
Abstract
Background:
Autistic people can face remediable barriers and challenges with driving, yet there is no consensus around effective support methods. This review therefore sought to evaluate the implementation and effectiveness of driving support interventions for autistic people.
Methods:
We conducted a multimethod, participatory synthesis of evidence. Studies were obtained from MEDLINE, Social Policy and Practice, ASSIA, PsycINFO, CINAHL, ERIC, Scopus, and Epistemonikos. Data were extracted from those that implemented a driving support intervention with autistic people. No specifications on study design, outcomes, or comparators were made. Risk of bias (ROB) was appraised using the Cochrane ROB and Risk Of Bias in Non-Randomized Studies (ROBINS) tools (for controlled quantitative studies), as well as the EPPI-Centre (for qualitative studies) and NHLBI (for other uncontrolled studies) quality tools. The application and effectiveness of support interventions were narratively synthesized, while focal delivery components and mechanisms of action were examined using realist synthesis. All analyses were coproduced and developed by autistic adults.
Results:
Only 17 relevant studies (involving 402 autistic participants) were identified, which utilized varying designs and were generally appraised to be low in quality. The most well-researched form of support was simulation training; however, e-learning applications, anti-anxiety medication, listening to music, and cognitive-behavioral programs were also studied. Although positive results were documented for all interventions, at least in some form, assessments typically consisted of simulated driving tests and various contextual factors were overlooked. Specific delivery components were identified from the effective support programs, but evidence was lacking with regard to intervention mechanisms.
Conclusion:
Our participatory syntheses of data highlight that research is urgently required to address the driving barriers and challenges faced by autistic people. Despite promising but inconclusive evidence for simulation training and holistic cognitive-behavioral programs, widespread limitations are evident in existing studies and rigorous, generalizable intervention assessments are lacking.
Community Brief
Why is this an important issue?
Many autistic people face barriers or challenges with driving a car, which can prevent them from traveling independently. If research can identify effective driving support methods for autistic people, then we could potentially reduce these negative experiences and improve broader quality of life (e.g., by increasing access to employment, health services, and wide-ranging social opportunities).
What is the purpose of the review?
We examined various different driving support methods for autistic people that have been studied so far. We explored which methods are effective, what impacts they have on a person’s driving experiences, and which specific features or processes are common in successful support programs.
What did the authors do to review the literature?
We searched through seven scientific databases, looking for studies that focused on a form of driving support for autistic people. Once eligible studies were found, we examined what each support method consisted of, how they were practically delivered, and the effects that they have on various driving outcomes. We also examined information about the studies themselves (e.g., details about the measurements taken and population involved) and the overall “quality” of this evidence (using well-established assessment criteria). When analyzing this information, we worked with a group of autistic research partners (including both qualified drivers and non-drivers), who used their personal insight and lived experiences to develop findings and conclusions with our team.
What studies did the authors find?
Although 1216 articles were checked by our team, only 17 of these were relevant for our review. These 17 studies covered a range of support methods, including simulation training, e-learning apps, anti-anxiety medication, listening to music, and cognitive-behavioral programs. However, the studies that we assessed were generally low in quality.
In summary, what did those studies show?
Some positive results were reported for all support methods, particularly simulation training, but there is not enough evidence yet to make strong conclusions about any of them. It seems that programs have success when they try to reduce people’s anxiety, or when they use combined support packages (e.g., by delivering specialist driving sessions with classroom activities or occupational therapy). Programs that used personalized methods and extra learning materials also appear effective (e.g., workbooks, onboarding tutorials, guidance for instructors). However, it is likely that “effectiveness” will depend on various individual factors, such as how accessible support is and whether co-occurring conditions/difficulties are being suitably accommodated for.
What are the remaining gaps in the literature?
There is a general lack of studies examining driving support methods for autistic people. Existing studies often overlook important factors that might influence their results and rarely measure people’s driving skills or experiences during real-world road tests.
Based on this review, what do the authors recommend?
Our research team and partners conclude that there is an urgent need for future studies. Researchers and practitioners (e.g., organizations in the driving industry) must work together to develop new, evidence-based support tools that allow autistic people to overcome key barriers associated with driving.
Background
The ability to drive is an indispensable practical skill for many adults, which can have significant impacts on quality of life. Indeed, obtaining a driving license can lead to greater independence, reduced feelings of isolation, and improved access to employment, health care, and social activities. 1 Nonetheless, autistic people appear less likely to learn to drive and acquire a license than the rest of the general population. 2 For individuals who wish to drive, this may contribute to wide-ranging challenges and inequalities, in areas that are considered research priorities by autistic stakeholders3,4 (especially when considering the additional accessibility issues within public transport/services5,6). For instance, in practical terms, barriers to driving may also represent barriers to pursuing work or social opportunities (e.g., at times or places where other transportation is not viable), or barriers to completing routine daily tasks freely without undue stress (e.g., when shopping, visiting a gymnasium, or attending appointments).
Some driving challenges may relate to the cognitive and sensory differences of autistic people. For instance, autistic learners and qualified drivers self-report difficulties interpreting other drivers’ behavior or managing unexpected road environments.7,8 However, there are no conclusive data to show that autistic people are inherently “worse” at driving than non-autistic people, and self-reported difficulties might reflect lower self-confidence and wider systemic barriers (rather than objective skill differences). Indeed, many driver training and licensing procedures are poorly adapted for autistic people,7,9,10 and there is a perceived lack of support expressed by neurodivergent stakeholders.11–13 Moreover, driving difficulties may relate to co-occurring conditions that are disproportionately common in autistic populations, such as developmental coordination disorder (DCD), attention-deficit/hyperactivity disorder (ADHD), and anxiety. 14 Overall, studies therefore illustrate that there are greater barriers to driving for autistic people, and that research needs to identify effective methods for limiting these barriers and better helping individuals prepare for driving independently.
On this basis, it is important to consolidate the existing multidisciplinary evidence available within the literature to identify equitable driving support interventions for autistic people. Given the lack of systematic reviews with focused synthesis on this topic, it is necessary to identify any prominent approaches or scientific consensus that is beginning to emerge, while accounting for individual factors and lived experiences. Moreover, from the perspective of developing future support initiatives and systemic changes, it is necessary to explore possible mechanisms of action and delivery components associated with positive study outcomes. 15 Here, delivery components refer to the specific practices, processes, structures, and formats through which an intervention is implemented, which are likely to contribute to its effectiveness (at both an individual- and service- or environmental-level) and are common or translatable across different programs and contexts. 16
Accordingly, the aim of this systematic review was to evaluate the implementation and effectiveness of any interventions that have been used to support autistic people with driving. Using a combination of multimethod and participatory evidence synthesis approaches, we sought to align emerging scientific data and consensus with pertinent insight and lived experiences from autistic people, focusing on the following questions:
What types of driving interventions have been used to specifically support autistic people? Are these interventions effective in reducing autism-related driving barriers/challenges? How do these support interventions impact on autistic people’s experiences of driving? What delivery components characterize effective support interventions, and how are these programs implemented? What do the different sources of evidence suggest about intervention mechanisms, and how are these mechanisms contingent upon contextual and/or individual factors?
