
Abstract
Background:
This study presents the preliminary psychometrics of the Self-Assessment of Autistic Traits (SAAT) item pool, which is the first comprehensive self-report tool of autism traits for teens and adults coproduced with autistic people. Two autistic researchers led the SAAT item development and leveraged descriptions of autism by autistic people to generate items designed to encompass the internal experience of autism using strength-based accessible language.
Methods:
Autistic (N = 500) and non-autistic (n = 80) people, 16 years or older, completed the SAAT. The sample included community-ascertained autistic adult participants, as well as participants from a large academic medical center-based research network, which broadened the spectrum of participants studied to include more gender-diverse, older, and nonspeaking individuals.
Results:
Exploratory factor analysis followed by a unidimensional confirmatory factor analysis revealed four factors as follows: Modulation/Social Communication, Strengths/Passions, Brain–Body Disconnect, and Negative Community Context. Three of these factors are sensitive to autism in comparison with non-autistic people across age, gender identity, assigned gender at birth, and gender diversity status.
Discussion:
The SAAT shows promise as a multidimensional self-report tool that is reliable and valid with respect to the samples that we examined. The SAAT item-set may yield a useful screening tool for people of different gender identities, assigned gender at birth, and gender diversity status, from 16 years old through adulthood, who are questioning whether they may be autistic. In addition, it has potential as a phenotyping tool that captures individual strengths as well as challenges and could provide information that helps guide the creation of opportunities and supports that enable autistic people to thrive. Given the preliminary nature of the current study, a cross-validation study with respect to larger and diverse groups of the sample is the necessary next step to further develop and refine the set of items as a useful tool.
Community Brief
Why is this topic important?
Clinicians don’t always recognize when people are autistic, especially when these people are teens, adults, girls, women, or gender-divergent. Recognizing autism is important because it can give people access to supports and connection to autistic communities. So, we wrote the Self-Assessment of Autistic Traits (SAAT) to measure the internal experience of autism and help catch the people who clinicians don’t recognize. The SAAT is a self-report autism questionnaire. Autistic researchers and non-autistic researchers wrote the SAAT together. However, we still need to study if people answer questions on the SAAT the way we think they will.
What is the purpose of this article?
In this article, we analyzed if the SAAT works the way we thought it would.
What did the authors do?
First, we collected data from 500 autistic people and 80 non-autistic people. Next, we figured out how items on the SAAT group together can make factors. We also determined whether SAAT scores were higher for autistic people than for non-autistic people. Finally, we checked if a person’s age or gender would systematically impact their SAAT score.
What did the authors find?
We found that the SAAT has four groups of items, or factors, as follows:
Factor one: Modulation/Social Communication—the control of attention, sensory information, thinking and actions, and flexibility, including repetitive actions and switching to new thoughts, social-communication abilities and preferences, and feelings of overwhelm.
Factor two: Strengths/Passions—passionate interests, attention to detail, pattern recognition, preference for routine, and other preferences and strengths.
Factor three: Brain–Body Disconnect—a disconnect between an intention or desire and the motor movement needed to act on it, also difficulty with independent demonstration of daily living skills and variability in skills.
Factor four: Negative Community Context—experiences of being treated unfairly and invalidated.
We also found that autistic people have higher SAAT scores than non-autistic people on Factors one, three, and four. Autistic people and non-autistic people scored the same on factor two. Finally, we found that a person’s age or gender did not change their SAAT score.
Why are the findings important?
The SAAT works mostly how we thought it would. But we need to edit it before it is done. These findings mean that the SAAT could become a useful autism screener, especially for adults, girls, women, and gender-diverse people. What are the next steps for the SAAT?
First, we are going to rewrite some items that did not fit into any of the four factors. Second, we will write more items about Negative Community Context, since it only has four items right now. Finally, the new SAAT will be tested with autistic and non-autistic people of all races, ethnicities, and genders to check if it works for all kinds of people. After refining the final set of items based on a more fine-tuned measurement model in a new sample, we hope the SAAT will be ready for use as an autism screener and/or phenotyping measure.
Keywords
Background
Despite clear evidence for the importance of early identification, significant disparities exist in access to an autism diagnosis. 1 Recent literature reports some progress in addressing racial and ethnic disparities, but delayed diagnosis still occurs for “female sex.” Most literature on the relationship between gender and diagnostic timing to date does not differentiate assigned gender at birth from gender identity, thus people referred to as “female” in the literature (PRF; undifferentiated in prior research as to whether “female” refers to assigned gender at birth or gender identity) are at greater risk of late or missed autism diagnosis than people referred to as male (PRM).2–7 Diversity in gender identity, which is significantly over-represented8–10 in autism, is also related to delayed autism diagnosis. 11 Unrecognized autism deprives people of timely supports, 12 increases vulnerability to abuse, 13 and is associated with depression 14 and other psychiatric comorbidities.15,16 The stakes are high in gender-related diagnostic disparities, as psychiatric comorbidity rates in autistic people assigned female at birth (AFAB) exceed those expected based on gender differences in the general population. 17 Gender diverse (GD) autistic people show increased suicidality compared with autistic cisgender or non-autistic transgender people. 18
Current assessment tools, which do not fully capture the presentation of autism in AFAB and GD people, hinder timely referral and recognition of autism in these populations.19,20 Some researchers critique these tools for lacking sensitivity in people who are older, have stronger verbal ability, and greater compensatory skills. 21 Researchers and clinicians rely on diagnostic criteria and assessment tools developed with predominantly White, cisgender male pediatric samples, creating a self-reinforcing cycle of bias, which excludes some from access to diagnosis and participation in research that informs knowledge of the autism phenotype. One meta-analysis provides evidence of this cycle of bias through its finding that studies using active case ascertainment and high-quality methodologies consistently identify a lower PRM-to-PRF ratio than the commonly reported 4:1. 7 A survey of autism diagnosticians concluded that 90% of this population view autism assessment as more challenging with PRF, citing a “mismatch between the female expression of Autism Spectrum Disorder (ASD) and instruments” commonly used to diagnose autism. 22
Sex and gender moderate the expression of autistic traits. In contrast to autistic PRM, autistic PRF show fewer repetitive motor behaviors, greater social motivation, and more gender stereotypical play, communicative gestures, and pragmatic competence. Autistic PRF have more “rehearsed impression management skills.” 23 Developmental patterns indicate that autistic PRF present as less characteristic of autism compared with autistic PRM. 24 Compensation, including rehearsal and impression management, can obscure the behavioral expression of autism, thus making information on the subjective experience important to identifying autism, especially in females and GD individuals. Autistic people’s descriptions of the inner experience of autism can enhance our understanding of measurable components of autism beyond the behavioral observations that researchers and clinicians have relied heavily on to date.
