
Abstract
Augmentative and alternative communication (AAC) includes methods and technologies to support communication and aid individuals with limited speech. There are many widespread misconceptions about AAC use, however, that can negatively impact how children with disabilities are taught in classrooms. In this article, we describe the main types of AAC systems and how they are used to promote child success. Then, we identify and dispel common myths about AAC use and provide evidence-based recommendations for practitioners to support children who use AAC in the classroom.
Keywords
“Importantly, professionals can dispel these myths by sharing their knowledge of AAC research with other professionals and with the families they serve.”
Approximately four million Americans with complex communication needs (CCNs) cannot rely solely on their natural speech to communicate, and thus rely on augmentative and alternative communication (AAC) strategies and systems to meet their daily communication needs (Beukelman & Light, 2020). AAC interventions and systems are designed to aid and support communication for individuals with little or no functional speech. AAC can increase the quality of life for individuals with a range of disabilities (Johnston et al., 2012).
Unfortunately, there are many widespread misconceptions about AAC that can negatively impact how children with disabilities are taught in classrooms. The beliefs educators hold about effective strategies and practices for supporting early language and literacy development are related to the approaches they enact to support children and children’s development of language and literacy skills (Piasta et al., 2020). Inaccurate beliefs can ultimately limit access to and use of quality learning opportunities, like use of AAC interventions and systems for young children. This is true despite the fact that research indicates that AAC can support young children’s communication, language, and social development (Ganz et al., 2012).
This article describes AAC and how it is used to promote child success across domains. Then we discuss common myths about AAC held by some educational professionals (i.e., teachers, speech-language pathologists, and other related service providers) to bring awareness to and counter these issues. Finally, to help educators re-envision current practices that may be influenced by the identified myths, we synthesize our own work and the research literature to provide research-based recommendations for educational professionals to support children who use AAC. Widespread understanding of the myths and realities of AAC is an essential step to move the field toward acceptance and adoption of AAC intervention and systems for individuals with CCN.
What is AAC?
