
Abstract
In recent years, increasing attention has been directed toward the role of immune responses in the pathogenesis of Alzheimer's disease (AD). The pathological proteins amyloid-β (Aβ) and tau protein are closely associated with immune dysregulation and neuroinflammatory processes during AD progression. Peptide vaccines targeting Aβ and tau have emerged as an active immunotherapeutic strategy designed to induce antigen-specific immune responses against pathological protein aggregates, and several candidates have advanced to early-phase clinical trials. Although preliminary studies have demonstrated acceptable safety profiles and the ability to elicit immune responses, substantial challenges remain in vaccine design, epitope selection, and clinical translation. This review summarizes current progress in peptide vaccine development for AD and discusses their potential applications from an immunological perspective.
Introduction
With the ageing of the population, the prevalence of Alzheimer's disease (AD) is projected to increase rapidly. 1 Epidemiological studies indicate that approximately 30–35 million people worldwide are estimated to be living with AD, and this number is projected to rise to 100 million by 2050. 2 Consequently, identifying disease-modifying therapeutic strategies for AD remains a major challenge in contemporary medicine. Cholinesterase inhibitors and the NMDA receptor antagonist memantine are the primary FDA-approved drugs for AD. However, these therapies mainly provide symptomatic relief by improving cognition and daily functioning and do not halt or reverse disease progression.3,4
Recent studies have demonstrated the important role of the immune response in AD pathogenesis,5–7 where peptide vaccines targeting amyloid-β (Aβ) and tau have shown promise.8,9 Aβ and tau pathology are closely associated with neuroinflammatory responses observed in the disease. 10 Peptide vaccination aims to induce a controlled immune response against these proteins, potentially halting neurodegenerative processes.11–14
This review summarizes recent advances in peptide vaccines for AD, focusing on their immunological mechanisms, clinical development, current limitations, and the key challenges and potential strategies involved in developing effective AD vaccines.
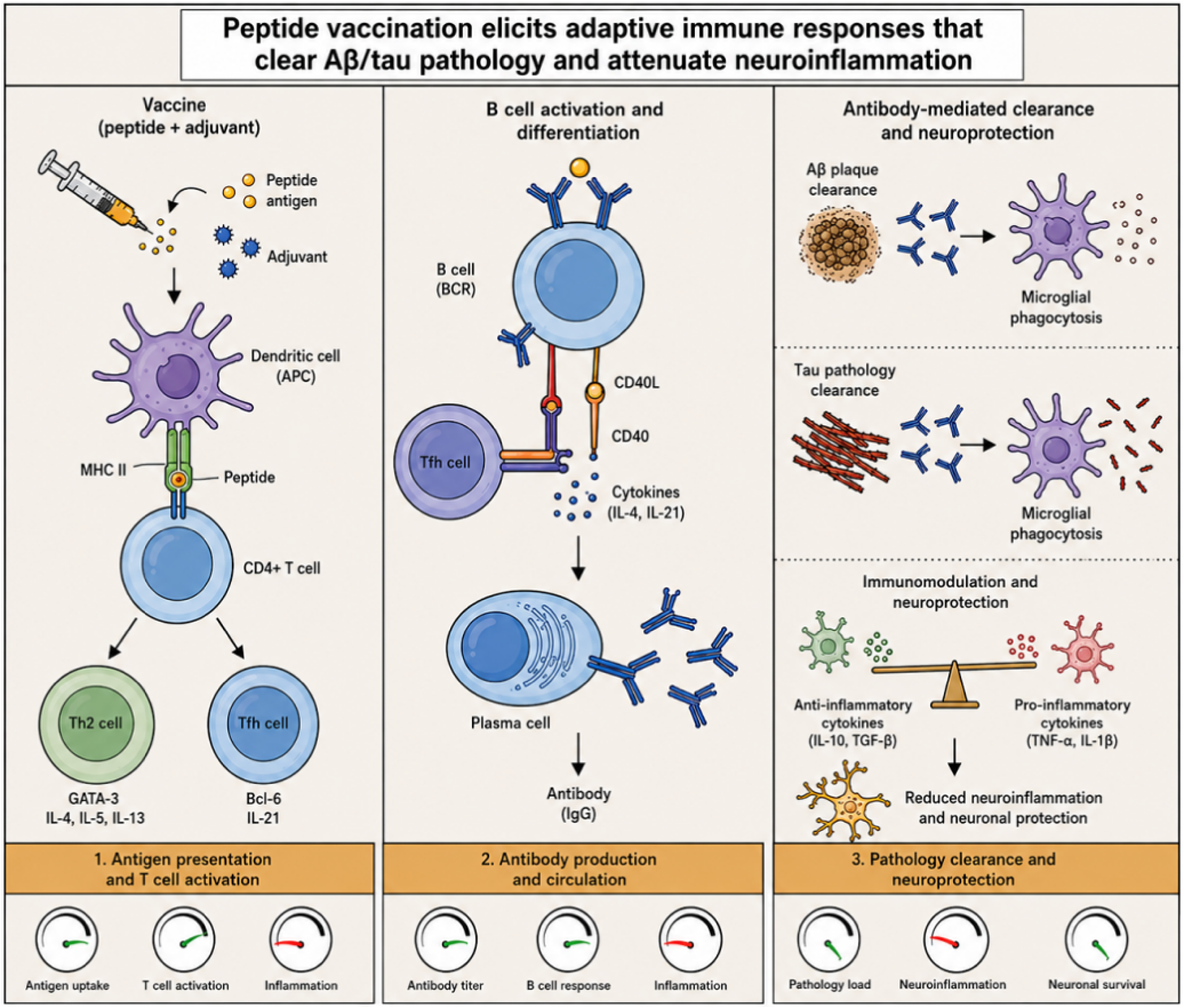
Mechanisms of peptide vaccine–mediated immunotherapy in Alzheimer's disease.