Despite early skepticism,25,26 autistic self-report is valid in many cases. 27 Autistic people’s self-report is a more powerful predictor of biological correlates of anxiety than informant report, 28 for example. Autistic youth as young as 12 years of age self-report a nuanced profile of executive function challenges that is highly consistent with their parents’ report 27 and their performance on cognitive tasks. However, currently available comprehensive autistic trait self-report questionnaires overemphasize observable behaviors and autistic traits observed in PRM. The Social Responsiveness Scale (SRS/SRS-2) 29 includes many items that ask the respondent to rate how other people perceive or react to their behavior (e.g., “I behave in ways that seem strange or bizarre to others”; “When I tell someone my reason for doing something, it strikes the person as unusual or illogical”). These items center observed traits, impose a negative interpretation of behavior, and fail to assess the reason for the actions taken. They also require the respondent to guess at the thoughts of others, which may limit the validity of the measure. Critiques of the SRS cite poor specificity30–33 and oversensitivity to behavior problems, age, and intelligence. The Autism Spectrum Quotient (AQ) 34 also has poor specificity for autism,33,35,36 as well as a strong gender bias. 37 Neither the SRS nor the AQ probe compensation or sensory experience, whereas four items on the AQ focus on dates and numbers (e.g., “I am fascinated by dates”). The Ritvo Autism and Asperger Diagnostic Scale 38 in contrast has good sensitivity and specificity for autism compared with a mixed neurotypical (NT) and other psychiatric conditions group. It also queries internal states (e.g., “I like to copy the way certain people speak and act, it helps me appear more normal”), but it includes items that: require the respondents to infer other people’s reactions to them (“I am considered a compassionate type of person”), are linguistically complex (“I keep my thoughts stacked in my memory like they are filing cards, and I pick out the ones I need by looking through the stack and finding the right one or another unique way”), and repeatedly reference “normal” behavior (“I speak with a normal rhythm”). The Comprehensive Autistic Trait Inventory 39 represents an important step forward, as a focus group of six autistic adults was consulted regarding traits to include and labeling of subscales. It also measures a broad range of autistic traits, including compensatory and sensory experiences; however, peer reviewed publications to date have focused primarily on its psychometric qualities in non-autistic adults.
Autistic communities have shared their own rich descriptions of autism online and identified a variety of traits and internal experiences that might amplify our understanding of autism as it is experienced by autistics across gender, race, ethnicity, age, and other diversity. Yet there is currently no comprehensive self-report tool designed to capture the lived experience of autism with items that are accessible and acceptable to autistic people. To fill this gap, we are developing a scientifically rigorous, reliable, and autistic-centered self-report item-set that contains items that autistic people believe are fundamental to the experience of autism and that they find acceptable and accessible. We hope that this set of items yields meaningful scores with reasonable sensitivity and specificity, allowing us to further validate the measure as a potential first-line self-screening tool. In addition, we hope that the item-set includes items that are useful for measuring the phenotype of autism, including traits that can be helpful when identifying vocational directions and support needs.
To date, a team of autistic and non-autistic clinician-researchers and measure development experts have developed an item pool of 58 descriptors of autistic traits and the inner experience of autism called the Self-Assessment of Autistic Traits (SAAT). The SAAT item pool was developed and refined under the leadership of two autistic researchers and is based on descriptions of autism written by autistic people, with iterative feedback from a panel of autistic experts and cognitive interviewing with autistic teenagers (see Ratto et al., 2023 for a full description of the SAAT development process). 40 This process resulted in an item-set that is deemed important by autistic people and presented in accessible language. SAAT items capture internal states and include aspects of autistic strengths and joy, as well as compensatory strategies. The SAAT item-set aligns well with the neurodiversity framework because it presents some traits that society often pathologizes (e.g., intense interests, repetitive actions) in a neutral or positive manner and frames autistic traits through an autistic lens (e.g., describing intense interests as deep passions, rather than “all-consuming interests that eclipse all other interests”). 19 The SAAT’s centering on the lived experiences of autistic people also led the author team to include items describing autistic traits and experiences that are not in other comprehensive measures; for example, autistic inertia, 41 loss of skills after childhood, inconsistency in demonstrating skills, and experiences of being manipulated and undermined by others.
The development team organized the SAAT item-set into five domains based on their theoretical understanding as follows: (1) Sensory/Motor Loop addresses sensory and motor experiences (e.g., My senses are extreme); (2) Strength in Specificity highlights strengths in identification of patterns and details and developing deep knowledge (e.g., I often notice details that other people don’t); (3) Social Communication focuses on communication and language (e.g., It is hard for me to come up with my own words. It is easier to repeat things I’ve heard other people say); (4) Executive Functioning and Related Traits taps flexibility, overload, burnout, and demonstration of daily living skills (e.g., I can’t always do what I need to do, because it feels like my mind and my body are disconnected); and (5) Negative Community Context, which addresses experiences of systemic discrimination and chronic social strain 42 (e.g., People tell me my experiences aren’t real).
In the present study, we evaluate the psychometric properties of the SAAT item-set to guide its further development as a freely accessible and equitable self-report measure of autistic traits and a screening tool. In recognition of the importance of the accurate and equitable representation of the autistic community, this study includes a community sample of self-identified autistic adults, as well as a rigorously characterized group of autistic and non-autistic participants in a multisite NIH Autism Center of Excellence study. We predict that the preliminary SAAT item-set will:
Exhibit five underlying hypothesized factors, representing the domains described above, Demonstrate adequate internal and test–retest reliability of factor scores, Demonstrate concurrent/known group and convergent validity of scores by:
Distinguishing autistic from non-autistic groups with or without controlling for demographic (i.e., age, gender identity, assigned gender at birth, gender diversity status) variables. Correlating with an established measure of autistic traits, the SRS-2.
29
In addition, we will explore whether SAAT scores differ based on the typical communication modality [i.e., mostly speaking, mostly Augmentative and Alternate Communication (AAC), or a combination of the two] of autistic respondents.
Methods
The current study examined SAAT responses from two samples obtained through different IRB-approved ascertainment strategies (Children’s National and University of Virginia Institutional Research Boards). All participants provided consent through procedures approved by the relevant IRB. We included an online community-ascertained group of self-identified autistic adults to broaden the demographic spectrum of included individuals, specifically autistic individuals who might be excluded from research that imposes academic research criteria for autism.7,20
Participants
Sample 1: Community Ascertainment: We recruited autistic adults (n = 440) from online autistic self-advocacy networks accessed through listservs and social media from the Autistic Self Advocacy Network and the Autistic Women & Nonbinary Network. Study inclusion criteria were as follows: age 18 years or older, a self-disclosed diagnosis of autism, Asperger’s Syndrome, or Pervasive Developmental Disorder, and complete responses to the online consent questions. We did not independently confirm participant report of autism diagnosis. We excluded participants if they provided no demographic or SAAT data or if we questioned the validity of their online responses related to one of the following: two or more illogical responses to five validity probes embedded in the SAAT item-set (e.g., I was born on February 31st); a mismatch between reported birth year and age; an unusual response to a free response question that was repeated verbatim by multiple respondents; and raised concerns regarding a bot. 43
Sample 2: Academic Medical Center Ascertainment (GENDAAR): We recruited autistic youth (n = 60), their unaffected siblings (n = 23), and NT participants (n = 57) for inclusion in the second wave of the Gender Exploration of Neurogenetics and Development to Advance Autism Research (GENDAAR) project (NIH Data Archive Data Collection #2804). We included autistic youth based on the Diagnostic and Statistical Manual of Mental Disorders autism spectrum disorder criteria, as applied by a research reliable clinician informed by the Autism Diagnostic Interview-Revised 44 and/or Module 3 or 4 of the Autism Diagnostic Observation Schedule, Second Edition. 45 We excluded participants with intellectual disability and participants under 16 years of age. Participants were included in the NT group if they did not have a diagnosis or were not suspected of having a neurodevelopmental or mental health condition and did not have autistic first- or second-degree relatives. The NT and unaffected sibling groups did not differ significantly in age, although there were more of assigned female gender at birth in the NT participants than in the unaffected siblings. The numbers of GD individuals were too small for statistical comparison. Although we could not compare the NT and unaffected sibling groups across racial and ethnic identities due to sample size limitations, the two groups did not differ in overall proportions of people of color [χ2(1) = 0.68, p = 0.41] or on age or SAAT factor scores, so we combined them into one non-autistic comparison group (n = 80) for this investigation. See Table 1 for demographics.
