
Abstract
Background:
There is a general belief in the scientific community that autistic people have emotion recognition (ER) difficulties. Despite this, the research is inconclusive, with roughly half of the studies showing that autistic people have similar ER ability to non-autistic people. The alexithymia hypothesis posits that ER differences found in some autistic individuals might be due to concurrent alexithymia, with some incipient research backing this claim. One limitation of past literature is the focus on facial expressions, with ER from body language remaining understudied, especially in relation to autism and alexithymia.
Methods:
Adults (N = 364) completed a face and body ER task containing video expressions of all basic emotions, during which we measured their accuracy, confidence, and intensity ratings. Participants also completed Alexithymia (PAQ) and autism traits (AQ-10) questionnaires. After data cleaning, we split participants into an autistic group (n = 71) and non-autistic group (n = 279). We used alexithymia scores to further split the two autism groups into high and low alexithymia categories. We investigated the effects of autism and alexithymia on body and face ER accuracy (unbiased hit rates), confidence ratings, and intensity ratings.
Results:
Autistic individuals had slightly lower accuracy and confidence than non-autistic individuals. When alexithymia was modeled with autism, autistic people were no different than non-autistic people on accuracy and confidence. Alexithymia was a better predictor of confidence than autism and interacted with modality. Bodies were harder to recognize than faces, but we found no interaction between modality and autism or alexithymia. Our results did not find differences in intensity ratings.
Conclusion:
Alexithymia may account for differences in ER accuracy and confidence between autistic and non-autistic people. Our findings support the alexithymia hypothesis of autism. This is the first study comparing facial and bodily ER in autistic and non-autistic people and in low- and high-alexithymia-score individuals.
Community Brief
What was the purpose of this study?
Autistic people are often seen by the scientific community as having impairments in social abilities. When it comes to recognizing emotions, scientists believe that autistic people are worse. However, only half of the studies done so far found autistic people to be less accurate at recognizing emotions. The beliefs of the scientific community, especially when not entirely true, can be damaging to autistic people’s self-worth and the way other people treat them.
Why is this an important issue?
We tried to see if another trait, alexithymia, explains the mixed findings in emotion recognition (ER) studies with autistic people. Alexithymia is a personality trait, not a diagnosis. Alexithymic people describe themselves as having difficulties identifying their feelings, describing their feelings, and focus more on external happenings instead of internal experiences. We wanted to see if alexithymia explains ER difficulties that some people experience, instead of autism.
What did the researchers do?
We tested 364 people using an online test to see how accurate and confident they are in recognizing anger, disgust, fear, joy, sadness, and surprise. We also asked them to rate how intense they thought the emotion expressions were. They also completed alexithymia and autism self-report questionnaires. After cleaning the data, we split the people into two groups: autistic (71) and non-autistic (279). We compared the two groups on how they recognize emotions, how confident they are in their abilities, and how intense they perceive the emotions to be.
What were the results and conclusions of the study?
It seemed like autistic people did not have reduced ER accuracy and confidence when taking alexithymia into account, regardless of whether they looked at emotions expressed in the face or the body. In other words, alexithymia explained ER differences in autism. Alexithymia was a better predictor of confidence in ER than autism.
What is new or controversial about these findings?
This is the first study comparing facial and bodily ER in autistic people, showing that autistic people are not better or worse at body expression recognition. It also supports the alexithymia hypothesis of autism, which says that ER difficulties are due to alexithymia, not autism.
What are potential weaknesses in the study?
This study could not gender balance the autism groups, with more males and non-binary people in the autistic sample. In addition, most of the people in the study were young adults; more research needs to be conducted on older adults and children.
How will these findings help autistic adults now or in the future?
First, these findings cast doubt on the idea that autism is associated with ER problems, contrary to stereotypes that may harm autistic people. Second, it could inform non-verbal communication support practices, calling attention more toward alexithymic individuals. It points toward the existence of a high alexithymia subgroup on the autistic spectrum, a group of people that might benefit from understanding alexithymia better and from additional non-verbal communication support.
Background
There is a general axiomatic acceptance in psychological sciences that autistic people have “impaired” (facial) emotion recognition (ER) ability, with an entire subfield of research dedicated to measuring and teaching emotion recognition to autistic children and adults.1–3 Despite this, most papers published in the past couple of decades tend to describe mixed findings. A systematic review of behavioral and neuroimaging research found that behavioral studies are marginally more likely to find lower facial ER ability in autistic people than no differences at all. 4 A more recent meta-analysis of 146 facial ER studies found reduced ER ability in autistic people (children and adults) when compared with non-autistic people. 5 Despite the overall effect, 47% of the studies included in the meta-analysis did not demonstrate a significant difference in ER. A similar proportion of studies finding no difference arises from ER studies involving the recognition of non-verbal vocal expressions (see Day et al., 2023, for a review of the vocal ER literature). 6 Harms et al. 4 commented that, despite the mixed findings in behavioral studies, neuroimaging and electrophysiology studies consistently find that autistic people perceive and process emotion differently. It is likely that certain task characteristics and individual differences are responsible for the mixed findings in behavioral studies.4,5 In the present study, we aimed to investigate both some lesser known task characteristics, including a relatively novel type of emotion recognition, as well as a personality trait that is associated with autism and ER.
The personality trait that has been the subject of much debate in recent years is alexithymia. The most common definition of alexithymia describes it as a subclinical trait characterized by difficulties in identifying feelings, difficulties in describing feelings, and externally oriented cognitive style, 7 with some definitions including poor imagination/fantasizing ability. 8 Theoretical accounts of alexithymia rely on a link between understanding one’s own emotions in order to understand others’ emotional expressions, suggesting that alexithymia may lead to impaired understanding of others’ emotions.9,10 Indeed, most initial studies found negative associations between ER ability and alexithymia in both clinical and non-clinical samples (10 out of 12 studies). 11 More recently, alexithymia co-occurring with reduced ER ability has been uncovered in a variety of conditions, such as personality disorders, 12 eating disorders, 13 alcohol misuse, 14 or craniofacial pain. 15 In most of these studies, alexithymia accounted for, or mediated, the negative relationships between ER ability and degree of condition. Alexithymia is estimated to be present in 50% of the autistic population, in comparison to just 5% of the non-autistic population. 16 This comparatively high prevalence within the autistic population has resulted in some researchers proposing that those with both conditions may reflect a subset of the autistic population16,17 and may explain some of the emotional difficulties in identifying and describing feelings reported by some autistic individuals. 18 While a number of studies demonstrate the association of ER and empathic differences to alexithymia rather than autism per se,19,21,24,25,30 others suggest a more complex picture: In some instances, alexithymia is associated with emotion processing differences only in co-occurrence with autism,22,23 and others find relationships between ER and autism, rather than alexithymia, although these may be task-specific or emotion-specific. 26 These mixed findings necessitate further investigation in the autism-ER dyad, using more up-to-date methodology in both ER and alexithymia measurement.
