
Abstract
Background
The “head-turning sign” (HTS) and Neurocognitive Questionnaire (Neucop-Q) capture toritsukuroi (saving appearance) behaviors commonly observed in Alzheimer's disease (AD). Neucop-Q is a brief screening questionnaire assessing current event memory (News; N), self-awareness/concern (Consciousness; C), and engagement in pleasurable activities (Pleasure; P). Previously, HTS-positivity and impaired N/impaired C/normal P (NimpCimpPnor) combination show high specificity for amyloid PET positivity.
Objective
To investigate the neuroanatomical correlates of HTS and specific Neucop-Q response patterns across the AD continuum.
Methods
One hundred thirty-seven individuals (54 cognitively normal controls, 9 preclinical AD, 36 mild cognitive impairment, and 38 AD dementia patients) underwent clinical evaluation and structural MRI. Gray matter volumes were analyzed using voxel-based morphometry with MVision software based on a Multi-Atlas Likelihood Fusion approach. Regional volumes were normalized to intracranial volume and adjusted for age and sex. Group differences were tested with false discovery rate (FDR) correction, and logistic regression assessed associations between regional volume and Neucop-Q responses.
Results
HTS was significantly associated with right hippocampal atrophy (FDR-corrected p = 0.024). In the logistic regression analyses, none of the associations survived correction for multiple comparisons. The NimpCimpPnor combination was correlated with medial and inferior temporal lobe atrophy (FDR < 0.01) and larger globus pallidus (FDR = 0.034), with logistic regression surviving correction.
Conclusions
HTS reflected reduced right hippocampal volume, whereas NimpCimpPnor involved broader temporal atrophy with relatively larger pallidal volumes, suggesting distinct regional gray matter patterns across behavioral response profiles.
Introduction
Alzheimer's disease (AD) is a progressive neurodegenerative disorder characterized by early episodic memory impairment followed by deficits in executive function, language, and visuospatial processing, along with neuropsychiatric symptoms such as apathy, anxiety, depression, irritability, and diminished social engagement, ultimately leading to impaired activities of daily living and loss of independence.1,2 Early AD often manifests with distinctive behavioral and neuropsychiatric features, including personality changes and mood swings. One such behavior is the so-called “saving appearance responses,” or toritsukuroi in Japanese, a tendency for individuals to feign understanding or fabricate plausible answers to maintain social appearance.3,4 This compensatory social behavior can mislead caregivers and clinicians, masking disease severity in the early stages. Toritsukuroi behaviors are thought to depend on relatively preserved judgment and social cognition despite emerging memory impairment, 3 and they tend to diminish as verbal recall and executive functions decline. 5
A visible, non-verbal correlate of toritsukuroi is the head-turning sign (HTS), in which patients turn to their partners for assistance when asked a question. 6 Although HTS may have limited sensitivity—reflecting factors such as impaired comprehension, reduced confidence, or limited insight—and can be remembered in other neurodegenerative conditions as well as occasionally in cognitively normal individuals,7–9 it remains a rapid, intuitive, and low-burden in-clinic observation that requires no special equipment and can be readily incorporated into routine clinical encounters. As such, HTS serves as a practical screening cue that may prompt further evaluation for AD. Importantly, HTS may capture subtle social–behavioral changes that are not detected by conventional cognitive tests.
On the other hand, the Neucop-Q was developed as a brief, caregiver independent dementia screening tool. 10 It consists of three open-ended questions assessing (1) current event memory (News; N), (2) self-awareness of cognitive difficulties (Consciousness; C), and (3) engagement in pleasurable activities (Pleasure; P). The response patterns to these questions can capture subtle cognitive and metacognitive dysfunctions. For example, vague or outdated answers to the news question (impaired N; Nimp) may reflect impaired recent memory, reduced interest, or verbal toritsukuroi; denial of difficulties (impaired C; Cimp) may represent unawareness or façade behavior; while specific answers about pleasure (normal P; Pnor) may indicate preserved affect or attempts to mask impairment. The combined pattern of NimpCimpPnor has been proposed to represent a form of toritsukuroi expressed through verbal responses rather than interpersonal reliance. 6 While responses to Neucop-Q are somewhat subjective, previous studies have shown that both HTS and specific Neucop-Q response patterns exhibited high specificity for AD or amyloid-positive amyloid positron emission topography (PET) findings.6–8,10,11 However, the neural mechanisms underlying these compensatory behaviors remain largely unexplored.