Demographics and Self-Assessment of Autistic Trait Scores for Autistic and Non-Autistic Groups (See Supplementary Table S1for Comparisons of GENDAAR and Community Samples)
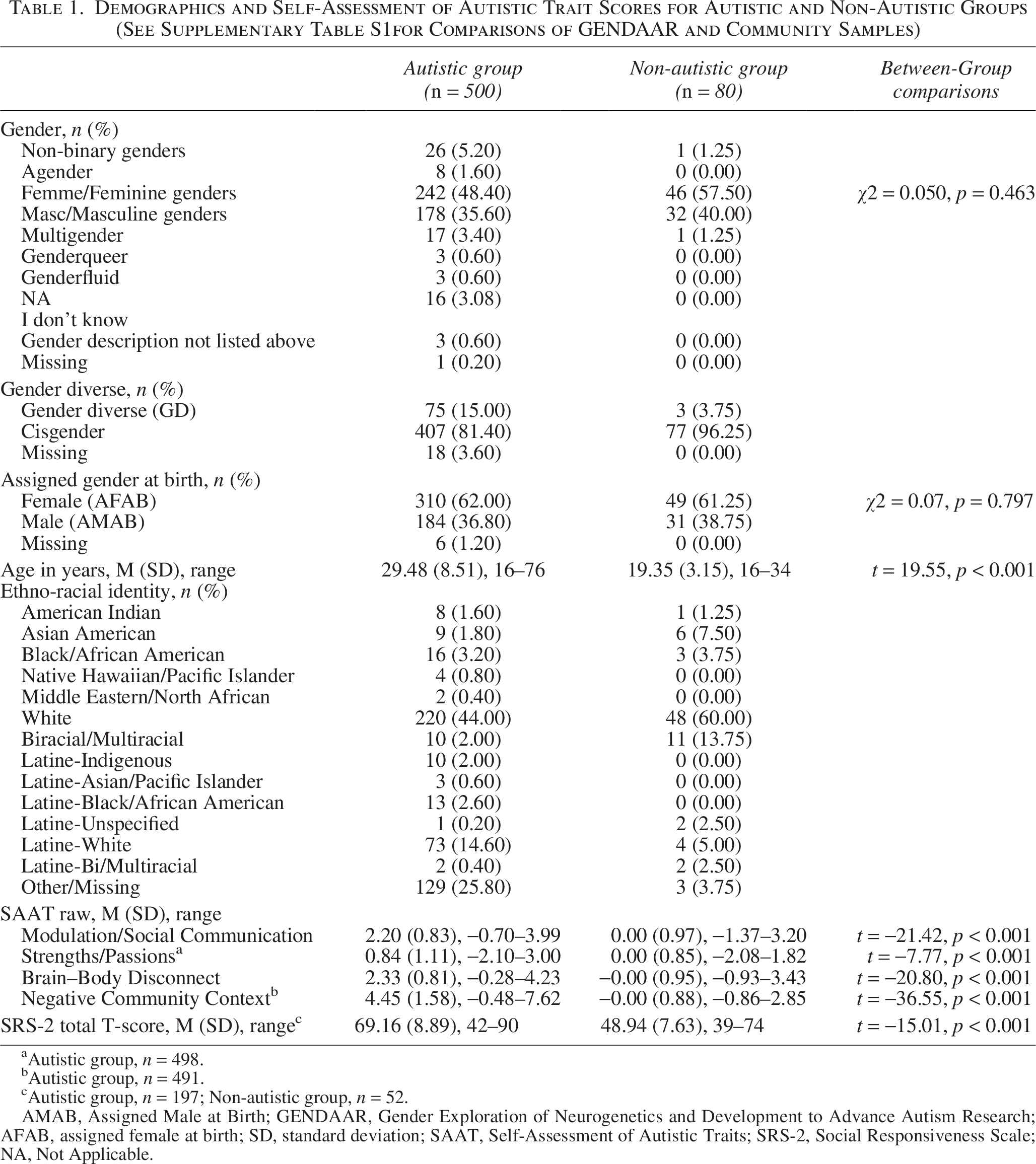
Autistic group, n = 498.
Autistic group, n = 491.
Autistic group, n = 197; Non-autistic group, n = 52.
AMAB, Assigned Male at Birth; GENDAAR, Gender Exploration of Neurogenetics and Development to Advance Autism Research; AFAB, assigned female at birth; SD, standard deviation; SAAT, Self-Assessment of Autistic Traits; SRS-2, Social Responsiveness Scale; NA, Not Applicable.
Combined Autistic Group from Samples 1 and 2: The autistic participants from Samples 1 and 2 did not differ in terms of their overall proportions of people of color [χ2(1) = 0.42, p = 0.52]. We could not compare groups across specific racial and ethnic identities due to sample size limitations and missing data. Due to investigator error, we did not initially collect data on race and ethnicity from Sample 1. Realizing this error, the team recontacted respondents and requested data on race and ethnicity, but some participants did not respond to the second query. SAAT scores for each racial-ethnic identity reported by at least 10 autistic participants are reported in Supplementary Table S1 for reference. The community sample was older and had a larger proportion of feminine genders and participants who were AFAB than the GENDAAR sample. See Supplementary Table S2. Supplementary Table S3 indicates all of the gender identities indicated by participants. Differences between Samples 1 and 2 reflect important aspects of heterogeneity within autism; thus, autistic participants from the community and GENDAAR samples were combined into one group (n = 500). See Table 1 for demographics on the combined autistic group.
Measures
Community Sample 1: We asked participants to complete the SAAT through an online survey and indicate their age, gender identity, assigned gender at birth, ethnic and racial identity (with a follow-up survey), and preferred communication modality, as indicated by selecting one of three options as follows: More than half the time I prefer to express myself by speaking aloud; More than half the time, I prefer to express myself using AAC such as typing/writing, using pictures or symbols, signing, or another approach that does not involve speaking aloud; or I use both of these methods about equally. A subset of participants also completed the SRS-2-Adult Self Report. 29 We invited a subset of participants to complete the SAAT a second time after a 2-month delay to evaluate test–retest reliability.
Academic Medical Center Sample 2: As part of a more extensive protocol which included neuroimaging, collection of genetic material, and diagnostic and cognitive/behavioral tasks, our research network collected data on participants’ age, gender identity, assigned gender at birth, and ethno-racial identity. Participants completed online surveys, including the SAAT. Those who were 18 or older also completed the SRS-Adult Self Report. 29
Measures of interest
SAAT item-set includes 58 self-report items for people 16 years of age and older. We collected SAAT response data through a REDCap survey that asked respondents to endorse whether or not each item was an accurate descriptor of their own experience. We collected responses with a slider scale that could be placed anywhere along a line. Although not apparent to the respondent, whole number scores were assigned to the slider scale position between 0 and 100, with 100 being the strongest endorsement that the item reflected their own experience. The beginning of the SAAT prompts respondents to practice using the slider scale by answering practice items not included in scoring. See Supplementary Data for the SAAT instructions, items, and response format.