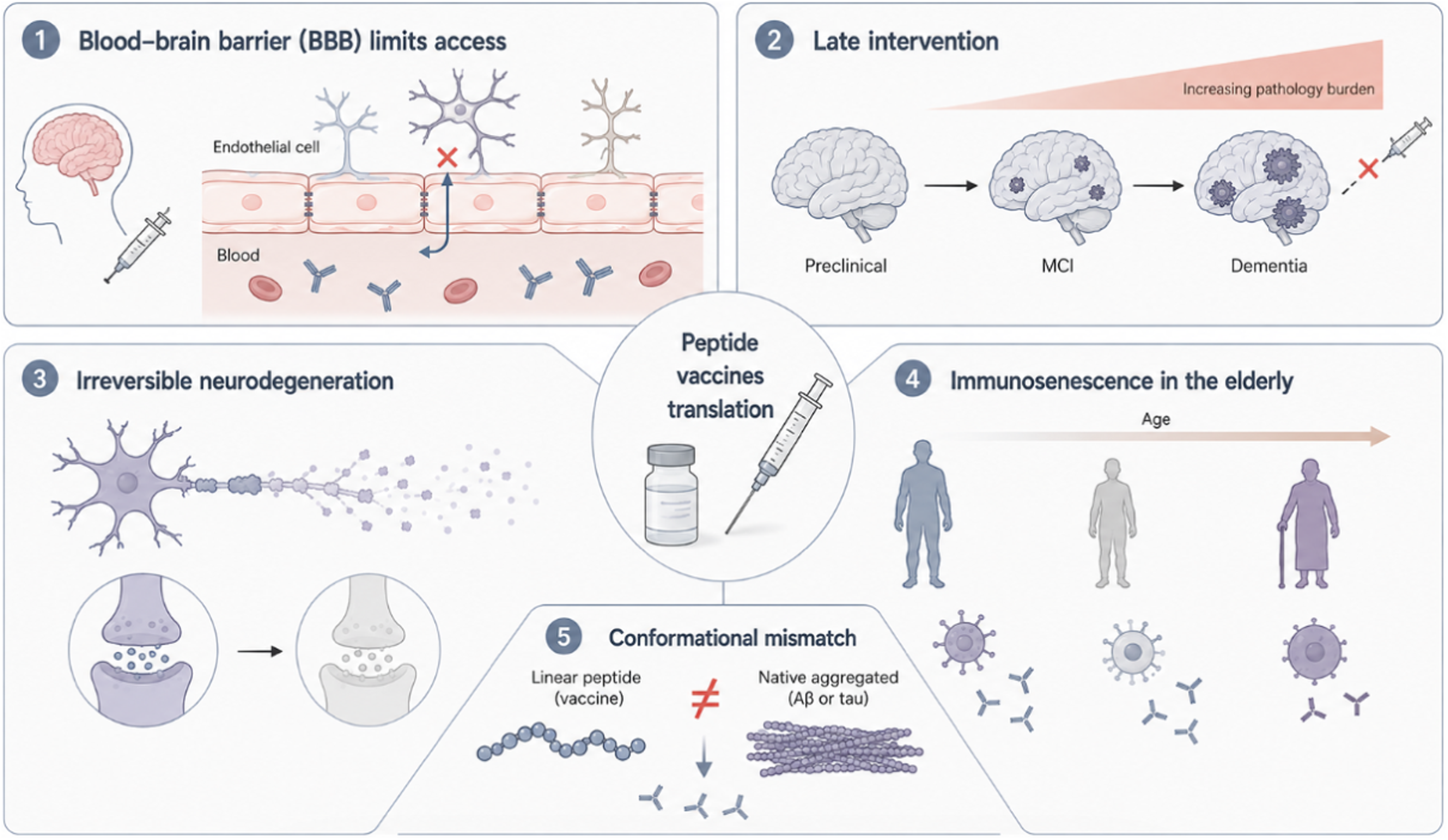
Challenges in the clinical translation of peptide vaccines.
The literature discussed in this narrative review was primarily retrieved from PubMed and Web of Science databases, covering studies published between 2015 and 2026. Search terms included “Alzheimer's disease”, “peptide vaccine”, “amyloid-β (Aβ)”, “tau”, “immunotherapy”, and “active immunization”. Priority was given to representative studies, high-quality clinical trials, and recent advances closely related to the topic.
