
Abstract
Background:
The 988 Suicide & Crisis Lifeline (“988”) in the United States provides people experiencing suicidal ideation or distress with free access to trained counselors via text messaging, phone calls, or online chats. The present qualitative study investigated the following research questions: (1) What opinions are held by U.S.-based autistic adolescents and young adults ages 13–22 years old about 988; and (2) What have autistic adolescents and young adults experienced when they contacted 988 for help?
Methods:
Self-report online survey data were collected from English-speaking individuals ages 13–22 years old in the United States between June 2022 and October 2023 as part of a larger, parent study called Project Lift Up. Of the 295 participants who reported that they were autistic, 188 (64%) submitted a write-in response to a question about why they would or would not use 988. We used a content analysis approach to identify themes related to why they would or would not want to use 988.
Results:
Autistic individuals reported mixed opinions about the U.S. 988 Suicide & Crisis Lifeline. While some liked the idea of talking to a stranger or trained counselor when in crisis, others expressed anxiety about the idea that emergency services could be dispatched and questioned the preparedness of counselors to support their complex and unique needs as autistic people. Among those with direct experience with 988, some reported problems included long wait times, feeling like the counselor was using a script or interacting in a robotic way instead of authentically, and that the counselor was not able to communicate with the autistic user in a manner that felt supportive to them.
Conclusions:
Upgrades to 988 that will result in better crisis support for autistic people are needed, feasible, and should be evaluated.
Community Brief
Why is this an important issue?
The U.S. 988 Suicide & Crisis Lifeline (also called “988”) is supposed to help people who are feeling suicidal or very upset. We do not know if autistic people are likely to call, text, or chat 988. Some autistic people may have heard things about 988 that stop them from using it. Meanwhile, there are autistic people who have used 988. We want to know what those autistic individuals experienced when they contacted 988.
What was the purpose of this study?
This study was designed to find out the opinions of U.S.-based autistic adolescents and young adults about 988. It was also designed to find out about what autistic adolescents and young adults have experienced when they contacted 988.
What did the researchers do?
The researchers advertised a survey to the youth in the United States who were 13–22 years old as part of a research project about suicide called Project Lift Up. The researchers included questions about 988 on the survey, and they included a question about autism status. This research study focused only on the people who said they were autistic and that they had heard of 988. The researchers looked at what the individuals (N = 188) wrote when they were asked if they would use 988 or not. The researchers used qualitative data analysis methods to code the written-in answers, study the patterns, and group the patterns into themes.
What were the results and conclusions of the study?
The autistic people in this study had some positive expectations about 988, and among those with direct experience using 988, some had found it helpful. For example, some autistic people said it helped them when they wanted to hurt themselves, and some autistic people who had never used 988 said they thought it would be a good resource in case they were feeling distressed. However, many more autistic people felt unlikely to use 988, either based on things that they had heard or thought might be true about 988 or based on direct experience that they had with 988. Autistic people who had not used 988 wrote that they were scared that emergency services would be dispatched if they used 988. They also wrote that they were concerned that 988 would not know how to meet their specific needs, and some wrote that they would not use 988 because they dislike making phone calls (and they did not realize that 988 also has text and chat options). Among the autistic people who had used 988, reasons that they might not use it again included the long wait times and feeling like the counselors were unable to say or do things that helped them.
What is new or controversial about these findings?
988 offers an important service that many people find very helpful. However, it may still need to be improved to meet the needs of some autistic people.
What are potential weaknesses in the study?
People could self-select to participate in the research survey, and the people who chose to fill out the survey might represent a special subset of all autistic people rather than a representative subset. It is also possible that some autistic people who reported that they had used 988 were remembering a different hotline, so their criticisms might not be specific to 988.
How will these findings help autistic adults now or in the future?
These findings will help autistic adults advocate for improved crisis line services in the United States and elsewhere to benefit autistic people in crisis. The findings also help explain why some autistic people may not have their needs met by 988 and document that some autistic people think favorably about the possibility of using 988.
Introduction
The U.S. Interagency Autism Coordinating Committee has stated that it is a priority to support the development of interventions that address depression and suicide among autistic people. 1 It has been established that autistic youth and adults are more likely to die by suicide than their non-autistic counterparts. For example, population-based studies find that autistic adults are 9-fold to 14-fold more likely to die by suicide.2,3 In general, the rates of suicidal thoughts and behaviors in U.S. youth are higher than they have been in the past. In 2023, 20% of high school students reported having seriously considered suicide in the past year, and 10% of high school students reported that they attempted suicide. 4 A recent review of 29 studies, including 34,011 autistic youth less than 26 years old, found a pooled prevalence of 25.2% for suicidal ideation and 8.3% for suicide attempts. 5 Although these rates do not exceed those found for non-autistic youth, it is a problem for autistic youth that might demand a solution different than those for non-autistic youth.