SRS-2 29 Adult Self Report is a 65-item assigned sex-normed measure of autistic traits. We administered the Adult Self Report to participants in this study who were 18 and older. The measure is normed on those 19 and older. Participants responded using a four-point Likert scale (1 = Not True, 4 = Almost Always True). T-scores are generated for subdomain scores and a Total Score. Higher scores indicate higher levels of autistic traits. The SRS-2 Adult Self Report has high internal consistency (Cronbach’s alpha = 0.92–0.95) and solid interrater reliability (r = 0.61–0.95) in adults.
Data analytic approach
We investigated each of our primary hypotheses with the following statistical approaches.
The SAAT item-set will exhibit five predicted underlying factors. We conducted a confirmatory linear normal factor analysis (CFA) on data from the Combined Autistic Group (n = 500), in which each item loads on one of the five hypothesized factors, and five factors are correlated. The SAAT will demonstrate adequate internal and test–retest reliability of scores. We calculated a reliability index (i.e., proportional reduction in square error)46,47 for each factor score (the default factor score in Mplus is Expected A Posteriori), and we calculated the correlation between factor scores measured on two occasions within a subset of Community Sample 1 to evaluate test–retest reliability (n = 46). The SAAT will demonstrate concurrent/known group validity by:
Distinctive latent distributions of factors between autistic and non-autistic groups. We conducted a multiple group linear normal factor analysis with respect to two groups (autistic n = 500; non-autistic n = 80) to obtain the model-based latent distribution of the scores of known groups, then created the
a
receiver operating characteristic (ROC) curves to evaluate the specificity and sensitivity of hypothetical cutoff scores for each factor. Distinguishing autistic from non-autistic groups after controlling for age, gender identity, assigned gender, gender diversity status, and their interactions. We fitted three sets of logistic regression models with age, one of the following gender predictors, and their interactions as follows: (1) binary gender identity (masculine/feminine); (2) assigned gender at birth (AMAB/AFAB); and (3) gender divergence (yes/no) to examine whether each of the SAAT factor scores, age, and gender or their interactions are associated with group status (autistic vs non-autistic). We entered predictors into each of the three models hierarchically (step 1: SAAT factor score, step 2: we added age and gender variables; and step 3: we added interactions). We excluded nonbinary genders due to the lack of representation of nonbinary participants in the non-autistic group, although we included them in the overall gender divergence (yes/no) categorization. The SAAT will demonstrate convergent validity by correlating with an established measure of autistic traits. We evaluated the relationship between SAAT factor scores and the SRS-2 Total score using the Pearson correlation coefficient (r) statistic in the subsets of the community and GENDAAR autistic (n = 197) and non-autistic (n = 52) participants who completed the SRS.
Finally, we explored whether any association exists between SAAT factor scores and preferred communication modality in the Community Sample 1. We used a multivariate analysis of covariance (MANCOVA) with communication modality as a between-subjects variable, SAAT factor scores as within-subjects variables, and gender identity, assigned gender at birth, and age included as covariates. Where Mauchly’s Test of Sphericity was significant, we interpreted the Greenhouse–Geisser statistic. Post hoc t tests probed significant interactions.
We used Mplus 8.3 for all analyses that pertain to latent variables (e.g., CFA), R for generating graphs, and SPSS for observed variable analysis that includes logistic regression and MANCOVA.48–50 We estimated all latent variable models with maximum likelihood estimation and used Sandwich estimator for information matrix and mean- and variance-adjusted likelihood ratio statistics for goodness of fit assessment, offered by MLMV option in Mplus and recommended by Maydeu-Olivares (2017). 48
Results
We provide results of our data analyses below, organized by our original hypotheses:
The SAAT item-set will exhibit the five predicted underlying factors. Supplementary Figure S3 provides a flow chart of the iterative measurement validation process described below. CFA showed that the hypothesized factor loadings are all significantly different from zero, but the hypothesized five correlated factor model itself did not fit the empirical data well, yielding unsatisfactory model fit indices: comparative fit index (CFI) 0.7, Tucker–Lewis index (TLI) 0.6, and root mean square error of approximation (RMSEA) 0.074. In addition, we detected a high linear dependency among hypothesized factors. Accordingly, we concluded that the hypothesized factor structure was not well supported by the empirical data and decided to examine the underlying factor structure empirically with an exploratory factor analysis (EFA) approach. Between the CFA and EFA, we also tried a semi-EFA approach in which the number of factors was five as hypothesized and a target rotation was used to examine how much expected factor loadings are aligned with the empirical data. Both simple structure and bifactor structures were considered in this process. Since none of these attempts yielded theoretically explainable results in the presence of noise, such as repetitive expressions or direction of words (e.g., negated items), we decided to step back and examine the underlying factors behind the item responses using an EFA with a blind rotation. In conducting the EFA, we removed 9 of the total 58 SAAT items (see Supplementary Table S4) because they represented different constructs (e.g. fine motor skill, pragmatic language, executive function) but demonstrated “local dependence”
b
which did not have face validity according to the content experts. These items appeared to be related due to repeated use of the same phrase.
49
The EFA with respect to the remaining 49 SAAT item responses revealed that a five-factor solution is statistically acceptable to describe the data because the models kept being improved with an additional factor extraction but started exhibiting a trivial factor (i.e., only one or two items load on it) once more than five factors were extracted. The five correlate factor model yielded acceptable model fit indices: RMSEA 0.046 (95% CI: 0.045–0.049), CFI (0.927), TLI (0.909), and SRMR (0.029). While there are arguably other ways to determine the number of factors in EFA, we would like to emphasize that the goal of this EFA is to balance complexity and parsimony in extracting the factors that are theoretically explainable given the set of items by content experts. In addition, the performance of SRMR is known to be sound in this linear normal factor analysis context.
50
The number of eigenvalues larger than 1 and the traditional scree plot also supported the five-factor solution. As we expected the five factors to be correlated and the goal is to identify a simple structure as much as possible to increase the interpretability of each factor, we used an oblique rotation method CF-Quartimax, a member of the Crawford–Ferguson family (Brown, 2001), that is known to be efficient to identify simple structure. The rotated solution and item contents are reported in Table 2. Twenty-four items heavily (≥0.3) load on the first factor, and a substantial number of items also cross-load on multiple factors when we use the typical cutoff of 0.2 or 0.3 for the factor loadings. We also report the full factor loading matrix (rotated solution) in Supplementary Table S9 for reference. Content experts, in this case the SAAT development team (see Ratto et al., 2023 for description), reviewed the EFA results and named each factor based on item content. We placed those items that loaded on more than one factor on the factor that best represented its content for simplicity and interpretability of the latent factor. We named the weakest factor among the five Patternizing; it contained five items with factor loadings above 0.3. However, all cross-loaded on the other factors, and we determined that three of these items were more suitable for the other factors. There were two items that did not belong to other factors based on content. Accordingly, we removed them and reserved them for future examination. We removed two other items that loaded on multiple factors, but without clear content-based connections (There are times I suddenly lose skills that I used to know very well; I say things I don’t mean because I get stuck saying the wrong words). This resulted in a total of four factors and 45 items. We named the factors as follows (see Table 2 for a list of all the items in each factor):
Modulation/Social Communication—23 items concerning the modulation or regulation of attention, sensory information, thinking and actions, or flexibility, including repetitive actions and switching to new thoughts, or social-communication abilities and preferences, or the experience of overwhelm. Strengths/Passions—10 items related to passionate interests, attention to detail, pattern recognition, preference for routine, and other preferences and strengths. Brain–Body Disconnect—eight items, many of which address a disconnect between an intention or desire and the motor movement needed to act on it, such that a person does not act on their desires or acts in conflict with their desires. It also includes items about difficulty with independent demonstration of daily living skills and variability in skills. Negative Community Context—four items that address experiences of being treated unfairly and invalidated. We conducted a unidimensional CFA to examine if each scale is essentially unidimensional and supported by the empirical data. The model fit indices and the standardized factor loadings are reported in Table 3. RMSEA ranged from 0.0 to 0.04, CFI and TLI were between 0.92 and 1.00, and SRMR were between 0.01 and 0.04, indicating acceptable to great model-data fit. To detect potential local dependency among items within each scale, we also examined modification indices. Only one pair of items (Items 3 and 4) for the first factor was flagged with the threshold of 10, and the model fit improvement was also minimal even after allowing the residual correlation. We further examined the nature of the 23 items that load on the first factor by conducting another EFA with respect to only these 23 items. A two-factor solution explained the common variance of 23 items: We named these factors Modulation and Social Communication based on the item content (see final 2 columns of Table 2). However, the correlation between Modulation and Social Communication factors was 0.9, indicating that more than 80% of variance in one subfactor factor can be explained by the other subfactor. Given the high overlap between the two subfactors, we retained the major factor named Modulation/Social Communication as a unidimensional measure in this study. The existence of subfactor opens up the possibility of a bifactor or higher order structure for this factor; however, we decided not to pursue the structure further in the same sample in consideration of interpretability of the scores and instability of the factor structure across samples as noted by Bonifay et al. (2017).