Recent advances in image analysis now enable quantitative assessment of subtle volumetric and microstructural changes that were previously imperceptible.12–14 Therefore, the present study aims to identify the neuroanatomical correlates of HTS and Neucop-Q response profiles across the AD continuum using automated volumetric MRI analysis. By examining associations between distinct behavioral manifestations—dependent (HTS) and independent (NimpCimpPnor) forms of toritsukuroi—to regional gray matter alterations, we sought to characterize structural patterns related to these clinical response profiles.
Methods
Participants
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee for Human Research of the Keio University School of Medicine (#N20170237). Written informed consent was obtained from all participants. The study was conducted between July 2018 and May 2024. The participants included cognitively impaired individuals who visited the Memory Center at Keio University Hospital and cognitively normal volunteers recruited through external organizations, as described in our previous work.6,15,16 All participants were aged 40–85 years and had at least 12 years of education. All participants underwent neuropsychological evaluation and amyloid PET imaging. Those with positive amyloid PET findings were classified as being on the AD continuum. Participants with non-AD dementia (e.g., vascular dementia, frontotemporal lobar degeneration, Lewy body disease), traumatic brain injury, or Geriatric Depression Scale score > 6 were excluded. The inclusion criteria for dementia and mild cognitive impairment (MCI) were based on those established in our previous study, 17 incorporating standard cognitive and functional assessments with modifications informed by the Alzheimer's Disease Neuroimaging Initiative (ADNI) protocol. 18
The inclusion criteria for AD dementia patients were as follows:
Mini-Mental State Examination (MMSE) score < 24, Clinical Dementia Rating Global Score (CDR-GS) = 0.5 or 1. Wechsler Memory Scale (WMS) Logical Memory II Delayed Recall (LM-D) score < 9 for <16 years of education (YOE) or <11 for ≥16 YOE.
The inclusion criteria for MCI patients were as follows:
MMSE score ≥ 24, CDR-GS = 0.5 with a memory domain score ≥ 0.5, WMS LM-D score < 9 for <16 YOE or <11 for ≥16 YOE.
The inclusion criteria for cognitively normal (CN) participants were as follows:
MMSE score ≥ 24, CDR-GS = 0, WMS LM-D score ≥ 5 for <16 YOE or ≥9 for ≥16 YOE,
Preclinical AD was defined as participants who are CN with evidence of cerebral amyloid deposition on PET imaging. The distinction between cognitively normal individuals and those categorized as preclinical AD was based on visual assessment of PET imaging. Given the potential continuum between these groups, both were included in the present study. Final diagnoses were made according to standard clinical criteria.19,20
Clinical evaluation
The clinical assessments included the HTS and the Neucop-Q screening tool, both described in detail in previous publications.
10
Head-turning sign (HTS):
HTS was considered positive when a participant turned their head toward their study partner/primary caregiver for assistance during the interview, typically in response to a question requiring personal knowledge or recall. When no such behavior was observed, HTS was classified as negative.
Neucop-Q:
The Neucop-Q is a brief, caregiver-independent screening interview comprising three open-ended designed to assess recent memory, self-awareness, and engagement in pleasurable activities::
“What is the most notable current/recent news/topics?” (News; N) “Do you feel that you have more difficulties in your daily life than you used to?” (Consciousness; C) “Could you tell me about your daily pleasures or pastimes?” (Pleasure; P)
Each response was categorized as normal (nor) or impaired (imp) based on predefined criteria. Participants who mentioned recent and concrete news were categorized as Nnor, whereas vague, outdated, or no responses were labeled Nimp. Those acknowledging daily difficulties were labeled self-aware (Cnor), whereas those denying such issues were classified as unaware (Cimp), even if they were cognitively normal. Specific and concrete answers about pleasure or pastime were labeled Pnor, whereas vague or absent responses were labeled Pimp.
For exploratory analyses, combinations of these response patterns were also examined. In particular, the NimpCimpPnor profile was treated as a distinct subgroup, representing participants who exhibited impaired responses to the News and Consciousness questions but preserved responses to Pleasure.
All assessments were administered by trained clinicians during structured clinical interviews conducted on the same day as neuropsychological testing.
