
Abstract
Introduction and Objectives:
Strict photoprotection is essential for the management of photodermatoses. However, we have not found studies on photoprotection (topical and/or oral) prescribed in clinical practice. Our objective was to describe the characteristics of topical and oral photoprotection recommended for photodermatoses, including the prescription of a topical broad-spectrum sunscreen containing ectoin (BSSE).
Materials and Methods:
An anonymous survey carried out (as a pretest) among dermatologists at an online photoprotection event held on May 20, 2023, in Spain.
Results:
The survey was answered by 90 dermatologists (45.4% [90/198] of the attendees). Of these, 67.8% (61/90) were women, and 83.3% (75/90) worked in public hospitals; 98.9% (89/90) reported always or almost always prescribing sunscreens in cases of photodermatoses. The most important characteristics of sunscreens were: protection against ultraviolet A (UVA) (95.6%) (86/90), against visible light (76.7%) (69/90), and the cosmetic acceptability of the product (67.8%) (61/90); 90% (81/90) reported regularly prescribing a BSSE for photodermatosis, and 60.7% (54/90) claimed that this product was effective or highly effective in reducing symptoms. Oral photoprotection was recommended by 95.5% (85/89) of respondents, and 97.7% (86/88; 2 nonresponders) reported observing a decrease in symptomatology when oral photoprotection was prescribed together with sunscreens.
Limitations:
Online survey, potential inclusion bias.
Conclusions:
The majority of dermatologists surveyed prescribed sunscreens with high protection against UVA and visible light for photodermatoses, recommended oral photoprotection with Polypodium leucotomos and reported observing a decrease in symptomatology after recommending topical plus oral photoprotection.
Introduction
Photodermatoses are a heterogeneous group of disorders that can be classified as immunologically mediated or idiopathic, drug- or chemical-induced photosensitivity, photoaggravated dermatoses, and photodermatoses associated with defective DNA repair (genetic disorders). Ultraviolet A (UVA) radiation is involved in the pathophysiology of multiple conditions, such as polymorphic light eruption (PLE), cutaneous lupus erythematosus, solar urticaria, actinic prurigo, porphyrias, chronic actinic dermatitis and phototoxic/photoallergic reactions, among others. Their pathophysiology is complex and not fully understood, with ultraviolet B (UVB) radiation and longer wavelengths such as UVA and visible light (VL) frequently involved.1,2 Management can be challenging, and strict photoprotection together with treatment of the underlying disorder is essential. 3 Although conscientious photoprotection, including the use of broad-spectrum sunscreens (BSSs), is crucial for the management of photodermatoses, 3 we found no studies addressing the type of photoprotection (topical and/or oral) recommended for patients with photodermatoses seen in routine clinical practice.
Most studies on the usefulness of topical photoprotectors in photodermatoses treatment have been conducted on individuals with PLE and have shown a reduction in symptoms of this condition.2,4–7 Ectoin (1,4,5,6-tetrahydro-2-methyl-4-pyrimidinecarboxylic acid) synthesized by various bacteria, has multiple protective properties, including barrier-stabilizing, hydrating, and cytoprotective effects that may help mitigate UV- and VL-induced cellular damage.8,9 A topical BSS with Sun protection factor (SPF) >100, UVA protection factor >40, and 1% ectoin (FotoUltra ISDIN Solar Allergy, ISDIN Laboratories, Barcelona, Spain) demonstrated the ability to prevent UVA-induced PLE flares in a randomized study. 2
Polypodium leucotomos (PL) is a fern extract that has been shown in multiple studies to possess antioxidant/anti-inflammatory and photoprotective properties, 10 and may serve as an adjuvant in the management of photodermatoses such as PLE, solar urticaria, and actinic prurigo.11–13 PL-containing supplements are considered a form of oral photoprotection and are commercially available in several formulations.
Our objective was to describe the characteristics of both oral and topical photoprotection prescribed for photodermatoses in routine clinical practice, including the prescription and perceived efficacy of a BSS-containing ectoin (BSSE).
Methods
Online survey
An anonymous online survey was conducted among dermatologists from all over Spain who attended a symposium on photoprotection and photodermatoses in May 2023. The survey was carried out as a pretest before the online symposium. It consisted of nine questions (Table 1) about the prescription of topical and oral photoprotection in cases of photodermatoses, and the characteristics of these products. The survey was conducted outside the venue of the symposium, and no commercial products, corporate logos, or marketing elements were displayed. Respondents authorized the management of the data and publication of the results.