Methods
Research design
A multimethod review was undertaken, which synthesized evidence concerning the application of autism-focused driving support interventions, their outcomes, delivery components, and mechanisms of action. The focus of this review was determined at a public involvement event at the Centre for Applied Autism Research (University of Bath, UK). This event sought to establish the preferred research goals and priorities of autistic people in the southwest of England, based on the center’s ongoing research activities and expertise. Our ensuing review examined specific research topics and questions that were identified at the event, and forms part of a broader project aiming to codevelop new driving support tools for autistic people (see https://medicine.exeter.ac.uk/phss/research/vital/autistic-drivers/). A protocol was preregistered on the Open Science Framework (https://osf.io/q8ae2/), with our search strategy, eligibility criteria, and data extraction/synthesis methods all specified. The review follows the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines and recommendations for conducting inclusive neurodevelopmental research. 17
Eligibility criteria
First, population criteria stipulated that included studies must involve autistic people or individuals with a diagnosis of a directly associated condition (e.g., autism spectrum disorder, Asperger’s syndrome, pervasive development disorder not otherwise specified). Studies that did not present data from autistic people were excluded (e.g., reports from the perspective of instructors, or research involving people with nonspecified disabilities). However, we did not require any formal, clinician-based diagnosis to be reported and did not exclude studies that involved people with co-occurring conditions, such as ADHD and DCD. Moreover, we did not exclude studies based on any specific conceptions or classifications of autism (e.g., studies based on neurodiversity approaches and varying ICD/DSM criteria were eligible, to capture evidence from diverse scientific fields, time points, and international contexts).
For intervention criteria, the review included studies that implemented a driving support intervention as a major focus of their research. To be eligible, studies presented data associated with any driver skills/training program or method that was explicitly framed as a potential means of reducing autism-related driving challenges or barriers. Studies that did not contain an appropriate intervention were excluded (e.g., appraisals of public transport mobility programs or observational assessments of usual driving challenges). However, to capture a broad range of possible support methods, both single- and multi-component interventions were eligible. Moreover, we included studies relating to various subjective and objective intervention outcomes, including indicators of effectiveness (e.g., relating to any given driving skill or barrier), implementation data, user experiences, and economic evaluations.
Finally, study design criteria ensured that the review synthesized diverse evidence; thus, designs were not restricted to any given language, dates, or region, and any included studies could be comparative or noncomparative in nature. Eligible designs included randomized and nonrandomized controlled trials, cross-sectional comparisons, pre- to post-test experiments, crossover studies, factorial analyses, pilot/feasibility assessments, cohort observations, validation tests, qualitative evaluations, and proof-of-concept investigations. Studies were excluded if they were not published as full-text articles (e.g., conference abstracts) or if they did not constitute primary research (e.g., literature reviews, book chapters).
Search and selection
Searches were undertaken on January 26, 2024, in MEDLINE (Ovid), Social Policy and Practice (Ovid), ASSIA (ProQuest), PsycINFO (Ovid), CINAHL (EBSCO), ERIC (EBSCO), Scopus (Elsevier), and Epistemonikos. These searches included terms for the review’s population and intervention, along with database-appropriate subject terms and combinations. Search strings are detailed in Supplementary Data S1 and were informed by the Cochrane Handbook. 18 In line with the broad scope of this review, we also conducted searches for gray literature evidence (including full-text reports and theses), and no filters for study designs were applied. Authors were contacted in cases where a full-text article could not be accessed. Search records were exported into an EndNote library (Clarivate) and deduplicated. Titles and abstracts were then examined by two reviewers (T.A. and D.H.), independently and in duplicate, for relevance and inclusion. Retained records were merged into a shortlist of studies, and full texts assessed against the preregistered inclusion criteria. These assessments were made independently and in duplicate by two reviewers, with any disagreements resolved via recourse to a third reviewer (G.J.M.-T.). We recorded study exclusions hierarchically, in order of (1) inappropriate interventions; (2) inappropriate populations; and (3) inappropriate study types or report focus.
Data labeling and extraction
Identified studies were initially labeled to facilitate mapping analyses and data syntheses. We assigned descriptors based on the relevant population, study type/design, and the outcomes reported in each trial. Labels relating to the support intervention were also assigned, with respect to its type, setting, region, time frame, and any co-interventions implemented. Once labeled, summary details of each study were extracted as free text by two reviewers, including further information about the study design, intervention, controls, location, measures, sample, and participant characteristics (e.g., information about ethnicity, social demographics, and co-occurring conditions). We additionally extracted the headline findings of each study, along with information about the size and direction of any observed effects. In cases where there were missing data, we contacted the authors to seek clarification. When sought information was not available upon request, it was recorded as missing on the data extraction forms and addressed as a potential limitation in the quality and risk-of-bias (ROB) assessments (see Methodological quality and ROB assessments section).
Methodological quality and ROB assessments
All included studies were independently assessed for quality and ROB by two reviewers in our team. Quantitative studies were assessed using the Cochrane ROB or Risk Of Bias in Non-Randomized Studies (ROBINS) tools, while qualitative studies were assessed using the EPPI-Centre tool for quality appraisal. Although differing in their specific evaluation criteria, each of these tools addresses the rigor of key methodological components, including sampling, data collection, analysis, and the reporting of study outcomes. For the ROB and ROBINS tools, studies were identified as having “low,” “high,” or “unclear” ROB within each assessment domain. Similar “low,” “medium,” or “high” criterion ratings were also assigned across the dimensions of the EPPI-Centre tool, although these evaluations were made in relation to each study’s reliability (i.e., the extent to which methods could minimize bias or error in results) and usefulness (i.e., the extent to which methods helped address the overall research questions). Upon completing appraisals independently, we compared evaluations and resolved any disagreements via discussion with an additional third reviewer.
Data synthesis
Evidence mapping and thematic analyses
Using the devised descriptor labels, we organized extracted data into an evidence map that detailed the different intervention methods and study design features within the identified research. Here, labeled categories were tabulated and general findings were extracted as free text into a pooled spreadsheet for qualitative synthesis. Free-text extractions focused on outcome data (e.g., quantitative assessments of user experience, context-dependent results) and process evidence (e.g., qualitative observations, statements about implementation). At this point, each cell of the evidence map was narratively synthesized to address the consistency, range, and quality of extracted study data. We particularly focused on identifying the types of interventions that have been used to support autistic people (Research Question #1), as well as the experiences of participants within studies (Research Question #3).
Informed by the evidence maps, we subsequently organized studies by intervention type and outcome for comprehensive evaluation of effectiveness. Here, a narrative synthesis approach was again undertaken, whereby the summary findings of each study were examined and compared, demonstrating the extent and range of outcomes for different support approaches. These synthesis procedures were undertaken in collaboration with our autistic research partners (see participatory synthesis). At this stage, information relating to the study population/context, intervention setting, and parallel cointerventions was considered, as well as the heterogeneity between and within studies. Analyses were intended to provide consensus around the efficacy of interventions in reducing autism-related driving challenges and barriers, and the different factors that potentially influence these outcomes (Research Question #2).