Beyond faces27–29 and voices, 30 recognition of expressions in bodies is the least studied ER field, with less than 5% of ER studies conducted by 2009 using some form of body expression stimuli. 31 Evidence suggests that body expressions of emotion (with no facial information) can be recognized in both static and dynamic stimuli and in both point-light displays 32 and full-light displays.33,34 The body expression paradigm opens a new angle of research on ER in autism. Multiple studies have noted that autistic people, in contrast to non-autistic people, process non-verbal expressions differently. More specifically, autistic individuals tend to look less at the eyes-nose-mouth area, 35 especially the eyes, 36 than non-autistic individuals and focus more on bodies and contextual cues, especially in dynamic stimuli.37,38 One facial ER study found lower ER recognition accuracy for autistic adolescents, but not when the eyes in the stimuli were digitally covered. 39 More pertinent to the alexithymia hypothesis of autism, studies have found that differential gaze patterns are predicted by co-occurring alexithymia in both autistic and non-autistic individuals.40,41 Although many of these findings are about emotion perception, not recognition, they raise questions about facial ER in contrast to bodily ER: Are emotional body movements more useful for autistic and/or alexithymic people’s recognition processes than facial ones? The autism and body ER literature suffers from similar mixed findings as the facial ER literature, with perhaps more variability of results. Some studies found no differences in body ER ability,42–44 while others found overall reduced accuracy for autistic people,45–47 or reduced accuracy only for some specific emotions.48–50 One recent study reported slower response times on dynamic stimuli, but no accuracy differences on static or dynamic point-light displays and full-light displays. 51 There are many problems and gaps to address in this subfield. First, most of the studies reviewed above looked at the bodily ER ability of children, toddlers, or adolescents, with fewer studies conducted with adults. Second, the methodology used was extremely heterogeneous, with the use of either static and dynamic body expressions, point-light displays and/or full-light displays, different types of tasks (e.g., categorization vs. matching), different sets of basic 52 emotions between studies, and body stimuli that contain additional context to aid recognition (e.g., being angry at a defective laptop).5,46 Third, no studies controlled for the effect of concomitant alexithymia on ER. Fourth, very few studies analyze the direct difference between facial ER ability and bodily ER ability from the same actors and displayed using similar methodology. Finally, very few studies considered a related but understudied construct, ER confidence.53,54 Confidence in recognizing facial expressions, but not ability, may be lower in autistic and alexithymic individuals20,55,56; thus far, to the best of our knowledge, no studies have investigated ER confidence using bodily expressions, either alone or alongside facial expressions, nor explored its relationships with autism and alexithymia.
In the present study, we aimed to address the gaps in the literature outlined above. Our main goal was the comparison of face and body ER ability (accuracy) of autistic and non-autistic adults when controlling for alexithymia. Analogously, we explored confidence and intensity mirroring the analyses conducted on ER accuracy. We improved on past approaches through (a) utilizing a more recent measure of alexithymia, underpinned by contemporary understanding of the construct and with stronger psychometric properties58,59; (b) using a new set of ER stimuli, created using a novel method; and (c) the stimulus set contains dynamic videos of bodies and faces of the same actors, devoid of context, and presenting all of the basic emotions; this allowed direct comparisons between facial ER and bodily ER across each of the basic emotions. (1) We hypothesized, based on the overall picture from existing literature, 5 that autistic people would have lower face and body ER accuracy than non-autistic people. In a novel extension of previous explorations, we also examined a possible interaction between ER modality (face, body) and autism group (autistic, non-autistic). (2) We expected that autistic people had lower facial ER confidence, similar to past literature. 55 We explored previously unknown differences in body ER confidence for the first time. (3) Accounting for alexithymia should remove differences between autistic and non-autistic individuals, according to the alexithymia hypothesis. 21 We explored similar patterns in ER confidence and intensity, but we formulated no hypotheses due to novel nature of the question. (4) In addition, we explored emotion-specific differences in ER between autistic and non-autistic individuals, and between low- and high-alexithymia-score individuals. Since no coherent pattern of differences in specific emotions emerged from past literature, this research question was exploratory.
Methods
Participants
Initially, we recruited 406 participants via online opportunity sampling at the University of Lincoln and on a survey recruitment platform—Prolific.co. 60 After data cleaning (described in Data Analysis), the sample size was N = 350. Participants were aged between 18 and 76 years old (M = 27.27, Mdn = 21, SD = 12.70). Seventy-one participants reported having an autism diagnosis, while 279 did not have a diagnosis. We used the AQ-1023,61 to verify if the autistic group scores higher in autistic traits than the non-autistic group, given that we asked for no proof of formal diagnosis from participants. More demographic details about the participants can be found in Table 1. All uses of gender categories in the present study, for both actors and participants, referred to self-identified gender. The gender question was an open-text question where participants wrote their gender identity. We combined instances of “Male” and “Man” to form the male gender category, and we combined “Female” and “Woman” to form the female gender category. We considered both gender categories in a broad sense, with no further gender questions being asked about gender assigned at birth or gender transition.