AAC systems come in many forms, such as visual symbols, manual signs, communication boards, or computer programs (Beukelman & Light, 2020). There are two categories of AAC systems: unaided and aided. Unaided AAC does not require the use of technology (e.g., formal and informal sign language, gestures), whereas aided AAC involves the use of physical items or aids such as communication books and boards, as well as computers or tablet applications. Individuals may use different types of AAC in different settings or at different stages in development. Examples of common types of AAC are shown in Figure 1.
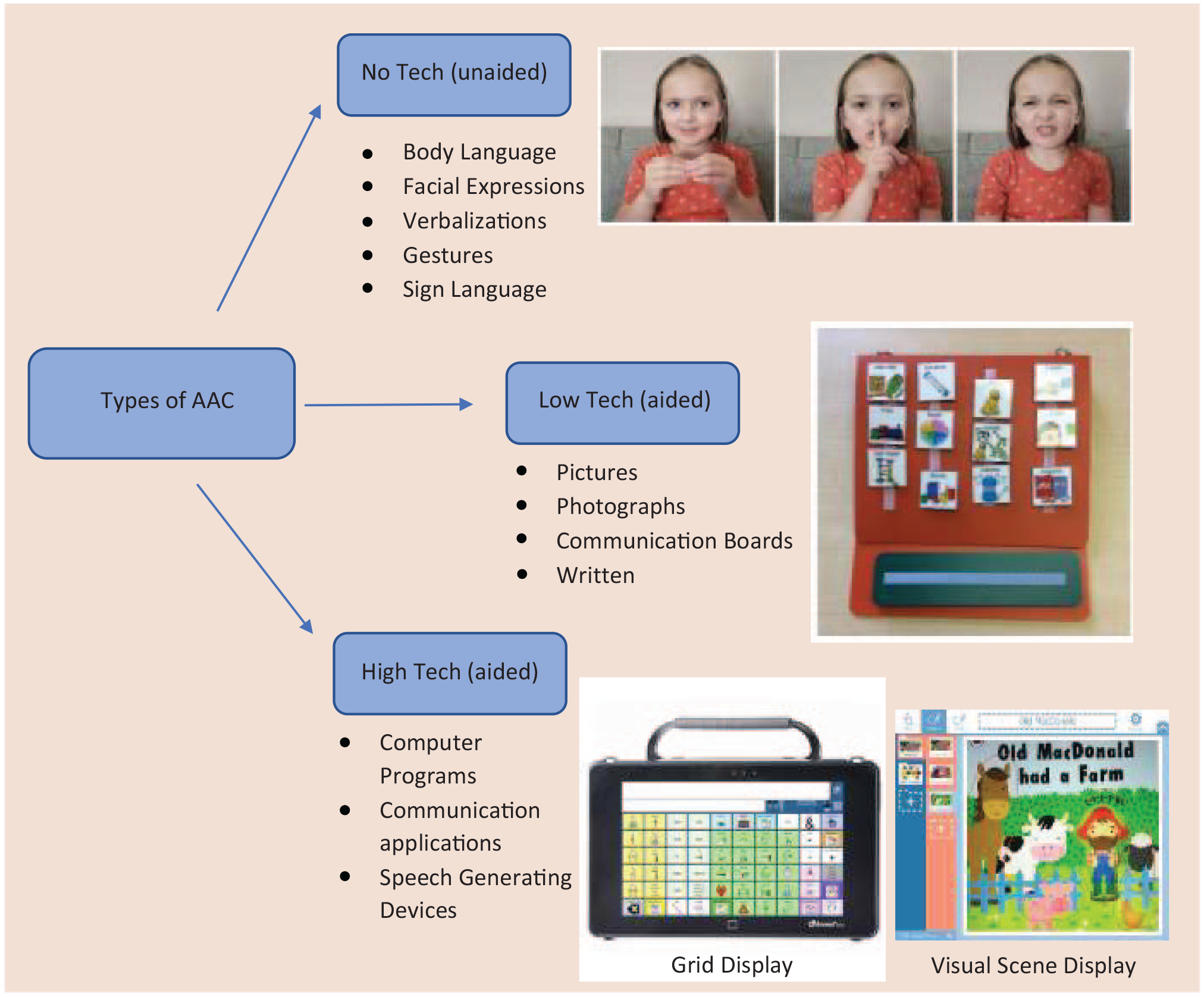
Types of AAC
AAC systems are used by individuals with CCN, including those with a variety of disabilities such as autism spectrum disorder (ASD) and intellectual disabilities (Beukelman & Light, 2020). AAC also includes intervention to support the skills needed to communicate using the AAC system; providing an AAC system is not enough to help a child learn to communicate with that system (Chung & Stoner, 2016). Early foundational work in this area suggests four core purposes of communication and the need for intervention to support these purposes: expression of wants and needs, transfer of information, social closeness, and social etiquette (Light, 1988). AAC interventions and systems provide children with limited speech ability to engage in these necessary types of communication. AAC, especially when implemented at early ages, allows children with CCN to maximize their communication, language and literacy skills, and social connections (Johnston et al., 2012).
Let us examine common myths some professionals, like educators and speech-language pathologists, may believe about children and AAC and the research evidence that dispels each myth. Dispelling these myths is an essential first step to promoting accurate and effective use of AAC to support young children’s success in language development, in school, and in life.
Common Myths
Myth 1: AAC Hinders Language Development
A common myth addressed in the literature nearly two decades ago is that AAC hinders language development (Romski, 2005). Despite the time that has passed since this myth was first addressed, many still believe that AAC will prevent a child’s innate desire to learn aspects of language, such as vocabulary and phonological awareness, or literacy, including alphabet knowledge, phonemic awareness, and print concepts. They believe the child will focus all of their energy on learning the AAC system, rather than learning language.
In contrast, research shows that AAC interventions and systems help children to develop language skills across a variety of domains (Romski et al., 2015). For example, AAC has been shown to improve both expressive and receptive language in children with ASD (Lal, 2010; Rose et al., 2020). Language growth is even more pronounced when peers participate in the communication process (Barker et al., 2013; Logan et al., 2017). AAC has also been shown to support literacy skills (Machalicek et al., 2010).