Thematic syntheses were undertaken to review implementation and process evidence. Here, we focused on the free-text qualitative and quantitative data in the evidence maps, with descriptive codes allocated to capture the content of each intervention. Coding procedures initially used the same terminology that was used in the original study reports but then regrouped and organized data to reflect suitable higher order themes. This process occurred iteratively over time and aimed to facilitate reciprocal translation across studies (in a manner that is not constrained by any broader assumptions or theories 19 ). Our resulting outputs provided a synthesized overview of how driving interventions are implemented (Research Question #4) and the contextual factors that may influence results (Research Question #5).
Intervention component analysis
Next, we sought to categorize the delivery components associated with effective interventions (Research Question #4). To do this, we applied intervention component analysis, 15 an inductive approach that groups features relating to the delivery of support from the evaluated studies. Here, a comprehensive list of descriptors was coded using NVivo (v.14; Lumivero, Denver, Colorado, USA), which was linked to the specific activities, actions, frequency, intensity, duration, personnel, and setting that characterized the driving interventions. This coding followed a two-step process. First, an exhaustive list of free-text descriptors was generated from five of the most recent and high-quality studies20–24 (which were deemed to be diverse in population and delivery characteristics). Thereafter, the remaining study interventions were examined and suitable descriptors subsequently collapsed or added as required. Output codes were axial and organized hierarchically, relevant to specific component (e.g., contact with support), subcomponent (e.g., support from instructor or friends/family), and within-component features (e.g., variability in contact duration) that emerged within the literature. Together, such analyses were designed to capture how an intervention is materially delivered, irrespective of the actual content or type of support that was implemented. This approach will provide a basis for future driving initiatives and could help ensure that support is delivered more effectively or efficiently in prospective research and applied practice.
Realist synthesis
Analyses sought to determine the mechanisms through which evaluated support interventions impact on autistic driving experiences and behaviors (Research Question #5). Here, data from the evidence mapping, thematic syntheses, and intervention component analysis were reexamined alongside broader evidence as part of a realist synthesis approach. 25 This approach focused on theoretically applicable causal processes that could underpin changes in driving outcomes and/or user experiences. Specifically, focal delivery components and contextual variables were extracted and used as a template for qualitative assessments. Thereafter, we inductively examined the relationships between contextual variables and mechanisms, and the processes through which these relationships may have generated different outcome patterns within and between studies. The degree to which possible causal processes were supported, refuted, or unevidenced by the extracted study data was determined iteratively and collaboratively, by both the review team and the participatory research partners.
Participatory synthesis
In addition to the public involvement activities that shaped the focus of this review (see the Research Design section above), we utilized a participatory synthesis approach within our analyses, following guidelines outlined by Fletcher-Watson et al 17 and in the Centre for Applied Autism Research “Blueprint for Autism Community Involvement in Research”. 26 Here, pertinent insight and lived experiences from five autistic adults (two males, two females, one nonbinary person; aged 26–55) were used to develop empirical findings and resolve uncertainties in the extracted study data. These individuals assumed the role of research partners on the project, as part of the “Evidence Synthesis Group for Autistic Drivers,” and helped coproduce the results and conclusions presented hereafter.
More specifically, the “Evidence Synthesis Group for Autistic Drivers” consisted of two UK-qualified drivers, one US-qualified driver, and two nondrivers, while including individuals with co-occurring conditions (ADHD, anxiety disorder). Once informed of the project aims and methods, this group engaged in a 90-minute workshop, where they were presented with an overview of extracted study data, including the types of support that have been studied, the content and delivery of interventions, and the “headline” results associated with each support method (e.g., the general effectiveness and range of different outcomes observed). Group discussions then sought to resolve uncertainties in these data and advance our understanding of the broader topic, using insight and lived experiences shared by the research partners. Following this activity, separate online consultations were completed on a one-to-one basis. These follow-up consultations served to cycle findings back and forth between partners, to ensure that all inputs were being captured sufficiently and accurately.
Results
Included studies
As illustrated in Figure 1, our searches of the literature identified 1216 unique citations after removal of duplicates, all of which were screened by title and abstract. Of those initially screened records, 1135 were excluded and 79 full-text articles were subsequently examined for eligibility. From full-text screening, 17 studies were deemed eligible for inclusion, with 44 excluded due to inappropriate interventions, 5 excluded due to inappropriate populations, and 13 excluded due to inappropriate study designs and/or reporting (see Supplementary Data S3 for a full list of excluded studies and their reasons for exclusion).
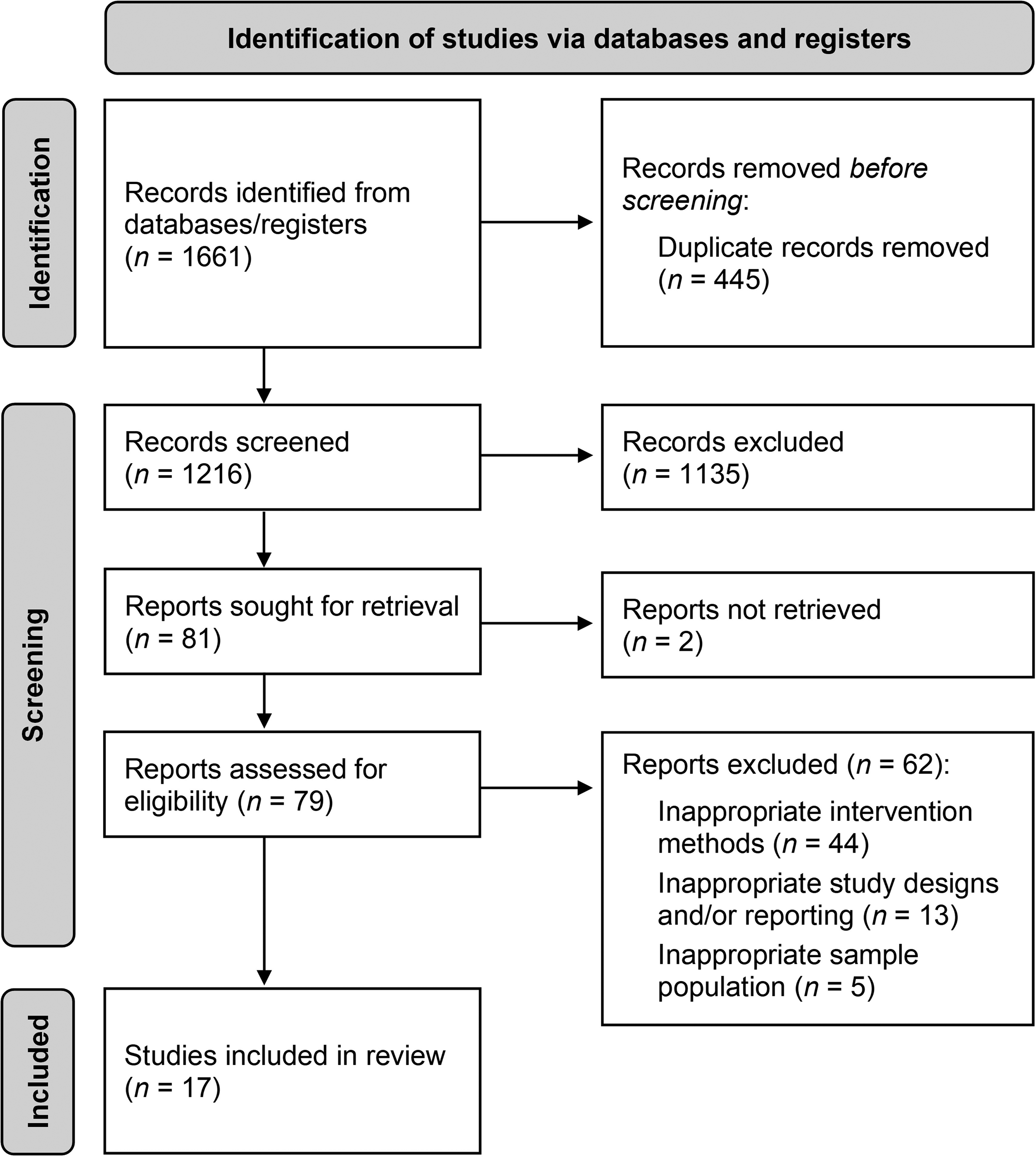
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) flow diagram of retrieved, screened, and included study articles.
