
Abstract
Introduction:
Hemp-derived semi-synthetic cannabinoids are marketed as legal alternatives to cannabis containing ≥0.3% Δ9-tetrahydrocannabinol (THC) but remain unregulated at the federal and state levels. Their growing availability underscores the urgent need to investigate patterns of use and associated health risks.
Methods:
Data were collected via an online survey on self-reported patterns and associations of semi-synthetic cannabinoid use, as well as related factors and effects, from a sample of U.S. adults (≥18 years old) who reported past-year cannabis use.
Results:
In the sample (N = 229; 55.5% male, 63.8% White, 80.3% not Hispanic/Latino), nearly half (44.5%) reported using at least one semi-synthetic cannabinoid in the past year. Patterns of use varied by cannabinoid: Δ7-THC (10.0%), Δ8-THC (21.8%), Δ10-THC (14.0%), THC-O-acetate (5.2%), THC homologue tetrahydrocannabiphorol (24.4%), and hydrogenated derivative hexahydrocannabinol (3.5%). Older individuals had lower odds of reporting past-year semi-synthetic cannabinoid use (adjusted odds ratio [aOR] = 0.96, 95% confidence interval [CI] = 0.94, 0.99, p = 0.004); factors associated with higher odds of reporting semi-synthetic cannabinoid use included reporting 101–1,000 lifetime cannabis uses (vs. <100 times; aOR = 2.55, 95% CI = 1.02, 6.38, p = 0.046), reporting 1,001–10,000 lifetime cannabis uses (vs. <100 times; aOR = 4.40, 95% CI = 1.57, 12.33, p = 0.005), and reporting non-inhaled forms of cannabis as the most frequent route of administration in the past year (vs. smoking; aOR = 2.98, 95% CI = 1.18, 7.53, p = 0.021). Adverse effects were reported across all semi-synthetic cannabinoids.
Discussion:
Semi-synthetic cannabinoid use was prevalent among this sample, especially among younger individuals. Despite their popularity, adverse effects underscore the need for regulation and research to address these products’ safety and public health implications.
Introduction
The passage of the 2018 Agriculture Improvement Act (2018 Farm Bill) in the U.S. legalized hemp, defined as cannabis containing 0.3% delta-9-tetrahydrocannabinol (Δ9-THC) or less by dry weight. While the legislation aimed to bolster agricultural development, it inadvertently prompted the rapid expansion of semi-synthetic cannabinoids derived from hemp.1,2 These semi-synthetic cannabinoids are derived by chemically altering natural cannabinoids, such as cannabidiol (CBD), with some occurring naturally in the plant at very low concentrations. Examples of unregulated semi-synthetic cannabinoids include the Δ9-THC isomers delta-7-THC (Δ7-THC), delta-8-THC (Δ8-THC),3–5 and delta-10-THC (Δ10-THC), as well as the THC homologue tetrahydrocannabiphorol (THCP), the THC ester THC-O-acetate (THCOA), and the hydrogenated derivative hexahydrocannabinol (HHC). 6 Many of these semi-synthetic cannabinoids, particularly THC isomers, are hypothesized to produce effects similar to those of Δ9-THC, in part due to their actions as cannabinoid receptor type 1 (CB1) agonists.7,8 The biological effects of Δ9-THC are primarily attributed to its CB1 partial agonism. 9 The isomers, homologues, esters, and derivatives of THC may have varying potencies depending on their level of receptor agonism. 10 For example, THCP has been reported to be more potent than Δ9-THC, likely due to its higher binding affinity for the CB1 receptor.11,12 Despite the wide availability of these cannabinoids to consumers, the safety profile and psychoactive effects of most are unknown, raising significant public health concerns and highlighting a critical gap in regulatory oversight.
Semi-synthetic cannabinoids are often marketed as intoxicating and comparable to cannabis, containing greater than 0.3% Δ9-THC, while complying with the 2018 Farm Bill. However, while some states have begun restricting semi-synthetic cannabinoids, there are no federal or state regulations guiding the manufacturing, sales, or quality control of these products. 11 Due to their complex legal status, novelty, lack of quality control, and the absence of even rudimentary research on their safety and effects, these products pose a significant public health concern. To mitigate risks, it is crucial to determine who is using these products, how and why they are consuming them, where they are acquiring them, and the potential adverse effects.
Emerging and preliminary research highlights several reasons for the use of semi-synthetic cannabinoids. Consumers are drawn to these products for their legality, lower perceived risks, and the potential for either stronger or milder intoxicating effects compared to cannabis with greater than 0.3% Δ9-THC.13–16 In addition, some users seek them for potential therapeutic applications related to physical and mental health conditions. 17 Furthermore, research suggests that individuals residing in states without legalized non-medical cannabis (henceforth defined as cannabis with ≥0.3% Δ9-THC) are more likely to use semi-synthetic cannabinoids. 15 While several motivations for their use have been identified, methods of consumption (i.e., smoking, vaping, oral ingestion, etc.), sources (i.e., regulated or unregulated cannabis dispensaries), similarity of effects to Δ9-THC, and adverse effects remain largely understudied.