Imaging and postprocessing
All participants underwent amyloid PET and structural MRI. Protocols for amyloid PET imaging have been described previously in the literature. 15 Briefly, a 20-min PET scan was performed 90 min after intravenous injection of [18F]florbetaben using Biograph mCT (Siemens Medical Solutions USA Inc., Hoffman Estates, IL, USA). Image reconstruction and correction were conducted using standard protocols, and visual assessment for amyloid positivity was performed by a trained neuroradiologist using the regional cortical tracer uptake (RCTU) scoring system. Amyloid positivity was defined as an RCTU score >1 in at least one of four predefined brain regions.
Structural MR images were acquired using a 3.0 T Discovery MR750 scanner (GE Healthcare, USA) with a three-dimensional T1-weighted brain volume (BRAVO) sequence (repetition time = 6.8 ms, echo time = 3.0 ms, field of view = 23.0 cm, voxel size = 0.9 × 0.9 × 1.0 mm, flip angle = 8°). Automated segmentation was conducted using MVision (Corporate M, Tokyo, Japan), which is based on the multiatlas pipeline implemented in MriCloud (Johns Hopkins University, Baltimore, MD, USA).21–25 Automated segmentation was conducted with Mvision (Corporate M, Tokyo, Japan), which uses the multi-atlas pipeline implemented in MriCloud (Johns Hopkins University, Baltimore, MD, USA).21–25 Briefly, MVision is based on the Multi-Atlas Likelihood Fusion (MALF) method. This highly accurate technique works by first taking a library of expertly labeled brain atlases and non-rigidly registering (warping) each one to the participant's MRI scan, followed by a label-fusion algorithm. Then, the “hierarchical parcellation” is achieved through a structural framework that defines over 500 brain structures across five levels of granularity, enabling analysis from lobar regions to fine-grained subregions. In this study, the highest-granularity parcellation was generated for each participant (Supplemental Figure 1). Regional brain volumes were calculated by summing the voxel volumes corresponding to each anatomical label in the final MALF segmentation. The accuracy of the segmentation has been validated previously. 22 Raw volume values were converted into relative volumes (normalized to total intracranial volume) by dividing the volume of each structure by the total intracranial volume, which was defined as the sum of gray matter, white matter, and cerebrospinal fluid volumes. For clarity in interpretation, these volume fractions were expressed as percentages (volume fraction × 100) and used in subsequent statistical analyses.
Statistics
Group comparisons were conducted to examine differences in demographic and clinical variables [age, sex, education, CDR-GS, MMSE, and Alzheimer's Disease Assessment Scale (ADAS)] between binary classifications (HTS, individual C/N/P responses, and the NimpCimpPnor combination). Continuous variables were assessed using independent samples t tests or Wilcoxon rank-sum tests, depending on the normality of the distribution determined by the Shapiro‒Wilk test. Categorical variables such as sex were compared using the chi-square test or Fisher's exact test, as appropriate. The mean and standard deviation (SD) were reported for each group.
The associations between regional brain volumes and specific clinical features were examined using linear and logistic regression models to assess both structural differences and predictive relationships. Participants were grouped on the basis of the presence or absence of HTS, individual N/C/P responses, or the NimpCimpPnor combination.
For each of the 96 gray matter regions, linear regression models were applied to assess group differences in relative volume fractions, adjusting for age and sex. Corresponding t statistics and p values were calculated, and false discovery rate (FDR) correction was applied to control for multiple comparisons. Effect sizes were quantified using partial R2 values for the group term in each linear regression model, indicating the variance in regional gray matter volume explained by group status after adjusting for age and sex.
Next, logistic regression was performed to examine associations between gray matter volume and the presence of each clinical sign. Gray matter % volume fractions (continuous variables, expressed as percentages and multiplied by 100 to improve interpretability of odds ratios) were entered as the independent variable and clinical features (HTS, C/N/P responses, or the NimpCimpPnor combination) as the dependent variable. All models were adjusted for age and sex. Separate models were fitted for each brain region, and odds ratios (ORs), 95% confidence intervals, and p values were calculated, with FDR correction applied for multiple testing.
Effect sizes (ORs and beta coefficients) and their 95% confidence intervals were used to aid interpretation of the strength and direction of associations, beyond reliance on p values alone. Statistical significance was defined as an FDR-adjusted p value of < 0.05. All analyses were performed in R (version 4.4.2).
Results
Participant demographics
In total, 83 individuals on the AD continuum (9 preclinical, 36 MCI, and 38 AD dementia) and 54 cognitively normal individuals were included in the study. The demographics of the participants for each clinical measure are presented in Tables 1–4. Notably, the populations used for each between-group analysis (HTS, N/C/P responses, and the NimpCimpPnor combination) differed, as each grouping defined a unique subset of participants.