On inspection of the 17 included studies, 16 represented early-stage assessments, consisting of pilot tests, formative and system-based assessments (e.g., of feasibility, technical performance, usability, acceptance), and randomized or quasiexperimental investigations (e.g., using case–control or pretest–posttest designs). One study 21 was classified as a late-stage assessment: a randomized controlled trial that was implemented over multiple sites in Australia. All other studies were conducted in the United States. A summary of the studies is provided in Supplementary Data S4, with further extracted data detailed in Supplementary Data S5. Sample populations were typically younger aged people (as young as 13 years) in the process of learning to drive. Nonetheless, there were also studies involving participants who were fully qualified drivers23,27–34 and others involving complete driving novices. 20 Few studies24,28,33–37 used diagnostic screening measures (e.g., the ADOS or semistructured interviews). Most participants were male (total: n = 334, total females: n = 66, total other: n = 2), with data relating to race/ethnicity, education, and socioeconomic status infrequently reported. One study 27 reported including people with ADHD, DCD, and Tourette syndrome in their analyses. Possible differences relating to these co-occurring conditions were not examined in the study though. Moreover, the remaining studies either excluded people with co-occurring conditions or did not report any specific data on these individual factors.
Most studies (15/17) performed quantitative analyses only, although there was one qualitative process evaluation 23 and one mixed-methods design. 22 Driving task performance was measured in 11 studies, although 10 of these examined participants during simulated conditions and only one used on-road assessments. 21 Other user-focused study outcomes included the following: license attainment rates, hazard perception, knowledge of theory, psychomotor skills, executive functions, tactical proficiency, gaze behavior, psycho-affective responses (e.g., engagement, enjoyment, satisfaction, anxiety, mental workload), perceived difficulty, usability, and attitudes toward driving. Implementation-focused outcomes included intervention fidelity, adherence, tolerability, and acceptance.
Methodological quality and ROB
A detailed summary of our quality appraisals is provided in Supplementary Data S6. Although appraisal outcomes were variable, overall quality ratings were notably low. For all studies that used randomized or quasiexperimental designs,21,24,28,31–35,37 concerns over performance or detection bias were highlighted, due to a lack of information regarding the blinding of personnel and/or outcome assessors. ROB relating to incomplete outcome data and selective reporting was generally low for these studies but concerns over other sources of bias were common (Supplementary Data S6.1). As such, overall ROB was generally deemed high in these cases. While the studies that used nonrandomized controlled designs were judged to have low 30 or moderate 29 overall ROB, the studies that did not have control groups20,27,36,38 were rated as poor or fair due to wide-ranging limitations. Similarly, the qualitative design studies were deemed low 22 or moderate 23 in reliability and usefulness, with potential biases relating to data collection and analysis identified and nonrepresentative samples used. In general, concerns over ROB mostly related to a lack of information provided in the study reports (e.g., over blinding procedures, participant eligibility criteria, and outcome measures).
Intervention characteristics
Details relating to each of the evaluated study interventions are provided in Table 1. These took place across a range of settings and timescales, and were generally provided by researchers, driving instructors, and/or clinical specialists (e.g., educational psychologists, occupational therapists). Usual practice control interventions were implemented in 7/17 studies,21,24,28–31,37 while 3 studies24,37,38 implemented their primary intervention alongside cointerventions (e.g., simulator practice, occupational therapy, or conventional on-road sessions).
Summary of the Study Interventions and Outcomes
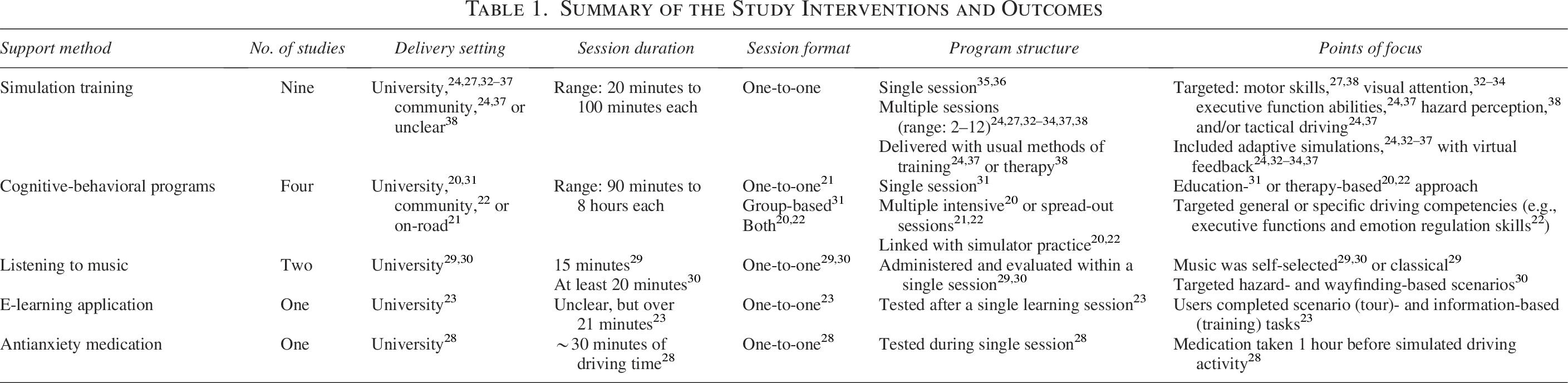
Simulation training represented the most well-researched form of support, being evaluated as a sole intervention in nine studies.24,27,32–38 Here, skills were practiced on virtual driving systems, which consisted of fixed-based platforms and 2D display screens. Practice sessions either occurred in university laboratories or occupational therapy settings and typically lasted 60 minutes or less (Table 1). The overall duration of study interventions varied: the shortest involved a single practice session,35,36 yet there were others involving repeated sessions over prolonged periods (from 3–6 days 33 up to 3 months37,38) The common rationale provided for these interventions was that they could enable skills and confidence to be developed in a safe, interactive learning environment. Seven studies24,32–37 examined novel adaptive simulation software, which provided automatic virtual feedback to users based on their task engagement, performance, and/or patterns of visual attention (Table 1). Control groups were only used in 6/9 studies: in these instances, researchers typically compared their novel simulation method with “routine” forms of training or simulation (e.g., learners might partake in their usual “on-road” lessons and have access to standard training manuals or logbooks).
