
Abstract
Introduction:
Autistic psychotherapists hold a unique and underexplored position within the mental health field. While research on autistic clients is growing, there remains a significant gap in understanding the experiences of autistic clinicians. This study adds to the emerging literature on neurodiversity-affirming care by centering the voices of licensed autistic psychotherapists.
Methods:
Using a qualitative approach informed by interpretative phenomenological analysis, this study explored the professional identities, challenges, and contributions of eight licensed autistic therapists in the United States. We recruited participants through targeted outreach in online communities and took part in in-depth, semi-structured interviews.
Results:
Analysis revealed six superordinate themes: (1) Integration of autistic identity into therapeutic practice, (2) challenges in navigating professional environments, (3) adapting therapy for autistic clients, (4) autistic therapist well-being, (5) unique contributions of autistic therapists, and (6) advocacy and systemic change. Participants highlighted the value of authenticity in their clinical work, the therapeutic benefits of shared identity with autistic clients, and the importance of peer support within autistic communities. They also described systemic challenges, including stigma, limited accommodations, and workplace environments built around neurotypical norms.
Discussion:
Findings underscore the need for more inclusive training, supervision, and workplace practices to support and retain autistic clinicians. Participants challenged deficit-based assumptions about autism and demonstrated how autistic therapists bring essential insight, innovation, and empathy to their work. This study contributes to the growing field of neurodiversity scholarship and offers practical implications for building more affirming, equitable mental health systems.
Community Brief
Why is this an important issue?
Autistic adults often face challenges when seeking mental health care, including finding psychotherapists who understand autism and offer affirming support. At the same time, more autistic people are becoming therapists themselves. These autistic therapists bring valuable insight to the field, but we know little about their experiences. This study helps fill that gap by hearing directly from licensed autistic therapists.
What was the purpose of this study?
The purpose of this study was to explore what it is like to be an autistic therapist. We wanted to understand how these therapists experience their work, how they manage challenges, and how their autistic identity shapes the way they practice therapy.
What did the researchers do?
We interviewed eight licensed autistic therapists. Each person took part in a one-on-one, in-depth interview over Zoom. The researchers then carefully studied the transcripts using interpretative phenomenological analysis (IPA). This method helps researchers understand how people understand their lived experiences.
What were the results and conclusions of the study?
The study revealed six key themes. Autistic therapists felt more connected to their work when they could be authentic, and they formed deeper bonds with autistic clients through shared understanding. However, they faced workplace challenges, including unrealistic expectations and limited accommodations. Many were cautious about disclosing their identity to colleagues due to fear of bias, although sharing with clients was empowering. Therapists regularly adapt traditional approaches to better support autistic clients. Burnout was a common concern, and participants emphasized the need for proactive self-care. Finally, they highlighted their unique strengths—empathy and pattern recognition—and embraced advocacy roles to promote neurodiversity-affirming care.
What is new or controversial about these findings?
This is one of the first studies to focus specifically on the experiences of autistic therapists. It challenges the idea that autistic people cannot be effective mental health professionals. Instead, it shows that being autistic can be a strength in therapy, especially when working with other autistic people. It also raises important questions about how mental health systems treat autistic professionals.
What are the potential weaknesses in the study?
The study had a small group of participants, most of whom were White and queer. Also, some were self-diagnosed, while others had formal diagnoses. This means the results might not represent all autistic therapists. More research with a broader group of people is needed.
How will these findings help autistic adults now or in the future?
These findings can help in several ways. They show the value of autistic therapists in the mental health field and may encourage more inclusive hiring, training, and workplace practices. They also show autistic clients the benefits of working with therapists who share their neurotype. Finally, the study supports the need for mental health systems to create environments that respect and support autistic professionals and clients alike.
Keywords
Introduction
Autism has undergone a significant shift in perception, moving from a deficit-based model to one that recognizes autism as a neurodivergent identity, rooted in inherent brain and nervous system differences, requiring societal accommodation and acceptance. 1 The neurodiversity paradigm has largely driven this transformation, as it challenges traditional notions of pathology and instead emphasizes that autistic individuals possess unique cognitive, sensory, and social strengths that contribute to human diversity. 2 Although still limited, a growing body of research has started to explore the lived experiences of autistic adults, increasingly centering themes of identity, well-being, and self-understanding.3,4
As research and public awareness have expanded, so has our understanding of the communication and social challenges that often arise in cross-neurotype interactions.5,6 This growing awareness has sparked increasing interest in exploring the experiences of autistic individuals when seeking medical and mental health support, mainly because these interactions frequently involve discussions of emotional, interpersonal, and deeply personal matters, contexts in which cross-neurotype communication barriers may be especially pronounced. Emerging research highlights the significant barriers autistic adults face in accessing mental health care from professionals who have a deep understanding of autism and how to work effectively with autistic individuals.7,8 However, much of this research has focused on autistic individuals as clients navigating the mental health system, with far less attention given to their experiences as professionals. This paradigm shift has coincided with an increase in autism diagnoses, particularly among adults who were previously undiagnosed or misdiagnosed. The Centers for Disease Control and Prevention now estimates that 1 in 36 children are diagnosed with autism, reflecting both improved diagnostic practices and broader awareness. 9 In addition, the growing recognition of autism in adults has revealed a “lost generation”—autistic individuals whom clinicians did not identify in childhood but recognized in adulthood. 10
The lost generation and clinical implications
This “lost generation” of autistic adults primarily consists of individuals who were not identified in childhood, often because they did not have co-occurring intellectual disability, are verbally fluent, and would now likely meet the criteria for an Autism Level 1 diagnosis under current DSM-5-TR criteria. Many of these individuals have significant mental health needs, with research suggesting that they face an elevated risk of psychiatric distress, suicidality, and misdiagnosis.11–15 While both high-support needs and low-support needs autistic individuals face nearly double the mortality risk compared with the general population, those without co-occurring intellectual disability experience a significantly higher risk of death by suicide.11,12 The delayed recognition of autism in this group has led to a surge in late diagnoses in adulthood, 14 often occurring only after individuals enter the mental health system in crisis.