51
The SAAT will demonstrate adequate internal and test–retest reliability of scores. For each factor score, we calculated a reliability coefficient (i.e., proportional reduction in mean squared error) for the autistic and non-autistic groups separately. Modulation/Social Communication factor score reliabilities were 0.93 for both the autistic (n = 500) and non-autistic (n = 80) groups. Reliability estimates for Strengths/Passions were acceptable at 0.83 and 0.73 for the autistic and non-autistic groups, respectively. Brain–Body Disconnect scores also exhibited acceptable reliability across the groups as follows: 0.81 and 0.90 for autistic and non-autistic groups, respectively. The Negative Community Context factor score only included four items, and reliability estimates were adequate as follows: 0.74 and 0.77 for the autistic and non-autistic groups, respectively. Evaluation of test–retest reliability in a subset of the sample (n = 46) revealed Pearson’s correlation coefficients of 0.87, 0.87, 0.92, and 0.81 for Modulation/Social Communication, Strengths/Passions, Brain–Body Disconnect, and Negative Community Context, respectively, indicating that the scores are quite stable. The SAAT will demonstrate concurrent/known group validity by: Distinctive latent distributions of factors between autistic and non-autistic groups We examined preliminary properties of scores, particularly the known group validity of the factor scores by applying multiple group CFA and creating ROC curves. In this analysis, we fixed the latent mean and variance of the non-autistic group at 0 and 1, respectively, for the model identification purpose, and we estimated the autistic group’s latent means and variances with
c
an assumption of full measurement invariance. The two groups’ latent distributions for each factor are depicted in Figure 1. Both Modulation/Social Communication and Brain–Body Disconnect factors showed similar distributions in that the autistic group’s means were higher than two standard deviations (SDs) above the mean of the non-autistic group. If we use factor scores two SDs below the autistic group means as cutoff scores (0.47 and 0.53, respectively), true positive rates are about 98% and the false positive rates were about 30%, indicating strong potential as a screening measure for autism. When a respondent is autistic, cutoff scores of 0.47 (factor scores) on Modulation/Social Communication or 0.53 on Brain-Body Disconnect factors would yield 98% likelihood of correctly identifying this respondent as autistic (sensitivity). On the other hand, when a respondent is non-autistic, there is still 30% chance of identifying this respondent as autistic (1- specificity). To achieve sensitivity of 80%, the cutoffs would be 1.47 and 1.57 for Modulation/SocialCommunication and Brain-Body Disconnect factor scores, raising specificity, as 90% with these cutoffs would be autistic. The known group distributions of the Strengths factor overlapped, indicating that this factor score is not useful for screening. Finally, the Negative Community Context factor score also exhibited high sensitivity and specificity, and it is noteworthy that the latent mean of the autistic group on this score is very high, but the variance is also large compared to other factor scores. This indicates that in the autistic group, the variability in Negative Community Context scores is larger than it is in other factors like Modulation/Social Communication and Brain-Body Disconnect. Distinguishing autistic from non-autistic groups after controlling for age, gender, assigned gender, gender diversity, and their interactions. Logistic regressions predicting diagnostic status (autistic versus non-autistic) with each of the four SAAT factor scores and demographic variables (age, gender identity, assigned gender, gender diversity; due to the lack of non-binary gender identities in our non-autistic group, gender identity analyses were conducted for feminine versus masculine genders only) and their interactions revealed that there were no significant interaction terms between each of the SAAT factor scores and age, gender identity, assigned gender, and gender diversity status. Therefore, following the rule of parsimony, we retained the blocks containing only main effects of age, gender identity, assigned gender, and gender diversity status, and we reported the estimation results in Supplementary Tables S5, S6 and S7. The lack of significant interaction effects indicates that the association of SAAT scores to autism diagnosis status is consistent across age, gender identity, assigned gender, and gender diversity status. The SAAT will demonstrate convergent validity. To examine the assumptions of Pearson’s correlations, we assessed the distributions of SAAT and SRS-2 Total Score data for normality. Skewness and Kurtosis values were < |1| for all variables in the each of the autistic groups, but not for the non-autistic group, as expected. Overall, there were moderate to large correlations (r’s between 0.45 and 0.54) between SAAT Modulation/Social Communication, Brain–Body Disconnect, and Negative Community Context factors and SRS-2 total scores, but SAAT Strengths/Passions factor scores and SRS-2 were not significantly correlated. See Scatterplots in Supplementary Figure S2. Exploratory: Do SAAT factor scores differ based on communication modality? Responses from 299 of the online participants indicated that one-third of the respondents prefer using AAC to communicate and an additional 16.7% prefer to use a combination of speaking and AAC. Factor scores were equivalent across the three communication modality groups for Brain–Body Disconnect, but were significantly different for Modulation/Social Communication, Strengths/Passions, and Negative Community Context, both with and without covarying effects of age, gender identity, and assigned gender at birth (see Supplementary Table S8). Effect sizes were small to medium. Post hoc comparisons revealed the following significant differences. Mostly speaking participants had higher scores, indicating more autistic traits, on Modulation/Social Communication than those who mostly use AAC (p < 0.001), and those who speak and use AAC equally had higher Modulation/Social Communication scores than those who mostly use AAC (p = 0.01). All groups were significantly different from each other on Strengths/Passions (p < 0.05), with mostly AAC users having the lowest scores and mostly speaking participants having the highest scores. Finally, those who speak and use AAC equally had higher scores on Negative Community Context than those who mostly use AAC (p < 0.05).
The correlations among these four factors (see Table 2) reveal that Modulation/Social Communication is correlated with Brain–Body Disconnect and Negative Community Context at the moderate level. Brain–Body Disconnect and Negative Community Context are also correlated with each other. In contrast, Strengths/Passions is weakly or not at all associated with the other factors.
