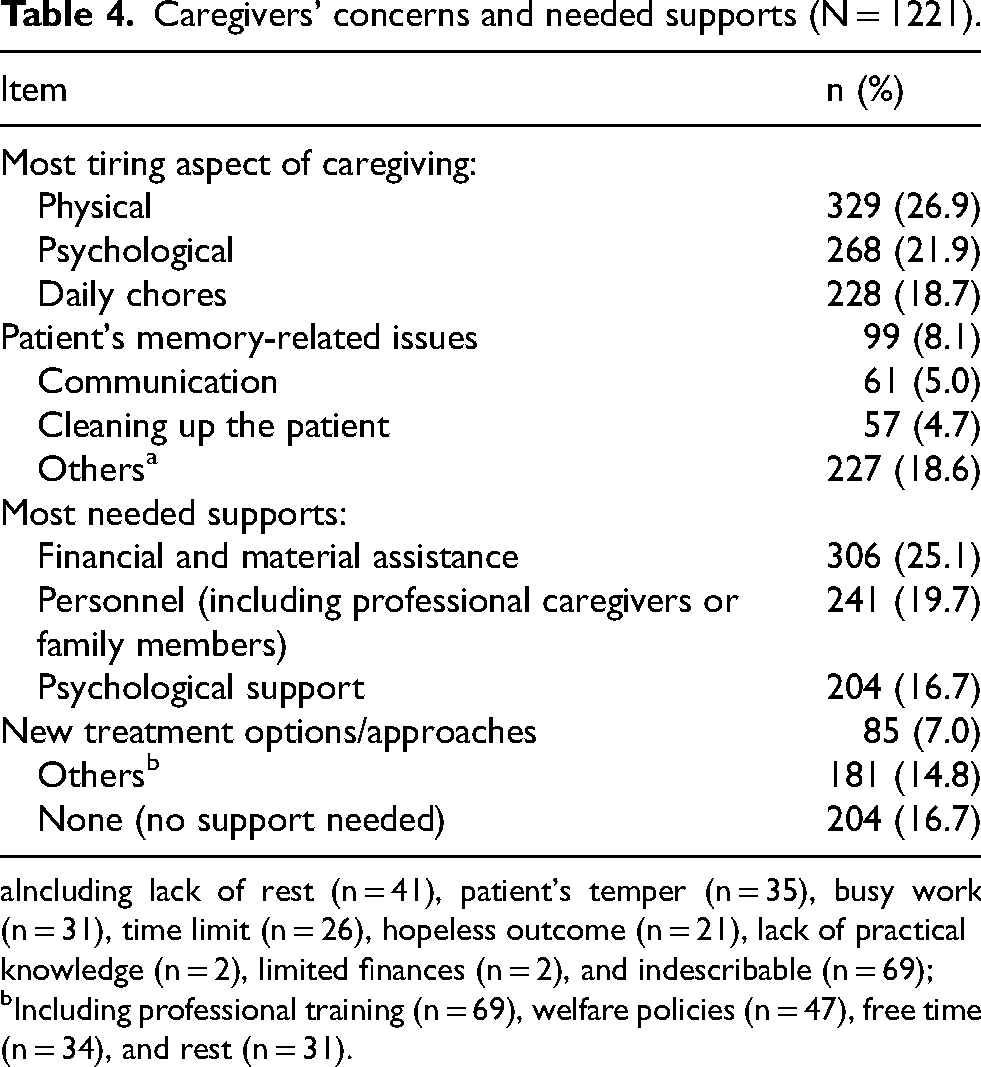
Including lack of rest (n = 41), patient's temper (n = 35), busy work (n = 31), time limit (n = 26), hopeless outcome (n = 21), lack of practical knowledge (n = 2), limited finances (n = 2), and indescribable (n = 69); bIncluding professional training (n = 69), welfare policies (n = 47), free time (n = 34), and rest (n = 31).
Independent predictors of caregiver burden
Of the 28 variables showing significant univariate associations with caregiver burden, 22 remained significant in the multivariable linear regression models as either predictors or protective factors (Figure 3, Supplemental Tables 1 and 2).