Further highlighting this clinical shift, research has documented a dramatic increase in late autism diagnoses over the past two decades. Atladóttir et al. 16 found that individuals born between 1999 and 2001 were over four times more likely to receive an autism diagnosis compared with those born just a decade earlier, reflecting both heightened awareness and evolving diagnostic criteria. Similarly, Nyrenius et al. 14 examined individuals seeking outpatient psychiatric care in Sweden. They found that 18.9% of patients had clinically significant autistic traits—meaning they were likely autistic—yet only 0.53% had an official autism diagnosis. This disparity suggests that a large proportion of autistic adults go unidentified within psychiatric settings, leading to potential misdiagnosis, inappropriate treatments, and barriers to accessing neuroaffirming care.
Most autistic adults also experience co-occurring mental health conditions, leading to a high demand for mental health services, including psychotherapy. 17 However, access to appropriate mental health support remains a significant challenge. Autistic adults most commonly report barriers such as therapists’ lack of knowledge and expertise surrounding autism, as well as clinicians’ reluctance or refusal to treat autistic individuals.7,8 This gap in accessible care further exacerbates mental health disparities for autistic adults, highlighting the urgent need for clinicians who understand autism from a neurodiversity-affirming perspective.
The lack of professional preparedness has created a critical challenge in mental health, as many clinicians feel ill-equipped to work with autistic clients. Traditional training often lacks adequate education on adult autism, contributing to misdiagnosis, inadequate treatment, and the persistence of outdated, deficit-based models.8,18 Autistic psychotherapists may be uniquely positioned to contribute to this affirming shift, offering insights that could help reshape clinical culture toward greater neuroinclusion. However, their experiences, perspectives, and professional contributions remain largely unexamined in research.
The increasing recognition of autism in adulthood has also led to greater disclosure of autistic identity among professionals in health care and mental health services. In response, an autistic clinician community has emerged, with directories such as ndtherapists.com, neurodivergentpractitioners.org, and autistictherapist.com listing autistic practitioners. These resources reflect growing interest within both the autistic and broader mental health communities in understanding the experiences of autistic clinicians. Despite this increasing visibility, no peer-reviewed studies have systematically examined the experiences of autistic psychotherapists. 1 At the time we initiated this study, no peer-reviewed research had systematically examined the experiences of autistic psychotherapists in the United States; however, a recent study from the United Kingdom has since explored related experiences among autistic counselors, underscoring the increasing scholarly attention to this area. 19
Problem statement
While research on autistic adults’ lived experiences has expanded,3,20 and studies on neurodiversity-affirming therapy for autistic clients have increased,21,22 researchers have largely overlooked the experiences of autistic professionals. This lack of research has significant implications for the mental health field, as it leaves critical gaps in understanding how autistic therapists navigate their professional roles. As mental health services increasingly recognize the need for neurodiversity-informed care, the absence of research on autistic clinicians means that training programs, supervision models, and workplace policies may fail to support or retain autistic professionals adequately. Thus, the primary objective of this study is to explore the lived experiences of licensed autistic psychotherapists through IPA, providing insight into how they perceive and make sense of their professional identities. The key research question guiding this study is as follows:
What are the experiences of being an autistic therapist, and how do they understand and make sense of their experiences?
Given the exploratory nature of this research, participants’ perspectives may generate new research questions and inform future studies on autistic professionals in mental health care. Beyond expanding scholarly knowledge, these findings have practical implications for the mental health profession that may help inform training programs, workplace policies, and supervision practices, helping to create environments that better support and retain autistic clinicians.
Methods
Ethical considerations
Alliant International University’s Institutional Review Board approved the study to ensure adherence to ethical guidelines for research involving human participants. We briefed all participants on the study’s objectives and procedures before participation. Participants provided informed consent through a digitally submitted form and again verbally before the start of each interview. We reminded the participants of their right to withdraw or stop the interview process at any time. At the completion of the interview, we debriefed the participants and provided them with mental health resources. Lastly, before concluding the interview, we asked participants if they would still like their data included in the study.
Study design
We used IPA, following the methodological framework developed by Smith et al., 23 because it offers a systematic approach in examining how individuals make sense of their unique experiences. The method is particularly well-formulated to capture nuanced insights into participants’ perceptions and interpretations, aligning closely with the study’s objective of understanding the lived experiences of autistic therapists. Given the significant gap in the existing literature on this topic, IPA also provided a valuable lens to capture the depth and nuance of participants’ perspectives, contributing to a foundational baseline understanding of autistic therapists’ experiences.
