
Abstract
Background:
While there is growing interest in the relationship between social media (SM) use and psychosocial well-being, little is known about this relationship in neurodivergent people. We undertook a systematic review to synthesize findings from studies exploring links between social (dis)connectedness and SM use in Autistic people and/or people with attention-deficit/hyperactivity disorder (ADHD), with the aim of exploring commonalities and differences in their experiences.
Methods:
We conducted systematic searches of four databases, retaining reports if they included SM-related measures and measures of social connectedness and/or disconnectedness in Autistic and/or ADHD populations. Two of us independently screened, coded, and assessed all records for methodological quality, with another of us screening just under 15% of records.
Results:
Our search yielded findings from 21 reports based on data from 18 studies. A narrative synthesis we undertook suggested that SM may be linked to greater social connectedness for Autistic people and greater social disconnectedness for those with ADHD. The literature was characterized by a predominance of cross-sectional research and the quality assessment highlighted measurement issues.
Conclusion:
Our findings suggest that SM may differentially support and hinder social connectedness for Autistic and ADHD SM user groups, respectively, although we discuss potential challenges to this conclusion, including potential biases in the way studies are framed and key constructs are operationalized across the different literatures. Our review highlights the need for further longitudinal and experimental research to establish underlying directions of causality and the robustness of our findings.
Community Brief
Why is this an important issue?
Social media (SM) use is becoming nearly ubiquitous, and there is growing concern that this may be linked to increases in mental health difficulties. Despite this, existing research suggests a range of potential benefits as well as harms, including the potential for SM to both enhance social connection and replicate offline experiences of disconnection. Such opportunities and risks may be particularly relevant to neurodivergent people, who experience high levels of stigma and discrimination.
What is the purpose of the review?
Our purpose in undertaking this review was to synthesize existing research into links between SM use and social connectedness and disconnectedness in Autistic people and people with ADHD. We were particularly interested in commonalities and differences in their experiences. Ultimately, we hope that the findings will inform future research and potentially shape the development of guidelines, tools, interventions, and/or supports to help neurodivergent people to flourish online.
What did the authors do to review the literature?
We conducted a systematic review to synthesize existing quantitative research that explored SM, social connectedness, and/or disconnectedness in Autistic and/or ADHD people. We ran searches of four key databases to identify articles focusing on these three areas, and synthesized the findings. We also used tools to assess the quality of the studies included.
What studies did the authors find?
We found 21 reports based on 18 studies that met our criteria.
In summary, what did those studies show?
The studies reviewed highlighted links between SM use and increased social connectedness for Autistic users, and between SM use and increased social disconnectedness for ADHD users. We also found that there was little consensus on how SM and connectedness/disconnectedness should be measured, and many of the measures used were not of the highest quality.
What are the remaining gaps in the literature?
Most of the studies reviewed included data from a single time point only, so that it could not be determined whether SM use impacts connectedness, or experiences of connectedness drive patterns of SM use. There was also a greater focus on potential harms in the ADHD literature, so that it is unclear whether the different findings we found for Autistic and ADHD SM users reflect differences in their actual experiences, or differences in the way that the research is approached.
Based on this review, what do the authors recommend?
From a research perspective, future research should use longitudinal and experimental designs to determine the underlying direction of causality. In addition, research should disentangle genuine differences in the online experiences of Autistic and ADHD people, from different methods used, which may be driven by researchers’ prior assumptions. Finally, research should explore how the design of SM platforms shapes users’ experiences. From a clinical perspective, we hope that this research will encourage mental health professionals to consider neurodivergent people’s online lives alongside their offline lives, particularly as a potential source of connectedness and/or disconnectedness.
Introduction
Research suggests that, at the population level, higher levels of social media (SM) a use are (on average) associated with poorer well-being.1,2 However, this nomothetic “dose–response” approach, which collapses the rich and diverse ways people use SM to time spent online, is highly reductive 3 and ignores interindividual differences in susceptibility to both the risks and benefits of engagement. 4 In response, there has been a move toward more contextualist understandings of SM use, which consider how individual, technological, and broader social-contextual factors interact to impact on mental health and well-being.3,5
Since social connectedness is closely related to mental health, 6 and SM is inherently social, this may be a crucial factor in understanding SM and well-being links. Social connectedness—the experience of acceptance and belonging to social networks and relationships 7 —has been linked to better mental health as well as reduced loneliness and mortality.8,9 SM offers opportunities for both social connection through opportunities to interact with others,10,11 and social disconnection, for example, through cybervictimization and online exclusion.10,12,13
The Interpersonal-Connections-Behavior-Framework (ICBF) 14 proposes that SM may be of benefit or harm to the well-being of the user to the extent that it supports satisfaction of core needs for acceptance and belonging, that is, the extent to which it increases or decreases social connectedness. Tibber and Silver’s 5 transdiagnostic cognitive behavioral conceptualization of SM use extends this notion, linking social motivations and social approach behaviors to a greater likelihood of satisfying such needs, and escapist/avoidant motivations and behaviors to a decreased likelihood of their satisfaction, with resulting implications for mental health.5,15 These frameworks guide both outcome selection and interpretation of findings in this review, offering a lens through which to understand the relational and motivational aspects of SM use.