Toll-free telephone or text messaging-based crisis lines—also known as “hotlines” or helplines—have been considered an important strategy for suicide prevention for at least 40 years. 6 The theoretical rationale for hotline services is that suicidal behavior arises out of crisis, and because suicidal people are often ambivalent about acting on suicidal ideas and may wish to be rescued, hotline services may help by providing immediate, easily-accessible support to those in a crisis and feeling ambivalent. 7 Moreover, although long-term follow-up studies evaluating effects are rare, recent research has found that crisis hotlines and text lines appear to reduce suicidal thoughts and behaviors, result in the use of mental health services post-lifeline contact, and are perceived as helpful by callers and texters.8–11 Despite this encouraging evidence, to our knowledge, there are no published studies that have evaluated the impact of crisis lifeline services for autistic individuals, specifically.
There is a notable lack of suicide prevention services specifically tailored for autistic people. Most existing services and programs were developed for the general population, and autistic individuals often report that mental health supports designed for the general population are inaccessible to them or inappropriate.12,13 This is part of the reason the current International Society for Autism Research Autism Community Priorities for Suicide Prevention Policy Brief lists “Identify how interventions could be adapted for autistic people and individual presentations” as one of its 10 priorities. 14 Given the paucity of autism-specific suicide intervention strategies, some clinicians and researchers have made efforts to adapt existing approaches for autistic people. For example, Autism Adapted Safety Plans that were coproduced with autistic people are presently being pilot-tested in England, Scotland, and Wales. 15 In addition, a new multicenter randomized controlled trial testing the effect of dialectical behavior therapy for autistic patients with suicidality or self-destructive behavior is now underway in the Netherlands. 16 However, to our knowledge, there have not been any studies of autistic experiences with suicide hotlines and crisis support services.
Autistic people who are in a state of crisis may present in ways that surprise crisis counselors who have not been trained about autism or are not familiar with autistic people. 17 Specifically, and as relayed in the “Crisis Supports for the Autism Community” tool kit authored by the autistic suicide prevention expert Lisa Morgan and available on the 988 website, autistic people may laugh when feeling distressed, be very sensitive to sensory input, have difficulty identifying emotions (e.g., would have trouble answering the question “how are you feeling tonight?”), have difficulty regulating intense emotions, be literal when responding to questions or counselor statements, feel weary about miscommunication, take more time to process and respond to questions, use echolalia, perseverate, and use an uncommon vocabulary, or speak in a “robotic”-sounding way. 17 As a result, crisis lifelines that rely on counselors without specific training on how to serve and support autistic people may be suboptimal for this population.
As a first step toward understanding whether and how crisis lifelines may benefit autistic people, the present qualitative study investigated the following research questions: (1) What opinions are held by U.S.-based autistic adolescents and young adults ages 13–22 years old about the 988 Suicide & Crisis Lifeline; and (2) What have autistic adolescents and young adults experienced when they contacted the 988 Suicide & Crisis Lifeline for help?
Brief history and overview of the 988 Suicide & Crisis Lifeline
On July 16, 2022, the 988 Suicide & Crisis Lifeline (referred to as 988 herein) went live in the United States. 988 is national in the sense that, since 2022, every U.S. state provides 988 services and receives federal financial support to operate local call centers. However, 988 is state-based in that each state proposes its own plan for handling 988 calls, onboarding and supporting counselors, and deploying mobile crisis units in emergencies. Within each state, there are typically multiple human services agencies that serve as call centers for that state, so there are more than 200 local call centers that receive contacts through 988.
Before the three-digit 988 number becoming universally available throughout the United States, there had been a toll-free (i.e., 1–800) national suicide prevention hotline in operation since 2005, with a Spanish language subnetwork available since 2006, a veterans crisis line established in 2007, a chat service instituted in 2013, a disaster distress option introduced in 2015, and a texting option added in 2020. 18 The transition from the toll-free number to the three-digit 988 represented three important improvements. First, the new three-digit number was expected to be easier to remember and, therefore, more useful than the 10-digit number. Second, the federal funding for 988 increased 18-fold from $24 million to $432 million in 2023 to increase crisis counselor staffing, strengthen the infrastructure, and permit crisis follow-up with suicidal people by call centers. 19 Third, 988 uses georouting to identify cell phone caller’s approximate physical location and route their call to a local crisis center. The advantage of georouting is that the crisis center can make a referral to a local behavior health resource, and in rare cases of imminent risk, emergency dispatches can be made more effectively. Importantly, to protect caller privacy, 988 does not engage in geolocation, which would pinpoint callers’ precise location, 20 although 988 can transfer contacts to 911, which does have that capacity.
After 988 became operational, it answered nearly 5 million contacts in its first year. In 2023, 988 added a subnetwork (an option choice at the beginning of each call) for LGBTQI+ youth and young adults. Aggregating across the general 988 Lifeline, Spanish subnetwork, and LGBTQI+ subnetwork (and noting that Veteran call data are unavailable), in 2024, 988 has responded to approximately 7.7 million contacts, 67% calls, 18% texts, and 15% online chats. 21
Methods
The research was approved by the University of New Hampshire Institutional Review Board.