The implementation of an e-learning application was examined in one study. 23 This application contained an information-based “training” and video-based “tour” section presented on a mobile tablet device. Learning content focused on attentional skills that autistic people can find challenging (although see concerns about restricting scope in Supplementary Data S2). While the duration of the intervention was unclear and appeared to vary on an individual basis, users completed at least seven 3–5-minute video scenarios in a single e-learning session held at a university. As the study centered on usability outcomes, no control intervention was examined.
Two studies explored whether listening to music could act as a strategy for promoting optimal sensory conditions and reducing autism-related driving challenges. Specifically, Goehmann 29 examined the effects of listening to classical or self-selected music during simulator-based driving scenarios, while Romer et al 30 provided participants with self-selected music only. The studies used experimental repeated-measures designs, and the strategic interventions took place in a controlled laboratory setting. Outcomes were compared with those from “no music” control conditions. Simulator activities were short in duration (Table 1), but varied in conditions (e.g., between rural and city roads, “hazard” and “wayfinding” tasks).
Fried et al 28 explored differences in driving behaviors following the uptake of anti-anxiety medication. Here, participants took 5 mg of buspirone an hour before undertaking a laboratory-based simulated driving exercise, where their performance and psychophysiological anxiety responses were recorded. Our participatory synthesis workshops highlighted significant concerns around the framing of this intervention as a wide-scale support method, due to potential adverse effects, nonfeasibility, and “over-medicalization” approach. It is also notable that this intervention was undertaken with qualified drivers only, and that the simulated task lasted only ∼30 minutes. The study used a repeated-measures crossover design, with intervention data compared versus unmedicated control conditions.
The remaining four studies evaluated cognitive-behavioral programs, which aimed to help autistic people via a collection of therapeutic and learning methods. Baker-Ericzen et al 22 studied the effects of a 10-week intervention that targeted executive functioning and emotional regulation skills in weekly 90-minute sessions. Dickerson et al 20 examined a more intensive driving and community mobility intervention, which used holistic occupational therapy and cognitive-behavioral learning activities (over five consecutive days). Smigiel 31 undertook a multifaceted education-focused intervention, providing classroom exercises that were adapted for learners with specific learning support needs. An adapted driver training program was also examined by Vindin et al, 21 where cognitive and behavioral skills were targeted through a combination of interactive online and on-road activities. These holistic support methods took place in a variety of naturalistic community- and classroom-based settings. Simulator practice was delivered alongside therapeutic activities in Baker-Ericzen et al 22 and Dickerson et al. 20 There were no control interventions in these studies, but conventional forms of driver training were used in Smigiel 31 and Vindin et al. 21
Effectiveness of interventions
Simulator training generally proved effective, with positive outcomes reported in 9/9 studies (Fig. 2). Evaluated interventions were found to improve simulator test performances,24,27,32–34,38 as well as hazard perception/responses, 38 executive functioning, and tactical driving skills 24 from pre- to post-training. Null performance effects were observed in Bian et al 35 and Wade et al’s 32 assessments of gaze-contingent training. However, this may be a result of short intervention durations and limited sample sizes, with positive effects demonstrated in subsequent studies by Wade et al33,34 (which involved a larger sample and longer intervention protocol). Changes in gaze behavior were nonsignificant or inconclusive in Wade et al 35 and in Baran’s34,38 hazard perception and response training intervention, although shifts toward more effective or “typical” behaviors were demonstrated in the former study 35 (and in Wade et al’s prior work 32 ). Analysis of parental reports suggested that participants were developing more positive attitudes to driving in Ross et al 37 (although see discussion of possible harmful attitudes: Supplementary Data S2). Multiple studies found simulation technologies to be feasible, reliable, and robust for future use24,33,36 and found that these systems could successfully capture autism-related driving challenges that exist in the real world.24,34 Moreover, the studies of adaptive simulation software24,32–36 showed that these systems prove functional in modifying task conditions based on user responses (e.g., in accordance with engagement, performance, attentional responses). No negative outcomes of simulator training were reported in any study, yet effectiveness data were notably lacking from on-road driving and real-world transfer tests.
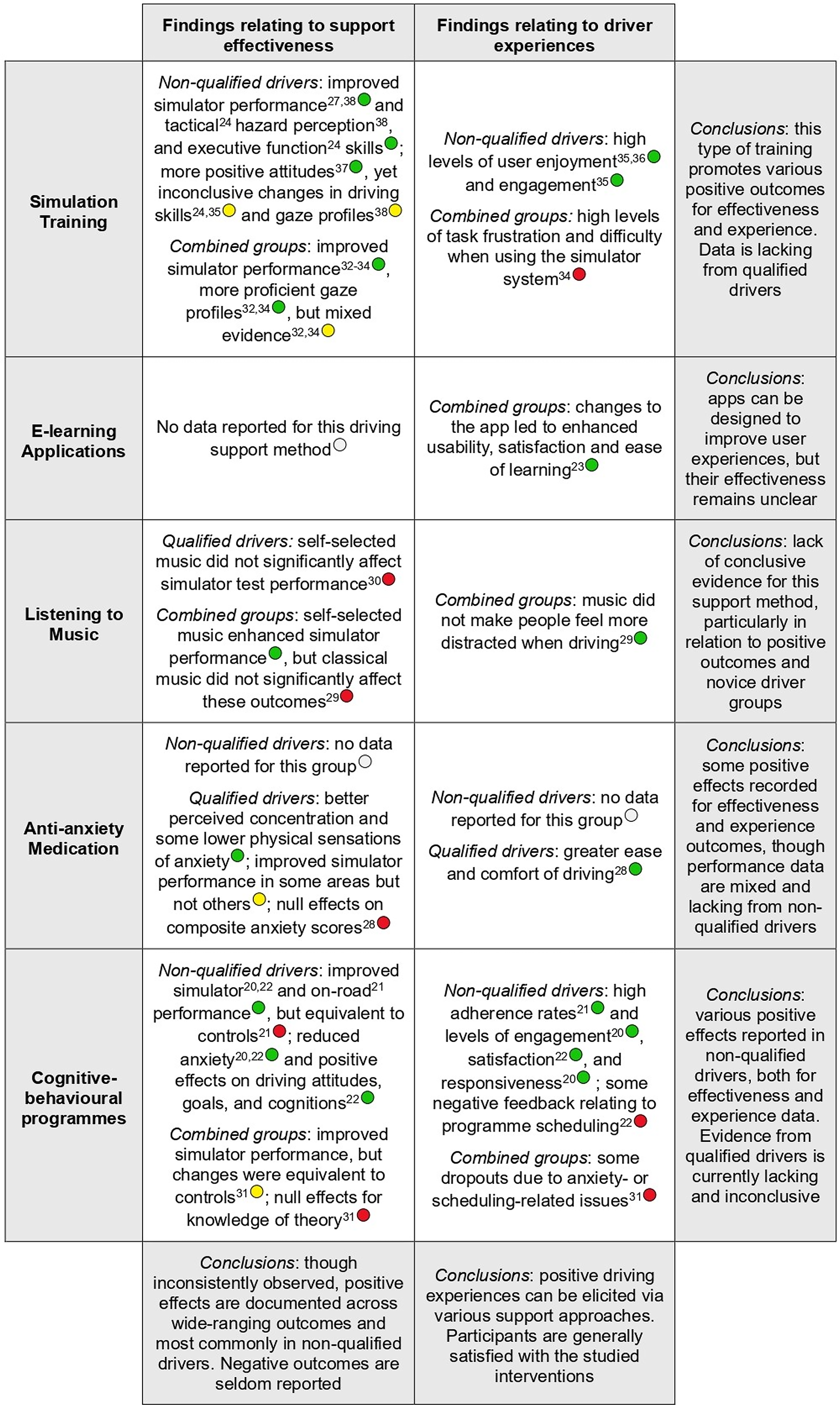
Summary of Findings Table (SoFT) for autism-focused driving support interventions. Green circles denote findings that support the efficacy of an intervention, while yellow circles highlight inconclusive evidence, and red circles signify null/undesired outcomes. Empty circles indicate that there is a lack of evidence within a given indication or population.