A small but growing body of evidence supports the ICBF.6,16 For example, cross-sectional research has linked escapist motivations and avoidant online coping approaches to poorer well-being. 17 In contrast, evidence suggests that when users engage with SM to cultivate meaningful connections, greater positive well-being and reduced loneliness may follow.18,19 Despite this growing acknowledgment that social connectedness and disconnectedness are critical to the putative harms and benefits of SM, little is known about interindividual differences that may be linked to risk and resilience in this regard.4,20,21 One emerging area of study in this regard is neurodivergence, particularly autism and attention-deficit/hyperactivity disorder (ADHD). However, related literature has often adopted a reductive lens based on notions of disorder and dysregulation, which tends to assume that difficulties arise from within-person deficits, obscuring the role of context, relationships, and systemic factors. 22
Relative to neurotypical people, Autistic b people and those with ADHD are exposed to more negative offline social experiences, including bullying,23,24 stigma, and lack of acceptance.25–27 These are linked to negative mental health outcomes, including anxiety, depression, and addiction.28,29 While many of these experiences risk being replicated online, SM may provide an alternative context for some neurodivergent people to connect, cultivate belonging, and affirm their identity/identities.30–32 For example, a qualitative study of Autistic adults reported that participants’ key motivations for SM use were maintaining relationships and gaining new social contacts. 33 However, Autistic SM users may also experience threats to social connectedness.34,35 For example, a cross-sectional study of Autistic SM users found that higher levels of engagement were associated with increased risk of cyberbullying and correlated negatively with self-esteem due to feelings of being ignored. 36
For ADHD SM users, the extant research is sparser still, and perhaps even more than in autism, heavily dominated by problem-saturated and deficit-focused narratives. Thus, the primary focus is on putative links between ADHD traits and problematic/addictive SM engagement.37–39 Nonetheless, some evidence supports an association between SM use and social connectedness for ADHD people also. 40 For example, a qualitative study with ADHD adults found positive aspects of online communities, including connecting with similar others and identity-affirmation. 32 However, participants also reported fears of rejection and experiences of not fitting in online, and other research has highlighted elevated risks of cyber victimization among ADHD SM users. 41
Overall, the existing literature suggests a potential for SM to harness social connectedness for Autistic and ADHD individuals, and also to mirror (and potentially even amplify) negative offline social experiences. Both have equally important implications for understanding (and potentially supporting) mental health.5,14 In this context, we systematically reviewed empirical, quantitative studies exploring links between social connectedness/disconnectedness and SM for Autistic and/or ADHD users, focusing on commonalities and differences in these literatures and the online experiences of Autistic and ADHD people. Due to the relative novelty of the area, the following broad research questions guided our review: what is the relationship between SM use and social connectedness/disconnectedness in (i) autism and (ii) ADHD and what, if anything, is (iii) common, and (iv) different across autism and ADHD in terms of these relationships?
We focused on autism and ADHD, specifically, for two main reasons. First, research shows that Autistic people and people with ADHD experience high levels of loneliness and marked inequalities across areas of health, education, and employment, as well as access to services, with sometimes lethal consequences. 42 Second, it would be unwieldy to include every neurodivergent group within the remit of a single review. Instead, by focusing on Autistic and ADHD people, for whom there is currently the strongest and most coherent bodies of literature relevant to our research questions, we aimed to conduct a focused and interpretable analysis that remained grounded in existing empirical work. Furthermore, two of us as members of the research team specialize in autism and ADHD research and have family as well as personal/lived experience of autism and ADHD, ensuring that we could undertake the review rigorously, accurately, and sensitive to the nuances of these populations.
Methods
Protocol registration
We registered the study protocol with PROSPERO (registration number: CRD42024591737). We undertook and reported methods and results in line with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines 43 ; see Supplementary Data S1 for the associated checklist.
Eligibility criteria
We deemed studies suitable for inclusion if they met the following criteria: (i) written in English; (ii) original quantitative study; (iii) published in peer-reviewed journals; (iv) included a measure of social connectedness and/or disconnectedness; (v) included diagnosed or self-identifying Autistic and/or ADHD people (or parents/caregivers reporting on their child’s experience); and (vi) included a measure related to SM.
With respect to our definition and operationalization of SM, informed by the concept of Web 2.0—the second generation of the worldwide web 44 —we conceptualized SM broadly as any app or platform that enables interactive, participatory communication and collaboration among users, who both create and share content in real time, including (for example) social network sites (SNS) and content communities. As such, we did not include studies exclusively focused on text messaging and emailing. We also intentionally excluded studies of gaming, since our core interest was on the extent to which SM is (potentially) socially connecting. Thus, while gaming can support social ties, 45 it is often solitary, 46 or occurs offline.
With respect to a measure of SM, we adopted a broad interpretation to include measures of any SM-related process or phenomenon linked to a user. This could include measures of general SM engagement, for example, time spent on SM, SM-related psychological constructs, for example, motivation to engage with SM, or SM-mediated behaviors or experiences, for example, SM-mediated social comparisons, as well as any measure that implied a form of engagement consistent with the affordances of a Web 2.0 application (i.e., even in the absence of explicit reference to SM per se). Studies could also be included if there was an explicit comparison of SM users and non-SM users.
We also adopted a broad conceptualization of social connectedness, aligned with Lee and Robbins’ 7 definition as relating to the experience of being part of a relationship, group, community, or network and linking to an individual’s sense of belonging and acceptance. 7 This could include constructs such as social capital, social support, number of friends, and relationship quality. We conceptualized social disconnectedness as any negative experiences of social relationships, such as social isolation, rejection, or loneliness. 47
Finally, with respect to both SM and social (dis)connection measures, we placed no restrictions on measurement quality or design; measures could be validated or unvalidated, custom-written or well-established, including single- or multi-item measures, or even measures with subscales or items relevant to the construct. Thus, as noted, our emphasis was on coverage, preferring quality to be captured at the quality appraisal rather than the screening stage.
Information sources
We ran searches on the following four databases: MEDLINE (Ovid), PsycINFO (Ovid), Embase (Ovid), and Web of Science (Core Collection). We initially ran the search on September 17, 2024, with databases searched since 1997, when the first SM site—Six Degrees—was released, and reran it with a date filter from the original search date to November 7, 2025, to bring it up to date following initial review of the article.