Participants
Self-report online survey data were collected from N = 4981 English-speaking youth ages 13–22 years old in the United States between June 2022 and October 2023 as part of an ongoing longitudinal study of bystander behavior in cases of self-directed violence (Project Lift Up). 22 Participants were recruited through social media, including Instagram and Facebook advertisements. The Project Lift Up study recruitment advertisements used colorful graphics depicting sports, video games, and anime and said: “Tell us about your life and experiences in this research survey,” “have your voice heard,” “make a difference,” “your voice matters,” and “we want to hear from you.” Interested individuals clicked on a link that directed them to a secure website with the study description and eligibility screening questions. Eligibility criteria included being 13–22 years old, living in the United States, and speaking English. Quotas were set for gender, age, and race/ethnicity to ensure a sufficiently diverse sample that reflected the U.S. population characteristics and ensured an oversample of gender and sexual minority youth. Of these participants, 2970 completed a follow-up survey 6 months after they completed the baseline survey. The present analysis includes data only from the follow-up survey, because only the follow-up survey included questions about opinions about 988.
Procedures
Before being directed to the main baseline survey, eligible youth were asked to review an assent or consent form and indicate willingness to participate. A waiver for parental consent was granted to protect youth privacy because the survey was on sensitive topics. A waiver was also necessary to avoid sampling bias that would occur by only including those who were willing to disclose sensitive information to parents. 23 Participants were emailed a $15 e-gift card after completing the survey. Data quality protocols were used to identify fraudulent data, including age verification, reverse lookup of IP addresses and phone numbers, review of names, addresses, social media accounts, time to survey completion, attention check questions, and direct participant outreach, as needed.
Data collection
Participants were asked to respond to the questions: “Have you ever heard about the 988 Suicide & Crisis Hotline,” and, if yes, “How likely would you be to use this if you needed it?” These two questions were followed by a third, open-ended question, which was: “Why or why not?” Participants then wrote in why they would or would not want to use 988 in a text field that permitted responses of any length. Responses ranged from one or two words to three sentences in length. Participant responses to the open-ended question were analyzed for this study. First, one team member read through all 188 responses and flagged those that revealed the participant had direct previous experience calling 988. For example, if a participant wrote: “I have used it before,” “the last time I called,” or “I tried it once,” this was considered an indication that they had used 988. The responses from the 29 autistic participants who indicated direct experience with 988 were analyzed separately from the 159 autistic participants who had opinions about 988, but did not relay that they had used it themselves.
Researcher positionality
We are a team of seven cisgender, White women who are non-autistic and one who is autistic. Six members of our team identify as middle class, one is extremely low income and uses public assistance, seven have graduated from college, and all acknowledge being exposed to the suicidal thoughts and/or behaviors of those we have personally known. The three authors who coded data reflected on our positionality and noted that our commitment to equity for autistic people was paramount and that we were therefore attuned to participant comments that relayed their fear of institutionalization, in particular. Other members of the research team acknowledged their own commitment to helping ensure that suicide prevention services exist for all in the United States, and this influenced their interest in adding statements to the Discussion that contextualized negative opinions about 988.
Data analysis
We used an inductive, content analysis approach. Following a standard approach to content analysis, 24 the steps of our data analytic process were as follows: (1) Read the data for a sense of the whole; (2) Generate an initial code list by identifying recurring patterns or terms in the data (i.e., derive codes from the data); (3) Assign codes to chunks of text; (4) Organize codes into meaningful groups to highlight patterns; and (5) Interpret the themes to answer the research question of interest. Accordingly, an initial code list was generated by E.F.R. based on an initial read through of all data. The initial code list was shared with L.G.H. and M.M. who also read all data to “get a sense of the whole” and suggested minor modifications to the code list. After the final code list and definitions of each code were agreed upon by E.F.R., L.G.H., and M.M., L.G.H. and M.M. coded all data independently (see Supplementary Table S1 for all codes). L.G.H. and M.M. then met to compare coding choices, discuss discrepancies, and arrive at a consensus coding choice where there were discrepancies. We made an intentional choice not to calculate inter-rater reliability, given recent discourse among qualitative research methodologists proposing that such a calculation is “an unwarranted attempt to import standards derived for positivist research” on to what is inherently a subjective process. 25 To validate the legitimacy of our analysis, we opt instead for transparent reporting of our analytic procedures, the presentation of “thick description” with multiple quotations from our raw data, and checking our interpretation with autistic people (i.e., M.M. and one 16-year-old autistic person). 25 After all data were consensus coded, L.G.H. and M.M. identified themes that emerged and selected illustrative quotations for each theme. E.F.R. then reviewed the themes and proposed grouping the themes into two primary themes (i.e., positive vs. negative comments about 988), and proposed four subthemes for each, which L.G.H. and M.M. then reviewed and endorsed. Using iterative rounds of discussion and interpretation, we used a reflexive approach and considered our own positionality as it influenced our interpretation of quotations, codes, and choices about themes.