Demographics of the Autistic and Non-Autistic Groups with Tests of Difference and Association
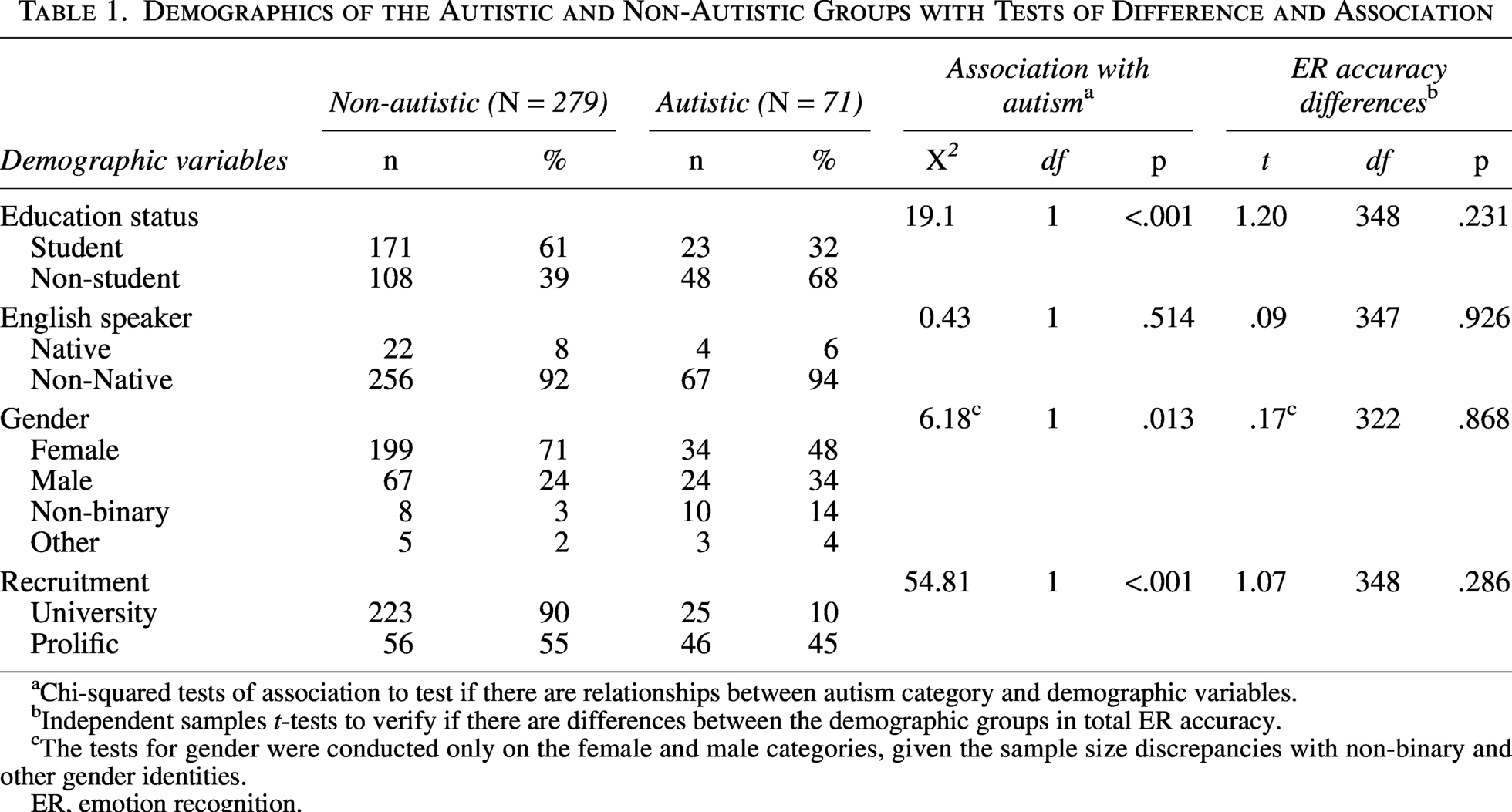
Chi-squared tests of association to test if there are relationships between autism category and demographic variables.
Independent samples t-tests to verify if there are differences between the demographic groups in total ER accuracy.
The tests for gender were conducted only on the female and male categories, given the sample size discrepancies with non-binary and other gender identities.
ER, emotion recognition.
Some of the recruitment involved using a student recruitment system at the University of Lincoln. Students who completed the study in this way were awarded with credit points that were useful for their dissertations. A smaller part of the recruitment involved paying participants on a research participation platform (Prolific.co). Participants on Prolific were paid £2.25 for completing the study. The proportions of participants from each recruitment method can be found in Table 1.
Materials
A short set of questions asked the participants to provide the following demographic information: age, gender, level of study (student or non-student), type of degree (psychology or other), English-speaking category (native or non-native), other languages spoken, and autism diagnosis.
Emotion expression stimuli
We created a new set of stimuli for the purpose of this study (Supplementary Data E). The ER test used 28 short video clips of people displaying one of seven basic emotions: anger, disgust, fear, joy, sadness, surprise, and neutral (14 facial expressions, 14 body expressions). One male and one female actor depicted all face and body expressions (Fig. 1). The body expression stimuli displayed the whole body of an actor with their face digitally covered with a fully opaque oval mask. The videos were grayscale, on a gray background (RGB: 128,128,128), with a dark gray facial mask (RGB: 84,84,84). We filmed the videos at 1920 × 1080 resolution, then cut to size depending on the actor movement. For more details about the filming and editing of the stimuli, see Supplementary Data D. When presented during the task, clips were a constant height of 500 pixels and a varying width of <500 pixels. The clip durations ranged between 1 and 4 seconds (25 FPS); however, participants had the option to replay the videos as many times as they needed without a response time constraint (HTML5 video controls). We asked individuals to categorize the emotion they thought the actor was depicting out of the full list of seven. We also asked participants to indicate how confident they felt about the categorization on a Likert scale (“How confident are you that you recognized the correct emotion?”; 1—very low confidence to 5—very high confidence), and how intense they perceived each expression to be on a similar 5-point scale (“Please rate the intensity of the emotion expression.”). Participants completed each trial only once for a total of 28 trials.