Participants
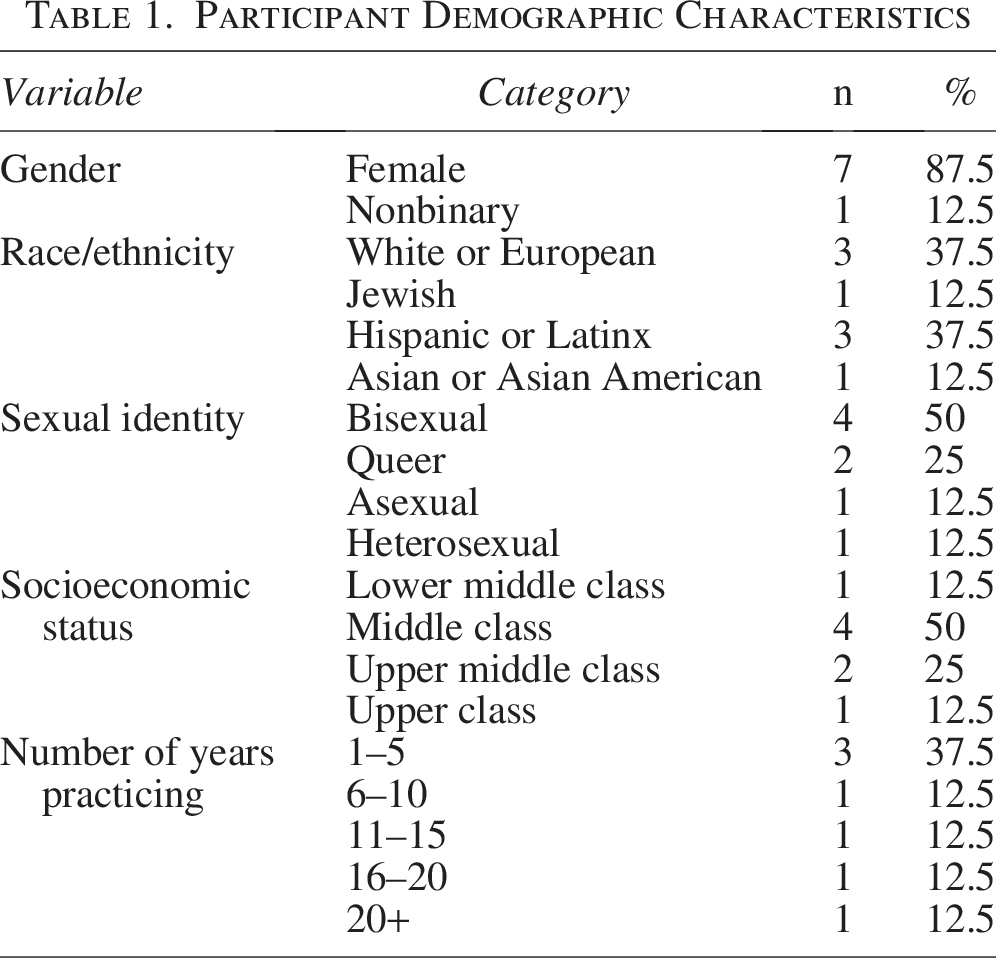
We recruited eight participants through purposive sampling (Table 1), which involved posting a flyer in neurodivergent clinician Facebook groups. The first author (J.H.) contacted interested participants via an online form that outlined additional details about the study and an online screening form. The research team subsequently contacted potential participants via email to confirm eligibility. The inclusion criteria were as follows: (1) age 22 or older, (2) active licensure to practice psychotherapy in the United States, and (3) self-identified or formally diagnosed as autistic. We excluded clinicians licensed for fewer than 12 months. Participants received a $25 Amazon gift card as compensation for their participation.
Participant Demographic Characteristics
Data collection
The researchers conducted semistructured interviews virtually via Zoom. Each interview lasted approximately 90 minutes. In line with research highlighting the importance of providing questions in advance to support autistic participants, 24 we sent all participants the full list of interview questions beforehand. This approach allowed for additional processing time, and we encouraged participants to prepare notes or ideas they could refer to during the interview.
The core research team developed an interview schedule consisting of 26 open-ended questions (see Table 2). We audio-recorded and transcribed all interviews using transcription software. We then reviewed transcripts for accuracy and returned them to participants for member checking, allowing them to clarify, revise, or expand upon their responses.
Interview Questions

To honor autistic communication styles and sensory preferences, we offered participants flexibility in how they engaged with the interview. 25 Options included turning cameras off, using Zoom’s chat function for text-based responses, engaging in body movements, eating or drinking during the session, and adjusting sensory elements in their environment as needed. In addition to verbal responses, we also invited participants to share supplementary materials—such as journal entries, poems, or visual media—allowing for expression through multiple modalities.
Data analysis
The research team analyzed the data using the IPA approach that Smith et al. 23 described and drew on foundational principles outlined by Smith and Osborn. 26 IPA aims to explore how people make sense of their experiences while recognizing that these experiences cannot be directly accessed; rather, researchers interpret them through a “double hermeneutic,” where participants seek to make sense of their lives and the researcher, in turn, seeks to make sense of that meaning-making. Analysis is idiographic and iterative, attending closely to individual accounts before considering patterns across participants.
Following IPA’s flexible but structured guidelines,23,27,28 the researchers (J.H., I.H., J.A.-G.) conducted the analysis through several stages. Each researcher independently read and reread the transcripts for immersion and made exploratory notes focusing on descriptive content, linguistic features (e.g., metaphors, repetition), and conceptual reflections. Each researcher then transformed these notes into emergent themes, which captured psychologically meaningful aspects of each participant’s experience. They then identified connections between emergent themes, clustering related concepts into higher level superordinate themes. They repeated this process for each case individually, with attention to maintaining an open stance so that new themes could emerge rather than imposing prior cases onto subsequent analyses. Only after completing this case-by-case analysis for all participants did the team look for patterns of convergence and divergence across cases, revisiting individual transcripts to ensure interpretations remained grounded in the data.
Each researcher independently conducted this analytic process and developed thematic structures for each case. The team then engaged in reflective dialogue to examine similarities and differences in interpretation and collaboratively synthesized a master thematic framework. While team-based IPA is less common, recent work by Rajasinghe et al. 28 demonstrates the value of collaborative analysis in enriching interpretive depth. Our collaborative approach enabled layered insight while preserving idiographic focus, particularly because all researchers involved in the analysis brought lived experience as autistic clinicians. The first author (J.H.) is an autistic licensed clinical psychologist. Coauthors (I.H., J.A.-G., and C.L.) are clinical psychology doctoral trainees who specialize in neurodiversity-affirming assessment and therapy. I.H. and J.A.-G. identify as autistic, and all members of the research team align with the neurodiversity paradigm that conceptualizes autism through a strengths-based, nonpathologizing lens. As autistic and neurodiversity-affirming clinicians, we recognize that our shared neurotype has shaped all aspects of our research process from design, recruitment, data collection, and interpretation.