Results
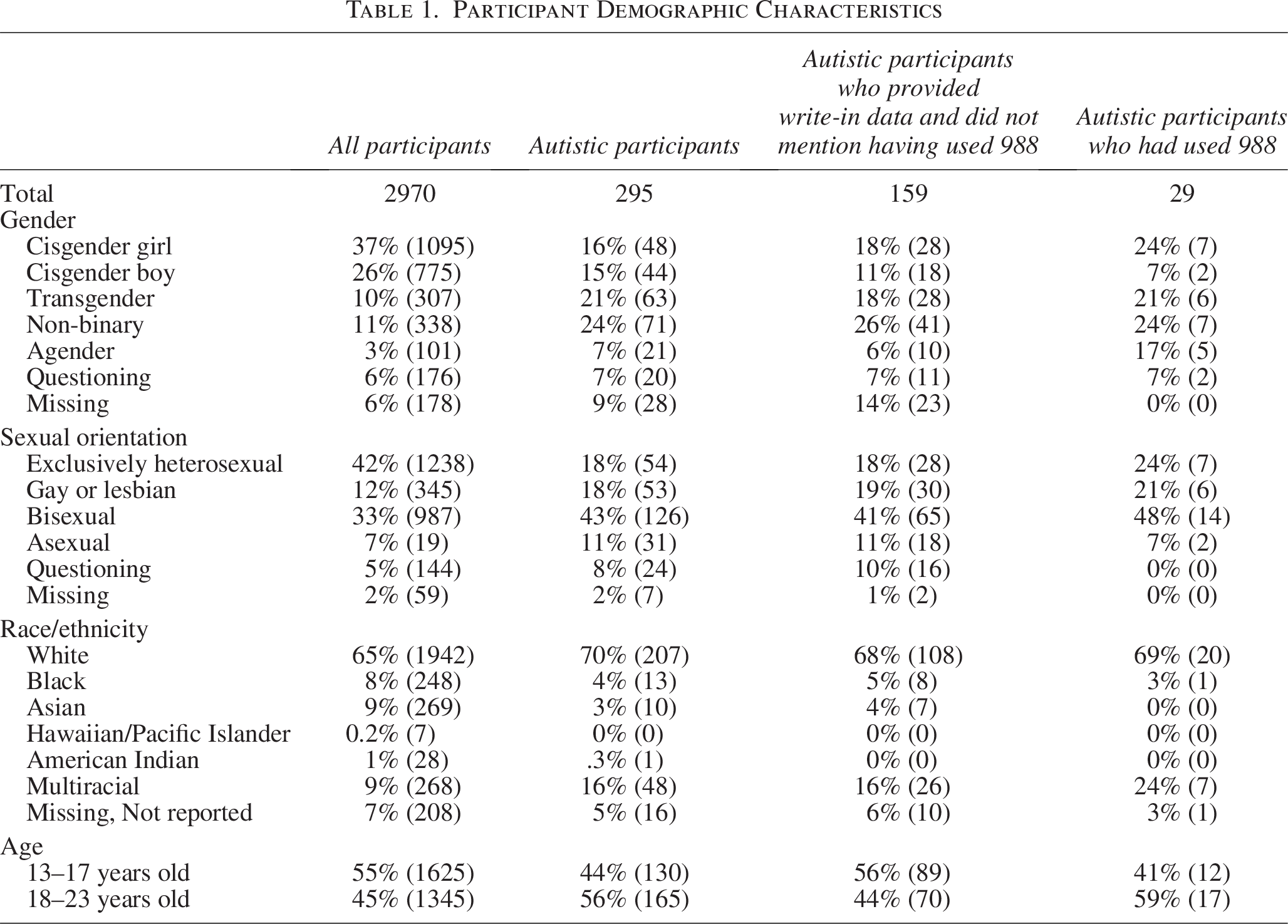
Of the 2970 participants who completed the follow-up survey, 295 responded positively to the question: “Have you ever been diagnosed by a doctor, therapist, or other professional with autism, pervasive developmental disorder (PDD), or Asperger’s?” (9.9%), and were classified as autistic. Of the 295 autistic participants, 87% had heard of 988, 23% of them reported being very likely or extremely likely to use 988, and 188 (64%) submitted a write-in response to a question about why they would or would not use 988. Of the 188, 29 wrote in responses that indicated that they had direct experience contacting 988 previously and 159 had opinions about 988, although they did not reveal that they had used it directly themselves. Thus, our analytic sample was N = 295 autistic youth. Participant demographics are available in Table 1.