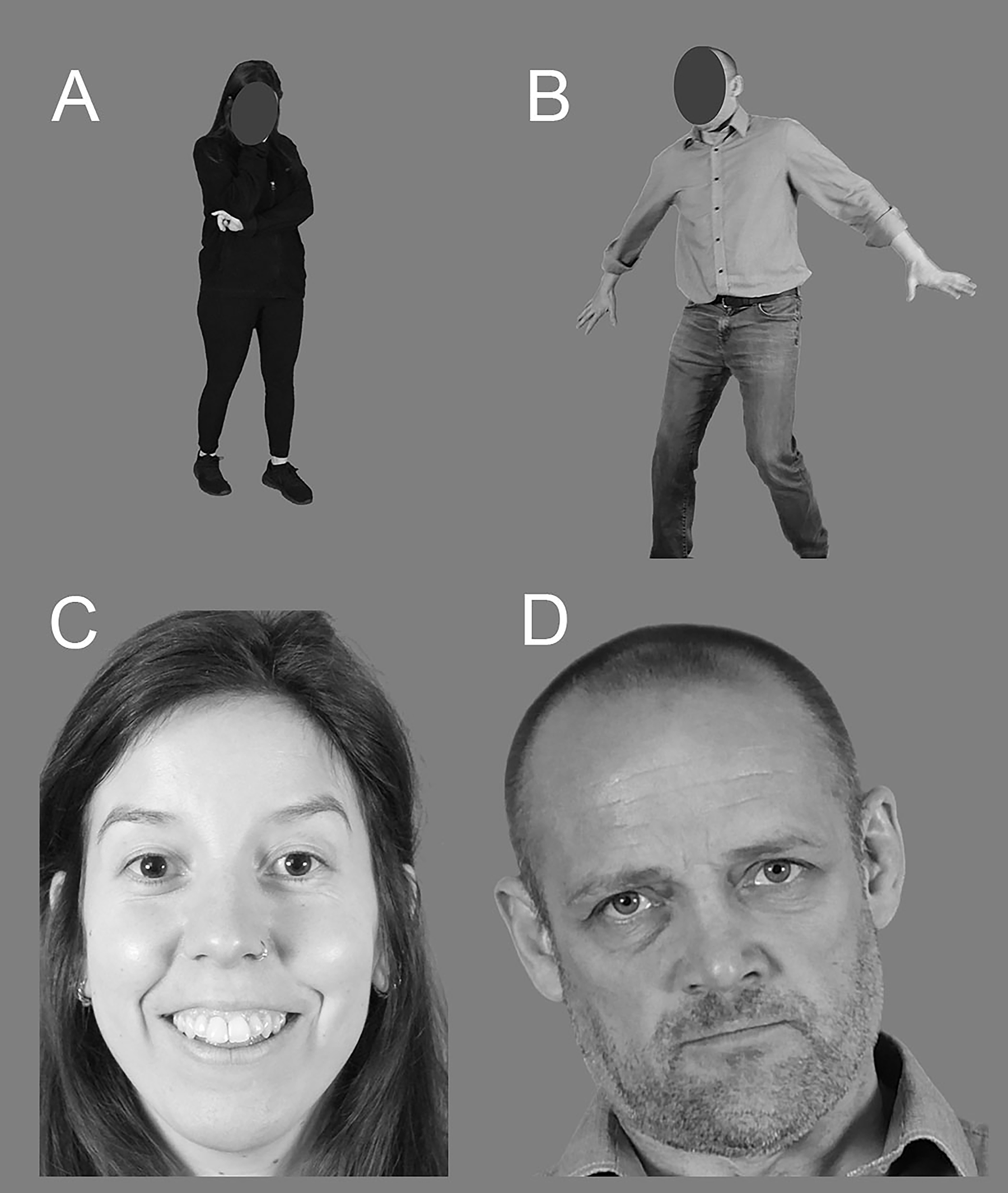
Examples of face and body stimuli from both actors.
Alexithymia questionnaire
The Perth Alexithymia Questionnaire (PAQ) 58 is a 24-item self-report questionnaire answered on a seven-point Likert scale (1 = strongly disagree to 7 = strongly agree). A higher total score indicated a greater level of alexithymia. There are three subscales (eight questions each): difficulty identifying feelings (DIF), difficulty describing feelings (DDF), and externally orientated thinking. The subscales of DDF and DIF can be further subdivided into positive and negative orientation, for example, difficulty identifying positive or negative feelings (P-DIF and N-DIF), with four questions for each. The present study used only the total alexithymia score. An example of a positively worded question is “when I’m feeling good, I can’t talk about those feelings in much depth or detail,” and an example of a negatively worded question is “when I’m feeling bad, I can’t make sense of those feelings.” In the total sample (N = 364), the PAQ had high internal consistency (α = 0.95).
Procedure
We conducted the study online, initially built in Qualtrics, 62 then replicated in QuestionPro 63 due to departmental license changes. Both surveys were identical in order and structure, with just a few inherent webpage style differences. We encouraged participants to remove distractions from their environment during the study. The survey was restricted from being run on mobile devices (phones and tablets) due to possible changes in video sizes.
Participants first completed the demographic questions before moving to the ER task. We fully randomized the order of stimulus presentation. On a single page, participants could see the video at the top, followed by the emotion categories, confidence rating and intensity rating (multiple-choice questions). After finishing the 28 trials, we asked participants to complete the questionnaires. Participants could only see the acronym of the questionnaire they were completing without knowing what it measures. The study took a median of 22 minutes. We obtained ethical approval from the University of Lincoln Research Ethics Committee (reference no. 2022_8946).
Data analysis
We visualized and analyzed the data using jamovi 64 and R/RStudio.65,66 In order to obtain ER scores, we calculated unbiased hit rates (Hu) using Wagner’s 67 method. Hu are expressed as a2/b*c, where “a” is the number of correct responses for a specific emotion, “b” is the number of stimuli for the emotion, and “c” is the frequency of selecting the emotion category (correct + incorrect). We calculated Hu for each emotion within the face and body conditions, as well as the total. We then averaged the Hu of specific emotions to obtain overall scores for body, face, and total.
We removed participants (n = 5) who did not disclose their autism diagnosis status (“prefer not to say”). As we employed opportunity sampling at the University of Lincoln over more than two years, alongside another study using the same stimuli, it is possible that people viewed the stimuli twice. We presented a question at the end of the ER task asking if people had seen the stimuli in the past, and how long ago they remembered seeing the stimuli. Out of the remaining participants, we removed 27 due to stating that they had seen the stimuli in a different study. We did not remove people who said that they were not sure or could not remember clearly whether they had seen the videos previously (n = 14).