There was limited evidence found in support of listening to music as a method of reducing driving challenges. No differences in simulated driving performance were observed across studies between the intervention and control groups (Fig. 2), and while self-selected music appeared to show some positive performance effects in Goehmann, 29 these outcomes were not replicated in Romer et al 30 or in terms of objective error data (e.g., for lane-keeping, collisions, or speed violation variables). Negative effects were not recorded in either study.
Fried et al. 28 found positive effects for anti-anxiety medication, with the buspirone treatment group showing superior simulated driving performance compared with controls, as well as lower self-reported anxiety and better perceived concentration. However, significant performance enhancements were only observed for lane positioning metrics, and not for speed or variability of speed data. Moreover, reductions in anxiety related to selected physiological sensations, and not for psychological scale metrics or composite anxiety scores. While no negative outcomes were reported for driving or tolerability measures, participatory synthesis workshops highlighted various possible limitations that have not been investigated (e.g., in terms of perceived dependency or adverse effects: Supplementary Data S2).
Positive effects were demonstrated for the cognitive-behavioral interventions across a range of studies and outcomes. These included improved on-road driving, 21 enhanced simulator performance,20,22,31 reduced anxiety 20 (although see Baker-Ericzen et al 22 ), and more positive driving attitudes, goals, and cognitions. 22 The magnitude of improvements was generally equivalent to that of control groups.21,31 Nonetheless, Smigiel 31 noted that their intervention group showed lower variability in outcomes than controls, suggesting that their holistic support program produced more consistent results than conventional methods. While there was no control intervention in Baker-Ericzen et al, 22 this study reported that nearly half of the people undertaking their cognitive-behavioral intervention acquired a permit or license within 2 months of the program. That said, there is a lack of analysis into who specifically benefited (and did not benefit) from the support methods across studies.
Due to a focus on usability analyses, there were no data reported in Monahan et al 23 with regard to intervention effectiveness, so it is not yet possible to evaluate the efficacy of e-learning applications as a support method for autistic people.
Driver experiences
While outcomes relating to driver experiences were less prominent than performance- or efficacy-related outcomes in the reviewed literature, some participant data were still reported (Fig. 2). The majority of these data were determined from quantitative measures, although qualitative user experience data were analyzed in two studies.22,23 Satisfaction scores were the most frequently assessed outcome, although acceptance, tolerability, workload, engagement, and adverse effects (e.g., drowsiness, simulator sickness) were also examined.
Simulation-based methods were found to provide generally positive experiences for users in terms of enjoyment and engagement (Fig. 2). However, Wade et al 34 indicated that these outcomes remained lower for autistic people than non-autistic people and that autistic participants concurrently reported higher task difficulty and frustration. Adaptive simulation functions typically enhanced aspects of user experiences through the means in which they were designed: for example, by increasing engagement (via data-driven adjustments in task difficulty 35 ) or providing more in-depth feedback (via eye tracking analyses 24 ).
Monahan et al 23 primarily focused on user experience outcomes for their e-learning application study. Various positive and negative aspects were detailed, ranging from broad usability (e.g., how people generally found using the tool) to specific design-related issues (e.g., the choice of certain words or phrases in text). The iterative nature of the study meant that negative experiences could be progressively reduced through making changes to the content and implementation of the application. As a result, enhanced usability, satisfaction, and ease of learning were demonstrated over time.
User experiences were not formally examined during the music-based studies. Although researchers speculated that the familiarity and likeability of self-selected music caused participants to relax, 29 there were no direct data to support these claims. Romer et al 30 indicated an absence of negative experiences in those who typically avoid noisy environments. Yet these effects were anecdotal and uncertain, and may not reflect all personal experiences.
Similarly, no negative user experiences were reported in Fried et al’s 28 study of anti-anxiety medication. In fact, buspirone treatment led to lower adverse effects during simulated driving (indexed via the Simulator Sickness Questionnaire), particularly in relation to “difficulty focusing” and “general discomfort.” Moreover, participants reported greater ease of driving during medicated conditions. Nonetheless, the potential for chronic adverse effects and the absence of data from novice drivers must be recognized.