Moreover, as the proliferation of semi-synthetic cannabinoids increases, so do concerns about product safety, such as contamination, inaccurate labeling, and the lack of standardized testing protocols.11,18,19 This research aims to examine the patterns and associations of semi-synthetic cannabinoid use, factors influencing their consumption, and user-reported adverse effects in a sample of U.S. adult cannabis consumers. By expanding our understanding of these substances and their use characteristics, this study seeks to inform evidence-based policies that prioritize public health and safety in the evolving cannabis marketplace.
Methods
Participants and recruitment
Data were collected via a Health Insurance Portability and Accountability Act-compliant Qualtrics online platform with expert review fraud detection between March and April 2024. Participants were recruited through advertisements on Facebook, X (formerly known as Twitter), Bluelight.org (an online drug discussion forum), and Craigslist, resulting in a convenience sample. Eligibility requirements included: (1) ≥18 years old, (2) U.S. residence, and (3) past-year use of cannabis and/or cannabis-based products (excluding products containing only CBD).
After participants clicked on the survey link within the advertisement, they were directed to a consent form containing a study overview. All participants provided informed consent, confirmed eligibility requirements, and received a $5 incentive upon completing the survey. If ineligible, the survey redirected respondents to a concluding page, thanking them for their time. Captcha verification, bot detection, straight lining, and multiple submission detection were implemented to remove potential bots and duplicate participation. In addition, demographic questions (i.e., age, state, zip code, etc.) were repeated throughout the survey. Inconsistent responses to these questions disqualified the survey response, as an additional measure to detect potential bots and fraudulent responses. Furthermore, self-reported state and zip code were verified by cross-referencing the geographic coordinates of the survey response. If incongruent, the survey responses were disqualified. Ethics approval was granted by the Institutional Review Board at the University of California, Los Angeles.
Measures
Sociodemographic characteristics
Participants reported their age (continuous, ≥18), biological sex at birth (male, female, other), race (White, Black, More than one race, Other/unknown), ethnicity (Not Hispanic/Latino, Hispanic/Latino, Other/Unknown), sexual orientation (heterosexual, gay/lesbian, other), education (some college, no degree or less, college and/or graduate degree), and state of residence.
Cannabis use
Participants reported past-year most frequent route of cannabis administration (smoking, non-combusted inhalation [vaping, vaporizing, etc.], non-inhalation [i.e., edibles, tinctures, etc.]), frequency of cannabis use in past three months (daily/almost daily, weekly, monthly, once or twice, or never), 20 and estimated lifetime cannabis use (<100, 101–1,000, 1,001–10,000, >10,000 times).
Semi-synthetic cannabinoid use
The primary measure of interest was past-year use of hemp-derived semi-synthetic cannabinoid products. Participants were provided with a list of emerging semi-synthetic cannabinoids that are CB1 receptor agonists (Δ7-THC, Δ8-THC, Δ10-THC, THCOA, THCP, HHC, Other, None of the above) with the following description: “Cannabis-based products can contain a variety of chemical components that are NOT naturally found in large quantities within the plant. The following questions will ask you about your use of these newly emerging cannabis-based chemicals. In the past year (past 12 months), have you used any of the following cannabis-based chemicals? (select all that apply)”. For each product they endorsed using within the past year, participants were asked to report (1) most frequent route of administration (smoking, vaporizing plant material, vaping oil/cartridge, concentrates, edibles, topicals), (2) source (check all that apply: dispensary—legal, illegal, or unsure, delivery service—legal, illegal, or unsure, a friend or family member, a dealer, homegrown, other), (3) reason for first use (more affordable/more accessible, legality/avoid positive drug test, stronger effect, weaker effect, curiosity), and (4) adverse effects (check all that apply: anxiety, paranoia, heart racing, sleepiness, nausea, stimulation, dizziness, confusion, psychotic-like experiences, headache, lightheadedness, other). A range of subjective drug effects were measured using 100 mm visual analog scales for each semi-synthetic cannabinoid: “How similar were the effects relative to cannabis?” (0 mm = completely different, 50 mm = somewhat similar, 100 mm = exactly the same), “How did the strength of the effects compare to cannabis?” (0 mm = much weaker, 50 mm = about the same, 100 mm = much stronger), and “How much did you like the effects?” (0 mm = strongly dislike, 50 mm = neither dislike or like, 100 mm = strongly like).
Data analysis
First, descriptive statistics were conducted to characterize participants among the total sample and among those who reported past-year semi-synthetic cannabinoid use, separately. Bivariate analyses, including independent-samples t-test and Fisher’s exact tests with Monte Carlo simulations (10,000 iterations) and post hoc pairwise comparisons, were used to examine sociodemographic and cannabis use differences between individuals with and without past-year semi-synthetic cannabinoid use. A multivariable logistic regression, including all sociodemographic and cannabis-related variables, was performed to identify factors associated with past-year semi-synthetic cannabinoid use. Analyses were conducted in SPSS v. 29.