Search
Search terms were based on the following three key concepts: (1) social connectedness/disconnectedness, (2) autism/ADHD, and (3) SM, combined using the AND operator. In line with a focus on coverage and broad definitions (described above), we derived a broad array of synonyms for these terms—as well as allied concepts—from relevant literature, including key theoretical articles and reviews, major diagnostic classification systems, and general language use (see Supplementary Data S2). We mapped terms to subject headings in Ovid platforms (MEDLINE, PsycINFO, and Embase) to facilitate a comprehensive search.
Screening
We screened records in two stages. In stage 1, we screened titles and abstracts of all studies retrieved for the inclusion of the three key concepts; in stage 2, we reviewed full articles to exclude those not meeting the inclusion criteria. A.L.P. and A.O.L. independently screened 100% of records at both stages. E.I. independently screened a random sample of 15% of the records that were retrieved in the first search (before the final search was rerun) at both stages. Thus, two of us screened 100% of the records, and three of us screened just under 15%. Inter-rater agreement, assessed using Cohen’s Kappa, was 0.85 and 0.95 for A.L.P./A.O.L. at stages 1 and 2, respectively, and 0.98 and 0.96 for A.L.P./E.I. We resolved any disagreements through discussion. Finally, A.L.P. conducted forward and backward citation searches for all the included articles.
Data collection
A.L.P. and M.S.T. developed a data capture form that included the following items (and independently coded the data): date of data collection; the country study was conducted in; sample size; sample population; summary participant demographics, including age, gender, and ethnicity; method of data collection; sampling strategy; study design; participant group (Autistic, ADHD, both); formal or self-identified nature of diagnosis; details of respondent (self-report, parent/caregiver, both); any other neurodevelopmental differences and/or mental health difficulties reported; type of SM(s) examined; measure(s) of SM included; measure(s) of social (dis)connectedness included; type and level of analyses undertaken; any subanalyses included; other variables/covariates modeled; and key findings and associated significance. In addition, the form included items relating to an assessment of study quality and risk of bias (see the following section).
Quality appraisal and risk of bias
We assessed included studies using the Standard Quality Assessment Criteria for Evaluating Primary Research Papers. 48 This tool was developed to assess a variety of study designs using 14 criteria (example items: “study design evident and appropriate?” and “controlled for confounding?”), with items assigned a score of 0 to 2 to capture the extent to which they met the criteria (2 = yes, 1 = partial, 0 = no, NA = not applicable). We calculated summary scores (indicating the overall quality) for each article. We included three additional custom-written criteria to assess study quality more rigorously: (i) presence of measures of effect size for main outcomes (yes/no); (ii) whether outcomes were assessed using valid and reliable measures of social connectedness/disconnectedness (yes/no); and (iii) whether outcomes were assessed using valid and reliable measures of SM (yes/no), scored separately from the above. See Supplementary Data S3.
Where data were missing from a study, we made a request for this information to the authors. A.L.P. and A.O.L. independently screened all the articles for quality assessment. We resolved any disagreements through discussion.
Synthesis of results
Given the level of heterogeneity in operationalization of constructs, methodology, and analytic approaches that we expected in the target literature, we deemed a narrative synthesis more appropriate than a meta-analysis. 49 A.L.P. independently interpreted the data and produced the narrative synthesis under discussion and guidance of M.S.T.
Results
Study selection