Demographics of the participants.

AD: Alzheimer's disease; AD-D: AD dementia; MCI: mild cognitive impairment; CN: cognitively normal; MMSE: Mini-Mental State Examination; ADAS: Alzheimer's Disease Assessment Scale.
Data are presented as the means ± SDs.
Demographics of the head-turning sign (HTS)-positive and HTS-negative groups.

HTS: head-turning sign; AD: Alzheimer's disease; AD-D: AD dementia; MCI: mild cognitive impairment; CN: cognitively normal; CDR-GS: Clinical Dementia Rating Global Score; MMSE: Mini-Mental State Examination; ADAS: Alzheimer's Disease Assessment Scale.
Participants who were not accompanied (2 AD-D, 10 AD-MCI, 6 AD-preclinical, 45 CN) were excluded. The data are presented as the means ± SDs. * Significant between-group differences, p < 0.05.
Participant demographics across Neucop-Q subgroups.

AD: Alzheimer's disease; AD-D: AD dementia; MCI: mild cognitive impairment; CN: cognitively normal; CDR-GS: Clinical Dementia Rating Global Score; MMSE: Mini-Mental State Examination; ADAS: Alzheimer's Disease Assessment Scale.
Data are presented as the means ± SDs. * Significant between-group (impaired/normal) differences, p < 0.05.
Participant demographics for the NimpCimpPnor combinations.

AD: Alzheimer's disease; AD-D: AD dementia; MCI: mild cognitive impairment; CN: cognitively normal; CDR-GS: Clinical Dementia Rating Global Score; MMSE: Mini-Mental State Examination; ADAS: Alzheimer's Disease Assessment Scale.
Data are presented as the means ± SDs. * Significant between-group differences, p < 0.05.
Correlation between HTS and brain volume
In the between-group comparison, after correction for multiple comparisons using FDR (q < 0.05), HTS status was significantly associated only with reduced right hippocampal volume (β = −0.028 ± 0.007, FDR-corrected p = 0.024) (Figure 1; Supplemental Table 1), corresponding to an approximately 10% relative reduction compared with HTS-negative participants (Figure 2). HTS explained 17.6% of the variance in right hippocampal volume after adjustment for age and sex (partial R2 = 0.176).
At the uncorrected level (p < 0.05), HTS was additionally associated with reduced volume in the left hippocampus (p = 0.024), bilateral entorhinal areas (right: p = 0.0062; left: p = 0.038), bilateral parahippocampal gyrus (right: p = 0.0053; left: p = 0.022), right angular gyrus (p = 0.0032), left supramarginal gyrus (p = 0.0079), right superior parietal lobule (p = 0.029), right superior frontal pole (p = 0.030), right amygdala (p = 0.035), left postcentral gyrus (p = 0.037), right entorhinal gyrus (p = 0.038), and right inferior temporal gyrus (p = 0.044), as well as relatively increased volume in the and left rostral anterior cingulate cortex (p = 0.019) and right superior frontal pole (p = 0.030) (Figure 1; Supplemental Table 1). However, none of these associations survived FDR correction and should therefore be considered exploratory.

Regional brain volume differences between the head-turning sign (HTS)-positive and HTS-negative groups. Adjusted group differences in gray matter volume fraction (percentage points), estimated from linear regression models controlling for age and sex. Negative values indicate lower volume fraction in the reference group. *HTS-positive participants showed a significantly reduced right hippocampal percent volume fraction [p = 0.024, false discovery rate (FDR)-corrected]. Other associations did not remain significant after FDR correction and should therefore be interpreted as exploratory. SF_pole_R: superior frontal pole (right); rostral_ACC_L: rostral anterior cingulate cortex (left); PHG: parahippocampal gyrus; ENT: entorhinal area; Amyg: amygdala; Hippo: hippocampus; SP: superior parietal lobule; IT: inferior temporal gyrus; A: angular gyrus; PoC: postcentral gyrus; SM: supramarginal gyrus.