The team approached reflexivity as an ongoing, active process: rather than attempting to “bracket” personal experiences, they critically examined and documented how their shared neurotype and professional identities shaped meaning-making. This transparency aligns with IPA’s recognition that all analyses are situated rather than neutral.
To enhance coherence and resonance, an independent researcher reviewed the final thematic structure and provided an external perspective. The team also invited participants to review emergent themes and offer feedback. We included the opportunity for participant input to support credibility and ensure that the analysis remained grounded in their lived experiences. However, none of the participants chose to provide feedback.
Results
As illustrated in Figure 1, the analysis of participant interviews revealed six primary themes, each endorsed by at least five of the eight participants. Within each theme, multiple subthemes emerged, offering additional depth to the participants’ lived experiences. To protect confidentiality, we have used pseudonyms for all participants.
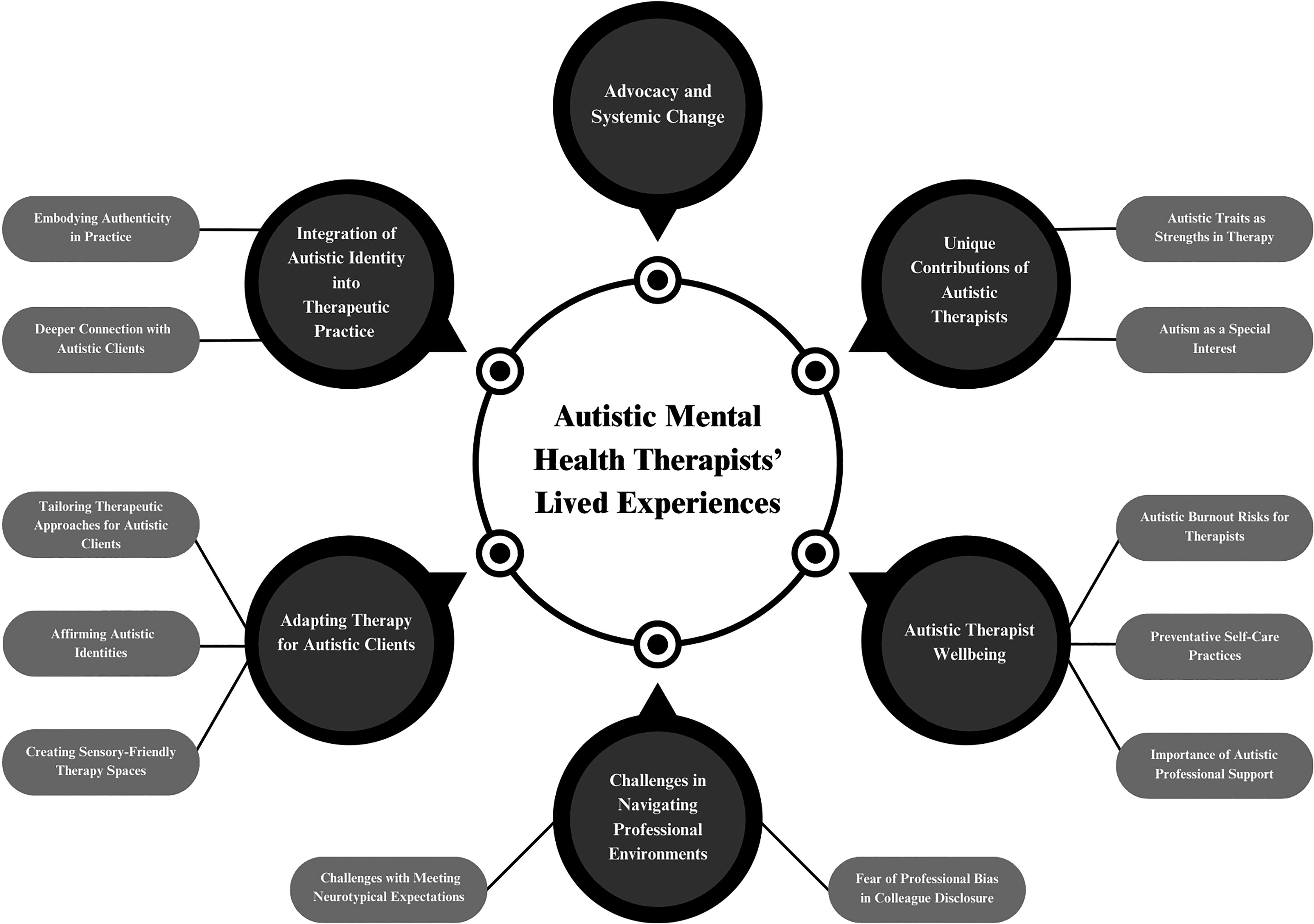
Diagram of superordinate themes and subthemes.
Theme 1: Integration of autistic identity into therapeutic practice
The first superordinate theme describes how participants’ autistic identity shaped the internal and relational aspects of clinical work, illustrating how participants’ autistic identity shaped the moment-to-moment therapeutic encounters.
Subtheme 1.1: Embodying authenticity in practice
Participants explained that incorporating their autistic identity into their professional roles allowed them to embrace authenticity and unmask. Marina explained, “I share my authenticity to the extent that I have learned to access that for myself. I share that process and my increasingly unmasked way of being with my clients.” Similarly, Taylor shared that they “don’t do faux professionalism,” describing it as a form of performance that felt inauthentic. Participants described both verbal and nonverbal ways of unmasking and embracing authenticity in their therapeutic work. Nonverbally, they shared that they allow themselves to stim, fidget, or avoid eye contact, rather than conforming to neurotypical nonverbal expectations. Verbally, some noted that they explicitly communicate their preference for direct communication and welcome spontaneous moments of connection. Therapists also found that openly disclosing their autistic identity helped to normalize autistic and strengthen the therapeutic alliance—particularly with autistic clients, who felt seen, validated, and empowered by the shared experience. In response, participants noted that their clients experienced a reduction in feelings of shame surrounding their own autistic experiences. As Jackie shared, “Being able to normalize like I use myself as an example for shit…I think it really helps people with shame.” By deliberately embodying authenticity through unmasking, participants challenged neurotypical norms of therapist conduct and created a therapeutic environment that not only validated autistic ways of being but also empowered clients to embrace their own authenticity.