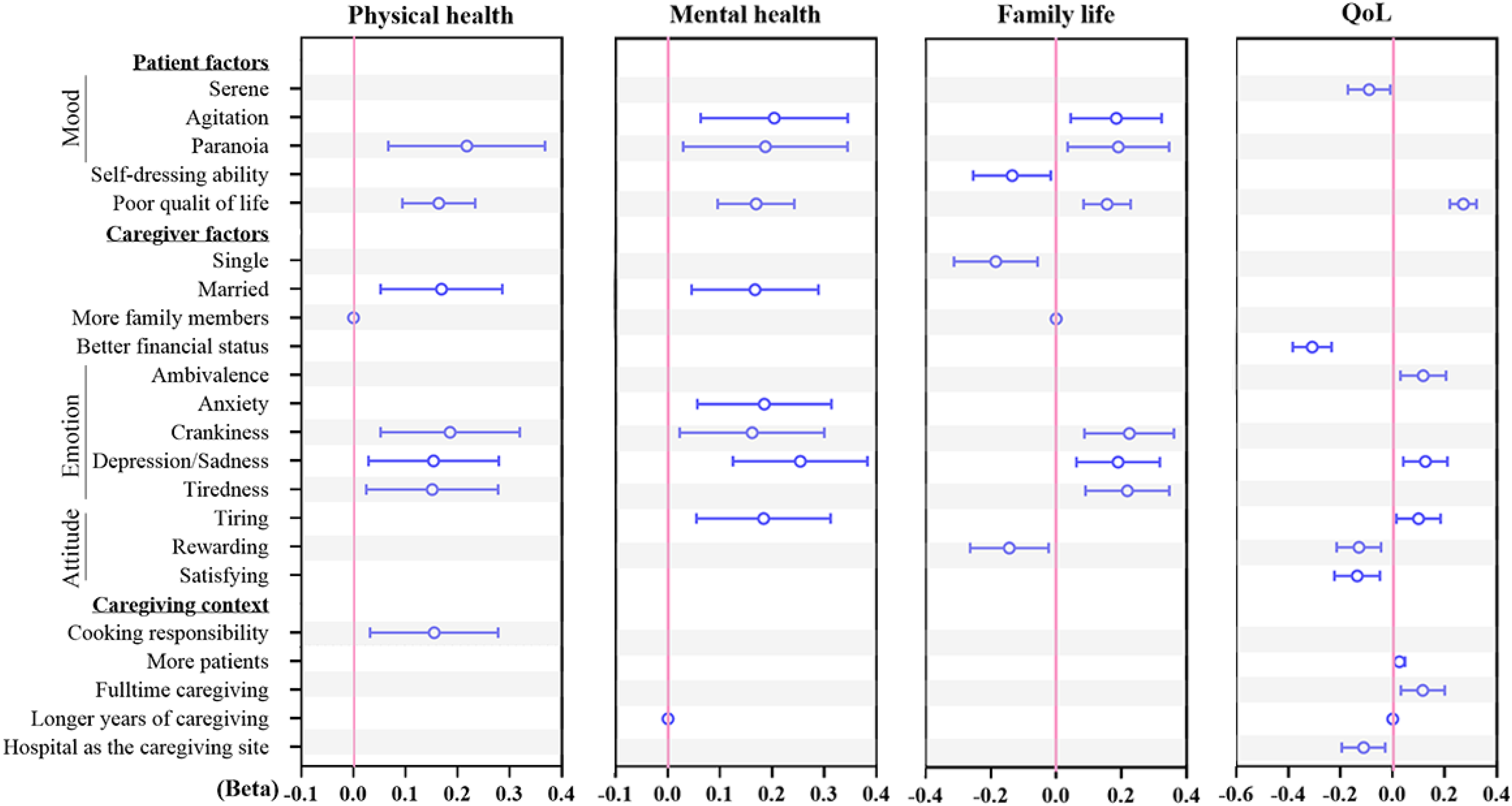
Multiple linear regression analysis of factors influencing perceived caregiver burden (N = 1221). Only variables with a significant association with the burden were included in the final regression models. Beta coefficients and 95% CIs are shown for each factor across four constructs.
Protective associations were observed for the patient's serene mood, caregivers’ rewarding or satisfying attitudes, better financial status, and care in a hospital setting, all of which were linked to the caregiver's QoL. Most other variables were positively associated with at least one burden construct, indicating greater perceived burden, whereas the unmarried status of caregivers was negatively associated with family life burden. Having more family members or longer caregiving duration was significantly associated with the burden, but with only a trivial effect. Effect sizes (beta coefficients and 95% CIs) are provided in Supplemental Table 2.