Results
Sociodemographic characteristics
On average, eligible participants who completed the survey (N = 229) were 39.0 years old (standard deviation = 12.7), majority were male (55.5%), heterosexual (82.5%), and had completed some college or less (55.9%). Most participants were White (63.8%), not Hispanic/Latino (80.3%), and living in a state with legal adult-use cannabis (76.4%; Table 1).
Sociodemographic and Cannabis Use Characteristics
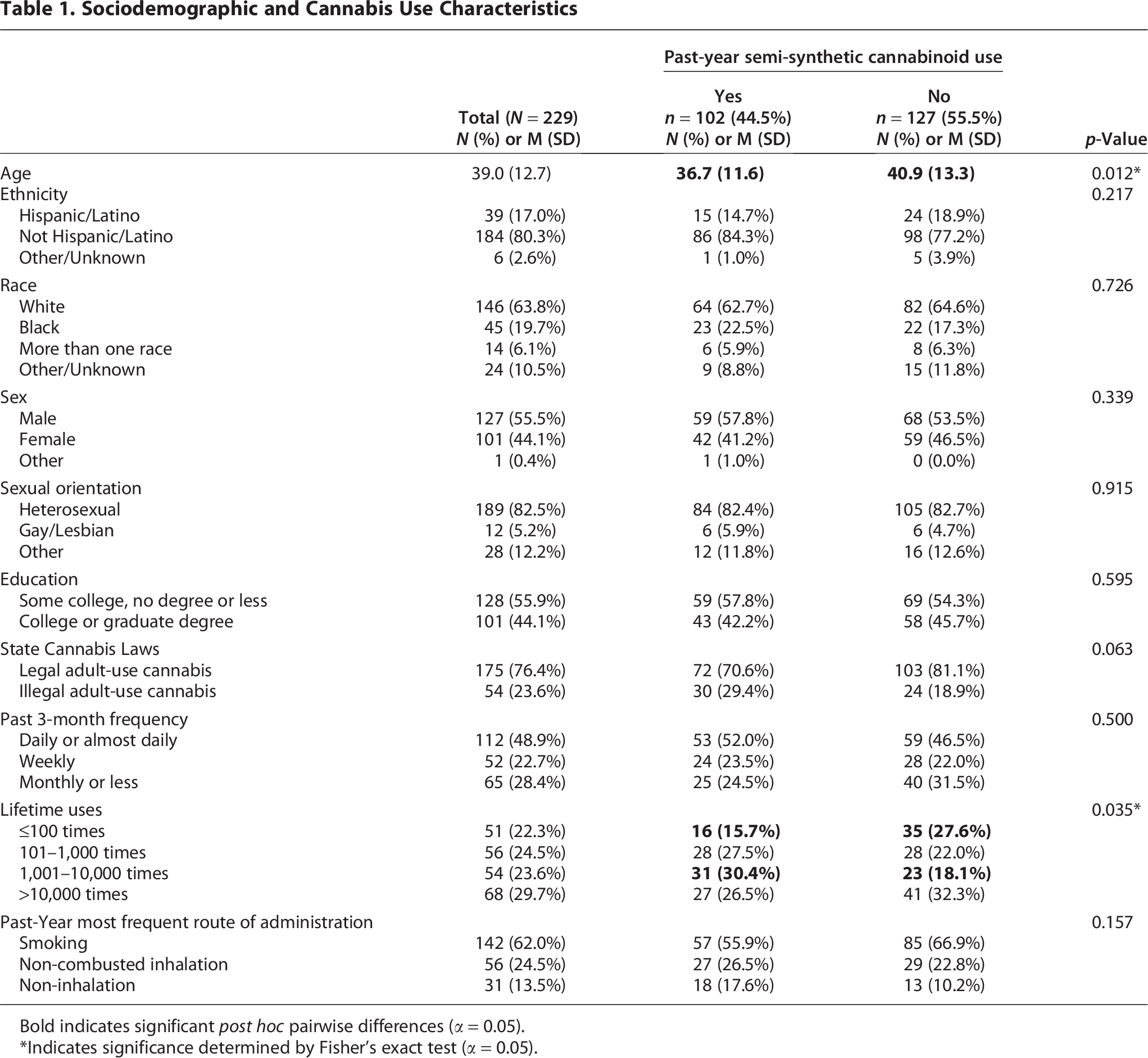
Bold indicates significant post hoc pairwise differences (α = 0.05).
Indicates significance determined by Fisher’s exact test (α = 0.05).
Cannabis use
Nearly half (48.9%) of participants reported daily or almost daily cannabis and/or cannabis-based product use within the past three months (Table 1). More than half (53.3%) reported >1,000 lifetime cannabis uses. Smoking (62.0%) was the most frequent route of cannabis administration reported.
Semi-synthetic cannabinoid use
Among all participants, 44.5% reported past-year semi-synthetic cannabinoid use. Patterns of use varied by cannabinoid: THCP (24.4%), Δ8-THC (21.8%), Δ10-THC (14.0%), Δ7-THC (10.0%), THCOA (5.2%), and HHC (3.5%) and Other (1.3%; “THCA,” “THCV,” “CBC”). Smoking was reported as the most frequent route of administration across all semi-synthetic cannabinoids (Table 2). For all types of semi-synthetic cannabinoids, the most reported source was a regulated/legal dispensary, and the most frequently reported reasons for first use were legality relative to other cannabis products and curiosity (Table 2).