Subtheme 1.2: Deeper connection with autistic clients
Participants highlighted that their autistic identity enabled them to cultivate a richer, more attuned connection with autistic clients. Clients of the participants have reported feeling seen, validated, and understood in a unique way as a result of this shared experience. As Jackie reflected, “My identity has largely brought me the clients that I work with, because they’re looking for somebody who gets it on that bone-deep level instead of guessing and trying to make sense of it.” Participants noted that clients actively sought them out specifically because of their autistic identity, often following prior experiences of misattunement or invalidation in therapy. Cameron shared, “I’ve had parents come to me specifically because I am Autistic… They were like, ‘We need her to see someone who is Autistic, because this is not working.’ Similarly, Taylor observed, “I started noticing that my Autistic clients thought I was the best therapist they ever had, and the only one that was the first to truly understand them.” Participants shared that their lived experiences often became clinical expertise, allowing them to meet autistic clients with deeper empathy and attunement, particularly when supporting them through shutdowns, meltdowns, or sensory sensitivities. As Jordan shares, “Yes, I can relate. Everything—meltdowns, shutdowns, dysregulation—I’ve been there.” These findings suggest that shared neurotype between therapist and client can significantly enhance therapeutic attunement, offering a uniquely validating and effective relational context for autistic clients.
Theme 2: Challenges in navigating professional environments
The second superordinate theme revealed that participants faced challenges in professional settings that lacked accommodations and understanding of their autistic needs.
Subtheme 2.1: Challenges with meeting neurotypical expectations
Autistic therapists often face challenges navigating the expectations of neurotypical professional environments, which can clash with their natural ways of processing and regulating. These are particularly pronounced in clinical settings that demand multitasking or rapid transitions between tasks without sufficient decompression time. Many participants described the emotional toll of managing unrealistic workloads that fail to account for their traits of heightened emotional sensitivity and deep attunement to others’ distress. As Taylor noted, “They pushed on a very high workload that doesn’t account for hyper empathy.” These experiences reflect the unrealistic expectations between neurotypical workplace norms and the needs of autistic therapists.
Subtheme 2.2: Fear of professional bias in colleague disclosure
Participants reported significant hesitation in disclosing their autistic identity to peers, citing concerns about bias, disbelief, and damage to their professional credibility. Many feared that others would question their competence upon learning of their diagnosis. Marina stated, “I both fear that other therapists are going to see I’m Autistic and have biases and assume I can’t be competent” (Marina). Others echoed this concern, noting anxiety around being misunderstood. “I fear people will make assumptions that I can’t have normal and effective—perhaps even sometimes too much—empathy,” one therapist explained. “I also fear they won’t believe I’m Autistic because they see that I’m a therapist” (Marina). Some participants described negative consequences following disclosure. Taylor recalled a colleague distancing themselves: “I said, ‘Hey, I’m Autistic,’ and then the guy… just bowed out.” These findings reveal the pervasive fear of stigma and professional invalidation that autistic therapists face when considering disclosure to colleagues.
Theme 3: Adapting therapy for autistic clients
In the third superordinate theme, participants drew from their own lived experiences as autistic therapists to reflect on the unique ways they show up in the therapy room.
Subtheme 3.1: Tailoring therapeutic approaches for autistic clients
Many participants reflect on the limitations of using traditional models of therapy with autistic clients—often because they themselves had felt misunderstood by these models. Many participants shared that traditional models of therapy were not developed with autistic people in mind and often required substantial modification to be affirming and effective. As Jackie stated, “I recognize that every modality I use is going to have to be adapted in some way for the people that I work with because none of it was developed for Autistic people.” Rather than adhering rigidly to manualized models, participants emphasized a flexible, client-centered approach that prioritized attunement to individual needs. Participants explicitly rejected one-size-fits-all methods, instead drawing on multiple modalities and adjusting them as needed. For example, Jordan stated, “I don’t follow the traditional models rigidly. I adapt them to suit the person in front of me, especially when I work with neurodivergent people.”
Quinn shared that one challenge they face when working with autistic clients within traditional clinical communities is that deviating from evidence-based methods, which may not be most effective for autistic clients, can be stigmatized as “bad therapy.” This leaves Quinn feeling caught between professional expectations and what they know would best support their client. Similarly, Aya described the internal conflict of being expected to deliver evidence-based interventions that, in retrospect, felt deeply misaligned with their values. “I was mandated to do exposure therapy,” they recalled. “I’ve actually… run into some of my patients that I saw at the hospital, and I’ve apologized to them, saying I am so sorry I did exposure therapy with you.” Aya’s repetition of the phrase “I’m sorry” and the phrase “absolutely doing harm” reflects a sense of conflict and regret.
One challenge participants commonly discussed was working with clients who experience alexithymia. Participants noted that asking generic therapeutic probe questions often felt forced or ineffective. For example, Taylor shared, “In session, we’re always like, ‘How does that make you feel?’ and sometimes that annoys the hell out of my Autistic clients.” Rather than forcing emotion-labeling, participants often leaned on psychoeducation, both because clients preferred them and because they did too. As Jackie explained, “A lot of Autistic brains really like to have information as to why things are happening. If I understand why it’s happening, I’ll retain the information and be able to integrate it.” Participants also described psychoeducation as a key component of neurodivergent-affirming therapy. Participants reported that autistic clients often valued clear explanations and explicit frameworks that helped them make sense of their experiences. This therapeutic style often mirrored the way participants themselves preferred to learn. For participants, these adaptations were rooted not only in professional experience but also in a shared understanding of what autistic clients need to feel understood and supported in the therapeutic space.