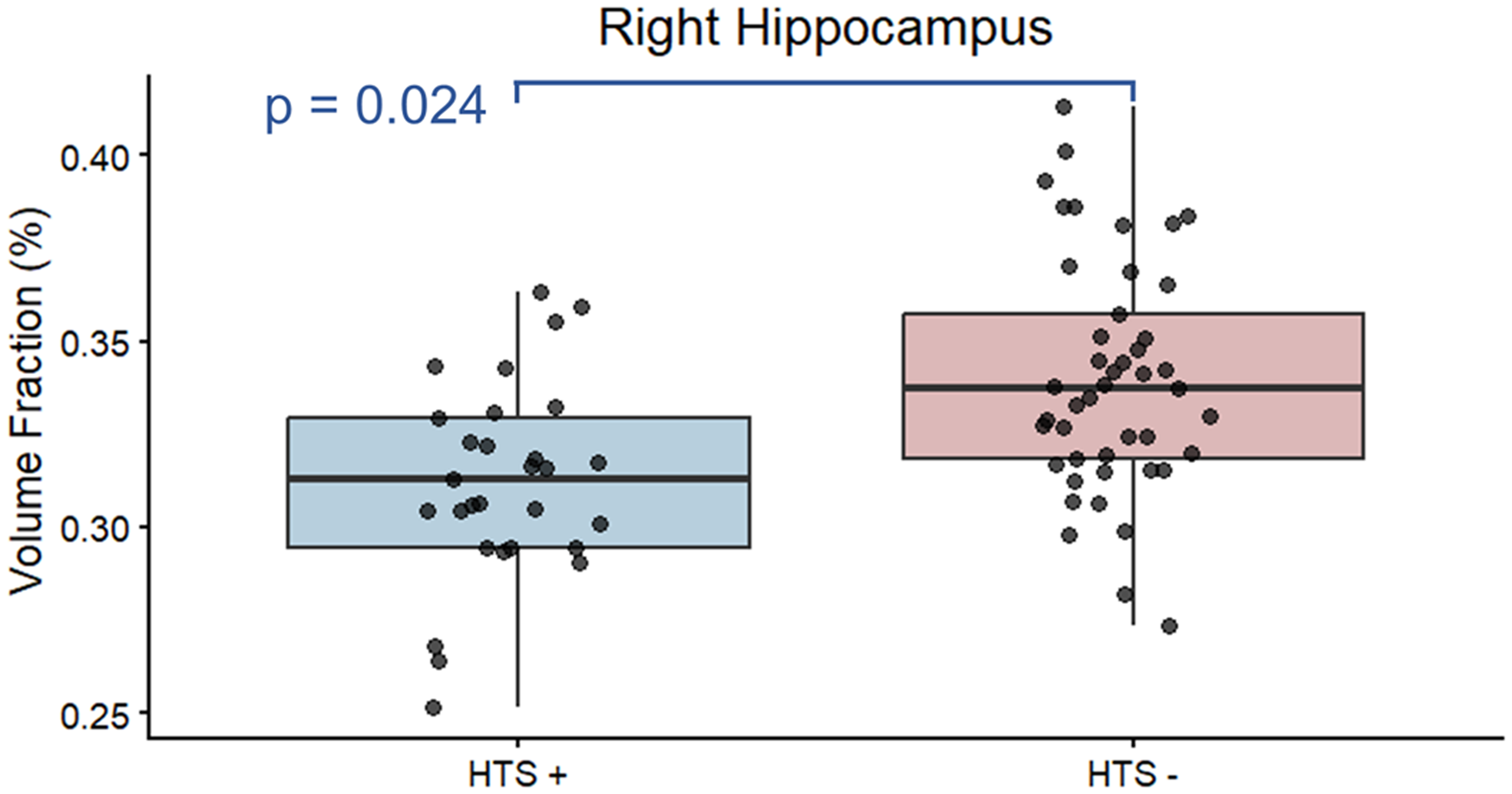
Comparison of right hippocampal volume fractions between HTS positive and negative groups. After adjusting for age and sex, participants exhibiting the head-turning sign showed lower right hippocampal volume fractions. Boxplots depict central tendency and spread, with individual observations superimposed. The p value indicates a statistically significant association after false discovery rate correction.
Logistic regression analysis of HTS further revealed potential contribution of volume reductions in the bilateral hippocampus (right: uncorrected p = 0.0012; left: p = 0.011), bilateral parahippocampal gyrus (right: p = 0.0054; left: p = 0.018), right inferior temporal gyrus (p = 0.030), right lingual gyrus (p = 0.031), and right supramarginal gyrus (p = 0.034), as well as relatively increased volume in the left rostral anterior cingulate cortex (p = 0.044); however, these associations did not remain significant after FDR correction (q < 0.05) (Supplemental Table 2).