Our original and updated search yielded a combined total of 12,730 initial records. After removal of duplicates (n = 5284), we screened titles and abstracts of 7446 records and completed full-text screening of 485 reports. No further reports were identified when we undertook forward and backward citation searches. Our updated search retrieved two additional eligible studies, which were included in the final review. We identified 21 reports of studies for inclusion. However, three reports50–52 were derived from a single dataset, and a further two from another single dataset,53,54 such that a total of 21 reports included were based on 18 studies. Figure 1 presents the PRISMA flow diagram of this process. 43
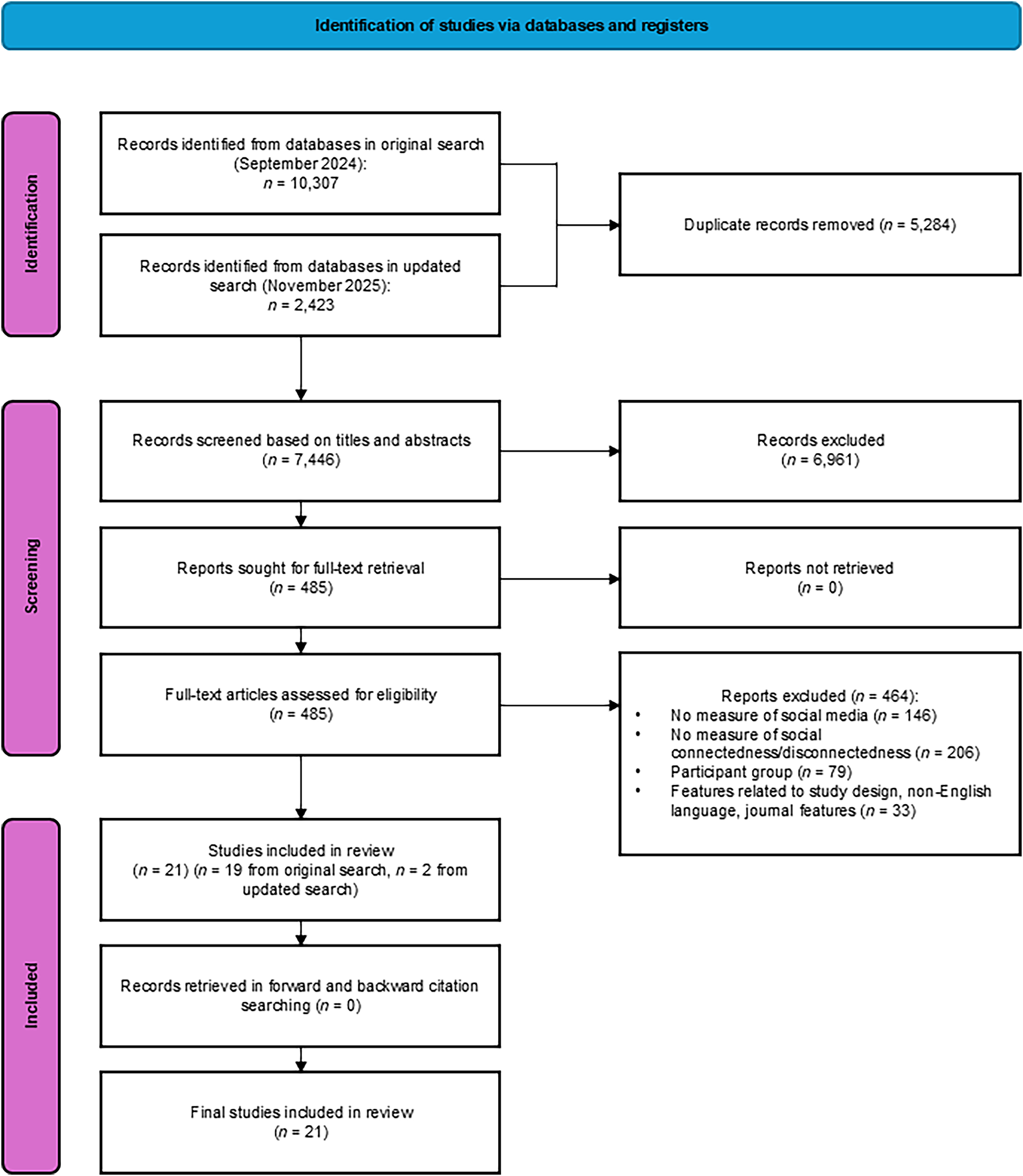
The PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram outlining the search process.
Study characteristics
Table 1 provides the extracted study characteristics and main findings for each report included (n = 21); see Supplementary Data S4 also. All 18 studies c were published between 2013 and 2025, reflecting the relatively recent development and uptake of SM. Data were collected in the United States (n = 8, 44.44%), Canada (n = 3, 16.67%), Taiwan (n = 2, 11.11%), and Turkey (n = 3, 16.67%), with single studies from the Netherlands and Israel.
Study Characteristics and Main Findings from the Included Articles

Three reports based on a single study (Wright, 2017 50 ; Wright, 2018 51 ; Wright & Wachs, 2019 52 ); two reports based on a single study (Halkett and Hinshaw, 2024; Mikami et al., 2015).53,54
n = 21 reports based on 18 studies.
CD, conduct disorder; CI, confidence interval; CMC, computer-mediated communication; ODD, oppositional defiant disorder; SIEC, social integration and emotional connectedness; SM, social media; SNS, social networking site.
Data collection methods included online surveys (n = 6, 30%), in-person surveys (n = 10, 50%), direct analysis of Facebook profiles (n = 2, 10%), and interviews (n = 2, 10%). The sampling strategies included convenience (n = 7, 38.89%), volunteer (n = 9, 50%), random selection (n = 1, 5.56%), and multiple stratified sampling (n = 1, 5.56%). The most common design d was cross-sectional (n = 17, 80.95%). Three had longitudinal designs (14.29%) and one had a retrospective cohort study design (4.76%).
Participant characteristics
Nine e studies (50%) focused on Autistic people, and ninee on ADHD (50%). Of the autism studies, two (22.22%) indicated that a portion of participants had co-occurring ADHD,56,62 with a mean reported co-occurrence of 39.5% (SD = 12.02). Of the nine ADHD studies, five excluded participants who were Autistic (55.56%), and one indicated that a portion (14.3%) of the participants were also Autistic. 70 Eleven studies (61.11%) included neurotypical participants (with data analyzed separately in all cases).
The 18 studies included a combined sample of 18,641 participants. Sample sizes ranged from 23 to 15,240 (M = 1035.61, SD = 3548.92; Mdn = 126). For Autistic participants, samples ranged from 23 to 664 (M = 105.67, SD = 81.06); for ADHD, 65 to 664 (M = 182.56, SD = 190.86).
Participant ages ranged from 6 to 84, with an overall mean of 18.27 f (SD = 8.91; 15 studies) and a mean of 15.01 (SD = 1.95) for ADHD participants and 21.79 (SD = 11.36) for Autistic participants. Outside of studies that focused exclusively on male or female participants, the majority included a higher proportion of males (vs. females) for both autism (7 of 9, 77.78%) and ADHD (6 of 6, 100%) studies. Only two studies (11.11%) reported participants who identified as a gender identity other than male/female. Ten of the 18 studies (55.56%) did not report information regarding ethnicity; for those that did, all eight (100%) reported “White/Caucasian” participants as the largest ethnic group.
Measurement characteristics
With respect to operationalization of SM, 11 studies used established measures (52.38%) g , and 10 (47.62%) created custom-written or adapted existing ones. With respect to operationalization of social (dis)connectedness, 14 studies (66.67%) used established and validated measures and seven (33.33%) used custom or adapted versions of existing questionnaires. The most commonly used measures were variants of the UCLA Loneliness Scale 71 (n = 5, 23.81%). Two studies (9.52%) used the Multidimensional Scale of Perceived Social Support. 72 No other scales were repeated across studies.