Mixed findings emerged for the cognitive-behavioral interventions. Positive results were reported for acceptance and satisfaction data in Baker-Ericzen et al, 22 and for user engagement and responsiveness outcomes in Dickerson et al. 20 However, negative experiences relating to the structure and scheduling of sessions were reported for these programs (Fig. 2), which were the sole reason for dropout reported in Smigiel. 31 While such issues may relate to delivery components, user experiences could be inequitably limited within these multifaceted interventions, regardless of how they are implemented. For example, the intensive nature of cognitive-behavioral programs may prevent anxious individuals from enrolling in or initially attending activities, as observed by Smigiel. 31
Delivery components
Many of the support interventions that differed in content and methodology were characterized by common delivery components, as outlined in Table 2. For example, both simulation- and cognitive-behavioral interventions were implemented using a formal curriculum,21,22,24,31 with dedicated familiarization activities,23,28–30,34–36,38 informational materials (e.g., training manuals or workbooks),20–22,31,37 and/or preparatory instructional content (e.g., step-by-step guides or video tutorials).21,33–36 The importance of providing these dedicated accompanying resources was emphasized in participatory synthesis workshops, although the possibility of “overloading” people with excessive information was identified as a risk. Our autistic research partners also supported the provision of additional guidance that was not driving-specific (e.g., support or advice for other practical and community mobility skills), in accordance with interventions in Baker-Ericzen et al, 22 Baran, 38 and Dickerson et al. 20
Summary of the Focal Delivery Components
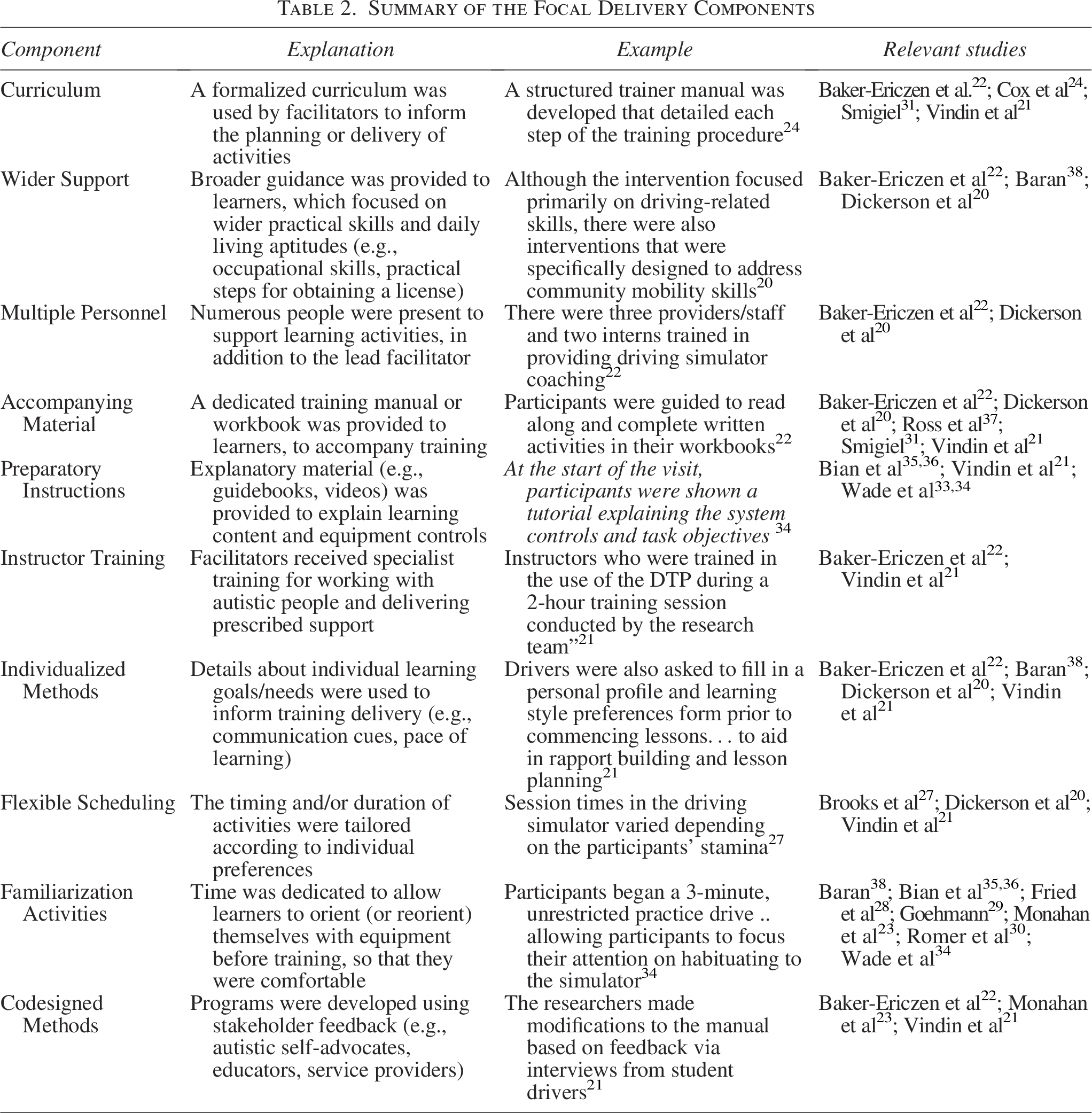
In addition, multiple interventions implemented aspects of codesign to inform and adjust how support was provided.21–23 Baker-Ericzen et al 22 and Dickerson et al 20 used multiple facilitators to deliver learning content, in addition to the lead instructors, although participatory workshops emphasized potential negative impacts on user experiences (e.g., access to support could be limited if it depends on several instructors/facilitators being available at once). Personalized aspects of delivery were broadly supported, whereby the implementation of content is tailored on an individual basis (across multiple studies21–23).
Finally, the provision of guidance or training for those facilitating driver support programs was identified as a focal delivery component within Baker-Ericzen et al 22 and Vindin et al. 21 Here, specialist educational content was given to individuals who were providing study interventions (e.g., driving instructors, simulator operators), to better prepare them for delivering autism-focused driving support. Participatory synthesis workshops indicated that this approach could be an effective component of wide-ranging support programs, but that possible negative, unintended consequences could also arise (Supplementary Data S2).
Mechanisms of action
A summary table of intervention mechanisms is presented in Supplementary Data S7, yet studies provided very limited insight in this regard. Only five studies20,21,24,27,34 directly tested whether intervention effects were predicted or moderated by other outcomes, and these mostly focused on driving history or demographic data (e.g., experience, baseline performance). Instead, our inferences are largely drawn from proposed context–outcome relationships (i.e., arguments laid out in article discussion sections). Participatory synthesis workshops highlighted a lack of investigation into individual and contextual factors that could impact on how interventions “work.” In fact, many of the studies implemented eligibility criteria that prevented investigation of these factors; for example, by excluding those with co-occurring conditions (e.g., DCD, ADHD) and/or high levels of certain autistic-like traits or difficulties.
Several studies considered the impact of reducing anxiety through targeted driving support and the contextual factors that could affect individual outcomes. Although only three studies measured anxiety directly,20,21,28 significant reductions were reported in all three cases (Fig. 2), while seven articles made theoretical links between positive outcomes and dampened anxiety responses.20,22,27–29,37,38 Our autistic research partners lent further support for these conclusions, particularly within simulator training and cognitive-behavioral support interventions (Supplementary Data S2). However, Vindin et al 21 found that anxiety did not moderate driving performance in their correlation analyses, and relationships between anxiety- and driving-related outcomes are likely to be contingent on wider variables, such as a person’s previous experience 29 or surrounding road conditions.
In support of attentional mechanisms, more proficient visual scanning responses and perceived concentration abilities were recorded.28,32,34 However, outcomes were inconsistent for attention-focused support methods, such as gaze adaptive simulation training (Table 1). From a more behavioral perspective, positive outcomes have been attributed to a process of increasing engagement and changing attitudes (Supplementary Data S7). Generally, high levels of engagement have been highlighted in training-based methods, where positive impacts on learning and long-term skill development are proposed.20,35,36 Similarly, the fostering of positive driving attitudes was highlighted as a means of improving competencies and gaining successful license outcomes within both simulation-based and cognitive-behavioral interventions.22,37 In these skill development programs, it is likely that mechanism–outcome associations are moderated by learning-related variables, including factors linked to training exposure and delivery (as well as adverse or unintended effects).