Subtheme 3.2: Affirming autistic identities
Across interviews, participants described a core belief shaped their clinical work: that being autistic is not something to be fixed. Much of this stems from their own experience knowing what it is like being dismissed by health care providers, as Marina and Quinn shared. Several described intentionally integrating neurodiversity-affirming values into their practice, which they shaped through their evolving relationship to identity and self-worth. As Taylor expressed, “I started bringing some of that affirming culture into my practice… the culture that there’s nothing wrong with you. You don’t need to be fixed. And let’s learn to love ourselves.” Similarly, Marina shared that giving an autism diagnosis often sends them home with “happy tears,” as they intimately relate and are moved by the relief and self-acceptance that come with having one’s identity affirmed. Rather than attempting to change their clients’ natural ways of being, participants saw their role as supporting clients in exploring and finding personal meaning in their autistic identity. As Quinn noted, “I am not here to make you not look Autistic… I’m here to help you figure out what does this mean for you?” This affirming stance involves honoring clients’ unique modes of communication and resisting the pressure to adapt to neurotypical standards. “We have to pivot and translate our language into theirs,” Taylor reflected. “It’s important to affirm their language and not teach them to speak ours.” Together, these accounts reveal how participants’ lived experiences reflect a shared commitment to honoring autistic identity in both philosophy and practice.
Subtheme 3.3: Creating sensory-friendly therapy spaces
Participants described the nontraditional use of sensory-aware technique practices they had developed for their own regulation and now integrated intentionally into the therapeutic relationship. Both Maria and Jackie described sensory self-care as “powerful” within their own lives and in session. One therapist shared, “I integrate somatic experiencing into sessions, especially when clients struggle with sensory overload” (Taylor). This helps clients manage their sensory experiences as well as providing tools for self-regulation that could be applied outside of therapy sessions.
Quinn reflected on what it meant to sit with a client whose sensory experiences neurotypical providers would likely minimize: “They were describing these little sensory hells that autistic people get, but an allistic therapist would be like, ‘just get over it.’ It’s always ‘just do this, just do that,’ but it’s not that simple.” During sessions, therapists encourage clients to express themselves freely, whether through stimming, moving around, or adopting comfortable postures. As Cameron described, their approach was grounded in what they themself needed in the room: “I tell people, you know, like, I’m going to do what my body needs. Want to be on the floor, you want to be on the couch, you want to take your shoes off, you want to eat in here. Whatever you gotta want to do, you can do.” By offering this freedom, they created space not just for client comfort, but for shared regulation. “All of my kids and teens love that,” they added—reflecting how their willingness to honor their own body in the room opened permission for others to do the same.” Others similarly shared how they coregulate with clients through stimming and movement, creating a collaborative and embodied experience. “I’ve got patients that I stop them talking, and we get up together, and we stim together… I need you to stand with me. I need your body moving” (Aya). Rather than separating their autistic identity from their clinical role, participants allowed their lived experience to guide how they create affirming, flexible spaces where clients can feel safe and supported in expressing their needs and ways of being.
Theme 4: Autistic therapist well-being
The fourth superordinate theme revealed that participants identified autistic burnout as a significant risk due to the emotional and sensory demands of their work. They shared that practices such as taking longer breaks between sessions or scheduling lighter workloads were essential to prevent burnout and maintain their well-being.
Subtheme 4.1: Autistic burnout risks for therapists
Therapists shared their experiences with autistic burnout, particularly in neuronormative settings where expectations were high and accommodations were lacking (see subtheme 2.1). Marina humorously described their ongoing struggle, saying, “I joke that I’m in the suburbs of Burnout City. I’m not in Burnout City proper, but it’s a quick ride back to Burnout City from where I am, and so I do have to be thoughtful about how I handle that.” Participants also stressed the need to recognize and address burnout early. As Jackie emphasized, “If you don’t set healthy boundaries to start with, you are going to burn out, and Autistic burnout is dangerous” (Jackie). Participants described burnout as a frequent and anticipated part of their professional experience, but made clear distinctions between general clinical fatigue and what they identified as autistic burnout. This form of burnout stemmed from the cumulative strain of working in systems that do not accommodate autistic ways of processing, relating, or regulating.
Subtheme 4.2: Preventative self-care practices
Participants described the need to implement various self-care practices to prevent autistic burnout, emphasizing the importance of proactively identifying and engaging in activities that sustain their well-being. As Jordan stated, “Figure out your preventative self-care… you want to prevent cycles of burnout.” Examples included building spacious schedules, limiting caseloads, and prioritizing rest. Some left time between sessions, took regular days off, or structured their week to allow for recovery. Therapists also made environmental and sensory adjustments to support regulation, such as working from home, controlling lighting and sound, using comfort objects or weighted blankets, and scheduling stimming or movement breaks. Others described journaling, drawing, or resting in silence between sessions as essential. These practices served as a buffer against autistic burnout, enabling participants to sustain clinical work while honoring their needs.
Subtheme 4.3: Importance of autistic professional support
Participants discussed the importance of communal spaces for autistic mental health professionals, noting that online groups and communities have provided a safe space for them to feel understood and supported. Avery shared that having to hide their autistic identity is “devastating,” emphasizing a need for a space to openly share their experiences as an autistic therapist and feel seen. Jordan stated that “connecting with other Autistic professionals online has been a lifesaver for me… it’s where I feel most understood and supported.” Regarding online autistic communities, Avery shared that “It kind of feels like professionally speaking the only safe place to talk about being a therapist and being Autistic.” Marina shared that although they value shared autistic spaces, they find that they often have to navigate the potential of running into their own clients, thus limiting their ability to participate fully in these communities, highlighting the need for a shared space for autistic clinicians exclusively. Such spaces not only normalized the experience of being an autistic therapist but also foster a professional environment grounded in shared understanding, mutual validation, and authentic support.