Assessment of quality
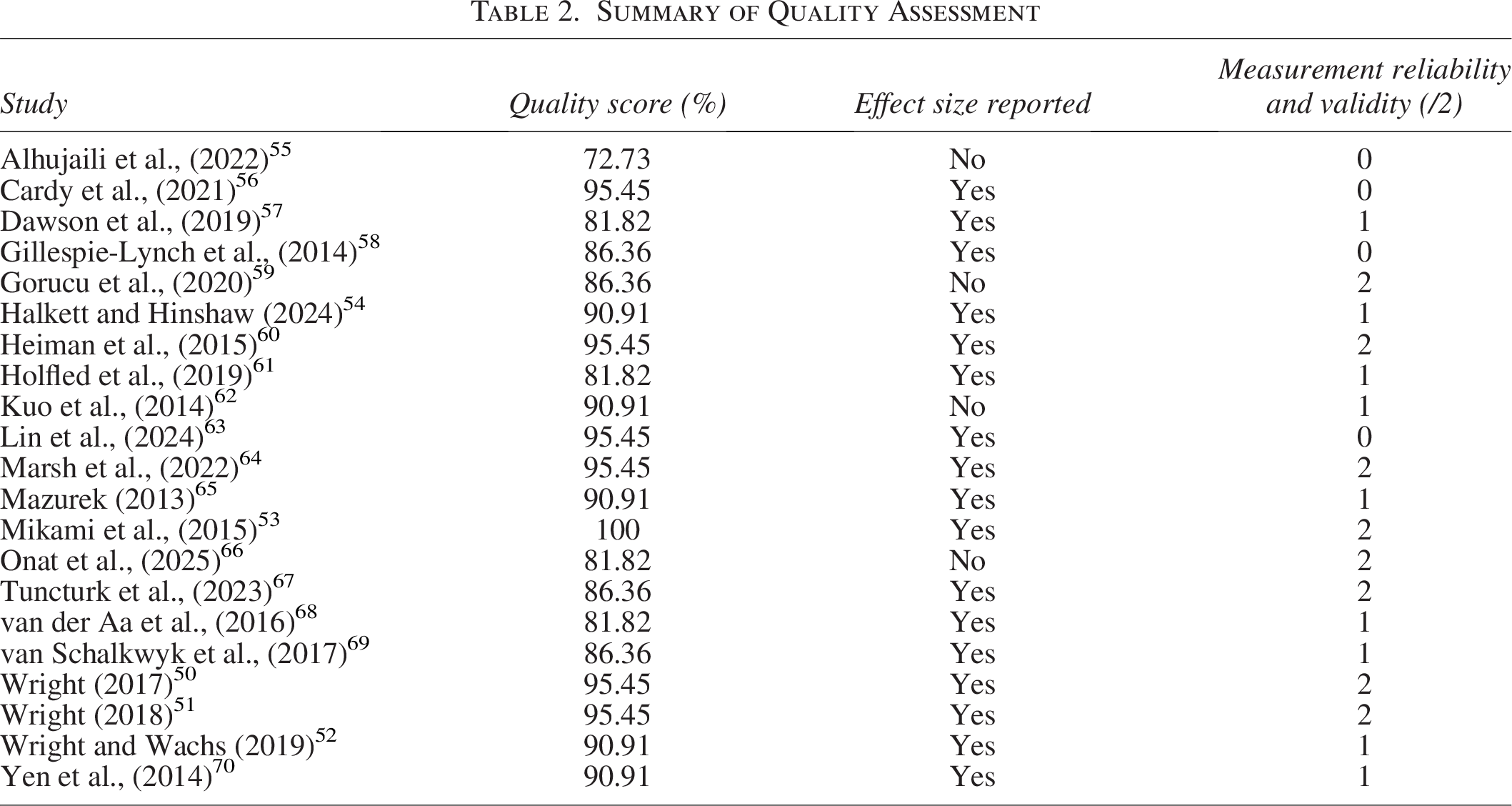
The quality scores for the included articles ranged from 72.73% to 100% (see Table 2). h We most frequently identified methodological limitations related to the method of participant selection (n = 8, 38.10%), a lack of well-defined measures (n = 11, 52.38%), an inadequate sample size (n = 6, 28.57%), and not controlling for potential confounds (n = 14, 66.67%). In terms of the extra custom-written quality items, we again identified issues around construct operationalization and measurement, with several studies using invalid or unreliable measures of social (dis)connectedness (n = 7; 33.33%) and/or SM (n = 10; 47.62%). We also noted limitations with respect to reporting, with a minority of studies (n = 4; 15.79%) not reporting a measure of effect size for main outcomes. See Supplementary Data S3.
Summary of Quality Assessment
Narrative synthesis
Findings from studies focusing on Autistic people
Of the 11 studies that examined SM use in Autistic people, seven explored associations between general SM use, SNS i use, or computer-mediated communication (CMC), j and social connectedness in Autistic people, and overall, highlighted a potential positive link in both adolescents and adults. Further, there was some evidence to suggest that these effects might be specific to—or at least more pronounced in—Autistic people, that is, relative to non-autistic people.
Thus, Autistic adolescents who used SNS reported greater security in their friendships than those who did not use SNS 62 ; furthermore, parents’ ratings of their adolescent child’s SM use were correlated with better friendship quality, 69 although this was only the case for a subset of Autistic adolescents who reported low levels of anxiety, and was not seen in Autistic adolescents high in anxiety, nor in non-autistic adolescents. Similarly, in Autistic adults, those who used SNS were twice as likely to report having a best friend than those who did not use the technology, 65 and Autistic adults reported having made more acquaintances online and appreciating CMC more than non-autistic adults. 68 Autistic adults also reported benefits from CMC such as making and maintaining contact with similar others, 58 a finding that was more pronounced than in non-autistic adults. In contrast, one study failed to find a significant correlation between SM use and perceived social support in Autistic adolescents, 61 and another found that during the COVID-19 pandemic, Autistic children lost significantly more time in offline social interactions as a consequence of their increased screen time than non-autistic children. 56 The latter study was based on parent reports, however.