Immunological basis of peptide vaccines for Alzheimer's disease
Immune responses to amyloid-β
Aβ is generated through the sequential cleavage of the amyloid-β protein precursor (AβPP) by β- and γ-secretases, producing Aβ peptides such as Aβ40 and the more aggregation-prone Aβ42.15,16 In contrast, α-secretase cleavage occurs within the Aβ domain of AβPP, thereby preventing Aβ generation and promoting the non-amyloidogenic pathway with neuroprotective effects.17,18 Insoluble Aβ fragments aggregate extracellularly to form senile plaques, a hallmark neuropathological feature of AD. These plaques activate microglia and astrocytes, triggering neuroinflammation and oxidative stress, which in turn exacerbate neuronal injury.19,20 Aberrant activation of the innate immune system accelerates Aβ deposition and the progression of neurodegeneration. 21 Vaccine therapy targeting Aβ is considered promising because Aβ accumulation, aggregation, and seeding processes contribute to AD pathology, and removing Aβ could reduce its toxic effects.22,23
Immune responses to tau protein
Tau primarily functions as a microtubule-associated protein, promoting microtubule assembly and stabilizing neuronal microtubules, which is essential for maintaining axonal transport and neuronal structure.24,25 Improper post-translational modifications of tau, particularly hyperphosphorylation, are central to the pathogenesis of AD. 26 Hyperphosphorylated tau loses its ability to stabilize microtubules, leading to microtubule disassembly, synaptic dysfunction, mitochondrial damage, and neuroinflammation—factors that collectively contribute to neurodegeneration and cognitive decline.27,28 Hyperphosphorylation promotes the aggregation of tau into neurofibrillary tangles, a hallmark pathology of AD closely associated with disease progression and severity.29,30 Experimental studies indicate that hyperphosphorylated tau has an increased propensity to aggregate and form toxic fibrils and may trigger further pathological tau aggregation, resulting in oxidative stress and neuronal apoptosis. 31 Tau is thought to propagate in a prion-like manner. Oligomeric tau species secreted into the extracellular space can propagate between cells through uptake and release mechanisms, thereby inducing misfolding of endogenous tau in recipient neurons,32,33 Despite challenges in clinical trials, immunotherapy remains an actively investigated therapeutic strategy targeting tau propagation, aiming to modulate disease progression by targeting the propagation behavior of tau (Figure 1).34,35
Development of peptide vaccines for Alzheimer's disease
Active and passive immunotherapy
Both active vaccination and passive antibody-based immunotherapy have been extensively investigated as strategies to target Aβ and tau pathology in the treatment of AD. 36 Among these, passive immunization primarily involves the exogenous infusion of monoclonal antibodies (mAbs) targeting Aβ to clear cerebral amyloid plaques, thereby delaying disease progression. 9 Representative antibodies include lecanemab (targeting Aβ42 protofibrils) 37 and donanemab (recognizing N-terminal pyroglutamate-modified Aβ plaques). 36 Both have demonstrated significant plaque-clearing capabilities in phase III clinical trials.35,38 Unlike first-generation antibodies, these second-generation antibodies selectively target aggregated pathological Aβ rather than monomeric forms, a feature closely associated with improved clinical benefits. 39
Despite these advances, the overall clinical benefits observed in patients remain relatively modest, and caution is required regarding side effects such as amyloid-related imaging abnormalities (ARIA), with a higher susceptibility in APOE ε4 carriers. 40 Additionally, issues such as heterogeneity in clinical trial outcomes and serious adverse events (e.g., meningoencephalitis) observed in early active immunization trials need to be addressed.41–43
However, several practical limitations hinder the widespread clinical application of passive immunotherapy: challenges in selecting appropriate target antigens, the need for lifelong repeated administration, high costs, and the fact that the blood–brain barrier (BBB) severely restricts the brain entry of antibodies.44,45 Another passive immunization strategy involves intravenous administration of immunoglobulins to treat AD. However, these agents have low specificity for oligomeric Aβ, making them inefficient at clearing toxic Aβ and potentially causing autoimmune-related complications. 46
Active immunization strategies for AD can be broadly divided into two categories: peptide vaccines, which are subunit vaccines that possess specific Aβ or tau sequences that contain specific lymphocyte epitopes and can selectively elicit B-cell or T-cell responses, and DNA vaccines are created by inserting target protein DNA sequences into plasmids or viruses, which are then inoculated into the body to induce an immune response after antigen expression. In terms of safety and controllability, compared with passive monoclonal antibody therapy, peptide vaccines may present a lower risk of ARIA-related complications in early studies.47,48
Advantages and design considerations of peptide vaccines
Peptide vaccines for AD are generally composed of three core components: (1) disease-specific peptide epitopes targeting Aβ or tau proteins; (2) carrier proteins or delivery platforms; and (3) immunostimulatory adjuvants. Among these, the peptide epitope represents the central antigenic element of vaccine design. These epitopes are typically engineered as B-cell epitopes to induce highly specific humoral immune responses against pathological Aβ or tau aggregates while minimizing the risk of aberrant autoreactive T-cell activation and associated neuroinflammatory toxicity. Depending on the design strategy, these epitopes may consist of native peptide fragments, chemically modified peptides, mimotopes, or rationally engineered synthetic sequences optimized for enhanced immunogenicity and conformational specificity. To improve antigen presentation and immune potency, peptide epitopes are frequently combined with carrier proteins, virus-like particles (VLPs), or nanotechnology-based delivery systems, while adjuvants are incorporated to enhance immune activation and shape favorable immunological profiles.
A major consideration in peptide vaccine design is the selective induction of immune responses against pathological Aβ or tau proteins while avoiding excessive inflammatory T-cell activation. The experience with the AN1792 vaccine highlighted the importance of excluding pro-inflammatory T-cell epitopes, as the inclusion of such epitopes induced detrimental Th1-mediated immune responses. Immunoinformatic approaches are therefore increasingly used to identify epitopes that maintain sufficient immunogenicity while promoting a controlled cytokine profile.49,50 Currently, most AD peptide vaccines retain N-terminal B-cell epitopes while removing C-terminal T-cell epitopes to minimize Th1 activation; some platforms additionally preserve Th2-associated epitopes to enhance protective humoral immunity. Overall, the goal of AD peptide vaccine development is to achieve a balance between robust antibody production and minimal inflammatory T-cell responses, thereby maximizing therapeutic efficacy and safety. 51 Furthermore, because Aβ and tau exhibit synergistic pathogenic interactions during disease progression, vaccine development has gradually shifted from single-target strategies toward multi-target approaches simultaneously engaging both pathological proteins.
Compared with inactivated or live-attenuated vaccines, peptide vaccines generally exhibit relatively low immunogenicity, making optimization of peptide design and adjuvant strategies essential.52,53 Current approaches to enhance immunogenicity include multivalent epitope presentation using VLPs or nanoparticles, optimization of adjuvant formulations, and refinement of vaccination regimens.
Aβ peptide vaccines
CAD106 is a complex of B-cell epitope (Aβ1‒6, DAEFRH) peptides derived from Aβ bound to Qβ phage shell proteins, 54 designed to elicit Aβ-specific antibody responses without activating harmful T-cell responses. A single complex contains 350‒550 peptides, which greatly increases the efficiency of antigen presentation. Clinical trials in patients with mild AD have demonstrated that CAD106 is generally safe and well tolerated, with no reported cases of meningoencephalitis or central nervous system inflammation, even after repeated and long-term administration.55,56 The 450 μg dose of CAD106 exhibited a more favorable balance between antibody response and tolerability compared to lower doses, inducing robust serological responses in the majority of treated patients.54,57 Longitudinal positron emission tomography (PET) imaging analyses in prevention-oriented studies demonstrated reduced amyloid accumulation over time in cognitively unimpaired APOE ε4 carriers receiving CAD106. 58 Long-term studies have shown sustained antibody titers without unexpected safety concerns, supporting CAD106 as a significant candidate for both prevention and treatment of AD. 59 CAD106 has been evaluated in phase II studies and prevention-oriented programs, although its long-term clinical efficacy remains under investigation.