Theme 5: Unique contributions of autistic therapists
The fifth superordinate theme revealed the unique strengths that participants’ autistic identity brings to their therapeutic work, including heightened empathy, pattern recognition, and a deep understanding of autistic experiences.
Subtheme 5.1: Autistic traits as strengths in therapy
Participants described various autistic traits as central to their therapeutic effectiveness. Cameron spoke of their love for “the puzzle part and the human behavior part,” highlighting how pattern recognition and analytic thinking supported their clinical insight. Sensitivity and embodied empathy were also commonly identified strengths. “Being sensitive can be helpful in working with people who are struggling,” Avery reflected. “When you can empathize, it’s a beautiful thing.” Many described developing strong observational skills early in life to navigate neurotypical environments—skills that later became assets in reading nonverbal cues and adapting communication in therapy. “The role-playing and masking I’ve done for so long… has actually helped me a lot as a therapist,” Cameron noted. Mirroring, once a survival strategy, was now used with intention to foster connection. Participants also described a deep, focused presence in session, often entering flow states. “It can feel like everything fades out,” Cameron shared. “I’m just… very like, there.” This immersion allowed them to remain attuned and engaged, with clients frequently commenting on how present they felt compared with previous therapists. In the interview with Quinn, they repeated variations of “we are really good therapists,” emphasizing both individual ability and shared identity: “Yeah, I mean, we’re out there, we are really good therapists. There’s really, really good therapists.” This repetition may reflect a linguistic attempt to reclaim authority and affirm professional legitimacy in the face of systemic doubt. Their emphasis on being “competent” and advocating for both themselves and others suggests a deeper resistance to ableist assumptions rooted in pride of their autistic identity.
Subtheme 5.2: Autism as a special interest
Participants described how their autistic identity shaped their professional journey, with autism itself becoming a special interest that drove their passion for learning, advocacy, and effective therapeutic care. For some, their personal connection to autism inspired their decision to become a therapist. As Jackie shared, “I became a therapist because I was Autistic… I wanted to help people and understand people.” Others described therapy as a domain that captivated their attention in the way special interests often do. “My specialty is this is what I think about all day long, all Autism all the time. So, you know, you’re not gonna get another therapist in town who is more affirming or knows more about autism than me. Now, granted, I live in a tiny little town, but I’m very confident no one else here knows more than me. So I might as well shout it out” (Taylor). This passionate focus not only positioned them as knowledgeable and affirming practitioners but also provided their clients with a deeper understanding of autism beyond diagnostic criteria.
Theme 6: Advocacy and systemic change
The sixth superordinate theme reflects the external and systemic application of autistic identity, as participants moved beyond individual clinical work to educate communities and advocate for structural change in mental health care. Participants described advocacy not only as a professional responsibility but also as a personal imperative tied to their lived experience. As Jackie explained, “Being open about my neurodivergence allows me to be an advocate for my clients and for myself.” Participants used their positions to educate others, reduce stigma, and promote affirming practices—efforts that extended into their communities. Taylor shared, “I teach an Autism class in my community… I explain to them what Autism is, how their brain works, and give them strategies on how to affirm themselves.”
A strong call to action emerged across interviews: participants urged clinicians, researchers, and institutions to listen directly to autistic voices. “Research only is telling us so much,” Marina emphasized. “We need to listen to lived experiences.” Quinn, in a moment of emotional intensity, pleaded with the interviewer, their tone exasperated and urgent, as they said: “Listen to us about it. Listen to Autistic voices and listen to us.” The repetition of “listen to us” and the trailing off at the end of the quote conveyed both urgency and emotional exhaustion, signaling a deep desire to be heard and validated in spaces where autistic knowledge has historically been dismissed. Aya shared this feeling of frustration. Their narrative was marked by anger and urgency, conveyed through expletives, sharp imperatives, and vivid metaphor. Phrases such as “go fuck yourself and learn better” reflected a drive for justice. Their metaphor—“I’m giving people antibiotics, and they’re still using leeches”—evoked frustration with outdated, harmful practices and positioned themselves as a bearer of more current, affirming knowledge. The repeated commands—“Learn better. Listen. Maybe learn something.”—created a rhythmic, insistent tone, signaling more than anger, a plea to be heard and taken seriously as an autistic expert. Participants expressed, both verbally and nonverbally, frustration at being excluded from shaping the very systems meant to serve them, calling for a shift away from deficit-based models and toward systems that center autistic perspectives, affirm lived experience, and meaningfully include autistic voices in shaping care.
Discussion
This study explored the lived experiences of autistic mental health therapists, with the aim of understanding how their autistic identities shaped their professional lives. Using IPA, the research uncovered several interrelated themes that illuminate both the challenges and strengths associated with being an autistic clinician. Central to these findings were participants’ experiences of stigma and masking in neurotypical clinical environments, the psychological toll of navigating unsupportive workplace norms, the protective value of peer connection, and the ways in which their autistic traits enriched their therapeutic work.