Correlation between Neucop-Q responses and brain volume
The NimpCimpPnor combination was significantly associated with widespread temporal lobe atrophy (Figure 3). Exact β coefficients, standard errors, FDR-corrected p-values, and partial R2 for all regions are provided in Table 5. Notably, the findings included reduced volumes in the amygdala (16% decrease for right; 12% decrease for left), entorhinal cortex (18% decrease for right; 16% decrease for left), parahippocampal gyrus (11% decrease for right; 13% decrease for left), inferior temporal gyrus (7.9% decrease for right; 8.3% decrease for left), and right hippocampus (9.5% decrease) (Figure 4). In contrast, a relative volume increase was observed in the left globus pallidus (8.1% increase) (Figure 4). Partial R2 values indicated that group status explained between 6% and 15% of the variance in regional gray matter volumes independent of age and sex, corresponding to effect sizes that are within the moderate range for neuroimaging studies (Table 5).

Regional brain volume differences between the NimpCimpPnor group and all other response combinations. Adjusted group differences in gray matter volume fraction (percentage points), estimated from linear regression models controlling for age and sex. All observed associations were significant following false discovery rate (FDR) correction. GP_L: globus pallidus (left); PHG_R: parahippocampal gyrus (right); ENT: entorhinal area; Amyg: amygdala; Hippo: hippocampus; IT: inferior temporal gyrus.

Comparison of volume fractions between the NimpCimpPnor combination and the remaining groups in selected brain regions that exhibited significant between-group differences. Boxplots depict central tendency and spread, with individual observations superimposed. The p values indicate a statistically significant association after false discovery rate correction.
Comparison between the NimpCimpPnor combination and other combinations.

FDR: false discovery rate.
Logistic regression for the NimpCimpPnor group demonstrated directionally similar associations across the same regions, which remained significant after multiple comparison correction (Table 6); however, the wide confidence intervals indicate limited precision of the estimates. Specifically, FDR-corrected p < 0.01 was observed for atrophy in the bilateral entorhinal cortex, bilateral amygdala, right inferior temporal gyrus, left parahippocampal gyrus, and right hippocampus. Additionally, FDR-corrected p < 0.05 was found for the left inferior temporal gyrus, right parahippocampal gyrus, and relatively larger volume in the left globus pallidus. Although logistic regression revealed a significant association between volume changes and the NimpCimpPnor group, the wide confidence interval suggests instability of the estimate and warrants cautious interpretation.
Logistic regression analysis of the NimpCimpPnor combination.

CI: confidence interval.
When analyzed individually, the Nimp group showed atrophy in multiple regions of the temporal lobes, predominantly on the left side, as well as part of the prefrontal cortex (p < 0.001 for the bilateral inferior temporal gyri, parahippocampal gyri, entorhinal cortices, amygdalae, left superior temporal gyrus, left middle temporal pole, right hippocampus, and right middle temporal gyrus; p < 0.05 for the left superior temporal pole, left fusiform gyrus, right middle temporal pole, left dorsolateral prefrontal cortex, left hippocampus, left angular gyrus, and left middle temporal gyrus). In addition, a larger caudate volume was observed (p = 0.014 for the right and p = 0.032 for the left). With respect to consciousness, no significant between-group differences were observed. The logistic regression model for Cimp revealed atrophy in the parahippocampal gyri, right dorsolateral prefrontal cortex, and other frontal and occipital regions, along with increased hypothalamic volume. However, only the right parahippocampal gyrus and dorsolateral prefrontal cortex remained significant (p < 0.05) after FDR correction. The Pnor/imp group presented a divergent trend, with no significant differences in volume.
Discussion
To our knowledge, this is the first volumetric study examining structural correlates of distinct toritsukuroi-related behavioral patterns along the AD continuum. HTS demonstrated a significant association with reduced right hippocampal volume after correction for multiple comparisons. In contrast, the NimpCimpPnor combination was associated with more extensive temporal lobe atrophy, including bilateral amygdala, entorhinal cortex, parahippocampal gyrus, and inferior temporal regions, as well as a larger volume in the left globus pallidus. Moreover, the observed effect sizes (partial R2 = 0.176 for HTS and up to 0.15 for the NimpCimpPnor combination) indicate measurable associations with regional gray matter variability after adjusting for age and sex. These findings indicate that different toritsukuroi-related response patterns show differential structural associations. Although some lateralized associations were observed, no clear or systematic pattern of hemispheric dominance was apparent across regions.