Characteristics of Semi-Synthetic Cannabinoid Use

Number/percentage of individuals out of the individuals who endorsed past-year use of the semi-synthetic cannabinoid.
Check all that apply.
Factors associated with past-year semi-synthetic cannabinoid use
Participants who reported use of at least one semi-synthetic cannabinoid within the past year were significantly younger (36.7 ± 11.6 years) than those who did not (40.9 ± 13.3 years; p = 0.012; Table 1). Past-year semi-synthetic cannabinoid use was not associated with ethnicity, race, sex, sexual orientation, or education (Table 1).
Past-year use of semi-synthetic cannabinoids was higher among those from states where adult-use cannabis is illegal, though this did not reach statistical significance (p = 0.06; Table 1). Those who reported 1,001–10,000 lifetime cannabis uses had higher odds of endorsing past-year semi-synthetic cannabinoid use, while those who reported ≤100 lifetime cannabis uses had lower odds of reporting past-year semi-synthetic cannabinoid use (both p < 0.05; Table 1).
An adjusted logistic regression analysis indicated that younger individuals had higher odds of past-year semi-synthetic cannabinoid use (adjusted odds ratio [aOR] = 0.96, 95% confidence interval [CI] = 0.94, 0.99, p = 0.004; Table 3); factors associated with higher odds of past-year semi-synthetic cannabinoid use included reporting 101–1,000 lifetime cannabis uses (vs. <100 times; aOR = 2.55, 95% CI = 1.02, 6.38, p = 0.046; Table 3), 1,001–10,000 lifetime cannabis uses (vs. <100 times; aOR = 4.40, 95% CI = 1.57, 12.33, p = 0.005; Table 3), and non-inhaled forms of cannabis as the most frequent routes of administration in the past year (vs. smoking; aOR = 2.98, 95% CI = 1.18, 7.53, p = 0.021; Table 3).
Adjusted Associations Between Sociodemographics, Cannabis Use, and Past-Year Semi-Synthetic Cannabinoid Use
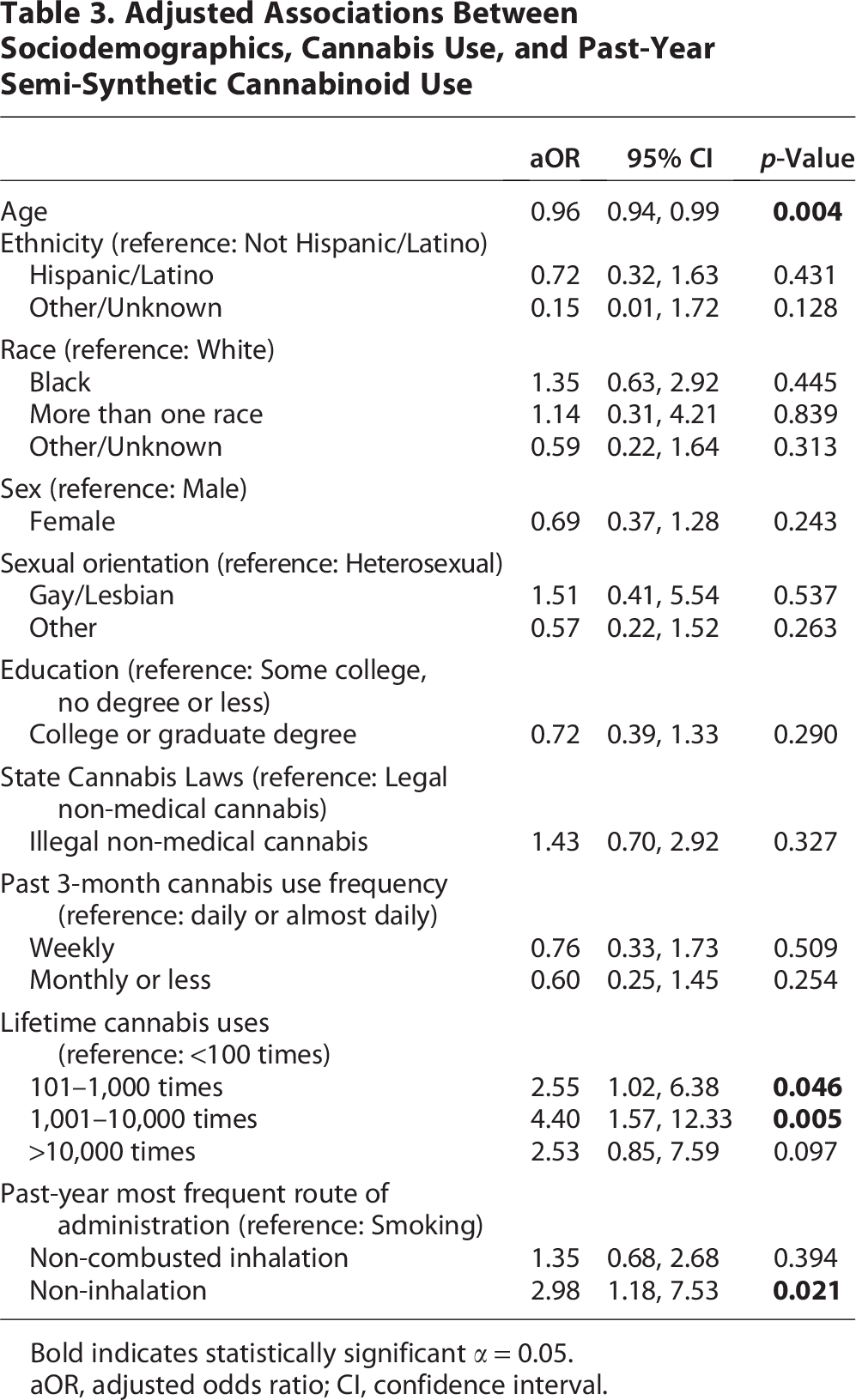
Bold indicates statistically significant α = 0.05.