A central theme was the impact of discrimination and stigma within clinical settings (Subtheme 2.2). Participants expressed concerns about being misunderstood by colleagues and supervisors, often encountering misconceptions about autism that cast doubt on their competence or suitability for clinical work. These dynamics required participants to carefully assess when and to whom they could safely disclose their identity, often weighing the potential risks of being seen as incompetent or unreliable by colleagues. Many autistic individuals choose not to disclose their neurotype because of previous negative experiences with disclosure, which further reduces access to support and increases the detrimental effects of masking. These choices are often rooted in survival, as organizational settings are rarely psychologically safe spaces for authenticity.29,30 This aligns with existing research showing that autistic professionals frequently experience stigma, bias, and exclusion due to widespread misunderstandings of autism and a lack of familiarity with autistic communication and support needs.31,32 Moreover, the decision to mask is often compounded by intersecting identities such as race, gender, class, and co-occurring disabilities, which influence how autistic individuals are perceived. 29 These environments often pressured autistic clinicians to conform to neurotypical norms of professionalism, which meant masking or camouflaging traits to avoid negative social or employment consequences.29,33
However, research consistently demonstrates that masking is both psychologically and physically costly. It is associated with heightened anxiety, stress, and a diminished sense of authenticity,29,34 increased symptoms of depression, and feelings of social disconnection. 20 These effects reflect a broader pattern whereby autistic individuals internalize the stigma they experience in educational and occupational settings, leading them to adopt individual coping strategies aimed at appearing neurotypical. 35 These strategies—such as masking, camouflaging traits, and avoiding disclosure—operate to protect the autistic individual from encountering stigma and discrimination, but ultimately reinforce the dominance of neurotypical norms and uphold systemic inequalities in the workplace.29,36 The result is a double bind: to be accepted, autistic professionals often mask the very traits that define their neurotype—yet this concealment contributes to autistic burnout, emotional exhaustion, worse mental health outcomes, and the persistence of ableist organizational cultures.37,38
Participants described how workplace pressures intertwined with their experiences of autistic burnout (Subtheme 4.1). Autistic burnout is a condition characterized by persistent, long-term exhaustion, diminished executive functioning, and heightened sensory sensitivity, stemming from chronic stress and a fundamental misalignment between external demands and internal capacity, exacerbated by inadequate support and accommodations.33,39 Participants emphasized that this burnout was not only the result of high caseloads but also the ongoing effort of navigating neurotypical workplace expectations that conflicted with their natural ways of processing and regulating (Subtheme 2.1). A lack of accommodations and understanding compounded these challenges, particularly in meeting neurotypical expectations around multitasking, brief transition periods, and limited time for emotional decompression between sessions. In clinical settings, such norms often overlook the cumulative cognitive load of masking, the emotional toll of hyper-empathy, and the need for alternative regulation strategies.
In navigating these professional challenges, participants emphasized the importance of social support, particularly from peers who share their autistic identity (Subtheme 4.3). Autistic colleagues offered validation, empathy, and understanding, which participants identified as pivotal in managing workplace stigma and isolation. Specifically, participants highlighted nontraditional forms of social support—particularly online communities (virtual peer groups, consultation/supervision groups)—as especially valuable. These digital spaces provided a unique opportunity for authentic, affirming interactions where participants could openly discuss their experiences without the pressures of masking or the fear of judgment often prevalent in workplaces steeped in neuronormativity. This aligns closely with existing literature that underscores the therapeutic value of online autistic communities as safe, empowering spaces that foster identity affirmation, mutual understanding, and emotional validation. 40 This innovative form of social connection appears particularly beneficial for autistic clinicians, who may face compounded stigma due to their intersecting professional and autistic identities.
In addition, many participants recognized their autistic identity as a clinical strength (Subtheme 5.1). They reported that their lived experience of autism enhanced their therapeutic practice by fostering deeper connections with autistic clients, promoting authenticity, and informing neurodivergent-affirming care. Their ability to recognize and validate the unique needs of autistic individuals positioned them as valuable advocates for autistic clients navigating mental health services. Tomczak and Kulikowoski 41 propose that job characteristics perceived as demanding for neurotypical employees may serve as strengths for autistic individuals. In a therapeutic context, autistic clinicians’ ability to maintain intense focus, ask questions that penetrate to the root of the problem, and engage in direct conversations—often less inhibited by social conventions—enhances intervention effectiveness. 42 This capacity for deep inquiry allows for a more precise understanding of clients’ difficulties, facilitating meaningful therapeutic insights. Participants also reported that autism itself became a special interest, driving them to deeply engage with neurodiversity research, refine their therapeutic approaches, and develop a nuanced understanding of autistic experiences—ultimately making them more informed, empathetic, and effective clinicians.
Limitations
This study has several limitations. First, the sample was predominantly queer (87.5%), which may limit generalizability to autistic therapists with other sexual identities. We also did not control for variables such as years in practice or duration of awareness of one’s autistic identity—both of which may influence professional perspectives. We limited recruitment to select Facebook groups, introducing sampling bias and likely overrepresenting individuals active in online neurodivergent communities. The sample lacked racial diversity, with 62% identifying as White, further limiting applicability. Finally, the study did not distinguish between formally diagnosed and self-identified autistic participants (five and three, respectively). While both experiences are valid, research suggests that self-diagnosed individuals may face distinct psychological and social challenges—such as self-doubt, limited access to services, and fear of invalidation—which can shape how they relate to their autistic identity and professional role. 43 Not accounting for these differences may limit the nuance of our findings.
Future directions
To deepen the understanding of autistic therapy, future studies should examine outcomes with both autistic and neurotypical clients, including the potential benefits of matching autistic therapists with autistic clients. Given the limited racial and sexual orientation diversity in this sample, research must adopt a stronger intersectional lens. Autistic therapists are not a homogenous group—they hold intersecting identities related to race, gender, and sexuality. Future studies should amplify the voices of those with marginalized identities to build a more inclusive knowledge base. Research should also explore workplace experiences of autistic therapists, including barriers, supports, and accommodations. While this study identified challenges in formal work settings, future work should investigate how organizations can better support autistic clinicians. Specifically, are clinical training and supervision adapting to their needs—and if not, what changes are needed? Employers must move beyond performative inclusion to implement meaningful, systemic support.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
There was no funding associated explicitly with this study.
Authorship Confirmation Statement
J.H., J.A.-G., I.H., and D.M. contributed to the study formulation and concept and developed the interview questions. J.H. led participant recruitment. J.A.-G. designed the screening questionnaire and extracted data. I.H. designed the recruitment flyer. J.A.-G. led the data collection. J.H., J.A.-G., I.H., and M.N. conducted data analysis and theme extraction. J.H., J.A.-G., I.H., C.L., M.N., and D.M. drafted the article. All authors have reviewed and approved this article before submission. This article has been submitted solely to this journal and is not published, in press, or submitted elsewhere.