UB-311 consists of two synthetic B-cell epitopes (Aβ1–14) fuzed to different Th2 cell epitopes. The vaccine formulation also includes adjuvant components such as oligonucleotide sequences and alum to maintain stable immunogenicity. 12 Preclinical studies in transgenic mice and non-human primates demonstrated strong immunogenicity, reduction in Aβ oligomers, protofibrils, and plaque burden, underscoring its therapeutic potential. Phase 1 clinical trials showed UB-311 to be safe and well-tolerated, with injection site swelling as the most common adverse event and a 100% antibody responder rate; Preliminary exploratory analyses over 78 weeks suggested trends toward slower cognitive decline, particularly in ADAS-Cog-related measures. A phase 2a randomized, double-blind, placebo-controlled study confirmed safety and tolerability over 78 weeks, with a robust immune response maintained at 93% antibody positivity and manageable adverse events including injection-site pain and amyloid-related imaging abnormalities. Although primarily focused on safety and immunogenicity, these trials revealed trends toward cognitive benefit in early-stage AD, providing a rationale for further development of UB-311. Overall, UB-311 represents a promising vaccine candidate with a favorable safety and immunogenicity profile, potentially capable of slowing cognitive decline in mild AD. 60
AFFITOPE technology is a novel peptide vaccine approach that uses artificially designed short peptides, typically six amino acids long, which structurally mimic conformational epitopes of target proteins such as Aβ42 in AD without sharing full sequence identity with the natural protein. This design aims to induce a strong antibody response while avoiding autoimmune reactions by not activating autoreactive T cells and focusing antibody specificity exclusively on pathological targets like Aβ, preventing cross-reactivity with related proteins such as AβPP. Two main AD vaccines developed using AFFITOPE technology, AD01 and AD02, target the N-terminal free sequence of Aβ to induce cross-immunity; clinical phase I trials have yielded favorable safety and immunogenicity profiles, with AD02 advancing toward phase II studies for potential disease-modifying effects.61,62 AFFITOPE vaccines have also shown efficacy in clearing oligomeric Aβ species and reducing amyloid burden in preclinical models, improving cognitive functions without triggering harmful immune responses. 63
ABvac40 is a therapeutic vaccine candidate composed of multiple copies of the C-terminal fragment (Aβ33–40) of Aβ40 conjugated to the carrier protein keyhole limpet hemocyanin (KLH), adjuvanted with aluminum hydroxide. Specifically targeting the C-terminal end of the Aβ40 peptide, its design aims to circumvent potential T-cell epitopes that could trigger adverse immune responses. An initial Phase I clinical trial demonstrated a favorable safety profile and elicited robust immune responses, with approximately 92% of patients developing specific anti-Aβ40 antibodies following three injections. 47 A subsequent randomized, double-blind, placebo-controlled Phase II trial demonstrated that ABvac40 was safe and well-tolerated in patients with mild cognitive impairment or very mild AD. Notably, the treatment showed no cases of amyloid-related imaging abnormalities-edema (ARIA-E), and the incidence of ARIA-hemorrhage (ARIA-H) was comparable to placebo. The vaccine induced a specific and sustained immune response, with antibodies detected in both plasma and cerebrospinal fluid, indicating effective penetration into the central nervous system. Over the treatment period of the phase II trial, exploratory cognitive and MRI volumetric analyses showed trends favoring ABvac40 compared with placebo, supporting its potential as a disease-modifying therapy. 64
Beyond the aforementioned vaccines, several others have recently demonstrated favorable safety profiles in animal models. The Aβ3-10-KLH vaccine, which conjugates the Aβ peptide to KLH to enhance immunogenicity, has been shown in murine models to reduce Aβ pathology, neuroinflammation, and cognitive deficits by inducing robust humoral immune responses and decreasing neurodegenerative markers. 65 Similarly, the CTB-Aβ15 fusion vaccine, linking the Aβ1–15 sequence to the cholera toxin B subunit, has elicited antibody production and improved cognitive function in preclinical studies. 66 A novel B-cell epitope vaccine targeting Aβ1–10, generated by conjugating this peptide to carrier proteins such as ovalbumin (OVA) or keyhole limpet hemocyanin, has been shown to markedly reduce Aβ deposition, attenuate neuroinflammation, and improve cognitive function. 67 Additionally, AV-1986R/A—a vaccine directed against the highly pathogenic pyroglutamate-modified Aβ (pEAβ)—elicits a highly selective immune response and efficiently clears cerebral pathology. 10 Furthermore, the oligomer-targeting peptide vaccine E22W42 specifically induces antibody production without triggering autoimmunity, while also improving spatial working memory performance in APP/PS1 transgenic mouse models of AD (Table 1). 68
Summary of Aβ-targeting peptide vaccines for Alzheimer's disease.