We conducted outlier removal on face and body accuracy scores, resulting in six participants (two autistic) being removed. These participants had very low accuracy and were removed in order for the analyses to meet assumptions of normality.
Finally, to improve the validity of comparisons between autistic and non-autistic people, we excluded from the analysis participants who reported being in the process of receiving an autism diagnosis (n = 14). The data cleaning reduced the sample from 406 to 350.
Before the main analysis, we conducted a few methodological checks, mainly involving possible extraneous variables (i.e., education, English level, gender, recruitment method, and age). We computed a t-test to verify differences in alexithymia between the autism groups. To compare participants with high and low alexithymia scores, we applied a median split on the PAQ scores (limitations of the median split are expanded upon in the discussion).
Our main objective for this study was to compare autistic and non-autistic groups on bodily versus facial ER before and after accounting for alexithymia levels. For this purpose, we calculated 2 × 2 mixed ANOVAs with the between-subjects factor autism group (autistic vs. non-autistic) and the within-subjects factor modality (face vs. body) for accuracy scores, confidence ratings, and intensity ratings. To verify if alexithymia explains any effects of autism, we computed an additional set of models where alexithymia level (high vs. low) was added as a between-subjects factor, resulting in 2 × 2 × 2 mixed ANOVAs for each of the ER measures. To explore specific differences between autistic and non-autistic participants on each type of basic emotion, we computed Mann–Whitney U tests.
For the main analysis, all assumptions of mixed ANOVA were met, with the exception of homoskedasticity (Supplementary Data A), for which we applied White’s corrections for heteroskedasticity. 68
Results
Descriptive statistics and correlations between all variables (ER task measures, PAQ and AQ-10) can be found in Supplementary Data C. We explored a few demographic characteristics as extraneous variables. Although some were related to autism, they did not have an effect on ER (Table 1). Autistic participants scored substantially higher on the AQ-10; age was not related to ER constructs (Supplementary Data F).
The distributions of PAQ scores of both the autistic and non-autistic groups are illustrated in Figure 2. Alexithymia was significantly higher in the autistic group (M = 102.15, Mdn = 107, SD = 32) than in the non-autistic group (M = 81.27, Mdn = 82, SD = 26.52), tWelch’s(95.87) = 5.07, p < 0.001, d = 0.71. After the median split on alexithymia, there were 125 participants with high alexithymia scores and 154 participants with low alexithymia score in the non-autistic group, while in the autistic group, there were 50 participants with high alexithymia scores and 21 with low alexithymia scores.
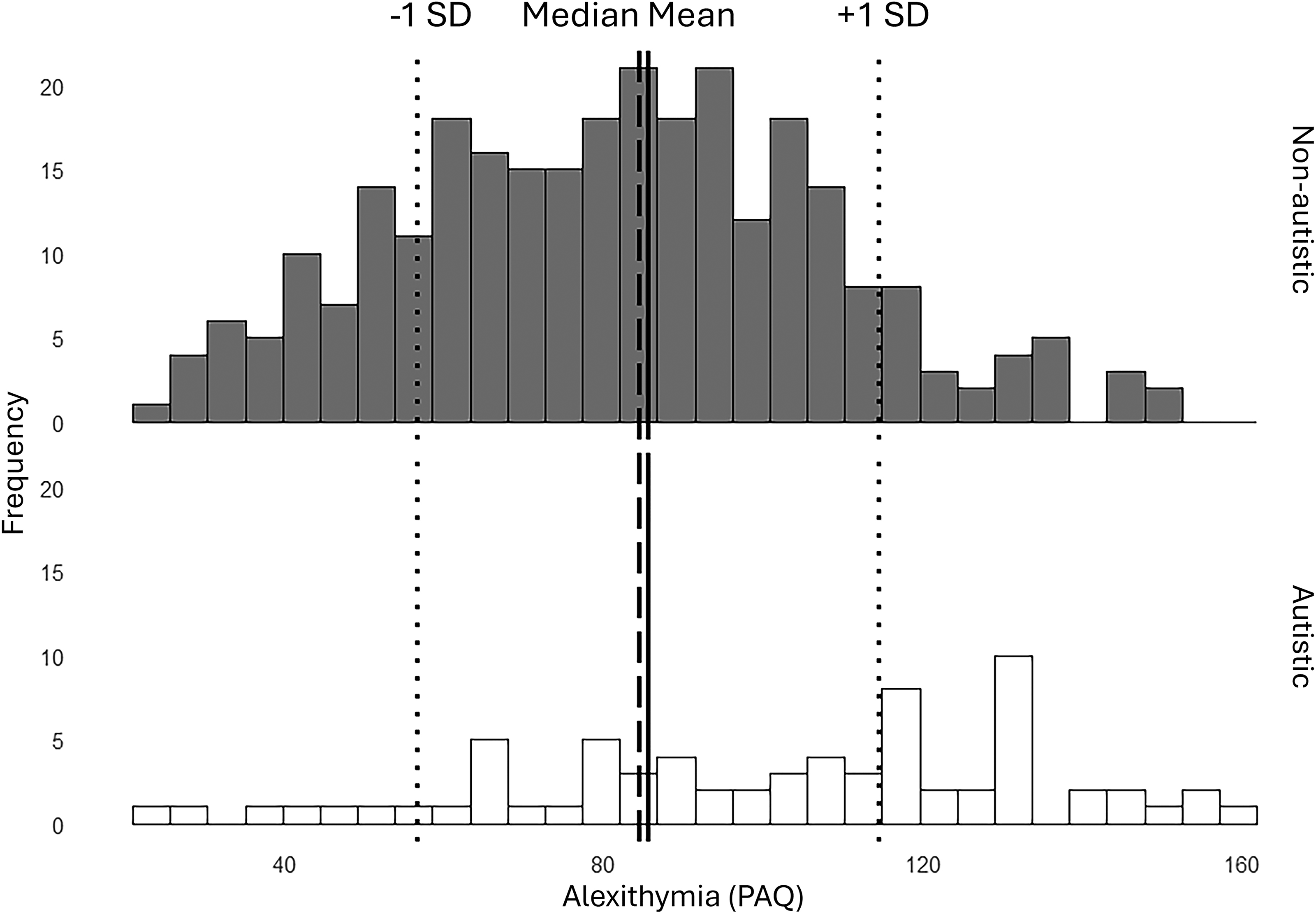
Distributions of alexithymia scores for both autism groups overlapped with whole-sample statistics. The lines denote the mean (solid), median (dashed), and standard deviations (dotted) of the total sample, in order to illustrate which participants were allocated to the high and low alexithymia groups in both the autistic and non-autistic groups after the median split.