Participant Demographic Characteristics
We identified two primary themes as follows: (1) Positive expectations about 988 and (2) Negative feelings or concerns about 988. Within the “positive” theme, we identified two subthemes, and within the “negative” theme, we identified five subthemes. Subthemes related to positive expectations about 988 included: (1a) Among those who did not relay that they had direct experience with 988, positive expectations of helpful, confidential services from nonjudgmental strangers; and (1b) Among those who reported direct experience with 988, positive experiences that would encourage them to use 988 again. Subthemes related to the negative feelings or concerns included three from those who did not relay that they had direct experience with 988, including: (2a) concern about emergency intervention, (2b) concern about counselors being underprepared to serve their specific needs, and (2c) a fear of using the phone. Negative subthemes from those with direct experience included: (2d) experience with wait times and (2e) negative experiences with counselor engagement.
Theme 1a: Among those who did not relay that they had direct experience with 988, positive expectations of helpful, confidential services from nonjudgmental strangers
Some research participants who did not mention that they had used 988, but were aware of it, had positive expectations about what it would be like to use it. For example, one 19-year-old, cisgender woman shared this positive expectation: “It’s because sometimes you need to share stuff with someone who won’t judge you for it or anything like that.” Similarly, a 13-year-old cis-girl wrote: “Because sometimes all you need is a person to talk you down.” Other youth reported that they felt positively inclined to use 988 because they trusted the privacy protocols and because they had faith in the professionalism of the counselors. For example, one 19-year-old, nonbinary participant wrote: “I feel safe and it’s confidential,” and a 21-year-old cis-woman wrote: “Sometimes when you’re in a bad place you need to speak with a trained professional and the crisis hotline is there for those times.” Similarly, one 15-year-old, cis-girl wrote: “Because they are a helpful resort and could convince you not to do a very bad thing,” and a 21-year-old, non-binary participant who had not used 988, but nevertheless had positive impressions of it as a potential resource, wrote: “It is a good resource.” A 16-year-old trans girl wrote: “It’s anonymous and consistent.”
Theme 1b: Among those who reported direct experience with 988, positive experiences of receiving help that would encourage them to use 988 again
Some participants with direct, firsthand experience with 988 reported that they would be inclined to use 988 again because it helped them. For example, a 19-year-old non-binary participant wrote: “I’ve used it before and it helped me take steps to stop myself from hurting myself.” Similarly, one 21-year-old non-binary participant who had firsthand experience using 988 wrote: “They helped me when I was in crisis and did not make me feel judged at all,” and a 19-year-old cis-woman wrote: “I have used it before and they were able to help me.”
Other youth had more mild positive feelings about 988 after having used it. For example, one 20-year-old non-binary participant wrote: “It has been helpful and harmful in the past for me so depends on the person and available forms of communication (call, text, email, etc.).” Other participants with direct experience with 988 felt that it might be a viable last resort if they needed help. For example, an 18-year-old non-binary youth wrote: “I have used it before, and it can be nerve-wracking, but I also think it is a good last resort.” A 22-year-old transgender woman wrote: “I’ve used it before. It’s better than nothing I guess.”
Theme 2a: Among those who did not relay direct experience with 988, concerns about police or involuntary hospitalization
Twenty-one youth who were aware of 988 but did not mention direct experience using it expressed feeling fearful about using 988 because they were worried about immediate physical intervention, the involvement of law enforcement or emergency services, and being institutionalized as a result. Comments typical of this subtheme included, for example: an 18-year-old non-binary person who wrote: “988 is authorized to send police to your location if they sense urgency, I don’t trust law enforcement officers to be able to understand or reason with neurodivergent or mentally ill people,” a 21-year-old, non-binary individual who wrote “I’m hesitant to call 988 because they sometimes involve law enforcement (police) in mental health crises,” a 17-year-old gender-questioning participant who wrote: “I don’t feel safe with the idea of police potentially being dispatched,” and a 16-year-old non-binary youth who wrote: “I’d be afraid of being put in a psych ward.” One 17-year-old non-binary person wrote: “If I was considering suicide then calling would be a one-way ticket to an institution.”
There were multiple comments about fearing the police, specifically. For example, one 17-year-old non-binary youth wrote: “I dislike the police…cops have a history of mistreating those who are queer, disabled, and mentally ill. it’ll likely be more traumatizing than helpful.” Similarly, a 19-year-old participant wrote: “I heard they automatically call police and escalate the situation.” One 17-year-old cis-girl wrote: “I’ve seen a lot of stuff online, mostly on Twitter, that these services can be a hit or miss. Stuff like: the operator doesn’t help, hangs up on them, or calls the police…The police would make the situation worse in my opinion since I have an (irrational) fear of them.”