The remaining three autism studies explored cyberbullying and highlighted a potentially protective role of social connection against associated harms. Thus, in a series of three reports based on a single study, Wright and colleagues found that a relationship between cybervictimization and depression in Autistic adolescents was weakened in the context of high levels of (parental) social support 50 and low levels of peer rejection, 52 and further persisted in longitudinal analyses at the one-year follow-up. 51
Finally, one study met our inclusion criteria as it incorporated measures with items relating to SM use and social connectedness but did not test associations between the two constructs. 55 Nonetheless, it is worthy of note that while non-autistic participants were found to use SM primarily for social purposes, Autistic users cited entertainment as their primary motivation.
Findings from studies focusing on people with ADHD
With respect to ADHD, two studies highlighted associations between SM use and negative online social experiences and experiences of disconnection, which further may be specific to—or at least more pronounced in—ADHD relative to non-ADHD SM users. Thus, one study comparing (emerging adult) female ADHD and non-ADHD Facebook users found that a childhood ADHD diagnosis predicted fewer Facebook friends as well as less closeness and support from Facebook friends’ posts (relative to non-ADHD Facebook users). 53 This was the case despite ADHD participants preferring online communication (relative to face-to-face) more than non-ADHD participants did, an effect that was mediated by offline peer difficulties. Relatedly, another study found that Facebook users with ADHD received a disproportionately high number of aggressive posts, and people with ADHD themselves made fewer supportive posts toward their online friends than was reciprocated. 57
Four studies explored cyberbullying in ADHD. Findings were mixed and complex, highlighting links between ADHD, loneliness, and cyberbullying, which may be elevated relative to non-ADHD people, as well as a potentially protective role of social support, although the latter was not seen across all the studies. Thus, in one study, both victims and witnesses of cyberbullying who were ADHD reported higher levels of loneliness and lower levels of social self-efficacy compared with non-ADHD participants in these groups 60 ; the authors also reported that being ADHD, experiences of cybervictimization, and lower levels of social support were all associated with loneliness. In another study that explored cyberbullying in adolescents, while no differences were seen for individuals who had experienced and/or perpetrated cyberbullying, among those with no such history, those with ADHD (relative to those without) reported higher levels of loneliness and a greater preference for online (over offline) interactions. 59
In a study of adolescents with and without ADHD, which included self-report and parent-report data, adolescents with ADHD reported more experiences of cybervictimization than non-ADHD adolescents. 64 Furthermore, a positive association was seen between experiences of being cyberbullied and internalizing symptoms (anxiety and depression), which was only present in adolescents who reported a strong connection to SM communication and online friendships. 64 Conversely, for those who had not experienced being cyberbullied, a greater connection to SM was associated with lower levels of anxiety (parent-report data only).
With respect to the potentially protective effects of social connectedness, one study found that satisfaction with peer relationships was not associated with the likelihood of perpetrating cyberbullying or being cyberbullied in male ADHD adolescents over the previous year. 70 This pattern did not change when co-occurring diagnosis of autism was added as a covariate. Another found that offline social support (positive atmosphere at school and greater family monitoring) was associated with lower risks of cybervictimization. 63 The latter effect did not interact with ADHD status and was also seen in offline bullying.
Finally, three studies explored problematic technology use. Higher levels of SM addiction and loneliness were reported in ADHD relative to non-ADHD participants, and a positive association was seen between these two constructs in ADHD participants. 66 In a longitudinal study of ‘problematic social internet use’ in ADHD and non-ADHD female children, girls with ADHD diagnoses at baseline reported a greater overall preference for online socializing, were more likely to use the internet to talk to people they met/only knew online, and to form close online relationships with people they had met online than those without a diagnosis. 54 Furthermore, inattentive (but not hyperactive/impulsive) ADHD traits were associated with greater problematic social internet use in baseline cross-sectional analyses. Finally, in a study that compared ADHD participants with problematic internet use to ADHD participants with internet gaming disorder, higher levels of loneliness were seen in the latter. 67
Discussion
We systematically reviewed empirical research exploring links between social (dis)connectedness and SM in Autistic people and in people with ADHD, focusing on commonalities and differences across these groups. Both literatures highlighted mixed findings and a complex and nuanced relationship between SM use and social (dis)connectedness. While we found limited evidence to infer causality, the findings are consistent with patterns observed in general population samples, in which SM use is associated with both higher and lower social connectedness, depending on the context. 16
With respect to positive links between SM and connectedness, the most robust finding we identified was that high levels of social connectedness seemed to have a protective effect against the harmful consequences of cyberbullying (assuming causality). However, this effect was not specific to one group but seemed to be present in Autistic,50–52 ADHD, 63 and neurotypical participants. 63
Aside from this shared finding, the existing literature more often reported SM use in association with increased social connectedness for Autistic participants and indicators of disconnection for ADHD participants. Thus, in Autistic participants, SM was linked to the making and maintaining of social connections,58,68 having a best friend, 65 greater friendship security, 62 and friendship quality, 69 with findings spread across studies of adolescents and adults. In fact, the only “negative” association between SM use and social connection seen in Autistic individuals related to parental reports of screen time displacing more face-to-face interactions for their child. 56 However, this presumes that parental reporting is reliable, and further, that displacement of face-to-face interaction is inherently problematic, which is not a given in the context of a large-scale shift to on-screen connection during the pandemic, 73 and the potential benefits of SM-mediated connection for Autistic people reviewed above, and elsewhere.35,74
With respect to the potential risks of disconnectedness in ADHD, the literature reviewed suggested that relative to non-ADHD SM users, people with ADHD were exposed to confrontational or unsupportive SM interactions more often,53,57 reported more pronounced impacts of cyberbullying, 60 and greater levels of loneliness,59,60,66 although it is unclear whether this reflects preexisting offline dynamics, platform-specific cultures, or ADHD-related traits. Despite this, there was some evidence to suggest that some ADHD SM users may prefer online (to offline) interactions 54 ; interestingly, however, this may reflect attempts to navigate offline conflict. 53 This is significant given the existing literature that has linked compensatory/escapist/avoidant motivations for SM use to more problematic patterns of engagement and negative outcomes.75,76 On the contrary, such preferences may also reflect adaptive strategies for managing offline dynamics, highlighting the need for future research to explore the conditions under which online interactions support resilience, well-being, and authentic connection.