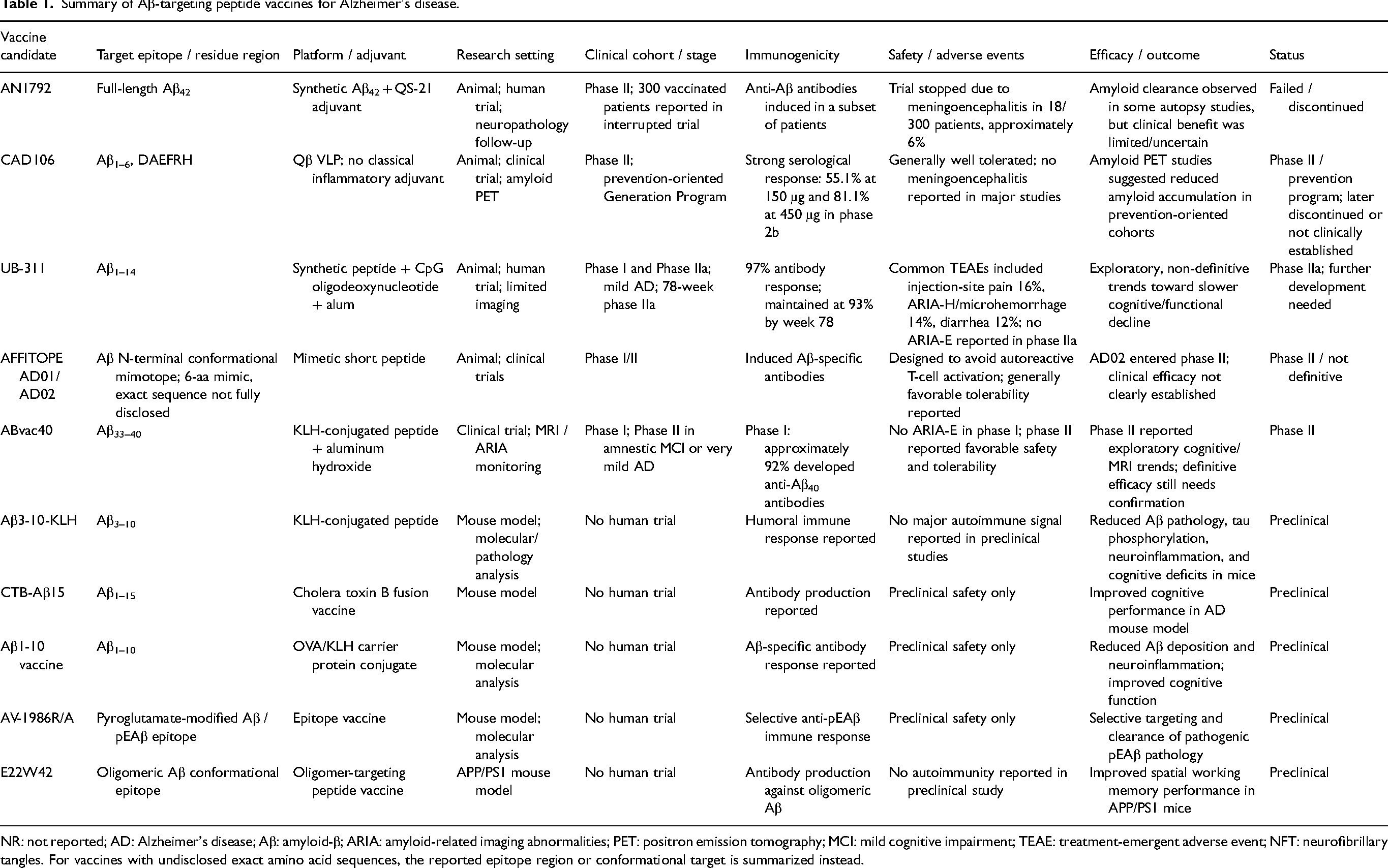
NR: not reported; AD: Alzheimer's disease; Aβ: amyloid-β; ARIA: amyloid-related imaging abnormalities; PET: positron emission tomography; MCI: mild cognitive impairment; TEAE: treatment-emergent adverse event; NFT: neurofibrillary tangles. For vaccines with undisclosed exact amino acid sequences, the reported epitope region or conformational target is summarized instead.
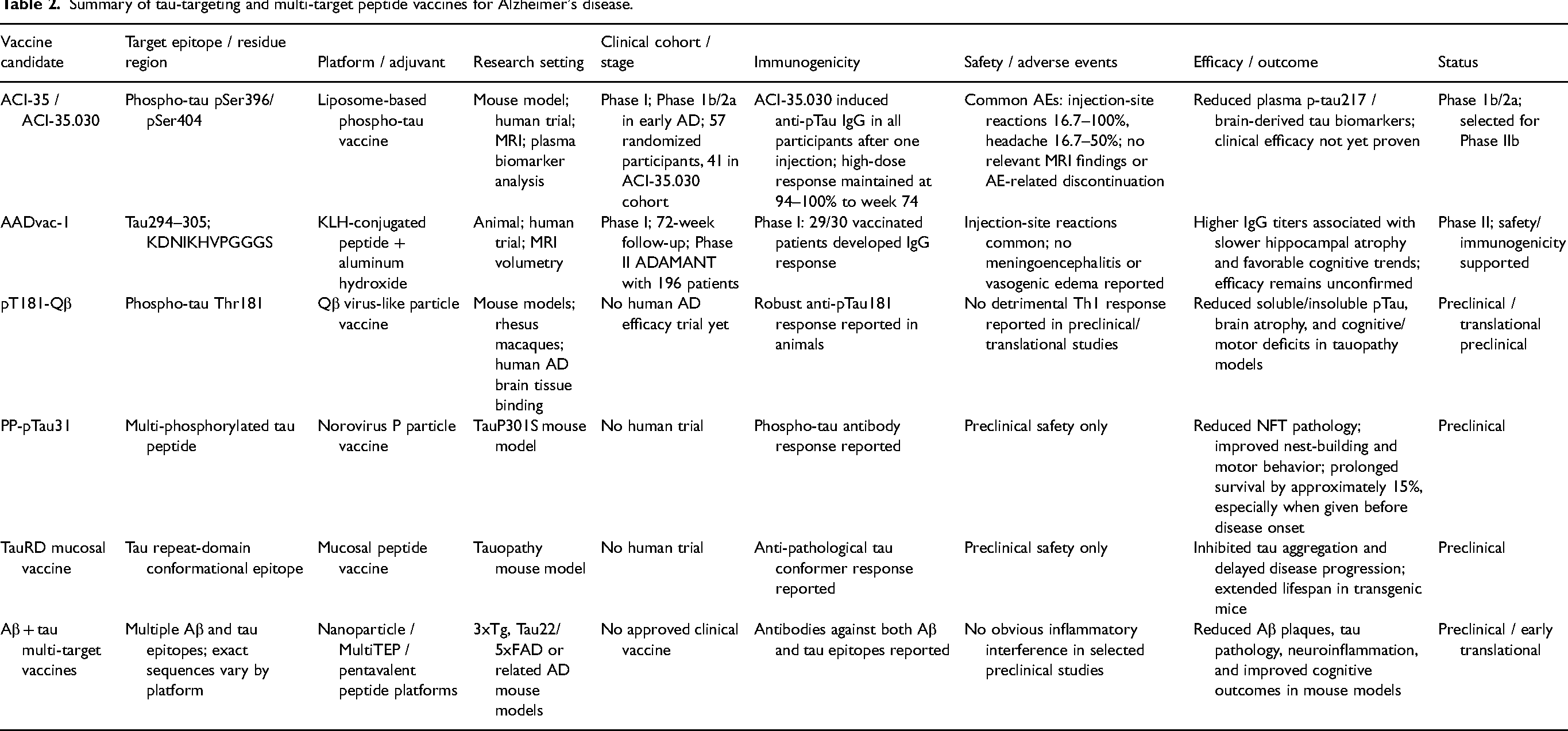
Summary of tau-targeting and multi-target peptide vaccines for Alzheimer's disease.