Theme 2b: Among those who did not relay direct experience with 988, concern about counselors being underprepared to serve their specific needs
Many participants who did not relay that they had direct experience with 988 expressed concerns that the counselors would be underprepared to meet their specific developmental or mental health needs, or that 988 wasn’t geared for them. For example, a 21-year-old non-binary participant wrote: “I don’t think the hotline would be educated enough on my physical and psychiatric conditions to provide me with any proper help. I worry that calling would only make me feel worse.” A 15-year-old non-binary person reported that they sometimes feel unable to speak and that this might be an impediment to using 988. They wrote: “When I am suicidal, I do not feel that I am worthy of getting help, or that others need it more than me. I also am often not able to speak when I have strong emotions.” One 20-year-old transgender participant who had not used 988 wrote: “As a sufferer of Post-Traumatic Stress Disorder (PTSD) and Dissociative Identity Disorder (DID), my issues are more deeply rooted than hotlines are able to effectively help with.” A 16-year-old trans boy wrote: “I fear they wouldn’t understand my transness or dysphoria. Or that they will send people to my house.”
Theme 2c: Among those who did not relay direct experience with 988, a fear of using the phone
One subtheme that came up frequently among those who did not indicate that they had used 988 was that autistic participants expected they would have to talk on the phone (rather than text or chat), which caused them to feel anxious and disinclined to use the service. For example, one 20-year-old cis-man said: “I have anxiety with calling and or answering a phone,” and a 16-year-old transgender participant similarly reported: “I struggle with phone calls severely as they are extremely overwhelming to me as an autistic individual.” A 21-year-old non-binary person wrote: “Phone calls are scary and I am misunderstood.” A 20-year-old transgender boy wrote: “I have horrible anxiety on the phone and have heard negative stories about the hotline.” An 18-year-old cis-woman said, “Not the most confident person on the phone.” Other participants expressed concern about phone-related privacy—such as not wanting their parents to see that they had called 988 from cell phone call records or to overhear them talking. One 18-year-old transgender participant who had not used 988 wrote: “My home is not a safe place to call these numbers.”
Theme 2d: Among those with direct experience, dissatisfaction with wait times
Some of those in this sample who had direct experience with 988 had experience of reported being unsatisfied with call wait times. For example, one 18-year-old cis-girl wrote: “Every time I try to contact them I literally get no response and I’m on hold or waiting for someone for hours at a time. They don’t respond and it’s ridiculous.” In addition, an 18-year-old non-binary person wrote: “Every time I have called a hotline I have been put on hold for over 30 minutes, which by that point I usually hang up because it’s not worth it,” and a 21-year-old cis-boy wrote: “Last time I tried, I was on hold for a very long time.”
Theme 2e: Among those with direct experience, negative experiences with the counselors
Of the 29 autistic individuals who had direct experience using 988, 10 had negative experiences with things the counselors said or did. Some relayed dissatisfaction in general terms. For example, one 19-year-old non-binary person reported: “I have used it before and have had horrible service that was not at all helpful,” and a 22-year-old non-binary person wrote: “Bad communication and not very attentive.” However, some participants relayed things that counselors said to them that they felt were harmful. For example, a 14-year-old gender minority individual wrote: “Because the last time I called, I was told that if food makes me sad or anxious to just eat less, although I already eat 700 calories or less every day.” A 16-year-old cis-girl reported: “Last time I called them they told me to do it and hung up.” A 17-year old reported “I called once…the person on the phone dismissed my feelings, told me it didn’t matter…I’ve never called after that.” The idea that there may be uneven quality by counselors was underscored by the following brief statement from a 17-year-old trans boy who reported: “Bad experience, uninformed volunteers.” Part of the problem, at least according to one 16-year-old non-binary participant, is that the counselors may have limited training or have difficulty concentrating during some calls. They wrote: “They rarely help. They have a very basic understanding of mental health and don’t remember what you just said half the time.” This was echoed in a statement by one 21-year-old cis-woman participant who indicated that they had experience with 988 calling emergency services to intervene with them. They wrote: “[988] is not accessible. I have communication differences and I have had the police unnecessarily called on me based on how I said something before.” There were also at least two participants who specifically struggled with the standardization of counselor responses. “All they do is carelessly parrot back what you say and send the same resources,” wrote a 22-year-old cis-girl. A 17-year-old cis-boy also expressed the idea that his counselor interaction felt impersonal: “Sometimes it feels like talking to a robot when I just need a friend,” he wrote, “I feel like it doesn’t really help.”
Discussion
This qualitative study analyzed the write-in responses of 13–22-year-old autistic youth and young adults who participated in a U.S.-based online survey that asked them for their opinions about the 988 Suicide & Crisis Lifeline. The study uncovered mixed feelings on the part of the participants about 988. Specifically, among those who had direct experience using 988, some had positive experiences and reported that 988 had helped them refrain from hurting themselves or otherwise provided support that they found useful. There were also autistic participants who did not report having used 988 themselves, but said that they were favorably inclined to use 988 because they expected that the counselors would be well-trained, non-judgmental, and that the anonymity would be important to them. In contrast, there were autistic participants who had used 988 and had negative experiences—including long wait times and unhelpful comments from counselors. And some autistic participants who did not indicate that they had used 988 reported being unlikely to use it because they were afraid of police intervention and being institutionalized, doubtful that their unique needs as autistic people or people with psychiatric disorders or gender-minority identities would be adequately supported, and because they do not like to talk on the phone, suggesting that they did not realize that 988 has text and chat options.