Myth 2: AAC Systems Discourage Speech Development
Another myth within the AAC literature is that using AAC systems will discourage children from developing speech (Millar et al., 2006; White et al., 2021). This belief is based on the idea that children will rely solely on their AAC system and will no longer use speech, which presumes that using an AAC system will be easier for the child than producing speech.
However, research shows that providing AAC intervention and systems does not inhibit the use of speech. In a meta-analysis (Millar et al., 2006), examining the impact of AAC use on speech production, the majority of included studies (89%) reported moderate gains in speech production for individuals using AAC. A recent systematic review (White et al., 2021) found that for children with ASD, AAC use did not result in decreased speech production. None of the participants showed a decrease in speech production. These findings provide promising evidence that AAC can support speech production in individuals with disabilities.
Myth 3: Young Children Are Unable to Successfully Use AAC
Another myth focuses on the belief that young children do not have the skills to be successful using AAC. Some argue that infants and toddlers lack the capability to communicate using AAC, given their burgeoning development (Davidoff, 2017).
However, research shows that very young children can be successful using both unaided (e.g., sign language) and aided AAC systems (e.g., speech generating devices); and that using AAC supports their communication development (Romski et al., 2015). Learning any language can be cognitively challenging. Learning to use AAC requires children to understand language structure, semantics, cause/effect relationships, joint attention, and more as they develop communicative competence (Light & McNaughton, 2014). Infants as young as 6 months have been able to successfully learn sign language to communicate their wants and needs (Rymanowicz & Cox, 2020). Evidence indicates that the earlier children are introduced to and supported to use AAC, the better the long-term communication outcomes will be for the child (Davidoff, 2017).
Myth 4: Children Who Use AAC Experience Social Challenges With Peers
Another myth is that children who use AAC will be isolated from their peers and unable to socialize effectively (Lal, 2010). The fear communicated by professionals is that the AAC will act as a barrier to developing relationships with peers.
Research findings indicate that AAC interventions can positively impact social skills. AAC use actually increases both the quality and quantity of social interactions of children with ASD and provides children with the ability to interact with others, including peers (Ganz et al., 2012; Lal, 2010). AAC gives children the tools and skills they need to learn to initiate and respond to conversations with peers and build relationships using language (Barker et al., 2013). Furthermore, peers can be important communication partners when implementing AAC interventions (Bourque, 2020). Peers can help model and teach the AAC system, use the AAC system to converse with the child, and encourage social interaction using the AAC systems and strategies (Thiemann-Bourque, 2012). When children have peers who use AAC strategies and communicate with them using their AAC system, they experience significantly more language growth than children who do not have peer support (Barker et al., 2013).
Myth 5: Prerequisite Skills Must be Met Before AAC Can Be Introduced
Another common myth is that children need certain skills to be successful using AAC. Commonly cited “necessary skills” include fine motor mastery, receptive communication skills, understanding of cause-and-effect, and left-to-right visual tracking, among others (Barker et al., 2013). This harmful myth is perpetuated by some educational and related service professionals.
In contrast, research shows that children can be successful using AAC without demonstrating prerequisite skills (Beukelman & Light, 2020; Romski et al., 2015). Using the AAC system is educational. Studies related to AAC note that even young children develop visual motor, cause and effect, language processing, and language skills as they use AAC systems (Maue, 2022). AAC technology has advanced significantly, and various systems are available for children with a variety of needs. Examples of AAC technology are discussed below and available in Figure 1. Explicit pre-service and in-service training related to AAC interventions and systems is necessary to combat this myth (Moorcroft et al., 2019).
Teaching Recommendations
Despite the widespread myths that persist within the field, ample research recognizes AAC intervention and systems as beneficial for promoting children’s communication, social interactions, and language and literacy development. One way to alleviate the impact of the myths discussed above is to encourage professionals to enact the following research-based recommendations for practice. These recommendations—derived from our own work and the research literature on effective AAC use—ensure educators and support professionals have access to tangible strategies they can use to make manageable and meaningful adaptations to their classroom environment and instruction in support of children using AAC.