Discussion
With Chinàs rapidly aging population, 28 the increasing prevalence of ADRD,5,29 and the growing burden on caregivers, a thorough understanding of the dimensions and determinants of caregiver burden in the Chinese context has become essential for developing targeted interventions. This nationwide study reports the experiences of ADRD caregivers across China, highlighting the multidimensional nature of the burden on their physical and mental health, family life, and the overall QoL, with emphasis on the neglected aspect of their emotional experiences.
PLWD in China are generally diagnosed in memory clinics following international guidelines, but the overall diagnosis rate remains low. 5 For example, in 2019, only 28% of all AD cases were diagnosed in memory clinics. Therefore, we chose dementia-dedicated online forums as our sampling site. Patients in this study were identified as having AD based on caregiver reports. Given the nature of online forums and potential diagnostic uncertainty among caregivers, we classified these patients as having ADRD.
ADRD patient profiles: Implications for care demand
In line with global evidence and previous reports from China,30,31 slightly more females than males were among the ADRD patients in this study. The median age of patients in this study (66 years) was about a decade younger than in comparable studies of Chinese PLWD in highly urbanized Jiangsu (mean 77.5 years) 31 and Shanghai (mean 76.0 years). 30 The difference highlights the importance of nationwide studies in capturing heterogeneity across populations. According to the World Health Organization, the onset of dementia symptoms before the age of 65 is defined as young-onset dementia (YOD). 1 Therefore, 33.0% of patients < 65 years old in this study were classified as YOD. Since our patients were diagnosed approximately 30 months before our investigation, the true prevalence of YOD may be higher. The proportion of YOD in this study is much higher than the global age-standardized prevalence of YOD, i.e., 96–119 per 100,000 persons,32,33 thus posing unique challenges, as documented previously, due to behavioral symptoms, disruption of familial and economic roles, and limited access to age-appropriate support services.34,35
Caregiver profiles: Younger, working, and increasingly male
Caregiving is generally undertaken by women worldwide. 36 Previous studies in China also reported the predominance of older unemployed female caregivers. For example, caregivers in Shanghai and Jiangsu were 65 years and 62 years old on average, respectively, with 84% being unemployed in Jiangsu.30,31 This study revealed a contrasting profile, with the majority of caregivers being male, employed, and younger than expected for a caregiving population, highlighting a younger and more economically active caregiver group. These differences may reflect cultural and policy influences.
Traditional Chinese family structures generally assign caregiving responsibilities to younger relatives, particularly children.37,38 Additionally, the one-child policy (1979–2015), son-preference practices, and rising life expectancy may have also shifted caregiving roles toward younger working males.39,40 As reported previously from Hong Kong, Chinese male caregivers could face a multidimensional caregiving burden, including heightened gender role conflict, reduced self-efficacy, distress, and depression.41,42 This demographic shift underscores the need for caregiver-supportive workplace policies in China. More importantly, a combination of YOD and younger carers in this study adds complexity to caregiving roles and distinct challenges that are not fully captured in previous studies with older populations.
Of note, unlike family caregivers or unpaid volunteers in prior studies,30,31 30.1% (368/1121) of caregivers in our sample received payment for caregiving. Therefore, the burden observed in our study may partially reflect the experiences of paid caregivers, whose motivations, stressors, and support needs may differ systematically from those of unpaid caregivers.
Caregiving context: Home-based care with limited support
The caregiving context observed in this study reflects the continued dominance of family-based dementia care in China. Most caregivers were direct relatives or adult children, consistent with cultural expectations of filial responsibility and the limited availability of formal long-term care services. 16 The presence of “customer” caregivers also suggests a growing reliance on paid domestic workers as demographic and economic changes reduce families’ capacity to provide full-time care. 19
Home-based care was the most common arrangement, aligning with national patterns in which institutional care remains underutilized due to cost, stigma, and cultural preferences. 18 It is also associated with a heavier workload and higher burden, particularly when behavioral symptoms are present and professional support is limited. 18 The wide range of tasks reported in our sample, such as personal care, cooking, and household chores, mirrors the multidimensional demands described previously. 19
Despite these intensive responsibilities, only a small proportion of caregivers had received formal training. This gap is consistent with evidence that dementia specific training remains scarce in China, especially for informal caregivers and paid domestic workers. 43 Lack of training has been linked to higher caregiver burden and poorer quality of care. 9 Although many caregivers reported receiving psychological or physical support from family members, reliance on informal networks underscores the limited reach of community-based services and respite programs, which remain unevenly developed across regions. 16
Overall, the caregiving context identified in this study highlights a system heavily dependent on untrained family caregivers, with limited formal support and growing but still insufficient supplementary care options. These structural and cultural factors likely contribute to the high levels of burden observed and reinforce the need for scalable, culturally tailored caregiver support interventions.