In a previous study, HTS and the NimpCimpPnor combination demonstrated high specificity and strong associations with amyloid and tau PET, as well as plasma AD biomarkers. HTS positivity showed the highest specificity and positive predictive value for both amyloid and tau PET (≥0.93 and ≥0.87). 6 The combined NimpCimpPnor profile showed the best specificity (0.972) and strong biomarker associations. 6 These screening responses were strongly correlated with AD blood biomarkers, such as the Aβ42/40 ratio and plasma phosphorylated tau 181 (pTau181). The present structural findings extend those observations by identifying regional gray matter volume differences associated with these response profiles. Moreover, each response profile was associated with atrophy in distinct brain regions: HTS with the hippocampus and parahippocampal gyrus, regions closely tied to memory impairment; the NimpCimpPnor combination with medial and inferior temporal areas, including temporal association cortices important for semantic processing; Nimp with widespread temporal lobe regions such as the inferior temporal gyrus, middle temporal pole, superior temporal gyrus, and medial temporal structures, which include regions critical for language comprehension and social cognition; and Cimp with the parahippocampal gyrus, dorsolateral prefrontal cortex, and additional frontal and occipital regions that support executive and self-monitoring functions. Whereas the NimpCimpPnor combination was closely associated with atrophy in brain regions typically affected in AD, associations with HTS positivity were largely limited to the right hippocampus. This pattern is consistent with more focal or heterogeneous structural correlates of HTS, whereas the NimpCimpPnor combination may represent a behavioral profile more closely aligned with characteristic temporal lobe involvement in AD.
In addition to regional atrophy patterns, we observed relatively larger volumes in selected regions, including the globus pallidus (NimpCimpPnor) and caudate (News). It is important to emphasize that these findings reflect relative volumetric differences within the study sample rather than demonstrated structural preservation relative to overall disease progression. Given the cross-sectional design and the absence of longitudinal atrophy trajectories, these apparent increases should be interpreted cautiously. They may reflect normalization effects, reference-scaling characteristics, segmentation variability, disease-related nonlinear volumetry trajectories, or other pathological processes such as inflammation-related pseudo-hypertrophy.
The biological significance of these relative volumetric differences remains uncertain, and it is unclear whether the observed behavioral response patterns reflect distinct mechanisms of toritsukuroi-related behavior or represent different manifestations or stages within a broader spectrum of compensatory responses emerging in the context of AD-related neurodegeneration. Additionally, the differences may reflect the involvement of other regions with relatively preserved volume, such as the globus pallidus. Further studies in larger cohorts will be needed to clarify these mechanisms.
Finally, no significant associations were observed between brain atrophy and responses related to pleasure. This finding is consistent with a previous study, which reported that Pimp was not linked to AD biomarkers and was highly specific (0.854) for non-AD tauopathies. 6 Pimp may reflect apathy and inertia, symptoms frequently observed in non-AD tauopathies such as frontotemporal lobar degeneration with tau pathology. 6 In addition, cultural factors and the subjective nature of pleasure-related assessment may have reduced sensitivity to detect subtle changes in this domain, particularly in a socially adaptive population. As the present study focused on the AD continuum, future studies incorporating other neurodegenerative diseases, particularly non-AD tauopathies, as well as culturally diverse cohorts may help clarify the neuroanatomical correlates of these responses.
This study has several limitations. First, the cross-sectional design and single-center retrospective nature of the study limit causal inference and generalizability. The sample was limited and relatively homogenous, consisting primarily of highly educated, urban-dwelling Japanese participants, and no independent replication sample was available. The preclinical AD subgroup was particularly limited in number, which may have reduced the stability of subgroup-specific estimates and reduced sensitivity to detect subtle associations at this disease stage. Accordingly, findings across the AD continuum should be interpreted as reflecting overall trends rather than definitive stage-specific effects. Cultural factors, such as heightened social awareness, may also influence the prevalence of certain behavioral responses, including toritsukuroi.
Second, the lack of pathological confirmation constrains interpretation of the underlying disease processes. Larger, multicenter studies with more diverse populations, integrating multiparametric neuroimaging approaches—such as analyses of cortical thickness trajectories, hemispheric asymmetry, and environmental modulation of brain structure26,27 —will be needed to confirm and extend these results. Longitudinal MRI follow-up of this cohort is currently underway and may help clarify the temporal relationship between structural brain changes and toritsukuroi-related behavioral profiles.