Tau peptide vaccines
Given its independent pathogenic role in AD and its parallel significance to Aβ in driving neurodegeneration and cognitive decline, tau has emerged as a critical therapeutic target. In response, a range of peptide-based vaccines targeting pathological tau epitopes have been developed, demonstrating promising preclinical and early-stage clinical efficacy.69,70
ACI-35 is a liposome-based vaccine comprising synthetic tau peptides phosphorylated at serine residues 396 and 404 to mimic pathological tau aggregates and elicit a targeted immune response. The liposomal formulation enhances antigen delivery and immunogenicity by promoting selective binding to pathological tau while avoiding cross-reactivity with non-phosphorylated tau, thereby improving its safety profile.71,72 In preclinical studies using two mouse models, ACI-35 induced robust phospho-tau-specific IgG antibodies, reduced pathological tau species in brain tissue, and improved motor function, demonstrating its efficacy in mitigating tau pathology and associated symptoms. 73 In a phase I/II clinical trial, a single dose of ACI-35.030 elicited superior IgG responses compared to earlier formulations, demonstrating selective binding to AD paired helical filaments. The vaccine was well tolerated, with no safety-related discontinuations or MRI abnormalities. Exploratory analyses revealed significant reductions in plasma p-tau217 and brain-derived tau levels relative to placebo after repeated immunization during the phase 1b/2a trial, supporting the continued development of an ongoing phase IIb trial. 74
AADvac 1 contains a synthetic tau fragment corresponding to residues 294 305 of human tau (KDNIKHVPGGGS), a peptide sequence associated with pathological tau misfolding and aggregation. 75 The KLH carrier in AADvac-1, combined with the aluminum hydroxide adjuvant, stimulates Th2 cell responses and humoral immunity, thereby eliciting robust IgG antibody responses in treated patients. Phase I clinical evaluation demonstrated that AADvac-1 is generally safe and well-tolerated, with the most common adverse events being injection site reactions such as erythema and swelling; no cases of meningoencephalitis or angioedema were reported. Robust immunogenicity was evidenced by strong IgG antibody responses in 29 out of 30 treated patients. 76 A 72-week follow-up study from the initial phase I trial confirmed the benign safety profile and showed that booster doses effectively restored antibody titers. Notably, In the 72-week follow-up study, higher vaccine-induced IgG titers were associated with slower hippocampal atrophy and trends toward improved cognitive outcomes, although causal clinical benefit remains to be confirmed. 77 The subsequent phase II ADAMANT trial, encompassing 196 patients, further substantiated the safety profile and immunogenicity of AADvac-1. 78 These findings suggest that current evidence supports the safety and immune responses of AADvac-1 in AD patients; however, its therapeutic efficacy warrants further investigation.
The pT181-Qβ vaccine is a VLP-based immunotherapy targeting tau phosphorylated at threonine 181, designed to elicit robust and durable antibody responses against pathological tau in AD. 79 In multiple murine models of tauopathy, including rTg4510 and PS19 transgenic lines, vaccination with pT181-Qβ significantly reduced both soluble and insoluble phosphorylated tau species, attenuated brain atrophy, and improved cognitive and motor functions, without inducing a detrimental pro-inflammatory Th1 response. The antibodies generated were shown to specifically recognize pathological tau in human AD brain tissue and were bioavailable within the central nervous system, underscoring their translational potential. 80
Furthermore, a plethora of peptide-based vaccines targeting tau pathology have been investigated in various preclinical and clinical studies, demonstrating significant promise as a viable strategy for preventing or slowing the progression of AD. Notably, a norovirus P particle-based multi-phosphorylated tau peptide vaccine (PP-pTau31) markedly ameliorated neurofibrillary tangle formation, improved nest-building and motor behavioral performance, and prolonged survival by approximately 15% in TauP301S transgenic mice, particularly when administered before disease onset. 81 In parallel, a mucosal vaccine targeting the tau repeat domain (TauRD), which selectively recognizes aggregated tau conformations, potently inhibited tau aggregation and delayed disease progression, leading to a significantly extended lifespan in transgenic mouse models. 82
Vaccines targeting both Aβ and tau have recently emerged as a promising strategy to address the multifactorial pathology of AD. Preclinical studies in transgenic mouse models have demonstrated that such vaccines elicit robust antibody responses against both Aβ and phosphorylated tau, leading to significant reductions in amyloid plaques, tau tangles, and neuroinflammation, alongside improved cognitive function. 83 For instance, a pentavalent nanoparticle vaccine displaying multiple Aβ and tau peptides induced antibodies to all epitopes without immune interference and was well-tolerated with no adverse inflammatory responses. 8 Similarly, a combination vaccine based on the MultiTEP platform generated high-titer antibodies and effectively reduced soluble and insoluble forms of both pathological proteins in double-transgenic mice. 14 Despite these encouraging preclinical results, clinical trials of dual-target vaccines remain limited and in early stages, with no multi-target vaccines yet approved (Table 2).7,84
Challenges and future perspectives of peptide vaccines
Most phase I and phase II clinical trials of vaccines generally report no serious adverse events, such as aseptic meningoencephalitis, hemorrhage, or neuroinflammatory reactions. However, in specific vaccines like CAD106, UB-311, and AADvac1, some systemic and local reactions, including nasopharyngitis, injection-site erythema, swelling, and fever, have been observed.85,86