Multidimensional nature of caregiving burden
Consistent with global evidence, caregivers in this study experienced significant proximal burden on physical and mental health, with the most pronounced downstream impact on the QoL and the diverse emotional burden. Our findings echo earlier research that identified emotional strain as a central component of caregiving. 44 The most frequently reported emotional experiences, such as ambivalence, grief, guilt, frustration, and anxiety, also suggest that caregivers are struggling with conflicting emotions and unmet expectations—both self-imposed and culturally driven. Such a multidimensional stress profile is distinct from those in previous studies30,45 where narrow-focused mental burden, like depression and anxiety, is emphasized.
Caregivers` attitudes, concerns, and needed supports
According to the “World Alzheimer Report 2024”, attitudes to dementia are so deeply informed by societal, economic, and cultural circumstances, beliefs, and norms. 29 The attitudes and support needs observed in this study similarly reflect the complex interplay between burden, resilience, and cultural expectations in dementia care. Despite reporting substantial physical and psychological strain, many caregivers still expressed positive views of their role, describing caregiving as responsible, rewarding, or satisfying. Similar findings are well documented in Chinese caregiving contexts, where filial piety and moral obligation can shape caregivers’ identities and emotional experiences.37,46,47 At the same time, the most tiring aspects, such as physical demands, psychological strain, and daily chores, mirror findings from other Chinese cohorts showing that functional decline and BPSD create a sustained workload and emotional exhaustion. 30 The strong desire for financial assistance, additional helpers, and psychological support underscores persistent structural gaps in China's dementia care system, where formal services remain unevenly distributed, and out-of-pocket costs are substantial. 43 These findings suggest that caregiving is unlikely to be sustainable when practical and emotional needs are unmet. Interestingly, a subgroup of caregivers reported not needing any support. This may reflect resilience, adaptive coping, or a strong sense of duty, but it may also indicate limited awareness of their own needs. Understanding this subgroup could help identify practical solutions to address unmet needs among the broader caregiver population.
Independent predictors of caregiver burden
Since caregiving burden is higher in Asia than the rest of the world, we are more concerned about relevant factors in low- and middle-income countries in Asia. 16 These include patient characteristics (female sex, older age, lower education, the presence of behavioral and psychological symptoms), caregiver profile (older age, unemployment/retirement, female sex, lower level of education, poor physical and mental health), and caregiving context (longer years of care and longer caring hours). 16 Our research, however, complements the existing evidence by identifying additional independent predictors of caregiver burden. They included patient factors, such as negative mood, poor physical status, and poor QoL; caregiver factors, such as negative emotions, attitudes, and being married; and caregiving characteristics, such as residential caregiving. In contrast, being single and holding positive caregiving attitudes (e.g., viewing caregiving as rewarding or satisfying) emerged as protective factors against caregiver burden.
Emotional feelings are well-established precursors to long-term psychological distress and burnout. Emotional experiences identified from in-depth exploration in this study highlight the need to consider emotion-based targeted interventions. These emotions are not just psychological states—they shape how caregivers respond to daily challenges, how they relate to care recipients, and how likely they are to seek or benefit from support.
Study limitations
The age and dementia stage of patients were reported by caregivers, which may be subject to bias, particularly when the respondents were paid caregivers or volunteers rather than family members. This limitation warrants caution when interpreting the notably high proportion of YOD observed in this study. Although caregivers from most provincial regions of mainland China were included, recruitment through online forums may have introduced selection bias and limited the generalizability of findings to populations with restricted internet access or low digital literacy, especially in rural regions. Additionally, our sample comprised both informal and paid caregivers (30.1%, 368/1221), which may account for differences from previous studies. While this study identified factors predicting holistic caregiver burden across all age groups, future research should investigate age- and region-specific determinants to guide tailored interventions.
Methodological considerations: Simplified caregiver burden assessment approach
In addition to the above limitations, the interpretation of the observed burden requires careful consideration of our assessment approach. For caregiver burden assessment, there exist several validated scales, including the most widely used Caregiver Burden Inventory (CBI) and Zarit Burden Interview (ZBI). 48 A systematic review of dementia caregiver burden in low- and middle-income countries in Asia, however, has highlighted inconsistencies across these scales; for example, the burden in China was rated high by the CBI but low by the ZBI, 16 suggesting scale-dependent variability that complicates cross-study comparisons. To avoid such inconsistencies and minimize respondent fatigue, we employed a concise, self-reported burden measure using a single 5-point Likert scale for each of four constructs (physical and mental health, family life, and QoL) and YES/NO questions for emotional experiences. This approach prioritizes practicality and interpretability while maintaining sensitivity to the burdens caregivers themselves identify as most salient.