Recommendation 1: Use Visual Supports in the Classroom
For many children with disabilities, visual information is easier to process than written or oral communication (Vaz, 2013). Visual supports can help children with disabilities process information, anticipate changes in the routine, and identify their preferred activities. Visual supports can also reinforce symbols used within the child’s AAC system. Visual supports can include a variety of symbols such as objects, photographs, or drawings. They include first-then boards which often support task completion or social stories which are used to support the development of social and life skills (Gray, 2022; Rattan & Wrightington, 2020). In addition, Visual Scene Displays (VSDs), a type of AAC technology that provides a photograph of a scene familiar to the child with programmed words/phrases corresponding to the areas within the scene (see Figure 1 for an example of a VSD), have been shown to promote language and vocabulary development, peer relations, and communication skills (Laubscher et al., 2020). Educational professionals can draw attention to visuals throughout the day to help children understand classroom routines, keep children engaged, and support their learning. In instances where children also have visual impairments, objects and tactile supports can be used in addition to or in lieu of visual supports (Roche et al., 2014).
Marcus is crying after nap time and continually pointing to [home] in his AAC system. His teacher, Ms. Willis, guides Marcus to the visual schedule they have in the classroom and uses the photographs to clarify what is going to happen before he goes home. She points to each image as she explains: “We will eat a snack [snack], then have free play [free play] time inside, and then go outside to play [outdoor play] before you go home. Then points to [home] [later] in his AAC system and reassures him.
Recommendation 2: Use Evidence-Based Strategies to Support AAC Interactions
Extensive research exists to guide professionals in setting up successful AAC interactions. Table 1 provides the steps outlined in common AAC interventions. Although these evidence-based strategies differ in detail, they share common elements such as: preparing the environment, engaging the child, waiting for their response, and modeling AAC. Preparing the environment includes preparing activities that motivate the child and ensuring the AAC system has the required vocabulary to support the child’s communication during the activity (Douglas & Gerde, 2019). Engaging the child occurs best when professionals provide the child with lots of opportunities to communicate by asking questions, providing choices, and commenting about the activity (Douglas & Gerde, 2019). Professionals should also wait 5 to 7 seconds after providing a communication opportunity to ensure ample time for the child’s communication (Sun et al., 2022). In addition to preparing, providing opportunities, and waiting, the professional can model AAC while they talk to show the child how to use their system (Biggs et al., 2019). Modeling provides the child with clear examples of how to navigate, find vocabulary, and communicate using their AAC system. Using AAC strategies consistently will provide the child with the support needed to learn to use their AAC system and will help to dispel AAC myths.
Examples of Evidence-Based Intervention Strategies for Implementation of AAC
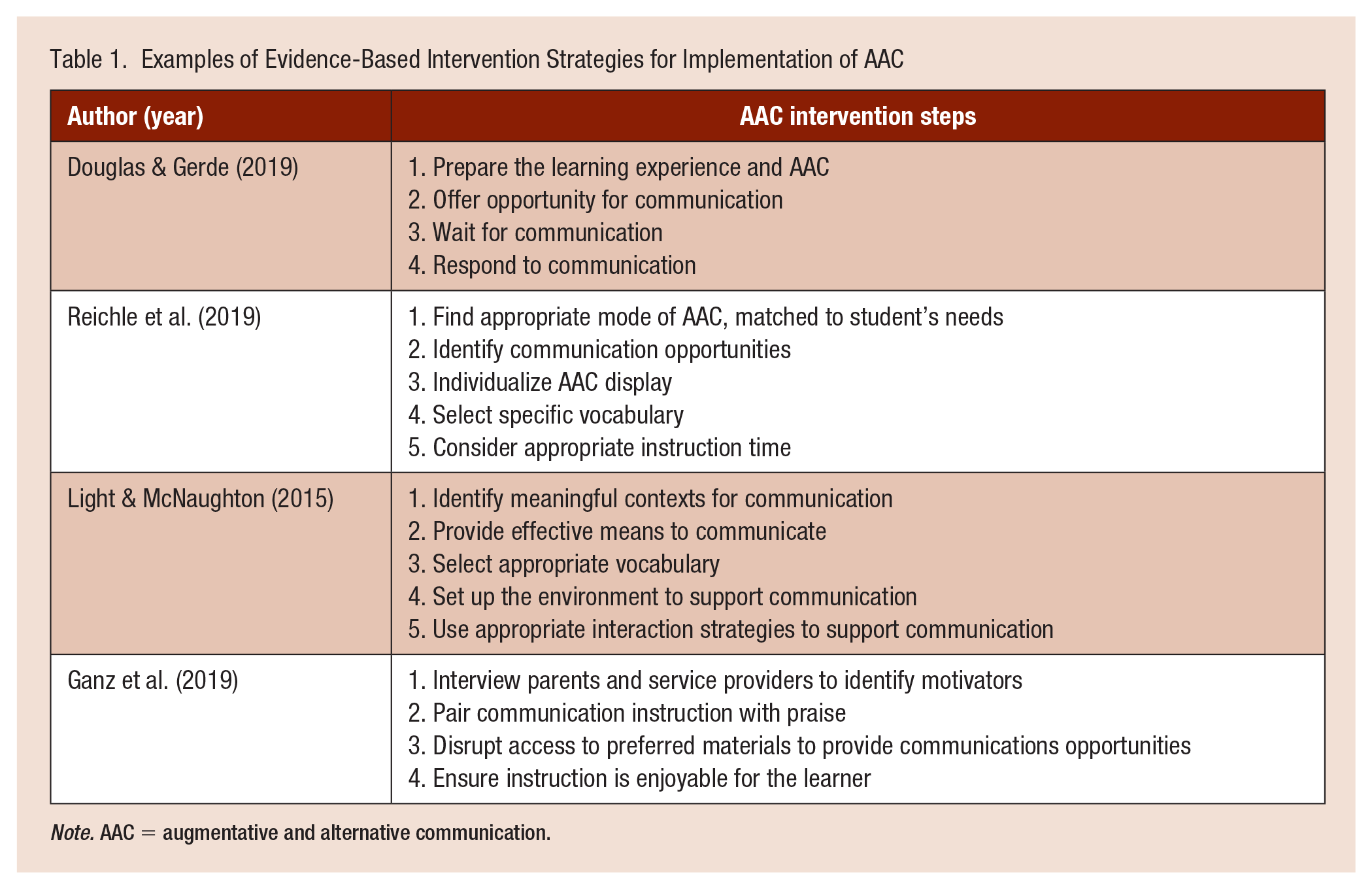
Note. AAC = augmentative and alternative communication.
Mrs. Smith spends some of her prep time reading a recent article about an evidence-based AAC implementation strategy (e.g., Douglas & Gerde, 2019). She forwards this article to her paraeducators and assistants and they discuss and practice the strategy in their next meeting. During this meeting, they plan how each educator will use the new strategy with particular children the following week. In the next planning session, they reflect on how the new strategy is working for each child and discuss continued implementation.
Recommendation 3: Utilize Peers in AAC Interactions
Communication partners are essential for children who use AAC. Involving peers in interactions using AAC interventions and systems significantly increases language growth, as it provides children more opportunities to communicate (Barker et al., 2013; Logan et al., 2017). In addition, using AAC with peers increases the social skills of the child who uses AAC (Ganz et al., 2012; Lal, 2010). Providing peer supports by matching a peer with a child who uses AAC can promote child development across a variety of developmental domains, including: social/emotional, cognitive, and language development. Peer supports can be tailored to each classroom. For example, a child who uses AAC may be matched with a peer who does not use AAC. Professionals can instruct the peer to encourage communication from the child who uses AAC a few times throughout the day, by asking questions such as: “What do you want to play with next?” or “What did you bring for lunch today?” or providing comments such as: “I like playing with the blue car” or “Your sandwich looks yummy.” The peer will benefit from the interaction in a variety of ways, including building friendship, learning acceptance, and increasing community involvement (Yu et al., 2015). In addition, the child who uses AAC will gain additional opportunities to develop communication skills and friendships with peers.