Questions Included in the Survey
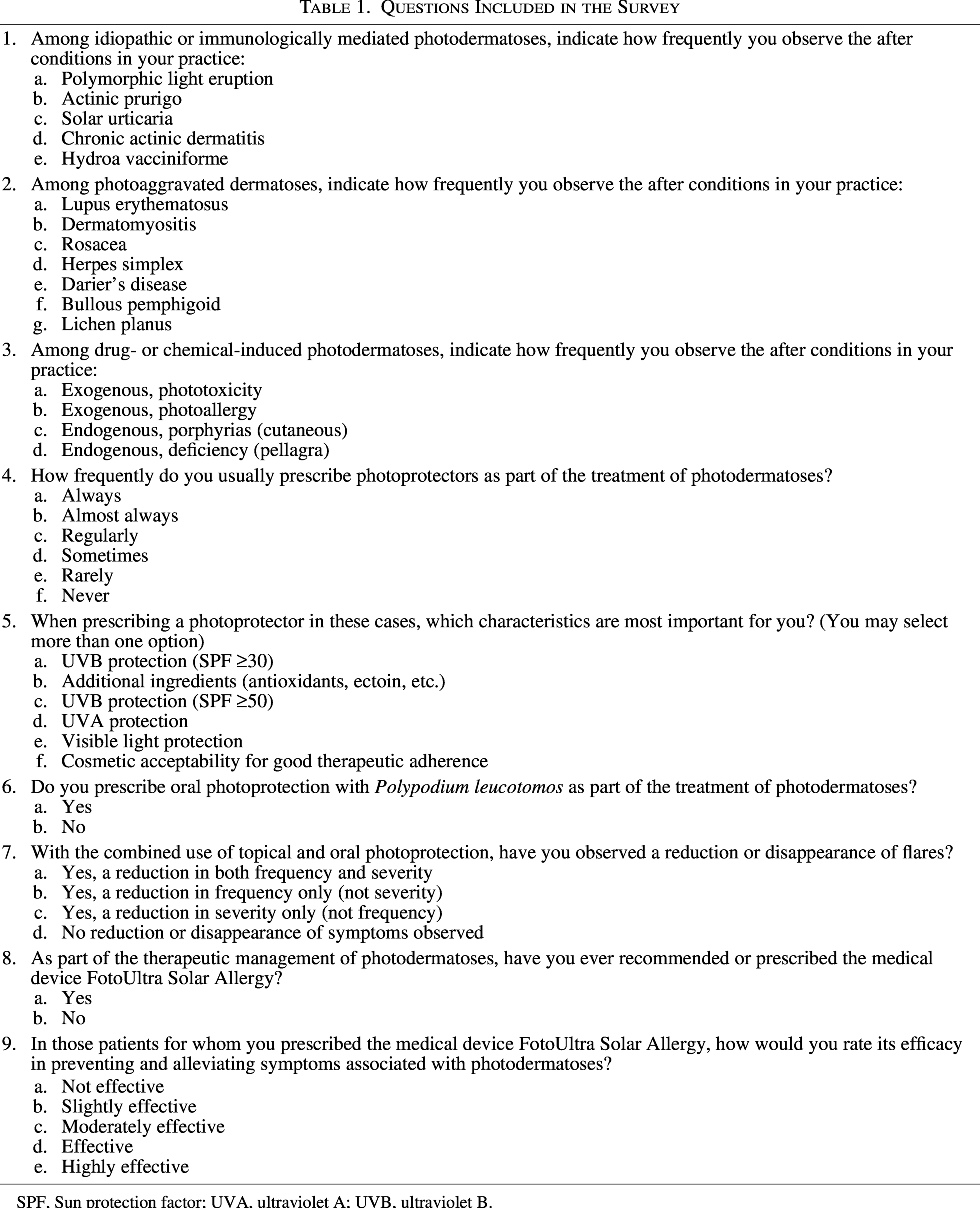
SPF, Sun protection factor; UVA, ultraviolet A; UVB, ultraviolet B.