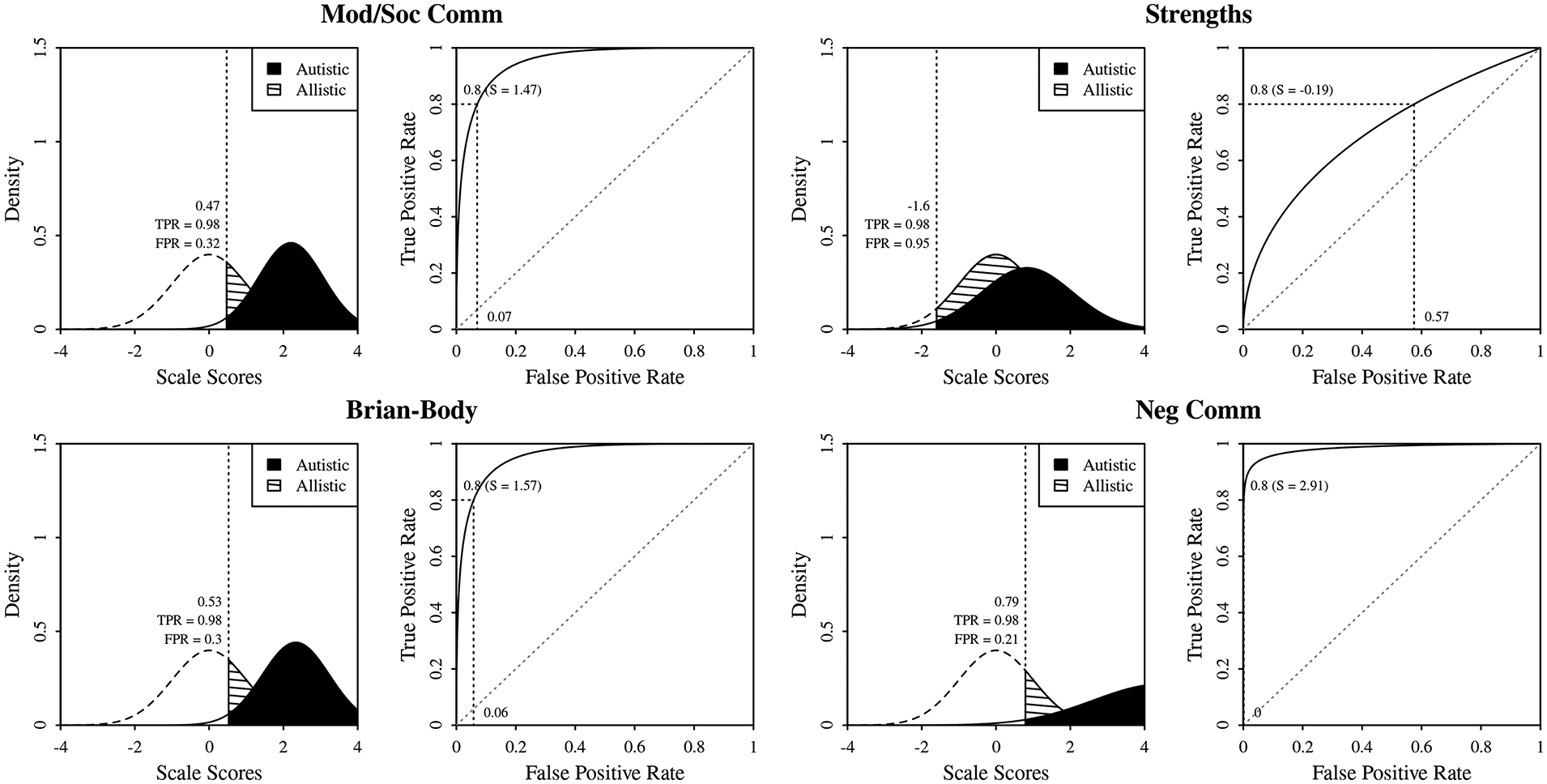
Model-based latent distribution of factors for autistic and non-autistic groups and receiver operating characteristic curves. The left graph of each factor displays the conditional distribution of autistic group (solid fill) and the non-autistic group (dashed line fill) and the true positive rate (TPR) and false positive rate (FPR) for the cutoff score that is +2 SD from the expected mean of the non-autistic group. The right graph displays the receiver operating characteristics curves along with the possible cutoff score that would yield 0.8 true positive rate. The false-positive rate for the score is also presented. SD, standard deviation.
Exploratory Linear Normal Factor Analysis Results
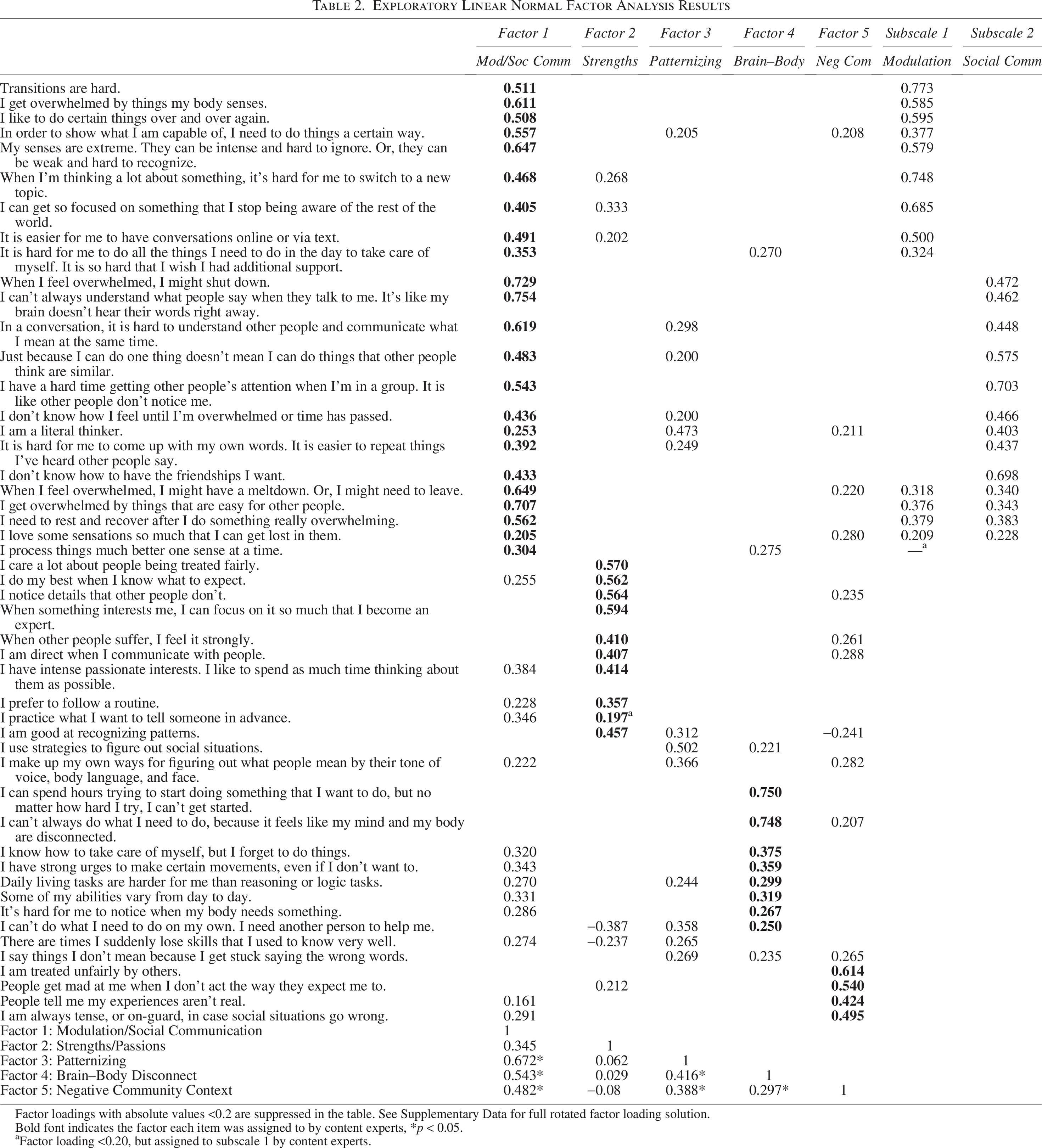
Factor loadings with absolute values <0.2 are suppressed in the table. See Supplementary Data for full rotated factor loading solution.