Thiemann-Bourque (2012) provides some helpful tips professionals can use to guide peers in supporting children who use AAC by using the “stay-play-talk” strategy. “Stay” encourages the peer who does not use AAC to stay with the child who uses AAC and sit close to them. “Play” encourages the peer to play with the child, including sharing and taking turns. “Talk” encourages the peer to talk with the child using words (verbal language), pictures (unaided AAC), and computer applications (aided AAC; Thiemann-Bourque, 2012). It is important to help the peer understand the importance of waiting for a response from the child who uses AAC. At first, using a stopwatch or timer can be helpful for this process.
Mr. Johnson has noticed that Carla and Mary spend a lot of time together in the classroom. To communicate with others, Carla uses an iPad with a communication application. Mr. Johnson explains to Mary how Carla communicates and teaches Mary the Stay, Play, Talk strategy. As they practice the steps, Mr. Johnson intentionally models waiting for a response. He says: “Carla is preparing her message using her iPad, so I am waiting. Then I will respond after she communicates her message. What do you want to say to Carla?”
Recommendation 4: Ensure AAC Training Is Provided to Practitioners
Successfully implementing AAC in the classrooms requires all professionals to be well-versed in each unique AAC system being used. This requires training for all professionals supporting children who use AAC so they can effectively use and implement AAC strategies such as modeling the AAC system for the child. Research has identified a significant positive association between the amount of training teachers received on supporting students using AAC and the communication abilities of their students (Andzik et al., 2018). Professionals supporting young children with CCN should seek out regular professional development opportunities to ensure they understand the AAC systems being used in their classrooms and gain knowledge of AAC interventions. This might be done through targeted training from speech-language pathologists in their school, AAC device manufacturers, or through shared professional development with educational teams who support children who use AAC.
Ms. Lopez has four children in her classroom who use AAC, but she and her staff have limited knowledge about their AAC systems. She has invited the speech-language pathologist to help train her and her staff on the AAC devices during an in-service day. During the training, Ms. Lopez and her paraeducators all learn how each AAC system is used, practice using each device, and role-play using the AAC systems with each other. They make a plan for using AAC with each child the next week and invite the speech-language pathologist to observe and provide feedback on their use to help improve their interactions using AAC.
Conclusion
Although many myths exist about the use of AAC which can impact how professionals interface with AAC in the field, research dispels these myths and highlights the benefits of AAC intervention and system use in childhood. Counter to the five myths about AAC use identified in this article, the research evidence is clear that (a) AAC improves language and literacy skills; (b) AAC improves communication and speech, (c) even very young children can be successful using a wide variety of AAC supports including unaided and aided formats, (d) AAC enhances the quality and quantity of children’s social interactions, which helps children build relationships with peers and adults, and (e) prerequisite skills are not needed but rather developed as children engage with AAC. Educational professionals can successfully promote children’s use of AAC by using visual symbols in the classroom, employing evidence-based strategies to set up AAC interactions, creating a peer system to encourage communication, and ensuring all members of the teaching team are familiar with AAC approaches used in the classroom. Importantly, professionals can dispel these myths by sharing their knowledge of AAC research with other professionals and with the families they serve.
Footnotes
Conflict of Interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Author Biographies
Emily Jensen is a doctoral student at Michigan State University. Her research focuses on holistically supporting children with disabilities and their families in medical and educational settings. She utilizes mixed methods research to understand the experiences of children and their families, as well as professionals working with this population, with goals to improve care systems and quality of life.
Sarah N. Douglas, PhD is an Associate Professor at Michigan State University. Dr. Douglas conducts research that focuses on communication partner training to support children who use augmentative and alternative communication (AAC). She has implemented AAC interventions with teachers, paraeducators, parents, and siblings.
Hope K. Gerde is a professor at Texas A&M University. Her research focuses on the early literacy development, particularly early writing development, for young children who are marginalized and effective approaches to teacher professional learning that promote high-quality teaching practices.