aOR, adjusted odds ratio; CI, confidence interval.
Effects of semi-synthetic cannabinoids
When asked about the strength of effect relative to cannabis containing greater than 0.3% Δ9-THC, participants reported that all semi-synthetic cannabinoids were stronger on average, apart from Δ8-THC (Fig. 1).
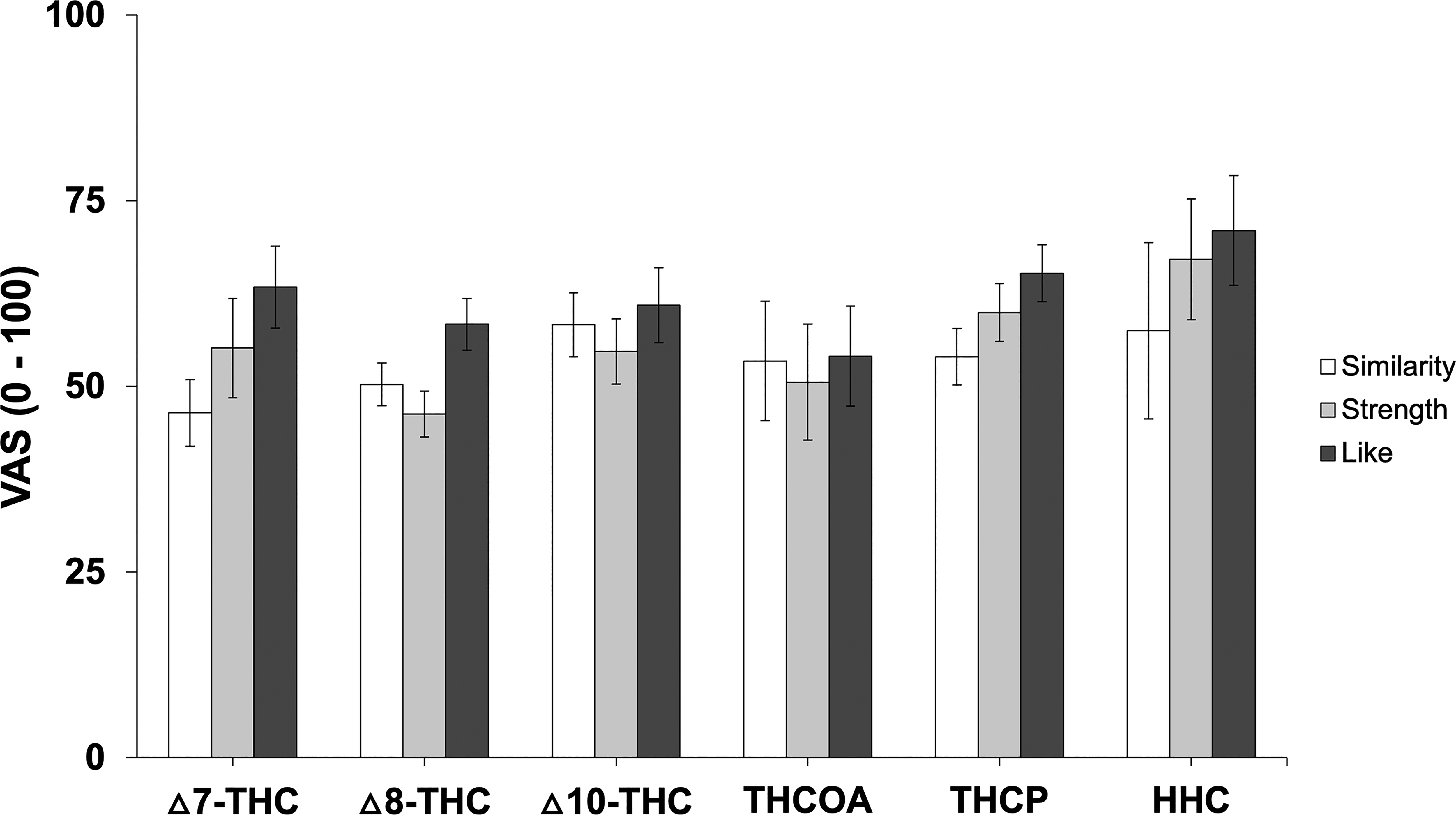
Semi-synthetic cannabinoid subjective ratings. Visual analog scale (VAS) data for subjective ratings of “how similar were the effects relative to cannabis?” (0 mm = completely different, 50 mm = somewhat similar, 100 mm = exactly the same), “how did the strength of the effects compare to cannabis?” (0 mm = much weaker, 50 mm = about the same, 100 mm = much stronger), and “how much did you like the effects?” (0 mm = strongly dislike, 50 mm = neither dislike or like, 100 mm = strongly like) for each semi-synthetic cannabinoid represented as mean ± standard error. HHC, hydrogenated derivative hexahydrocannabinol; THC, tetrahydrocannabinol; THCOA, THC ester THC-O-acetate; THCP, THC homologue tetrahydrocannabiphorol.