Third, although Neucop-Q responses were categorized using predefined criteria as described in references 6 and 10, the distinction between “normal” and “impaired” responses relies partly on clinical judgment, which may introduce subjectivity and potential rater bias.
Forth, technical limitations related to voxel-based morphometry and potential segmentation errors may affect the accuracy of regional brain volume measurements. Additionally, proportional normalizing of structural volumes may introduce bias by disproportionately affecting smaller brain regions.
Finally, several statistical limitations should be noted. Although we applied FDR correction to control for multiple comparisons, results with p values close to the significance threshold should be interpreted cautiously. The wide confidence intervals observed in the logistic regression analyses may reflect limited sample size, subgroup imbalance, or model instability (e.g., quasi-separation or collinearity) rather than precise estimates of effect magnitude.
Conclusion
Brain volumetry revealed that specific clinical response profiles were associated with distinct patterns of regional gray matter volume differences across individuals spanning the AD continuum. HTS responses were associated with reduced right hippocampal volume, whereas the NimpCimpPnor combination was linked to more extensive medial and inferior temporal atrophy with relatively larger pallidal volumes. Longitudinal studies in larger and more diverse cohorts are warranted to determine whether these behavioral profiles contribute to early phenotyping and prognostic stratification along the AD continuum. Such work may help inform future investigations into behavior-based clinical assessment strategies.
Supplemental Material
sj-docx-1-alr-10.1177_25424823261437682 - Supplemental material for Distinct brain volume changes associated with the head-turning sign and Neucop-Q response patterns in Alzheimer's disease
Supplemental material, sj-docx-1-alr-10.1177_25424823261437682 for Distinct brain volume changes associated with the head-turning sign and Neucop-Q response patterns in Alzheimer's disease by Memi Watanabe, Shogyoku Bun, Atsushi Shimizu, Yu Iwabuchi, Susumu Mori, Masahiro Jinzaki, Masaru Mimura and Daisuke Ito in Journal of Alzheimer's Disease Reports
Footnotes
Acknowledgements
[18F] Florzolotau, the tau PET tracer used for this research, was provided by APRINOIA Therapeutics, Inc. The authors would like to thank Drs. Sho Shimohama, Keisuke Takahata Hajime Tabuchi, Ms. Natsumi Suzuki, Ayaka Morimoto, Azusa Oosumi, of the Department of Neuropsychiatry, Mr Takayuki Hoshino, Ms. Yuka Hoshino, Dr Morinobu Seki of the Department of Neurology, for their help with the PET examinations and image processing at Keio University School of Medicine.
During the preparation of this work the authors used ChatGPT (OpenAI) to assist with R programming for data analysis. After using this tool, the authors reviewed and edited the content as needed and take full responsibility for the content of the published article.
The author would like to thank Shuya Watanabe of Rensselaer Polytechnic Institute (RPI), Troy, NY, USA, for his valuable advice on programming and assistance with the literature search.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee for Human Research of the Keio University School of Medicine (#N20170237).
Consent to participate
Written informed consent was obtained from all participants.
Consent for publication
Not applicable
Author contribution(s)
Funding
This research received support from the Japan Agency for Medical Research and Development (AMED) under Grant Number JP17pc0101006 and partially from the Japan Society for the Promotion of Science KAKENHI Grant Number 16H06277. The initial grant (number 17pc0101006) was awarded by AMED to EISAI Co., Ltd (![]() ), and a portion was subsequently allocated to Keio University School of Medicine. Neither AMED nor EISAI participated in the study design, data collection, analysis, or manuscript preparation. However, both organizations reserve the right to review the manuscript for intellectual property potential and may withhold publication if it contains significant new intellectual property.
), and a portion was subsequently allocated to Keio University School of Medicine. Neither AMED nor EISAI participated in the study design, data collection, analysis, or manuscript preparation. However, both organizations reserve the right to review the manuscript for intellectual property potential and may withhold publication if it contains significant new intellectual property.
Declaration of conflicting interests
D.I. is a Principal Investigator at Keio University of the Clarity AD Clinical Trial (NCT03887455) and received honorariums from Daiichi Sankyo, Nihon Medi-Physics, Kowa, PDRadiopharma, Eli-Lilly, and Eisai. There are no other relationships or activities that could appear to have influenced the submitted work.
S.M. is one of the co-founders of AnatomyWorks and Corporate M. S.M. is CEO Corporate M. These arrangements are being managed by the Johns Hopkins University in accordance with its conflict of interest policies.
The remaining authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data supporting the findings of this study are available on request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.