Statistical analysis
Data collection and statistical analysis were performed by an independent external company with no ties to the pharmaceutical industry. Descriptive statistics were applied to the variables collected. Categorical variables are presented as frequency distributions and proportions. Quantitative variables (continuous or ordinal) are presented using measures of central tendency (mean or median) and dispersion (standard deviation [SD] or minimum and maximum values). The analysis was performed using IBM SPSS Statistics version 26.0.
Results
A total of 90 dermatologists completed the survey (response rate 45.4% [90/198]). The mean age was 40.3 years (SD ± 12.5). Of these, 67.8% (61/90) were women, and 83.3% (75/90) worked in public hospitals (Table 2).
Epidemiological Characteristics of Respondents
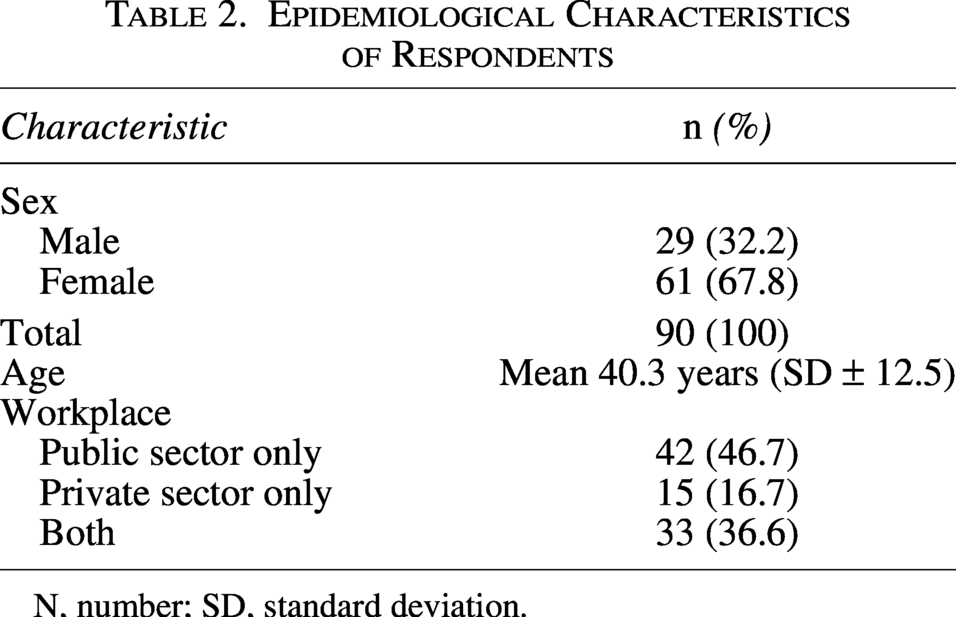
N, number; SD, standard deviation.
Types of photodermatoses in clinical practice
Respondents reported that the most frequent idiopathic photodermatosis seen in their practice was PLE (86.7% [78/90]); the most frequent photoaggravated dermatosis was rosacea (76.7% [69/90]); and the most frequent drug- or chemical-induced photodermatosis was phototoxicity (52.2% [47/90]) (Table 3).
Photodermatoses in Clinical Practice
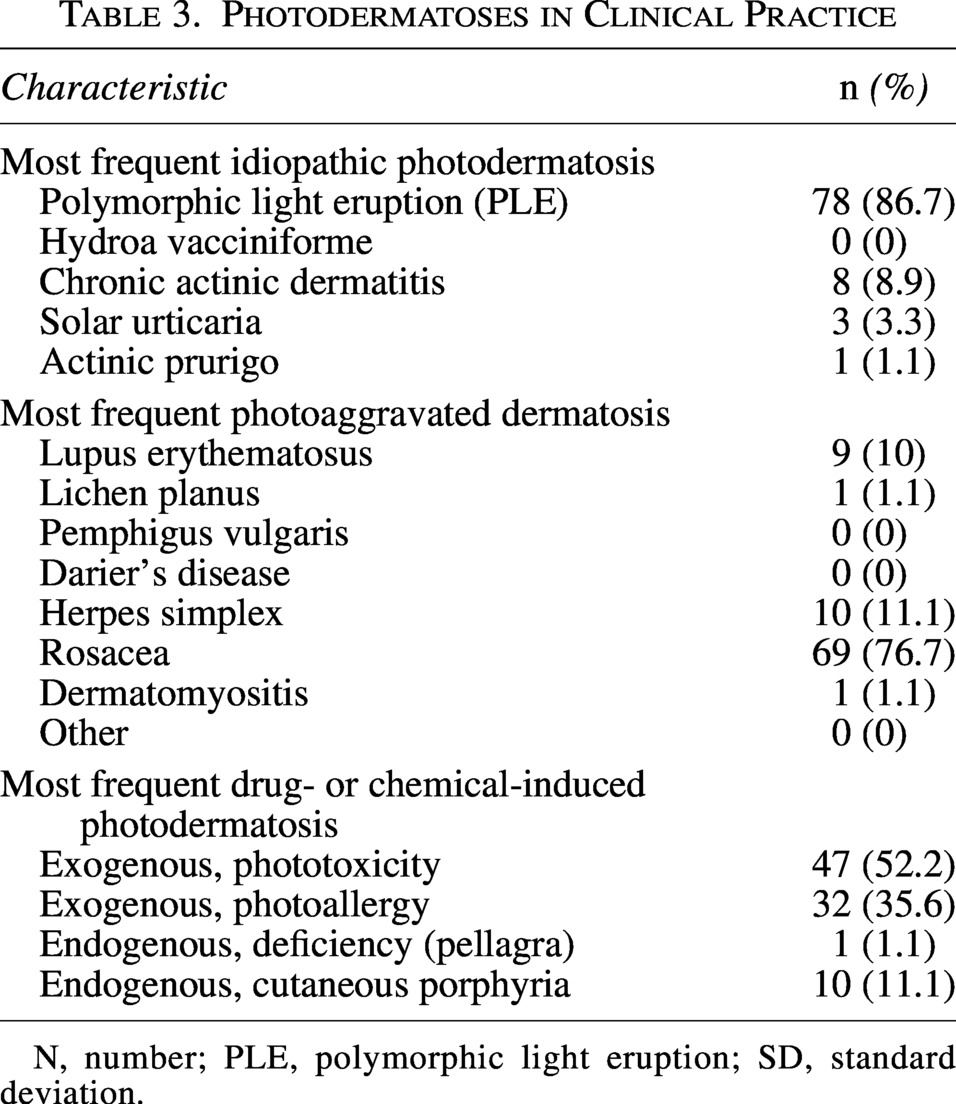
N, number; PLE, polymorphic light eruption; SD, standard deviation.
Prescription of oral and topical photoprotection for photodermatoses
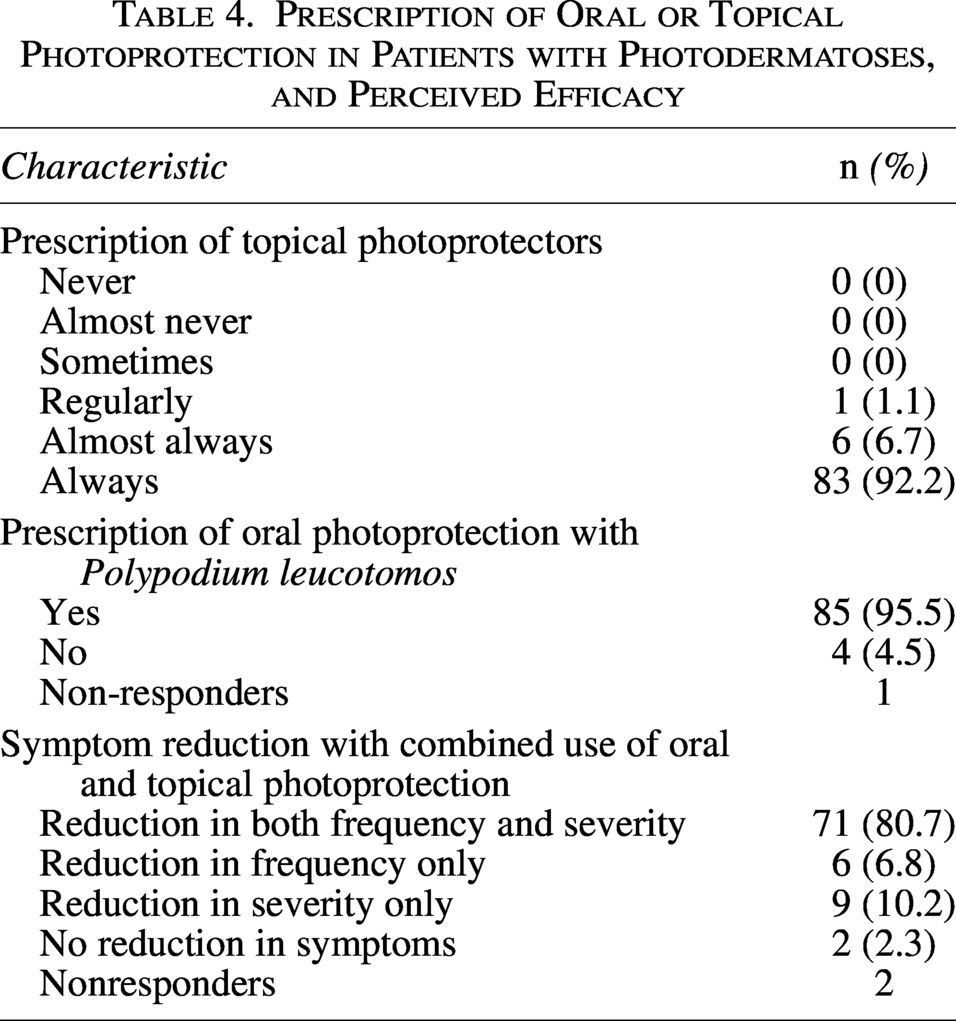
A total of 98.9% (89/90) of respondents reported prescribing topical photoprotectors always (92.2% [83/90]) or almost always (6.7% [6/90]) to patients with photodermatoses.