Despite encouraging safety profiles and immunogenicity observed in early-phase studies, the overall clinical efficacy of AD peptide vaccines remains limited, highlighting multiple unresolved scientific and translational challenges.87,88
Scientific and translational challenges in peptide vaccine development for Alzheimer's disease
One major challenge in vaccine development is the induction of high-affinity protective antibodies against pathological protein conformations at the level of vaccine design. AD-associated antigens, such as Aβ or tau, often exist in specific aggregated conformations during disease progression, whereas traditional linear peptide antigens are difficult to accurately mimic these conformational epitopes, thereby limiting the ability of vaccines to elicit effective antibody responses. In addition, some early vaccines exhibited shortcomings in antigen construction and adjuvant selection, for example by employing adjuvants that preferentially induce inflammatory Th1 immune responses rather than Th2-biased responses that are more favorable for protective humoral immunity, which to some extent increased the risk of adverse immune reactions. Meanwhile, the pathological process of AD is highly complex, involving not only Aβ deposition but also tau hyperphosphorylation and neuroinflammatory mechanisms. Consequently, vaccines targeting a single epitope or a single pathological pathway may be insufficient to comprehensively interfere with disease progression.
The BBB remains an important biological factor limiting the efficiency of immunotherapy. Only a small fraction of antibodies generated in the periphery can enter brain tissue, particularly when the BBB remains relatively intact during the early stages of disease, which restricts the effective concentration of vaccine-induced antibodies within the central nervous system.89,90 Therefore, the development of delivery strategies capable of promoting antibody transport across the BBB and maintaining stable intracerebral levels may represent an important direction for improving the efficacy of peptide vaccines.
Although some candidate vaccines have been able to successfully induce immune responses in clinical trials and have shown improvements in certain biomarkers, such as Aβ or tau levels, these changes have not consistently translated into clear clinical cognitive benefits. This phenomenon largely reflects the complex biological differences between animal models and human disease. Existing animal models of AD often reproduce only selected pathological features and fail to fully recapitulate the authentic long-term progression and network-level neurodegeneration observed in humans. Furthermore, most early-phase clinical trials primarily focus on the assessment of safety and immunogenicity rather than long-term cognitive outcomes. Consequently, even when reductions in pathological markers such as Aβ or tau are observed, significant improvements in cognitive function are frequently difficult to detect in human studies.
Finally, from the perspective of the underlying disease biology, most current immunotherapeutic strategies targeting Aβ or tau are more likely to slow or halt neurodegenerative processes rather than reverse established neuronal damage. Although several immunotherapies have been shown to markedly reduce amyloid plaques or neurofibrillary tangles in animal models, they are unlikely to restore neurons that have already undergone apoptosis or to reconstruct disrupted neural network structures. Therefore, even when vaccines effectively reduce pathological burden in the brain, corresponding improvements in cognitive performance are often difficult to demonstrate in clinical studies (Figure 2).91,92
Societal and environmental factors influencing the development and implementation of peptide vaccines for Alzheimer's disease
Beyond the scientific and translational barriers associated with peptide vaccine development, regulatory and socioeconomic factors will also influence the future implementation of peptide vaccines for AD. 52
To obtain regulatory approval, peptide vaccines generally require rigorous evaluation through multiple phases of clinical trials to comprehensively assess their immunogenicity, safety, and long-term therapeutic efficacy. 93 Importantly, substantial differences exist among global regulatory systems. Regulatory agencies such as the U.S. Food and Drug Administration (FDA) and the European Medicines Agency (EMA) often apply distinct requirements regarding clinical trial design, biomarker evaluation, and adverse event monitoring, which may increase the complexity of international collaboration and delay clinical translation. 94
From an economic perspective, peptide vaccines remain associated with considerable development costs due to the extensive preclinical investigations and large-scale clinical validation required for successful translation. Nevertheless, compared with monoclonal antibody therapies that require repeated administration and highly complex manufacturing processes, peptide vaccines may offer advantages in large-scale production capacity and long-term cost-effectiveness. 51
Equitable access to healthcare resources also represents a challenge for the real-world implementation of peptide vaccines, particularly in low- and middle-income countries where limitations in healthcare infrastructure and diagnostic accessibility may affect vaccine deployment. 95
From a public health perspective, successful implementation of peptide vaccines will likely require government-led policy support, including optimization of reimbursement strategies, expansion of public health education, and promotion of preventive healthcare programs for older adults. 96 Integrating vaccine-based prevention with healthy ageing initiatives and dementia awareness campaigns may further enhance public health literacy.97,98
Future directions in precision and preventive vaccine strategies for Alzheimer's disease
Despite the encouraging progress achieved in recent years, future research should increasingly focus on transforming peptide vaccines for AD from experimental immunotherapeutic approaches into clinically implementable interventions that are preventive, precision-oriented, and socioeconomically sustainable.