In terms of liking, none of the semi-synthetic cannabinoids were strongly liked or disliked, although participants reported the greatest “liking” for THCP and HHC.
Regarding similarity, participants generally rated the effects of semi-synthetic cannabinoids as moderately similar to cannabis containing greater than 0.3% Δ9-THC, with average ratings clustering around the midpoint of the scale (“somewhat similar”).
Adverse effects were reported across all semi-synthetic cannabinoids. For each, 50% or more of participants who endorsed past-year use reported experiencing at least one adverse effect (Table 4). Anxiety was the most frequently reported adverse effect of Δ10-THC and THCP, while both anxiety and stimulation were most frequently reported for Δ7-THC. Sleepiness was the most common adverse effect of Δ8-THC. For HHC, both sleepiness and stimulation were reported as frequent adverse effects, highlighting the variability of responses (Table 4).
Adverse Effects of Semi-Synthetic Cannabinoids
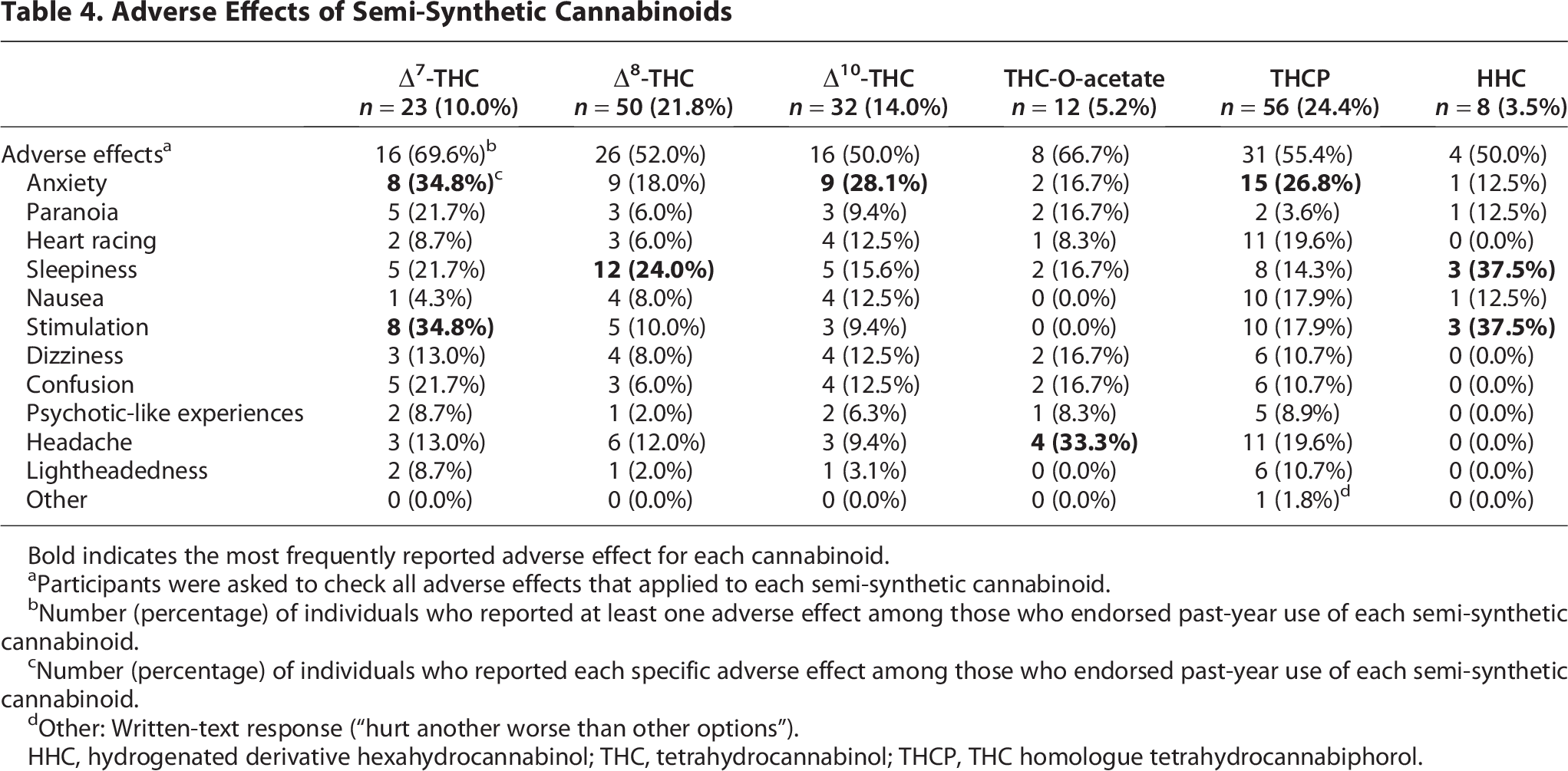
Bold indicates the most frequently reported adverse effect for each cannabinoid.