In addition, 95.5% (85/89) reported prescribing oral photoprotection with PL as an adjuvant. A total of 97.7% (86/88; 2 nonresponders) observed a reduction in patient symptoms when oral photoprotection was combined with topical photoprotectors, either in both frequency and severity (80.7% [71/88]), in frequency only (6.8% [6/88]), or in severity only (10.2% [9/88]) (Table 4).
Prescription of Oral or Topical Photoprotection in Patients with Photodermatoses, and Perceived Efficacy
Composition of topical photoprotectors prescribed for photodermatoses
Respondents reported that the most important characteristics of sunscreens for photodermatoses were UVA protection (95.6%) (86/90), VL protection (76.7%) (69/90), and the cosmetic properties of the product (67.8%) (61/90). A total of 54.4% (49/90) of dermatologists considered the presence of antioxidants or ectoin in the formulation to be important (Table 5).
Characteristics Considered Most Important in a Photoprotector for Patients with Photodermatoses
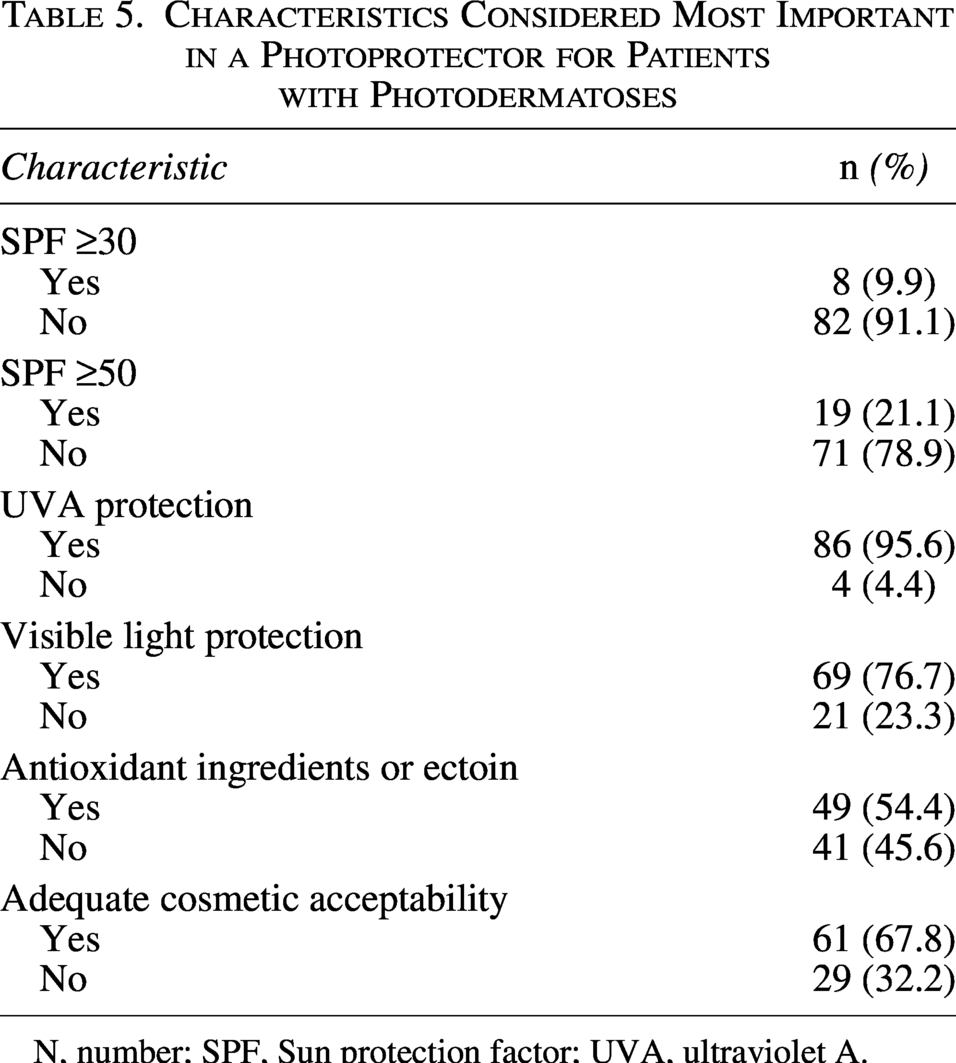
N, number; SPF, Sun protection factor; UVA, ultraviolet A.
Use of a BSSE in photodermatoses
A total of 90% (81/90) reported regularly prescribing a BSSE to patients with photodermatoses. Of these, 60.7% (54/89; 1 nonresponder) rated it as effective or highly effective in reducing symptoms associated with photodermatoses, while 32.6% (29/89) considered it moderately effective (Table 6).
Prescription and Estimated Efficacy of a Broad-Spectrum Sunscreen Containing Ectoin in Photodermatoses
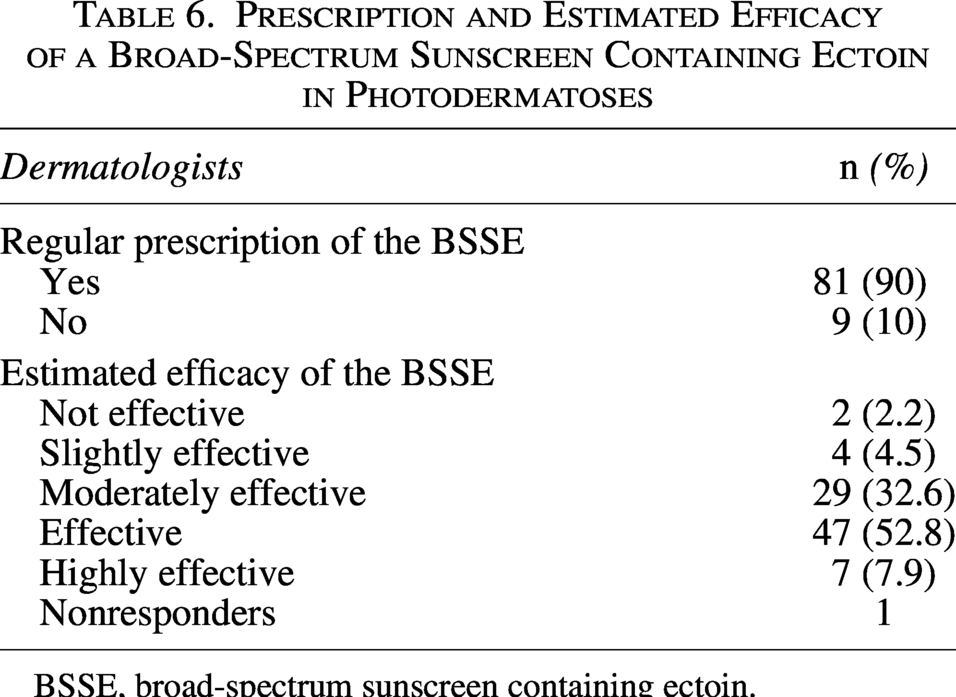
BSSE, broad-spectrum sunscreen containing ectoin.