These findings are broadly consistent with existing systematic reviews linking SM to increased social connection for Autistic people,35,74 while recognizing that it may not fully alleviate loneliness or replace in-person relationships. 35 Similarly, they echo a narrative review of problematic SM use in ADHD adolescents, 38 suggesting that while ADHD adolescents may seek online connectedness to compensate for offline peer challenges, they (often) encounter similar challenges online.
We can speculate as to why we found differences between Autistic and ADHD SM users’ experiences. For some Autistic people, features of SM may align with social communication preferences described in the literature. 77 Delays in communication allow more time to process information before responding, fewer nonverbal cues may reduce the risk of overwhelm during social interactions, 78 and social metrics such as “likes” and “shares” may reduce ambiguity.35,77,79 Online platforms may also foster connections around shared interests.80,81 As a result, it has been proposed that (some) Autistic SM users have the potential to gain more online. 35 On the flipside, certain features of SM communication (e.g., emojis, GIFs, hashtags, and unclear online social norms) may bring challenges to some Autistic users.81,82 Furthermore, in the context of challenges to ADHD SM users highlighted by this review, it is important to note that ADHD is more common in Autistic people than in non-autistic people. 83
In contrast, the features of the online world may be experienced as more challenging by ADHD users. Features designed to maximize attentional capture, 5 including notifications and “pop-up” advertisements, may increase distractibility and associated feelings of overwhelm,32,38,84 given that features of ADHD include differences in sensitivity to environmental stimuli and attentional control. Indeed, such affordances have been highlighted as potential barriers to online socializing by young adult ADHD SM users 32 ; thus, platform architectures optimized for rapid responses and constant engagement may interact with attentional and regulatory differences, increasing the likelihood of negative online experiences. 38 The well-known “online disinhibition effect” 85 as well as the potential for SM to “over-stimulate” ADHD users may also play a role.
Methodological issues may also explain some of the differences seen in the literature reviewed. For example, ADHD participants studied were typically younger (M = 15.01) than Autistic participants (M = 21.79). Thus, Orben and colleagues (2022) 86 highlighted windows of developmental sensitivity to negative effects of SM, with adolescents (14–15 for males, 11–13 for females) being particularly vulnerable. ADHD participants (which tended to be biased toward male samples) more clearly fell into this sensitive window, possibly inflating associations between SM use and negative well-being indicators compared with Autistic participants.
Differences in findings between Autistic and ADHD literature reviewed may also stem from lenses and assumptions brought to the research. In general, the studies of Autistic SM users that we reviewed tended to frame the research question and operationalize key constructs in terms of the potential for social connectedness; in contrast, the studies of ADHD SM users more often explored “threats” to social connectedness and “problematic” patterns of SM use, potentially pre-disposing the research toward certain findings. Therefore, it is unclear whether differences in framing reflect the actual differences in underlying tendencies between these two groups, which drive researchers’ and clinicians’ perspectives, or whether they reflect a priori assumptions and prejudices about autism and ADHD, which—in turn—drive research agendas.
Such negative framings are often reductive and risk overlooking how online and offline environments, platform design, and cultural norms shape users’ experiences. They also replicate deficit-based assumptions that have historically characterized both ADHD and autism research. The result is (in this case) a tendency to locate the cause of disconnection within the neurodivergent person, rather than in the interaction between the person and the structures, biases, and affordances of the environment. Without attending to these dynamics, research risks perpetuating the very marginalization it seeks to understand.
Finally, with respect to interpreting commonalities and differences between Autistic and ADHD people’s experiences, it is important to note both the high degree of co-occurrence of autism and ADHD, 83 and the variety of approaches taken in included studies to address this (or not). Thus, while some studied identified/screened and excluded people with co-occurring neurodevelopmental differences, others identified/screened and included them, and some simply did not explore such co-occurrences, likely introducing variability into the findings. However, given the relative paucity of extant literature, it is not feasible to undertake a more fine-grained analysis of findings comparing (for example) studies of Autistic, ADHD, and Autistic/ADHD populations.
Quality of reviewed literature
We identified several limitations in the literature that impact the generalizability and validity of the findings. Recruitment methods commonly used often introduce biases: online recruitment may skew toward certain genders, socioeconomic status, and motivations for engagement. 87 Recruitment from clinics risks reinforcing existing biases in access to services, with respect to socioeconomic status, gender, and ethnicity.88–90 Age and gender—shown to covary with SM use and well-being91–93—were frequently not controlled for.