Participants were asked to check all adverse effects that applied to each semi-synthetic cannabinoid.
Number (percentage) of individuals who reported at least one adverse effect among those who endorsed past-year use of each semi-synthetic cannabinoid.
Number (percentage) of individuals who reported each specific adverse effect among those who endorsed past-year use of each semi-synthetic cannabinoid.
Other: Written-text response (“hurt another worse than other options”).
HHC, hydrogenated derivative hexahydrocannabinol; THC, tetrahydrocannabinol; THCP, THC homologue tetrahydrocannabiphorol.
Discussion
This survey study assessed the patterns of use, associated characteristics, and reported effects of semi-synthetic cannabinoid use among a convenience sample of U.S. adult cannabis consumers. Nearly half (44.5%) of respondents reported using at least one semi-synthetic cannabinoid in the past year, with the most frequently reported being THCP (24.4%), followed by Δ8-THC (21.8%) and Δ10-THC (14.0%). Younger age, greater lifetime cannabis use, and preference for non-inhaled routes of cannabis administration were associated with increased odds of endorsing past-year semi-synthetic cannabinoid use. Notably, a substantial proportion of individuals who reported past-year semi-synthetic cannabinoid use experienced adverse effects, highlighting the urgent need for further regulatory and scientific attention to these emerging products.
The relatively high patterns of semi-synthetic cannabinoid use within this sample underscore the growing presence of these products in the U.S. cannabis marketplace in both states with and without adult-use cannabis regulations. The finding that younger individuals were more likely to use semi-synthetic cannabinoids is consistent with broader trends in novel substance use, where younger users tend to experiment more frequently with emerging drug products.15,21 In addition, greater lifetime cannabis use was associated with semi-synthetic cannabinoid use, suggesting that individuals with greater cannabis exposure may be more open to trying semi-synthetic cannabinoids. The preference for non-inhaled methods among individuals who reported past-year semi-synthetic cannabinoid use may reflect differences in product formulations or consumer perceptions of safety, potency, or legal status. 16 At the same time, our findings suggest that individuals who primarily use non-inhaled cannabis may turn to inhaled semi-synthetic cannabinoids due to availability or the desire for faster onset of effect, a pattern with potential clinical and public health implications given the increased exposure to combustion-related risks.
The trend toward higher past-year use of semi-synthetic cannabinoids in states where adult-use cannabis remains illegal (p = 0.06) suggests that legal restrictions on cannabis containing greater than 0.3% Δ9-THC may inadvertently drive interest in alternative, unregulated cannabinoid products. This aligns with previous research showing that restrictive cannabis policies can lead consumers to seek out legally ambiguous or unregulated substitutes.15,22,23 Given the lack of federal and state regulations on semi-synthetic cannabinoids, their increasing use raises concerns about product safety, including mislabeling, contamination, and unanticipated psychoactive effects.
Participants generally reported that the effects of semi-synthetic cannabinoids were moderately similar to those of cannabis containing greater than 0.3% Δ9-THC. However, perceptions of strength varied considerably by cannabinoid. Δ8-THC was most often described as producing weaker subjective effects, consistent with prior reports that Δ8-THC may act as a lower efficacy agonist at the CB1 receptor relative to Δ9-THC. 24 In contrast, THCP and Δ10-THC were more frequently described as stronger, which may reflect their higher binding affinity or greater efficacy for cannabinoid receptors or distinct metabolic pathways. However, these pharmacological mechanisms have not been systematically characterized. These subjective reports suggest heterogeneity in potency and efficacy that warrant careful pharmacological validation, particularly given the lack of standardized dosing or regulation of these products.
In terms of subjective reports of drug liking, none of the semi-synthetic cannabinoids were rated as being strongly liked or disliked overall, suggesting that participants’ experiences may have been mixed or variable. Notably, THCP and HHC received the highest ratings of liking, which could be due to their greater perceived strength or distinctive psychoactive profiles. Although liking was not uniformly elevated, these findings raise concerns about potential repeated use or misuse of certain semi-synthetic cannabinoids, particularly in the absence of established safety data.