Discussion
Photodermatoses can severely impact patients’ quality of life and may induce depression or anxiety disorders in a considerable proportion of cases. 14 PLE is the most frequent photodermatosis, with an estimated prevalence of approximately 20% in Europeans and 10 − 15% in North Americans. 15 This is consistent with the responses of the dermatologists surveyed in our study. PLE is characterized by a delayed-type hypersensitivity reaction to solar radiation. Its etiopathogenesis appears to involve oxidative stress and destabilization of keratinocyte membrane lipids, processes triggered by UVA radiation. 2 PLE is a chronic condition, and a recent study showed that after 20 years of follow-up, more than 70% of patients still had the disease. 16 This underlines the need for long-term follow-up of these patients and continuous reinforcement of photoprotection measures.
Photoprotection measures such as seeking shade, avoiding sun exposure during peak hours, wearing dark clothing that covers as much skin as possible, and using hats, sunglasses and topical photoprotectors are essential interventions in the management of photodermatoses. 17 However, studies on the efficacy of topical photoprotectors are limited. Most of the available evidence concerns the management of PLE,2,4–7 where the deleterious role of UVA radiation is crucial, as discussed above. 18 In addition, VL has also been implicated in many conditions.19–21 In our study, we found that most dermatologists considered UVA and VL protection to be the most important features when prescribing a photoprotector for photodermatoses, ranking well above the importance of simply ensuring a SPF ≥50. It is important to recall that physical filters such as titanium dioxide and iron oxides effectively protect against long UVA wavelengths and VL, 21 and thus sunscreens containing these filters should be recommended for patients with photodermatoses. Moreover, sunscreens should provide a UVA protection factor greater than one-third of the SPF, ideally approaching a 1:1 ratio. 3
Among the three most frequently cited characteristics considered important in photoprotectors was cosmetic acceptability, with the goal of improving treatment adherence. 22 This is consistent with studies recommending sunscreens with optimal galenic properties: pleasant texture, easy to apply and remove, and leaving no visible residue on the skin. In fact, “cosmetic elegance” was the most frequently cited positive attribute of sunscreens among consumers in one study, 23 and the most important factor for dermatologists when choosing sunscreens for themselves, according to a recent survey. 22
PL possesses multiple anti-inflammatory and antioxidant properties that have supported its use in a variety of dermatologic conditions, including pigmentary disorders such as vitiligo and melasma, as well as several photodermatoses.11–13,24–27 A recent study showed that supplementation with PL, green tea, and other antioxidants increased the minimal erythema threshold in volunteers. 10 In our study, almost all dermatologists reported prescribing oral photoprotection with PL for patients with photodermatoses, and most observed a reduction in symptoms when oral photoprotection was combined with topical sunscreens.
The majority of dermatologists in our study also reported regularly prescribing a BSSE and considered it effective in reducing symptoms. In a recent clinical trial, 15 patients with PLE applied this product to a segment of the trunk, leaving another segment untreated. The treated area was then irradiated with UVA (40–60 J/cm2). None of the patients developed PLE lesions in the treated area, whereas 13 of 15 patients developed lesions in the untreated area (p < 0.001). In addition, it effectively protected against UVA-induced erythema and pigmentation. 2 Notably, this product exhibits high UVA protection (UVA protection factor > 40) and contains ectoin, an innovative natural molecule that has been shown to protect against Langerhans cell depletion and UV-induced gene expression in keratinocytes. 28 It should be noted that ectoin is not exclusive to a single formulation, and topical photoprotective products containing ectoin are commercially available from different manufacturers.
Limitations and Strengths
This study has several limitations: it was an anonymous online survey, with a potential inclusion bias. Among its strengths, it should be noted that this is the first study to evaluate the prescription of oral photoprotection and topical photoprotectors for photodermatoses in routine dermatological practice, and it included a relatively large number of participants.
Conclusions
The management of photodermatoses can be challenging, and adequate photoprotection is the cornerstone of treatment. Nearly all surveyed dermatologists reported prescribing topical photoprotectors combined with oral photoprotection for photodermatoses and observed a reduction in symptoms with this approach. The most valued characteristics of topical photoprotectors were UVA and VL protection, as well as cosmetic acceptability.
Footnotes
Author Disclosure Statement
D.M.C. and J.P.C. have served as consultants for ISDIN Laboratories. J.D. works for ISDIN Laboratories.
Funding Information
This study was funded by ISDIN Laboratories.