Bold font indicates the factor each item was assigned to by content experts, *p < 0.05.
Factor loading <0.20, but assigned to subscale 1 by content experts.
Unidimensional Confirmatory Factor Analysis Results for Four Self-Assessment of Autistic Trait Factors
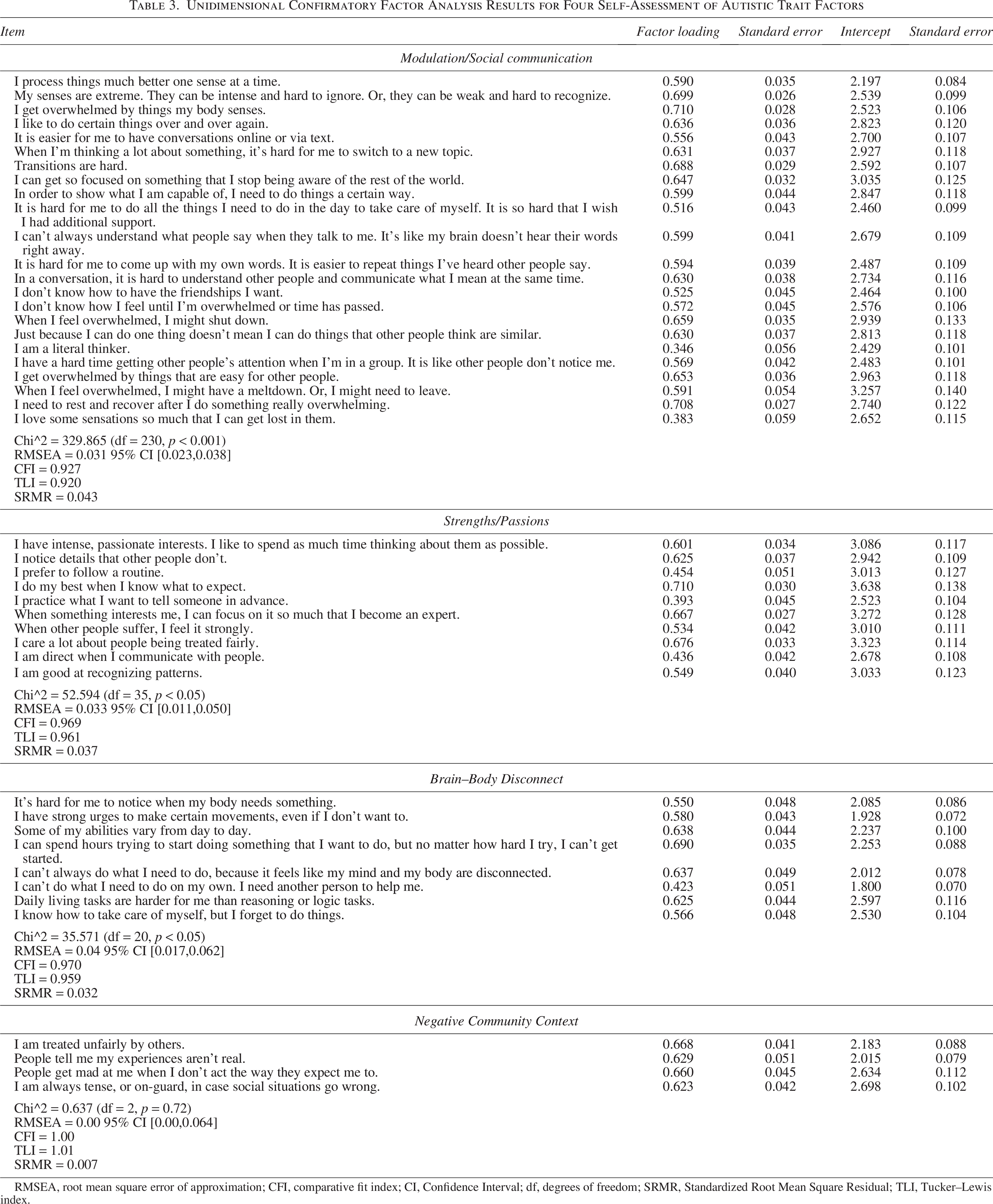
RMSEA, root mean square error of approximation; CFI, comparative fit index; CI, Confidence Interval; df, degrees of freedom; SRMR, Standardized Root Mean Square Residual; TLI, Tucker–Lewis index.
Discussion
The SAAT is the first comprehensive self-report tool of autism traits for teens and adults cowritten with autistic people. As such, it has the potential to address gaps in current screening and phenotyping assessment tools, including the need for an accessible measure that captures the lived internal experience of autism, as well as external observations of the person. The SAAT shows promise as a multidimensional self-report tool, which is reliable and valid with respect to the samples (500 autistic and 80 non-autistic individuals) that we examined. The factor structure of the SAAT items did not confirm the domains of the SAAT as hypothesized by the development team. However, EFA followed by a unidimensional confirmatory factor analysis revealed four strong factors as follows: Modulation/Social Communication, Strengths/Passions, Brain–Body Disconnect, and Negative Community Context. Three of these factors appeared to be distinctively distributed between autistic and non-autistic individuals, implicating that the factor score is sensitive to autism in comparison with non-autistic individuals across age, gender identity, assigned gender, and gender diversity status. This finding indicates that some items in the SAAT item-set may yield a useful screening tool for people 16 years or older, who are questioning whether they are autistic, regardless of their age, gender identity, or assigned gender. Other items from the SAAT item-set may not be useful in a screening measure, but may contribute to a phenotyping tool that captures important components of the autistic experience. Preliminary evidence of adequate internal and test–retest reliability increases our confidence in the potential utility of the SAAT item-set. With items that autistic people wrote, the SAAT has the potential to be a more accessible and acceptable tool for autistic self-report.
The first confirmatory factor analysis did not provide adequate empirical support for our hypothesized five factor structure (Sensory/Motor experiences, Strengths in Specificity related to identification of patterns, details, and the development of expertise, Social Communication, Executive Functioning and Related Traits, including flexibility, overload, burnout, and demonstration of daily living skills, and Negative Community Context). In addition, nine of the total 58 SAAT items demonstrated “local dependence,” which did not have face validity according to the content experts because they represented different constructs. We removed these items and investigated the factor structure empirically using EFA, which resulted in a four-factor solution. These factors appear to be reliable and stable with many similarities to the hypothesized five-factor structure, including the Negative Community Context factor, a factor focused on Strengths, and Social Communication as a subfactor, strong associated with sensory and cognitive modulation items. The executive functioning and related traits split between the Modulation subfactor and a new factor related to disconnections between brain and body. The SAAT development team reviewed the new factor structure in detail and determined that it was consistent with many aspects of the hypothesized factor structure and represented factors that capture the lived experience of autism.