Evidence-based suggestions
A variety of supportive measures for PLWD exist in China through memory clinics, memory schools, long-term care insurance, volunteer organizations, non-profit social service institutions, self-help groups, and online hospitals. 5 However, geographical coverage and utilization remain patchy, and most services are not designed to address caregiver burden; some even increase strain by requiring carers to accompany patients.5,30 Evidence shows that interventions are most effective when they are individualized. 20
While assistance with physical and financial burden benefits all caregivers, a wide range of emotional strains reported in this study requires individualized psychosocial interventions. Even emotions with lower reported prevalence (e.g., jealousy, disgust, loss) warrant attention for possible underreporting due to cultural stigma.
The following evidence-based non-pharmacological interventions20,22 can be considered:
Mindfulness-based interventions (MBIs), such as Mindfulness-Based Stress Reduction (MBSR) and Mindfulness-Based Cognitive Therapy (MBCT), reduce anxiety, stress, depression, and perceived burden,49,50 and may help mitigate ambivalence through improved emotion regulation. Psychoeducational programs enhance coping skills, reduce strain, and increase knowledge.
51
Such programs are particularly relevant for caregivers experiencing guilt, grief, and frustration. Caregiver behavioral management training (CBMT) can support caregivers struggling with frustration, crankiness, and disgust, particularly when dealing with patients’ BPSD, as demonstrated in a randomized controlled trial (RCT) in Zhejiang.
52
Peer support groups, either face-to-face or through web-based forums on platforms like QQ or WeChat, can alleviate loneliness, lack of appreciation, and resentment by fostering emotional solidarity and shared experience.
53
Supportive psychotherapy, framed within culturally resonant narratives of filial piety and family duty, can be helpful for those experiencing grief, loss, or ambivalence, as suggested previously.
47
Multicomponent intervention, e.g., MBI with self-care skills, support groups, or behavioral management, as shown in a recent RCT,
54
could be most suitable for caregivers with a multidimensional burden, as in this study. Workplace-based caregiver policies are also important, as most caregivers in this study were employed, and workplace interventions can target tiredness, impatience, and burnout, especially among younger male caregivers.
Of note, these interventions generally require trained professionals and can last for 6 weeks to 10 months, 22 and can be delivered in person or online to individuals, caregiver/care recipient pairs, and groups through existing support channels in China or adapted from models such as the Virtual Psychotherapy Program for Caregivers (VPPC), the U.S. Department of Veterans Affairs, 55 which offers comprehensive, home-accessible therapy options for individuals, groups, or families.
Conclusions
This nationwide study highlights the multidimensional burden faced by ADRD caregivers in China, revealing significant physical, emotional, familial, and QoL strains. Predominantly younger, employed, and male caregivers reflect shifting sociocultural dynamics. The high prevalence of YOD adds complexity to caregiving demands. Our findings underscore that evidence-based individualized psychosocial and workplace interventions should be prioritized to alleviate caregiver burden.
Supplemental Material
sj-docx-1-alr-10.1177_25424823261433567 - Supplemental material for Multidimensional burden of caregivers of Alzheimer's disease and related dementia in China: A nationwide cross-sectional study
Supplemental material, sj-docx-1-alr-10.1177_25424823261433567 for Multidimensional burden of caregivers of Alzheimer's disease and related dementia in China: A nationwide cross-sectional study by Dangui Zhang, Yongleng Fang, Minglong Huang, Meiyu Wang, Weijin Li, Yuhan Gong and William Ba-Thein in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
The authors would like to thank Dr Hui Pan for assistance with patient recruitment and hands-on information.
Ethical considerations
This study was approved by the Ethics Committee of Shantou University Medical College (approval: SUMC-2021-32) on March 14, 2021.
Consent to participate
Before participating in the survey, all participants provided informed consent by agreeing to the study's objectives and statements regarding anonymity, data confidentiality, and data use.
Author contribution(s)
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Undergraduate Research Training Program (UGRTP), grant number: LE0003.
Declaration of conflicting interests
This work was supported by the Undergraduate Research Training Program (UGRTP), grant number: LE0003, the Li Ka Shing Foundation.
Data availability statement
The data supporting the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.