Many studies also used poorly validated measures of SM and social (dis)connectedness. This speaks to wider criticisms of SM research in relation to poorly operationalized constructs and validated measures.94,95 The cross-sectional design predominated, precluding conclusions about underlying causality or directions thereof. In most studies it could not be determined if differences in SM use led to differences in social (dis)connectedness, or instead, differences in social (dis)connectedness led to differences in patterns of SM use. Furthermore, the literature often applied normative definitions of well-being despite potentially differing experiences and expressions of well-being for many Autistic and ADHD individuals. 96
The paucity of non-White, educated, industrialized, rich, and democratic samples 97 in the included studies reviewed was notable and risks reinforcing existing disparities in research and access to relevant resources and services.88–90 Relatedly, echoing wider patterns in the literature, the research reviewed did not include nonspeaking neurodivergent individuals.
Limitations of the review
As noted, our review focused solely on neurodivergent people who were Autistic and/or ADHD. While this enabled a more focused and clearly defined review of the literature, it did mean that some neurodivergent people’s experiences were overlooked. However, Autistic and ADHD people often experience multiple co-occurring experiences (e.g., dyslexia and obsessive-compulsive disorder), such that even by limiting the remit of the research to these areas, broader neurodivergent experiences will have been included to some degree. Nonetheless, future work should broaden this focus to encompass a broader range of neurodivergent people’s experiences.
Second, we excluded studies exclusively focused on gaming, since although games can be used socially, they can (and often are) used offline and/or in solitary; that is, the technology is not implicitly social in nature. Nonetheless, this exclusion may have limited the insights, particularly for neurodivergent communities who may find meaningful connection through online gaming communities. 98
Third, while we aimed to explore commonalities and differences in the experiences of Autistic and ADHD SM users, autism and ADHD commonly co-occur. 99 No included study compared both groups directly, and many did not screen for or ask about co-occurring neurodevelopmental differences (e.g., autism traits in ADHD samples, or vice versa), making it difficult to determine whether observed differences reflect genuine group differences or methodological variability (as noted). However, this (arguably) reflects a limitation of the existing literature rather than the review.
Fourth, by excluding gray literature and non-English language publications, we may have introduced biases, including an overrepresentation of positive findings. 100 As peer-reviewed journals may be subject to time lags, 100 including gray literature may have enriched our understanding, particularly given the rapidly evolving SM landscape.
While we considered a mixed-methods synthesis at the design phase, we ultimately decided to focus solely on quantitative studies. This was because we wanted to examine measurable associations between SM use and social (dis)connectedness to enable a more direct comparison between the two sets of literature (autism and ADHD), coupled with the fact that methodological frameworks and synthesis approaches for qualitative and quantitative research differ substantially. Nonetheless, we value qualitative research for deepening the understanding of lived experiences and suggest future mixed-methods or qualitative syntheses to complement our work.
Finally, while our research team includes one Autistic and one ADHD member, we acknowledge the limitations in our own positionality, particularly regarding racial intersectionality, which may have influenced the perspectives represented.
Implications
Given the (near) ubiquity of SM and the (potentially) increased uptake in neurodivergent populations, 101 it is crucial that we understand its nuanced impacts. From a research perspective, we think that the findings highlight social connectedness and disconnectedness as key constructs in understanding links between SM and mental health in Autistic and ADHD people. Future research should use longitudinal and/or experimental methodologies to explore underlying directions of causality and elucidate the precise role of social connectedness/disconnectedness in established SM/mental health links. Valid, reliable measures of SM engagement and associated constructs, and clear conceptual frameworks 95 are needed to facilitate comparison across studies and populations.
Clinically, our findings reinforce previous calls made to consider people’s online lives in mental health services, both in terms of potential benefits to capitalize upon and risks to manage. 5 This review expands upon this call, extending its proposed relevance to neurodivergent people, for whom the risks and benefits of engagement may both be amplified, particularly in the context of elevated risks of stigma, social exclusion, and threats to belonging.23,24,26,27
Finally, our findings suggest that SM’s capacity to connect and disconnect should be considered with respect to assessing individual vulnerabilities and protective factors, and further emphasize processes that may be of particular relevance when considering the well-being of Autistic and ADHD SM users, for example, potential benefits of social connection and potential risks of impulsive engagement, respectively. However, these dynamics cannot be located solely within the individual but reflect—and are embedded within—broader systemic and interpersonal processes.25,102–104 More research must hear directly from neurodivergent people themselves, to ensure interpretations reflect lived experience rather than outsider assumptions. 105 Such an approach is critical if education and digital practices are to be explicitly neurodiversity-respectful, and attentional differences and varied communication styles recognized, supported, and valued, rather than pathologized.
Conclusions
Our review is consistent with a complex and nuanced role for SM in the mental health and well-being of neurodivergent SM users. Our findings highlight a potential for SM use to support the cultivation of social connectedness in Autistic SM users, and drive social disconnectedness in SM users with ADHD. However, these findings should be interpreted with caution, particularly in the context of a predominance of cross-sectional research, dominant disorder-based narratives in the study of ADHD in particular, and several methodological and conceptual issues that may have driven (or contributed to) differences in the two literatures reviewed. We hope that our findings and recommendations will inform future research, and ultimately contribute to the development and coproduction of guidelines, supports, and/or interventions that will support neurodivergent people to flourish online.
Authorship Confirmation Statement
A.L.P.: Conceptualization, methodology, formal analysis, investigation, and writing—original draft. M.S.T.: Conceptualization, methodology, validation, writing—review and editing, and supervision. A.O.L.: Validation. E.I.: Validation. G.P.: Writing—review and editing. K.R.: Writing—review and editing.
Footnotes
Author Disclosure Statement
The authors have no known conflicts of interest to disclose.
Funding Information
No funding was received for this article.
Supplemental Material
Supplemental Material
Supplemental Material
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.