The SAAT Modulation/Social Communication factor includes items addressing well-documented traits for autistic people related to social communication and flexibility. Two other factors, namely, Brain–Body Disconnect and Negative Community Context, measure aspects of the autistic experience which other comprehensive tools do not capture. All three of these factors show good sensitivity to autism in comparison with non-autistic individuals. They also showed moderate-to-large correlations with the SRS-2 Total Score. The fourth factor, Strengths/Passions, which contains items related to passionate interests, attention to detail, pattern recognition, and preference for routines, is not specific to autism in our sample. Each of these factor scores can produce information that helps guide the creation of opportunities and supports that enable autistic people to thrive. Profiles of SAAT factor scores might inform priorities for support; for example, someone high on the Negative Community Context factor might need assessment for trauma and support for navigating experiences of discrimination and stigma. Information from the Strengths/Passions factor might guide the selection of vocations, roles, and activities that optimize an autistic person’s ability to thrive.
Given its development by autistic people reporting on their personal experience of autism, it is not surprising that the SAAT includes constructs identified in recent qualitative research on the experience of being autistic, but not included in comprehensive autism trait assessment tools constructed without autistic cocreation. The Brain–Body Disconnect factor includes items that reflect the phenomenon of autistic inertia52–54 and connect to recent research on autistic burnout. 55 Overwhelm and related meltdown or shutdown items in the Modulation/Social Communication factor also align with recent qualitative studies. 52 Another outcome of the SAAT’s autistic authorship is that even when it addresses commonly described and measured traits such as social communication or sensory challenges, it does so from an autistic person’s perspective. As a result, SAAT items frequently address a positive aspect of the experience (e.g., “I love some sensations so much I get lost in them”) or a possible compensatory strategy (e.g., “I process things much better one sense at a time”). Unlike any other measure of which we are aware, the SAAT contains items in the Negative Community Context factor that allow the respondent to identify the problematic actions of others (e.g., “People tell me my experiences aren’t real”).
The inclusion of a community-based autistic sample, in addition to those participating in an academic medical center-based investigation, broadened the age range (16–76 years) and expanded the representation of assigned gender at birth females (62% of the autistic sample) and GD individuals (15% of the autistic sample). The absence of significant interaction terms between any of the SAAT factor scores and age, gender identity, assigned gender, or gender diversity status in logistic regressions predicting diagnostic category provides preliminary evidence that three of the SAAT factor scores are sensitive to autism regardless of age or gender. Although there were participants with a broad range of ethno-racial identities in this study, missing data and small sample sizes for many ethno-racial identities prohibited statistical exploration of the impact of ethno-racial identity on SAAT scores, a major limitation of this investigation.
Because many autistic adults use AAC devices to communicate,56,57 at least some of the time,58,59 we asked community autistic participants in this study to indicate their communication modality preferences. Notably, almost 52% of the respondents reported that they prefer to communicate with AAC or a combination of AAC and speaking, a key finding which elevates the importance of increasing accessibility for AAC users in research and clinical settings. It also motivates further investigation of this communication modality and its possible relationship to previous findings of diminished reliance on inner speech in autism. 60 In this investigation, the AAC user group had significantly lower Modulation/Social Communication and Strengths/Passions factor scores than the predominantly speaking group. This raises the possibility that in these factors, the SAAT items may be somewhat less representative of the autistic experience for AAC users than those who prefer speaking. Alternatively, the items may not be written in a way that is inclusive of the social-communication experience of AAC users. For example, AAC users receive fewer opportunities for autonomous communications when in conversation with speaking individuals 61 and the pace of their communication is slower. More robust inclusion of nonspeaking autistic people for any future revisions of the SAAT item-set will be essential to address this concern. In addition, it is important to note that we did not ask participants about their communication history, only their current communication modality. As a result, it is not clear whether some of the participants did not speak throughout their lives or only in adulthood, which may be an important distinction regarding autism-related traits.
The SAAT item-set holds promise as a source of items to create two self-report questionnaires as follows: a screening tool and a phenotyping measure. Unlike current self-report questionnaires, the SAAT is shaped by autistic people’s concepts of what is central to their experience of autism, as well as their perceptions about accessible and acceptable language and descriptors. The use of specific examples, avoidance of figurative language, description of internal experiences, and framing of traits through their strategic or pleasure-related utility distinguish the SAAT from other measures of autism traits. Anecdotal evidence indicates the power of this approach, including this comment from multiple individuals taking the SAAT: “Finally, I feel seen.” The assessment process is more effective when the person being evaluated understands the evaluator’s questions, 62 feels respected during the evaluation, 63 and when the questions reflect their internal experience, as well as how they appear to others. For these reasons, we believe that the SAAT item-set will yield measures that increase access to a diagnostic evaluation and increase the quality of self-report data on autism traits in research and clinical settings.
Next steps regarding SAAT development include revision and augmentation of SAAT items. This includes revision of items which we removed from analyses reported here because they showed strong local dependence, probably due to a repetitive phrase (“…is easy…”) across items. We will also augment the Negative Community Context Factor, which currently contains only four items, and review all items for their relevance to nonspeaking individuals. We will then collect SAAT data from a large demographically representative group of autistic and non-autistic people, as well as from people with other psychiatric diagnoses, to allow for cross-validation of the findings and investigation of specificity in the context of individuals with other psychiatric conditions. We will intentionally recruit people of color and limit White, non-Latine participants to 50% in future studies of the SAAT to ensure adequate sample sizes to investigate the impact of race and ethnic identity on SAAT scores. Stronger representation of the global majority race and ethnicity is an essential next step, followed by collection and analysis of SAAT data in populations and cultures outside of the United States. We also acknowledge that the cross-validation study with the final set of items should include further refinement of the measurement model (e.g., addressing construct-irrelevant covariance, functional form of the relations between observed variables and latent variables, or non-normal latent distribution) and assessment of measurement invariance (e.g., examination of differential item functioning across gender identity, assigned gender at birth, age, and race/ethnicity, and autistic vs. non-autistic groups) based on the final model. We emphasize that this step is crucial and necessary to develop the SAAT as an equitable, reliable, valid, and accessible autistic screening and phenotyping tool.
Footnotes
Acknowledgments
The authors thank the participants in this study and the members of the ACE network consortium who collected the data analyzed in this study.
Funding Information
This work was funded by the NIH Autism Center of Excellence Network: Multimodal Developmental Neurogenetics of Females with ASD 2R01MH100028-06.
Authorship Confirmation Statement
L.K.: Conceptualization, methodology, validation, investigation, resources, writing—original draft, writing—review and editing, supervision, and funding acquisition. S.dV.: Conceptualization, methodology, and writing—review and editing. J.B.: Conceptualization, methodology, and writing—review and editing. A.R.: Conceptualization, methodology, and writing—review and editing. L.G.A.: Conceptualization, methodology, and writing—review and editing. A.K.: Writing—review and editing, data curation, formal analysis, visualization, and project administration. E.C.: Writing—review and editing, formal analysis, data curation, visualization, and project administration. J.F.S.: Conceptualization, methodology, and writing—review and editing. A.V.: Methodology and writing—review and editing. C.E.P.: Writing—review and editing. J.S.: Writing—review and editing and formal analysis. K.A.P.: Writing—review and editing and funding acquisition. J.S.Y.: Methodology, software, formal analysis, writing—original draft, visualization, and writing—review and editing.
Author Disclose Statement
There are no conflicts of interest for any of the authors.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.