When not accounting for alexithymia, autistic participants had significantly lower accuracy (d̄ = 0.03, or 3%) and confidence (d̄ = 0.2), with no intensity differences (ANOVA test statistics found in Table 2). When accounting for alexithymia, the differences in accuracy (d̄ = 0.02, or 2%) and confidence (d̄ = 0.11) were reduced and non-significant.
ANOVA Results of the Two Sets of Analyses for Each ER Measure
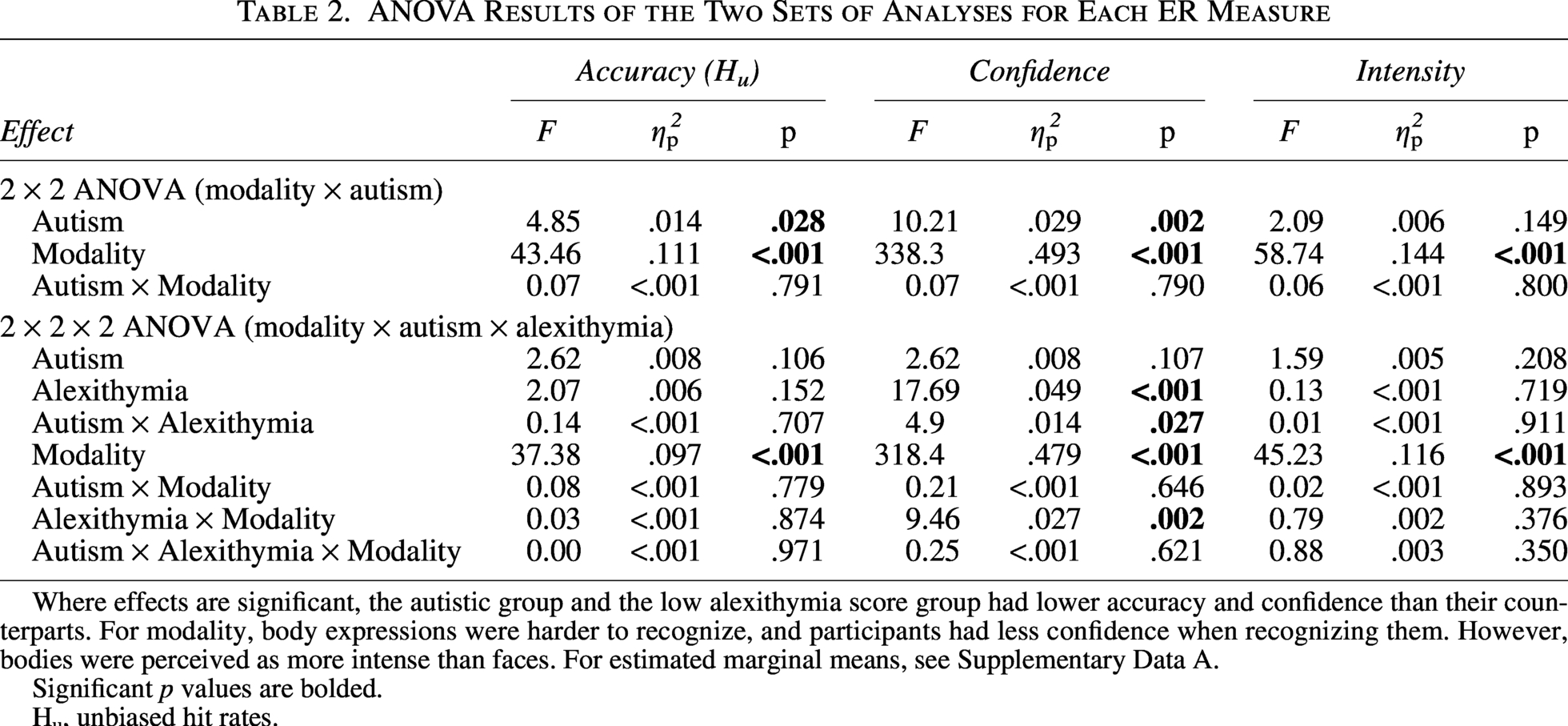
Where effects are significant, the autistic group and the low alexithymia score group had lower accuracy and confidence than their counterparts. For modality, body expressions were harder to recognize, and participants had less confidence when recognizing them. However, bodies were perceived as more intense than faces. For estimated marginal means, see Supplementary Data A.
Significant p values are bolded.
Hu, unbiased hit rates.
There were significant interaction effects only for the confidence measure. There was a compounded effect of alexithymia and autism on confidence: in the high alexithymia group, autistic participants (M = 3.20, SD = 0.52) had significantly lower (p = 0.001) confidence than non-autistic participants (M = 3.45, SD = 0.47), with no differences in the low alexithymia group (p = 0.713). In addition, the alexithymia x modality interaction revealed a larger difference between the low and high alexithymia groups in confidence of recognizing faces (d̄ = 0.20, p = 0.007) than bodies (d̄ = 0.35, p < 0.001). For post hoc tests, see Supplementary Data A. Group means are illustrated in Figure 3.