Some of the concerns expressed by the autistic people in this sample are not unique to autistic individuals. Our team has produced a separate article that analyzed non-autistic youths’ opinions about 988, which found that sexual and gender minority youth were less likely to say that they would use 988 than non-sexual and gender minority youth and that reasons included fear of police and hospitalization (Colburn et al., under review). These findings align with a report published online by the Trans Lifeline in 2024 that reported that fear about nonconsensual emergency interventions which pose a threat to people in crisis, particularly for Black, Brown, LGBTQI+, disabled, and poor people, deters some people from using 988. 26 And, in 2022 and 2024, National Public Radio aired segments about the fact that people on social media were warning one another not to call 988 for some of the same reasons that autistic individuals in this sample listed, such as a fear of emergency intervention, long wait times, and uneven counselor quality.27,28 However, the findings of the present study suggest that autistic people may face some unique barriers to getting the help that they need from 988 as well. Specifically, some autistic people in this sample reported that they don’t like using telephones and seemed unaware that 988 has text and chat options. Autistic people in the sample also commented that they have had experiences of being misunderstood by crisis line counselors or others (i.e., communication challenges) and worry that misunderstanding might increase the risk that emergency services would be dispatched. Prior research has also documented that autistic people tend to prefer modes of communication other than voice calling on a phone, 29 so our findings are consistent with that evidence. Importantly, the 988 Suicide & Crisis Lifeline has increased availability of texting and chat engagement since its inception, but some autistic people in the sample misunderstood and thought that they would need to contact 988 via a phone call.
Importantly, both the 988 Suicide & Crisis Lifeline administration and autistic self-advocates are aware of the ways in which the autistic user experience of 988 could be improved and have already implemented some strategies intended to address that. For example, autistic self-advocate Lisa Morgan and ally Dr. Brenna Maddox presently co-lead the international Autism and Suicide Prevention Workgroup (ASPW), which has a goal of improving community services for autistic people to prevent suicide and self-harm (personal communication, Maddox, 2025). The ASPW created several written handouts aimed at neurodiverse people or those who support them and which are now available through 988 website. These resources include the following: “Warning signs of suicide for autistic people,” “Crisis supports for the autism community,” and “Reasons for living” (all available here: https://988lifeline.org/help-yourself/individuals-with-neurodivergence/). None of the youth in this study mentioned these documents in their comments. While some autistic youth may be locating them, reading them, and finding them helpful, there is a possibility that the documents are not being noticed or utilized by a large percentage of autistic youth who are feeling suicidal. Finding ways to make information for autistic people about 988, and about suicide, easier to find and more likely to be used should be explored. For example, adolescents may be more likely to engage with brief video clips than with PDF files they need to download using a web browser. In addition, although there is information about what happens when a user calls, texts, or chats 988 available on the U.S. Substance Abuse and Mental Health Services Administration (SAMHSA) website, the information is provided in blocks of text. Some autistic people may find visual information easier to understand or remember, 30 or may benefit from “Easy Read” accessible information, 31 so translating the frequently asked questions on the SAMHSA website, in collaboration with autistic self-advocates, to be more accessible may be meaningful. In particular, users of 988 should know precisely what 988 can and cannot keep confidential, what data they collect and store, under what circumstances they share data and how, and what triggers an emergency intervention. 32
This study was unable to investigate whether 988 counselors are using neurodivergent-friendly scripts or protocols when interacting with autistic people, which would be a good topic for subsequent research. When 988 counselors are serving autistic texters or callers, they may find that the standard scripts and risk assessments they use with the general 988 user population may not work, although this possibility should be investigated through research. 33 It is possible that the length of the 988 chat interaction, the time that the autistic user needs for processing, the support that autistic individuals need if they enter into an overwhelmed state (i.e., meltdown), and risk markers for imminent harm could be different than what counselors typically experience. Additional research that investigates these possibilities would benefit the field. Moreover, research that evaluates the positive predictive validity of the risk assessment tools in use by 988 counselors that result in the dispatch of emergency services to autistic people should be continually assessed. It is also likely that the quality of 988 services that autistic users receive varies by state and by call center. Efforts to evaluate quality and the consistency of quality across 988 call centers should be supported. Efforts to hire autistic counselors and have autistic people audit 988 call quality may also be beneficial.