Another key factor influencing vaccine efficacy is the timing of therapeutic intervention. AD is a slowly progressive neurodegenerative disorder characterized by a prolonged preclinical phase, in which pathological alterations may begin several years or even more than a decade before the onset of clinical symptoms. However, most current clinical trials enroll patients who are already in the mild-to-moderate stages of cognitive impairment, at which point neuronal damage and synaptic loss are already extensive. Although antibodies induced by vaccination may facilitate the clearance of Aβ or tau pathology, their ability to restore cognitive function remains limited once extensive amyloid plaque deposition, neurofibrillary pathology, synaptic dysfunction, and neuronal loss have become established. Preclinical studies also suggest that prophylactic immunization is generally more effective than therapeutic vaccination after disease onset. 99 Consequently, intervention during the early or even preclinical stages of disease is likely to provide a substantially more favorable therapeutic window than vaccination after irreversible neurodegeneration has already occurred. 99 From an epidemiological perspective, a substantial proportion of individuals remain in the preclinical stage of AD, highlighting that preventive strategies may be as important as therapeutic interventions in clinical management.97,100 Accordingly, the development of more sensitive and specific early diagnostic tools, including novel plasma and cerebrospinal fluid biomarkers as well as advanced neuroimaging technologies, will be critical for identifying individuals in the preclinical stage and enabling early intervention, and may represent an important future direction for immunotherapy in AD. 101
Preventive vaccination may be particularly valuable for high-risk populations, including individuals carrying genetic susceptibility factors, exhibiting positive fluid or neuroimaging biomarkers, or presenting with early cognitive decline. Importantly, such strategies may also help address the challenge of age-associated immunosenescence. Because AD predominantly affects individuals aged 65 years and older, the progressive decline in immune responsiveness that accompanies ageing may substantially compromise vaccine efficacy. However, the vast majority of current preclinical studies continue to rely on young animal models, which fail to accurately recapitulate the aged immune microenvironment observed in elderly patients. Future studies should therefore incorporate aged animal models and systematically investigate strategies capable of enhancing vaccine immunogenicity while minimizing neuroinflammatory adverse effects in elderly populations.12,52
In parallel, precision medicine will constitute a critical foundation for the clinical translation of AD peptide vaccines. The integration of fluid biomarkers, including plasma and CSF Aβ42 and phosphorylated tau isoforms such as p-tau217, together with genetic information such as APOE genotype and longitudinal monitoring of immune responsiveness, may enable patient stratification according to pathological status, disease stage, and immunological characteristics, and individualized immune-modulatory requirements. In addition, digital biomarkers may enable continuous monitoring of cognitive, behavioral, and functional changes, thereby providing individualized assessments of vaccine efficacy while improving the efficiency of clinical trials.51,102,103
To achieve these objectives, future vaccine design must move beyond conventional single-target and traditional formulation paradigms. Given the multifactorial complexity of AD pathology, next-generation vaccine strategies will likely increasingly shift toward multi-epitope and combined Aβ/tau vaccine platforms capable of simultaneously targeting amyloid deposition and tau-mediated neurodegeneration, thereby enabling broader and potentially more effective pathological intervention.
Given the inherently limited immunogenicity of peptide vaccines for AD, together with the risk that inappropriate immune activation may provoke detrimental neuroinflammatory responses, adjuvant selection represents a critical determinant in vaccine design. For example, the aluminum-based adjuvant AD04 has demonstrated potential therapeutic benefit in patients with early-stage AD, highlighting its possible clinical relevance. 104 Meanwhile, multiple adjuvant systems, including QS21, Advax (CpG), AS02, and their combinatorial formulations, have been incorporated into various AD vaccine platforms, where they effectively enhance antibody titers against Aβ and tau while preferentially promoting humoral immune responses, thereby potentially reducing the risk of excessive inflammatory activation.85,105,106 In addition, the AFFITOPE platform, which is based on short peptide mimotopes, combined with the relatively safe aluminum hydroxide adjuvant, may improve antigen specificity while minimizing autoimmune-associated risks, underscoring the importance of synergistic optimization between adjuvants and antigen design in the development of AD vaccines. 107
To simultaneously improve immunogenicity and treatment safety, increasing attention has been directed toward next-generation vaccine delivery platforms. Nanoparticles, liposomes, VLPs, and carrier protein conjugation systems have all demonstrated the capacity to enhance antigen presentation, promote beneficial immune responses, and mitigate inflammatory reactions.47,67 For example, engineered hepatitis B core protein–based VLPs can markedly enhance peptide immunogenicity and preferentially induce Th2-biased immune responses, thereby alleviating neuroinflammation and improving cognitive decline. 108 Similarly, carrier proteins such as CRM197, OVA, and KLH have been shown to significantly enhance antibody production and ameliorate synaptic dysfunction. 6
Public health and socioeconomic implications of preventive peptide vaccination
AD imposes an enormous and continuously escalating burden on healthcare systems, families, and society as a whole. 109 Globally, dementia-related expenditures have already exceeded 1.3 trillion USD annually and are projected to rise further with ongoing population ageing. Beyond direct medical costs associated with pharmacological treatment, hospitalization, and long-term care, AD also generates substantial indirect socioeconomic losses through reduced workforce participation, premature retirement, and unpaid caregiving. Importantly, the burden of AD extends far beyond patients themselves, as caregivers and family members frequently experience sustained psychological stress, financial hardship, and reduced quality of life during disease progression. In this context, preventive and disease-modifying vaccination strategies may provide value not only by delaying pathological progression, but also by postponing the transition to advanced disease stages requiring intensive medical intervention and institutional care. Even modest delays in disease onset could substantially reduce the overall societal burden of dementia while alleviating long-term emotional and economic pressure on caregivers and families. 110
Continued advances in epitope engineering, adjuvant optimization, delivery platforms, precision-based patient stratification, and multi-target vaccine strategies may further improve vaccine efficacy and safety. With ongoing progress in early diagnosis and preventive intervention, peptide vaccines may ultimately evolve from experimental immunotherapies into clinically applicable strategies for long-term dementia prevention and management in ageing societies.
Footnotes
Acknowledgements
The authors have no acknowledgments to report.
Author contribution(s)
Funding
This work was supported by Joint Funds for the Innovation of Science and Technology, Fujian Province (grant/award number: 2024Y9123), and National Natural Science Foundation of China (grant/award number: 82301543).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.