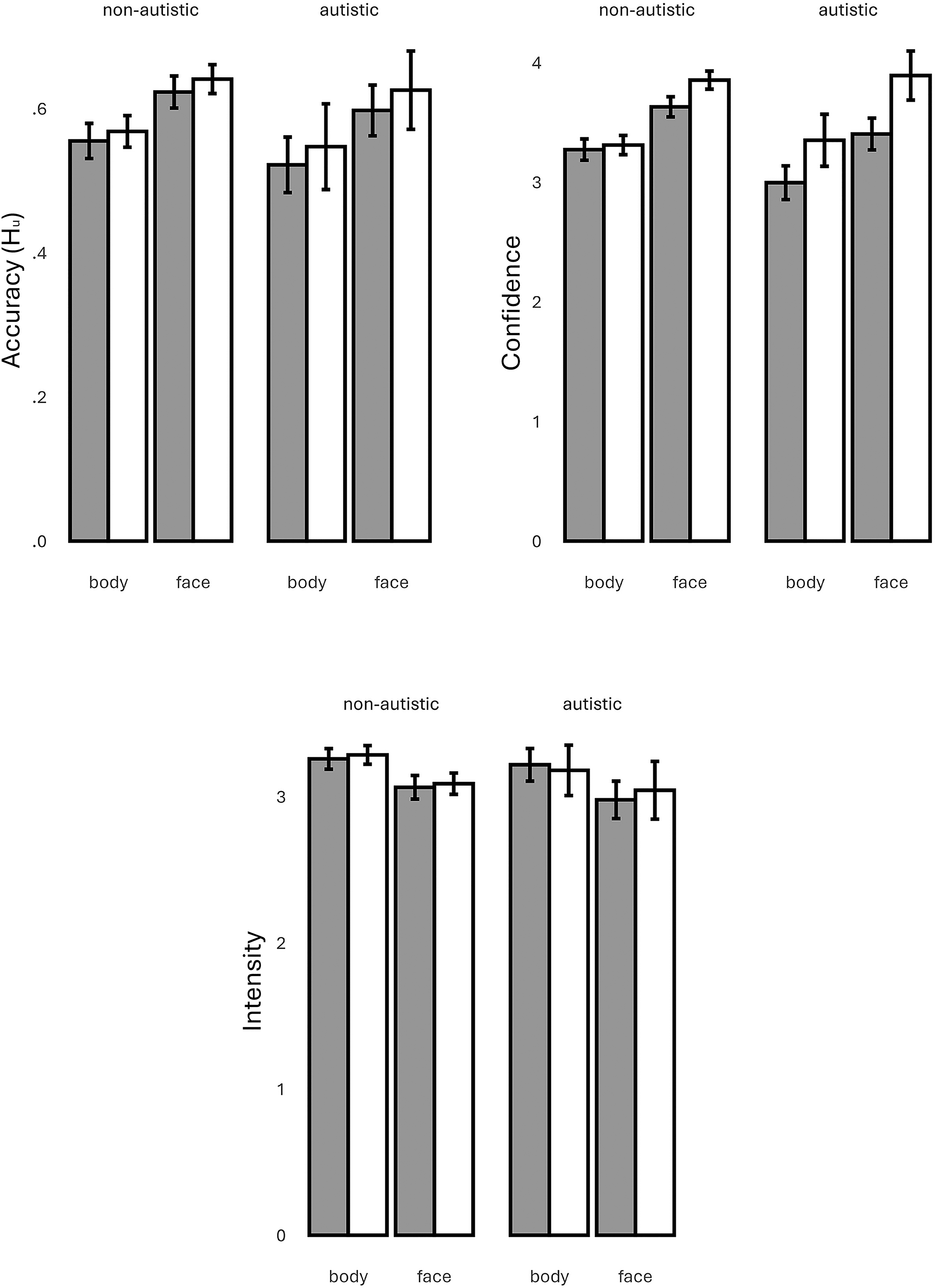
Group means of accuracy, confidence, and intensity by autism and alexithymia group. Alexithymia: gray legend element = high alexithymia, white legend element = low alexithymia. Hu, unbiased hit rates.
Emotion-specific comparisons necessitated non-parametric testing, given that the scores for each emotion and for each modality were obtained by averaging across only two trials. This meant that for accuracy scores, many accuracy DVs would be on a scale with three discrete categories (e.g., 0%−50%−100%). The ordinal variables confidence and intensity would be the average of two 5-point Likert scale ratings, which we were reluctant to consider quasi-interval. We conducted Mann–Whitney U tests with Bonferroni corrections for a family of seven tests (by emotion) to compare both alexithymia groups (high vs. low) and autism groups (autistic vs. non-autistic). Most tests produced non-significant results, with the exception of reduced accuracy in the high alexithymia group on surprise faces (rrank-biserial = 0.17, p = 0.028), and reduced confidence in autistic participants (rrank-biserial = 0.21, p = 0.035). In addition, there were significant differences between the alexithymia groups in confidence of recognizing faces in all seven emotions (Supplementary Data B).
Discussion
The findings of the present study suggest that accounting for alexithymia may eliminate the ER accuracy differences between autistic and non-autistic people, supporting the alexithymia hypothesis. 17 The study supports previous findings in facial ER studies,16–19 and is the first study to provide evidence for the alexithymia hypothesis in bodily ER accuracy. In other words, differences in face and body ER between autistic and non-autistic individuals are due to co-occurring alexithymia. We found no interaction between modality and alexithymia despite bodies being harder to recognize in general than faces, suggesting domain-general difficulties in ER ability. In addition, the study is the first to reveal a similar pattern in ER confidence, with alexithymia accounting for differences between autistic and non-autistic people. In line with previous research, we uncovered a higher difference in confidence between autistic and non-autistic people than in accuracy, with autistic people being slightly less accurate but moderately less confident.20,55,56 We found no effects of autism or alexithymia on perceived intensity ratings.
Alexithymia was a significant predictor of ER confidence, but not ER accuracy, when modeled with autism. Differences in ER confidence between high and low alexithymia score individuals were slightly larger in facial ER than body ER. Given that this pattern was not present in the accuracy measures, it could suggest a negative self-stereotype in alexithymic individuals. However, the results must be interpreted with caution, given that the stimuli used in this study were novel and not validated, making the possibility of one or two face trials being more difficult to recognize and bringing the average confidence down. Despite the limited non-parametric analysis, emotion-specific comparisons did reveal significantly reduced confidence on each emotion and on neutral face trials for high alexithymia score individuals, possibly strengthening the case for a negative self-stereotype, particularly in regard to facial ER ability in alexithymic people. Future research on autism and alexithymia could consider measuring confidence along with accuracy and response times in ER studies to further explore this effect. Moreover, autistic individuals with high alexithymia scores had lower confidence than all other combinations of alexithymia and autism groupings, with this effect not being observed in accuracy. This could suggest a compounded effect of self-stereotyping, adding up self-fulfilling prophecies from both autism and alexithymia ER self-efficacy beliefs. More could be uncovered by conducting mixed-methods research, such as conducting an ER test preceded and followed by a qualitative account of ER self-efficacy. This could reveal whether individuals hold negative self-stereotypes. Further qualitative experiments that could manipulate ER confidence using a within-subjects design would reveal if there is any causal effect of ER confidence on ER accuracy, particularly in alexithymic individuals.