With respect to similarity, participants indicated that the effects of semi-synthetic cannabinoids were somewhat similar to those of cannabis containing greater than 0.3% Δ9-THC. However, nuanced differences in dosages and concentrations present in the semi-synthetic cannabinoid products and subjective experiences suggest that while these products may mimic some of the psychoactive effects of cannabis, they cannot be assumed to produce identical experiences. These perceived similarities may explain their appeal as cannabis alternatives, particularly in jurisdictions where Δ9-THC products are restricted, but they also highlight the risk of users underestimating differences in the strength of effect and safety.
Adverse effects were commonly reported across all semi-synthetic cannabinoids, with at least half of participants who endorsed past-year use of any cannabinoid reporting at least one adverse effect. The most frequently reported complaints included anxiety, stimulation, and sleepiness, with notable variation across semi-synthetic cannabinoids (e.g., anxiety for THCP and Δ10-THC, sleepiness for Δ8-THC, and paradoxical reports of both sleepiness and stimulation for HHC). These patterns underscore the unpredictable nature of semi-synthetic cannabinoid effects and align with prior work documenting variability in both subjective and physiological responses. However, it should be noted that this study did not assess adverse event rates relative to cannabis, and therefore, it remains unclear whether these products are associated with similar, greater, or lesser risks compared to cannabis. Moreover, given the cross-sectional, descriptive design, causation cannot be inferred, and the directionality of associations cannot be determined. Taken together, these findings suggest that semi-synthetic cannabinoids may pose unique risks and highlight the urgent need for systematic research on their pharmacological profiles, safety, and regulatory oversight.
25
Several limitations should be noted. First, the relatively small, convenience sample limits the generalizability of the findings and precludes drawing population-level inferences. In particular, the predominance of participants from states with legal cannabis likely reflects, at least in part, the study’s eligibility criterion requiring past-year cannabis use, which may be more common or more easily reported in legal states. Other factors, such as differences in recruitment platform engagement or regional variation in survey participation, could also have contributed to this distribution. This overrepresentation of participants from legal states may limit generalizability and could influence the observed patterns of semi-synthetic cannabinoid use. Third, due to the cross-sectional design and reliance on self-reported behaviors and experiences, this study cannot be used to infer directionality or causal relationships. In addition, participants were not asked to report the dose or concentrations of semi-synthetic cannabinoids they consumed. Differences in dosage or formulation could influence perceptions of strength and similarity, and this limitation should be considered when interpreting our findings. Subjective ratings of relative strength and similarity may therefore be confounded by variability in product dose or frequency of use, which we were unable to systematically capture in this survey. While this study examined patterns of semi-synthetic cannabinoid use and associated characteristics, additional research must address the acute and long-term health consequences of these semi-synthetic cannabinoids through rigorous pre-clinical, clinical, and toxicological studies. Several case reports highlighted the potentially severe, and even near-fatal, effects of semi-synthetic cannabinoid exposure.27–32 However, for many of these case reports, the cannabinoid in the product was not verified, exposure could not be assessed through toxicological methods, the dose was unknown, and/or the presence of other solvents, cannabinoids, or other drugs was unknown. These reports in tandem with the current survey study underscore the need for greater regulation and carefully controlled research of these products.
This study identified the widespread use of various emerging hemp-derived semi-synthetic cannabinoids among a sample of U.S. adults who use cannabis. Younger individuals, those with extensive cannabis experience, and those living in states where adult-use cannabis is illegal were more likely to report past-year semi-synthetic cannabinoid use. Despite their increasing popularity, adverse effects were common and wide-ranging, reinforcing the need for regulation and research to support consumer safety. As the cannabis market continues to evolve, policymakers should develop evidence-based frameworks to regulate hemp-derived semi-synthetic cannabinoids that prioritize transparency, quality control, and harm reduction.
Footnotes
Authors’ Contributions
Conceptualization, methodoly, investigation and Writing—reviwing and editing: E.P., S.L., C.H.M., Z.D.C. Formal Analysis & Data Curation: E.P. Resources: Z.D.C. Writing—Original draft preparation: E.P. Visualization: E.P. Supervision: Z.D.C. Funding Acquisition: Z.D.C., S.L., E.P.
Author Disclosure Statement
Outside of this work, Z.D.C. reports receiving study drug from Canopy Growth Corp and True Terpenes, and study-related materials from Storz & Bickel. C.H.M. is the creator of the citizen neuroscience platform ![]() . All other authors declare that they have no competing interests or disclosures associated with this publication.
. All other authors declare that they have no competing interests or disclosures associated with this publication.
Funding Information
U.S. National Institute on Drug Abuse (R01DA047296, R01DA057252), the Semel Charitable Foundation, and Institutional Research Career and Academic Development Award at University of California, Los Angeles (K12GM106996). S.L. is supported through a Canadian Institutes of Health Research Banting Postdoctoral Fellowship. Z.D.C.’s research is funded by grants from the National Institute on Drug Abuse, National Center for Complementary and Integrative Health, California Department of Cannabis Control, Center for Medicinal Cannabis Research, and the California Highway Patrol.