Finally, an important implication of this research is that more investment in combating online misinformation about 988 is needed. According to a nationally representative survey conducted by Ipsos, most people (68%) who contact 988 report that they get the help that they need, 34 and available data suggest that only 1%–2% of 988 calls or texts result in emergency response. 32 The fact that 988 does help the majority of callers may not be known to autistic youth who are potential 988 users. That said, data on the percentage of autistic people who have used 988 and feel that they got the help they needed are not available, but would be an important datapoint to collect in future iterations of the Ipsos survey. If autistic people are disproportionately less likely to feel that they got the help that they needed when in crisis and in contact with 988, it would provide support for the idea that a special subnet for autistic individuals should be considered. Subnets or specific “lines” for subtypes of people experiencing a crisis who contact 988 are presently available for veterans, LGBTQI+ people, and Spanish-language speakers. When people in one of these groups first contact the crisis line, they can choose to connect to one of these specialty lines to talk with counselors who have received specific training for their subpopulation. There may be value in exploring whether a subnet for autistic, or neurodiverse people more generally, would be beneficial and drive an increase in the percentage of 988 users who report feeling satisfied with their experience. As an alternative, autistic people could be referred to warmlines that do not contact emergency services, such as the Wildflower Alliance, Trans Lifeline, Call Blackline, LGBT National Help Center, and StrongHearts Native Helpline. 35
This study faces several limitations. First, it was a qualitative study and as such not designed to produce generalizable results nor draw inferences from a representative subsample of autistic people. The study has uncovered the experiences of those who selected to participate in the online survey and provided an excellent starting point for thinking about ways that 988 may need to be improved to meet the needs of at least some autistic people, but it is possible that autistic people with more positive, satisfactory experiences with 988 chose not to participate in the survey. Second, our method for determining that 29 of the autistic participants had used 988 themselves may have classified some people as having used 988 when they had instead used a different crisis line or the previous iteration of 988, the National Suicide Prevention Lifeline. We interpreted comments in response to the question stem that referred specifically to 988, such as “I have used it and did not have a good experience,” to mean that someone had experience with 988. However, the individual might have been recalling an experience with a different hotline. It is also possible that we misclassified someone as having never used 988 who had, if we could not tell that they had from their written-in response. However, misclassifying participants as having used 988 when they did not would not have had a major impact on the results, as each theme was observed across comments from multiple participants. Third, we opted not to relay inter-rater reliability. There is a growing movement in the qualitative research community to eschew this type of calculation, which comes from quantitative approaches and “has roots in positivism and objective discovery with qualitative methods that favor an interpretivist view of knowledge.” 36 We agree with those who argue that qualitative researchers should focus on the meaning, richness, depth, and complexity of data and establish the trustworthiness of the coding through documentation of coding decisions, engaging in iterative coding discussions, and reflecting on positionality relative to codes together. As such, we opted to align our coding decisions through iterative communications and discussion. Fourth, this study was a secondary analysis of data collected through Project Lift Up, which is a study about suicide and bystander intervention among U.S. youth in general. A study designed to investigate issues related to crisis line use by autistic youth, specifically, will offer the opportunity to explore the issue in more depth. Fifth, Project Lift Up, the parent study from which these data were drawn, included an oversample of sexual and gender minority youth. Sexual and gender minority youth may have been more likely to express concern that they would not be understood or well served by 988. Sixth, individuals without access to devices to complete surveys, with impaired capacity (e.g., intellectual disability or traumatic brain injury), or without the reading skills to complete the survey were excluded. Future investigations on this topic should ensure access to research participation among such individuals.
Conclusion
Autistic adolescents and young adults report mixed perceptions about the quality of support offered by the U.S. 988 Suicide & Crisis Lifeline. While some autistic individuals like the idea of talking to a stranger and a trained counselor when in crisis, others expressed anxiety about using a phone, the idea that emergency services could be dispatched, and about the preparedness of counselors to support their complex and unique needs as autistic people. Although written handouts and information about 988 for autistic people are available online, autistic people in crisis may not be discovering those or be able to process the information contained in them. Upgrades and improvements to 988 that will result in better crisis support for autistic people are needed, feasible, and should be evaluated.
Footnotes
Acknowledgments
Data and/or research tools used in the preparation of this article were obtained from the National Institute of Mental Health (NIMH) Data Archive (NDA). NDA is a collaborative informatics system created by the National Institutes of Health (NIH) to provide a national resource to support and accelerate research in mental health. Dataset identifier: ![]() . This article reflects the views of the authors and may not reflect the opinions or views of the NIH or of the submitters submitting original data to NDA.
. This article reflects the views of the authors and may not reflect the opinions or views of the NIH or of the submitters submitting original data to NDA.
Author Disclosure Statement
All phases of this study were supported by National Institutes of Health grant R01MH128269.
Funding Information
This research was supported by the National Institutes on Mental Health of the National Institutes of Health under Award Number R01MH128269. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Authorship Confirmation Statement
E.F.R.: Conceptualization, formal analysis, and writing—original draft. L.G.H.: Formal analysis and writing—review and editing. M.M.: Formal analysis and writing—review and editing. J.C.: Writing—review and editing. D.C.: Project administration and writing—review and editing. V.B.: Funding acquisition, supervision, and writing—review and editing. K.M.: Funding acquisition, supervision, and writing—review and editing. The article has been submitted solely to this journal and is not published.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.