Strengths, limitations, and future directions
We have to raise attention to the small effect size of the differences between autistic and non-autistic individuals, even when not accounting for alexithymia (3% accuracy). While the detection of small effect sizes occurred due to fairly substantial sample sizes, the out-of-lab impact of such effect sizes could be minimal. A 3% accuracy difference corresponds, on average, to an autistic person guessing less than one emotion wrong compared with a non-autistic person (given our 28-trial ER task). In non-verbal communication, misunderstanding a small amount of expressions happens to every human and can be easily remediated by communicative strategies. 69 This is not a limitation of the study, but a positive finding which demonstrates that autistic adults have similar non-verbal ER ability to non-autistic adults. This finding is directly contrary to many mainstream beliefs that autistic people have ER impairment. 70
The study was limited in assessing emotion-specific differences in autism and alexithymia. This occurred due to methodological limitations, mainly the low number of repetitions for each emotion per modality (two repetitions, one for each actor). This study was part of a larger project where we conducted the same task with children as young as 5 in order to compare adult vs. child ER abilities. For this reason, we designed the task to be short and not difficult, having no time restriction to make an emotion choice and allowing participants to replay the videos. In addition, the task involved the use of unvalidated acted emotion expression videos (see Supplementary Data D and E). We created the stimuli for the purpose of this study; they have not been used previously, reducing the generalizability of the findings. However, this was necessary given that there are no emotion expression stimuli available where both face and body expressions are obtained from the same actors. Future studies could address the above limitations by using longer tasks with more repetitions and by validating the stimuli in large-sample studies.
The questionnaires used in this study also come with a few limitations. The AQ-10 has been criticized for reliability and validity issues.71,72 We employed this short version of the AQ (50 items) for the same reason as the shorter ER task: testing involving young children, where study duration needs to be kept as short as possible. The AQ-10 was not a central part of the analysis, however, and was just used to check whether the autism group differs in autistic traits from the non-autistic group. A larger concern can be the use of the PAQ instead of traditional alexithymia measures such as the TAS-20 59 or the BVAQ. 74 While theoretically the PAQ is purported to be built on a theoretical improvement of traditional alexithymia measures, 75 and to have stronger psychometric properties, 55 it is a recently developed questionnaire that has not been used to the same extent. More importantly, the PAQ does not have cutoff points (as the TAS-20) that separate participants into alexithymic and non-alexithymic categories, instead considering alexithymia to be a continuum of personality. As such, grouping people into alexithymia groups is required to be conducted based on sample statistics (based on the sample mean and first standard deviations). Given the autism-alexithymia overlap and the present study’s limited sample of autistic individuals, using the recommended statistical cutoff points 55 resulted in a small sample of low-alexithymia autistic individuals. Instead, we used a median split to obtain only two groups of high and low alexithymia score, resulting in a loss of statistical nuance compared with three groups (low, medium, and high). Future studies could address this issue by collecting data from large samples of autistic individuals (n > 150 for a similar between-subjects design), ensuring adequate sampling of low, medium, and high alexithymia individuals, autistic and non-autistic people.
The effect of alexithymia on the relationship between autism and ER could be affected by some confounders that have not been accounted for in this study. First, the age of the sample was skewed toward younger adults, and controlling for age was unfeasible due to the heteroskedasticity already present in the models, making an ANCOVA difficult to conduct. Future studies would benefit from exploring a wider range of ages. Second, the gender distributions of the autism groups were unbalanced, with more male and non-binary individuals in the autistic group and more females in the non-autistic group; this made matching participants by gender difficult and would have resulted in substantial loss of participants in the autism group. Third, IQ has been shown to impact ER in autistic versus non-autistic comparisons76,77; it has not been controlled for in this study. We also did not collect ethnicity data. Finally, there are a number of other personality traits that could have a confounding effect on ER in autism that were not investigated in this study, such as empathy, 78 depression, 79 anxiety, 80 and ADHD traits. 81 Future studies could attempt to measure a larger number of these interlinked traits and abilities, in very large samples, in order to determine the complex links with ER, autism, and alexithymia. In addition, we were unable to validate autism diagnoses; future studies should confirm diagnostic status for increased methodological rigor.
In the last 50 years of ER research, actor autism diagnosis was almost never considered, making it unknown if the actors that comprise many of the stimulus sets available to researchers are autistic or not. With recent evidence suggesting that non-autistic individuals have difficulties recognizing the emotions of autistic people, the possibility of an in-group preference in ER cannot be ignored. The interaction between actor diagnosis and recognizer diagnosis can introduce unsystematic variance, including in the present study. While communication barriers between autistic and non-autistic people can exist at different levels, the availability of a stimulus set containing actors from both populations could offer a better understanding of the double empathy problem, 70 allowing direct comparison at the ER level.
Footnotes
Acknowledgments
The authors would like to thank their volunteer actors for working with them to film the stimuli; this research would not have been possible without them. The authors also extend thanks to the Progressive Autism Group of the Autism Innovation Research Centre (lincoln.ac.uk/psyspw/psychologyresearch/aric), who have reviewed the output of this study and supported the authors during peer review.
Authorship Confirmation Statement
A.Z.: Writing—original draft, conceptualization, methodology, software, formal analysis, investigation, resources, data curation, visualization, supervision, project administration, and funding acquisition. J.L.: Writing—review and editing, conceptualization, methodology, and investigation. N.K.: Writing—review and editing, conceptualization, methodology, supervision, and project administration. P.M.J.P.: Writing—review and editing, conceptualization, methodology, supervision, and project administration. The article has been submitted solely to Autism in Adulthood.
Author Disclosure Statement
The authors have no conflicts of interest to declare.
Funding Information
This research received no external funding. A.Z. personally covered participant recruitment costs (∼£160) on Prolific.co.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.