Discussion
This review examined the implementation and effectiveness of driving support interventions for autistic people. Despite our comprehensive evaluation, analyses underline the general lack of research on this topic, 39 which aligns with a perceived lack of support expressed by autistic people and their instructors.11–13 Nonetheless, we identified a small but diverse collection of evaluated support methods, including simulation training, cognitive-behavioral interventions, e-learning applications, listening to music, and anti-anxiety medication. Studies generally reported positive results for these methods, although evidence remains in its infancy. Consistent improvements were shown for simulation training and cognitive-behavioral approaches across measures of driving performance, attitudes, tactical skills, hazard perception, executive functions, and anxiety. Other methods demonstrated mixed or limited effects and must be considered with caution alongside possible risks (e.g., relating to how safe, ethical, or scalable they are). These considerations must not be overlooked, since the challenges faced by autistic people often relate to societal barriers or negative experiences, rather than due to any proven differences in driving safety or performance. Despite this, there has been little examination of how support methods impact on experiences of driving. Indeed, while high levels of enjoyment, engagement, satisfaction, and ease of learning were reported, negative experiences may persist and some of the key barriers or adverse effects that accompany conventional driving activities could remain present (e.g., accessibility issues, autism-related stigma).
Unfortunately, the mechanisms through which effective support interventions “work” in this field, and the individual and contextual factors that influence these processes, also remain under-researched. Reductions in anxiety and enhancements in attentional control, engagement, and driving attitudes could provide a target for future programs, based on positive emerging findings. Moreover, from a delivery component perspective, our analyses identified that effective support programs often followed a personalized approach and provided additional material alongside the core constituents of an intervention (e.g., training workbooks, practical guidance, onboarding tutorials). Notably, these interventions were generally delivered or guided by facilitators with specialist backgrounds or lived experiences. For instance, some programs included dedicated training for instructors21,22 and codesign activities.21–23 That said, benefits are not guaranteed through these approaches, and unintended outcomes may still be produced (see Supplementary Data S2). Thus, until further empirical progress is made, we recommend that methods of best practice from wider applied autism research and implementation frameworks are incorporated in the development of future driving support interventions (e.g., from education and digital support sectors40–42).
Crucially, much of the inconclusive findings in this review can be attributed to lack of high-quality evidence. The majority of included studies represented early-stage assessments with moderate or high ROB, suggesting that general claims of providing “initial efficacy” or “proof of concept” must be taken with caution. Several studies did not include a control group, and those that did often provided vague details about any control intervention conditions. Moreover, there was a general lack of on-road assessment data, with measures largely being obtained from simulated driving activities. The degree to which simulation-based test outcomes capture meaningful “real-world” benefits in this space therefore remains uncertain, and there is even potential for negative transfer effects to occur (e.g., due to nonrepresentative driving attitudes, skills, or strategies being picked up; see relevant framework 43 ). Relatedly, many of the study samples cannot be regarded as representative of general autistic populations either, due to low numbers of female participants, insufficient reporting of demographic data (e.g., for race/ethnicity, socioeconomic status), and the exclusion of selected groups (e.g., autistic people with higher levels of behavioral traits and difficulties or with co-occurring conditions, such as DCD and ADHD). Indeed, little attention was paid to individual differences or equity-relevant characteristics, despite various study outcomes and indicators having been shown to vary with even basic demographic variables (e.g., age and gender can predict real-world driving behaviors44,45 and the uptake of digital simulation interventions 46 ). Taken together, these limitations create a weak, uncertain evidence base for support providers to work from, which compounds the general lack of studies in the field.
Review limitations
First, to broaden the review across diverse scientific and international contexts, our study selection and search methods were aligned to wide-ranging conceptions and scientific classifications of autism. Although no clinical or deficit-based criteria were operationally used, retrieved studies were often framed within a medical model of disability and their data may be limited by this perspective. An example, here, is that included studies only involved participants with a formal diagnosis of autism, yet many autistic people will not hold a diagnosis when facing driving-related challenges due to delays and inequity associated with diagnostic services.47,48 Hence, future research should incorporate more contemporary methodologies and evaluative approaches (e.g., based on the neurodiversity paradigm), to better challenge deficit-based conceptions and promote more inclusive scientific impacts. Furthermore, our analysis of support “effectiveness” was generally restricted to performance-based outcomes, yet broader practical and economic impacts could be equally significant for autistic people. For instance, while a training intervention might well improve driving skills and confidence, its labor-intensive requirements could conceivably make learning more expensive and inefficient. Similarly, prevalent barriers relating to license procurement and assessment processes7,49 could remain in place. Moving forward, we therefore recommend that research seeks to address systemic, noninclusive elements of driving programs and policies alongside the design of any new support methods and initiatives.
Conclusions
This review provides a comprehensive overview and evaluation of existing driving support for autistic people. For the most part, our findings highlight widespread limitations in the current evidence base, due to low-quality research methods, insufficient and nonrepresentative data, scarce consideration of contextual/individual factors, and a general lack of studies available. Given the clear driving barriers and challenges faced by autistic people, we can conclude that further research is urgently required. Simultaneously, however, our review also highlights promising avenues and approaches for future work. For instance, there is emerging support for the use of simulation training and holistic cognitive-behavioral programs, as well as for interventions targeting reductions in anxiety. Furthermore, we have identified numerous delivery components that may be characteristic of effective support methods, which could be readily incorporated within future programs.
Authorship Confirmation Statement
T.A.: Conceptualization, methodology, data curation, formal analysis, project administration, visualization, and writing (original draft). D.H.: Conceptualization, formal analysis, and writing (review and editing). S.R.: Methodology, formal analysis, and writing (review and editing). M.B.: Conceptualization, resources, supervision, and writing (review and editing). S.V.: Conceptualization, supervision, and writing (review and editing). G.B.: Conceptualization, supervision, and writing (review and editing). E.S.: Conceptualization and writing (review and editing). M.W.: Supervision and writing (review and editing). M.O.-M.: Conceptualization, formal analysis, and writing (review and editing). ESGFAD: Conceptualization and formal analysis. G.J.M.-T.: Conceptualization, formal analysis, methodology, supervision, and writing (review and editing). The article has been submitted solely to Autism in Adulthood.
Data Sharing Statement
All relevant data and supplementary materials associated with this article are available on this page.
Footnotes
Acknowledgments
The authors thank all the research partners who contributed toward their participatory activities and undertakings on this project. In particular, they express their gratitude to those who attended the public involvement workshops at the Centre for Applied Autism Research, who valuably informed their review focus and broader research objectives.
Author Disclosure Statement
The authors have no competing interests to declare that are relevant to the content of this article.
Funding Information
T.A. is the recipient of an ESRC New Investigator award (grant number:
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.