
Abstract
Infants and toddlers with significant support needs (SSNs) receive early intervention services under Part C of the Individuals with Disabilities Education Improvement Act. These services occur in a variety of children’s natural environments, which may include their home, child care, community parks, extended family members’ homes, etc. It is important that early interventionists who provide developmental services to children with SSNs and their caregivers are equipped with strategies they can use to promote meaningful inclusion of this unique population. This paper illustrates what high-quality inclusion can look like and provides strategies that early interventionists can implement with various caregivers in a child’s life.
Keywords
“Infants and toddlers with SSNs can be meaningfully included in all natural environments, including homes, child care programs, and community activities.”
Winston is a 23-month-old with a traumatic brain injury (TBI) who lives with his mom and dad, Ellie and Jarod, plus his 5-year old brother. Due to his TBI, Winston has extensive medical and developmental needs, such as using a tracheostomy tube to breathe and a gastrostomy tube for feeding. Winston communicates his wants and needs through gestures, sounds, and eye gaze and can move independently on the floor by rolling. His family is helping him gain strength in his legs by doing daily exercises they learned from his early intervention (EI) physical therapist. In addition to physical therapy, Winston receives occupational therapy and special instruction through EI. The focus of their sessions is on helping Winston’s family develop new skills they can use in their everyday life to help Winston be as independent as possible.
Individuals with significant support needs (SSNs) refers to the small percentage of the population who need extensive supports in multiple domains (e.g., health, physical, and communication) to facilitate their inclusion in society, and who without these supports would likely experience exclusion, segregation, discrimination, and/or the removal of rights (Giangreco et al., 2020; TASH, 2022). Infants and toddlers with SSNs qualify for EI under Part C of the Individuals with Disabilities Education Improvement Act (IDEA) (2004), which aims to minimize the risks listed above. These services are provided by interventionists (EIs) who represent a variety of disciplines such as speech-language pathology, physical therapy, occupational therapy, special education, and social work. EI differs from intervention provided to school-aged students, as a key focus is to help strengthen families’ capacities to support their children’s development within their everyday lives (IDEA, 2004). In addition, school-age children who receive special education services have an individualized education program (IEP) that lists their goals and services, whereas children in EI have an Individualized Family Service Plan (IFSP). Although both the IEP and the IFSP describe outcomes for children and a plan for how desired outcomes will be reached, an IFSP is more family-centered. The IFSP includes child goals and family goals, which are embedded in families’ everyday routines. In addition, the strategies in the IFSP are written so anyone can implement them, including the child’s family members.
IDEA (2004) requires that Part C services are provided in the natural environment; that is, settings in which same-age peers without disabilities typically participate (e.g., home, child care, parks, libraries). According to experts, natural environments are more than a place where services occur; they also are the experiences and interactions within these settings (Dunst et al., 2000; Jung, 2003; Workgroup on Principles and Practices, 2008). The natural environment is likened to inclusion, which is also not only about where services occur, but how they are provided (Beneke et al., 2019; Odom et al., 2011). Inclusion is not just a placement in a typical setting (e.g., general education classroom) but rather, involves intentional action and the use of evidence-based strategies so that all children are supported, welcomed, and valued. Infants and toddlers with SSNs can be meaningfully included in all natural environments, including homes, child care programs, and community activities (Guralnick & Bruder, 2016).
The Division for Early Childhood and the National Association of the Education for Young Children (DEC/NAEYC, 2009) released a joint position statement highlighting three essential components of inclusion: access, participation, and supports. Access is achieved when children can physically enter and take part in their natural environment. Participation involves children’s active engagement with peers and adults during activities and routines. Finally, a system of supports should be in place for adults to help them effectively implement inclusion (DEC/NAEYC, 2009). Given that access and participation for children with SSNs require ongoing, individualized, and intensive interventions (Giangreco et al., 2020), it is important to consider how EIs promote children’s meaningful inclusion across settings. Moreso, EIs must act on systems of inequity that disproportionately exclude multiply-marginalized children with SSNs (e.g., children of color with SSNs) from their natural environment (Love & Beneke, 2021). This paper illustrates what high-quality inclusion looks like for infants and toddlers with SSNs and includes descriptions of strategies aligned with the three components of inclusion, interwoven with strategies to purposefully include multiply-marginalized children. By increasing one’s awareness of these components and strategies that address them, readers will be able to promote the meaningful inclusion of all children with SSNs in natural environments.
Access
During an EI session with Tara, the special instructor, and Barb, the occupational therapist, Ellie confides that she is having a difficult time managing all of Winston’s care while Jarod is working. She wishes that she could go back to work too, as she misses her colleagues and the satisfaction she received from work. Barb asks if Ellie and Jarod have considered enrolling Winston in a child care program, and Ellie responds that she does not think any program could manage his needs. Barb asks Ellie if she would like to spend some time during next week’s session discussing child care options and Ellie confirms her interest. Barb and Tara commit to try to identify child care programs in the community that welcome children with disabilities, and Ellie says she will discuss her family’s goals and concerns about child care with her husband before their next session. The following week, the team discusses their goals and concerns related to Winston going to child care, and Barb takes detailed notes which she adds to an ongoing shared document of the team’s concerns and priorities for Winston (see Figure 1). The team works together to draft a plan (see Figure 2) to address Winston’s needs at child care that they can share with his teachers. Barb and Tara share the contact information of the child care programs that they know provide high-quality care for children with SSNs.

The Team’s Shared Document.

Winston’s If-Then Emergency Plan for Child Care Teachers.
The vignette illustrates how it can be difficult for families of children with SSNs to access environments that other families might access more easily. In fact, research shows that families of young children with disabilities face barriers accessing high-quality child care (Weglarz-Ward & Santos, 2018). Families of children with SSNs also may experience barriers within community settings such as the grocery stores, parks, and recreational programs. For example, going to the grocery store can pose a challenge to families of young children with limited mobility, given that child seats in standard shopping carts do not provide trunk support. Likewise, caregivers of children with disabilities have reported that playgrounds and recreational facilities are not accessible to their children due to a lack of adapted equipment (Stanton-Chapman & Schmidt, 2018). According to DEC/NAEYC (2009), a child has access to an environment when it does not contain physical or structural barriers and when it includes assistive technology that facilitates the child’s access. Returning to the example of grocery shopping, an adapted shopping cart with a 5-point harness (a low-technology adaptation), could eliminate this physical barrier and offer more families access to grocery stores. Structural barriers are ingrained within social systems and may cause certain groups of children to be excluded from natural environments (e.g., disproportionate expulsion rates of Black and Brown children, limited access to social services due to immigration status, communication barriers due to language differences; Love & Beneke, 2021). To address structural barriers, EIs can advocate with families and children, ground their work in inclusion that addresses all identities (i.e., not just ability), and use resources that reduce barriers (e.g., interpretation software) (Beneke et al., 2019). Table 1 lists six strategies (A1– A6) that EIs can use to promote access for children with SSNs across environments, which are illustrated in the vignette and described below.
Strategies Aligned With Components of Inclusion.
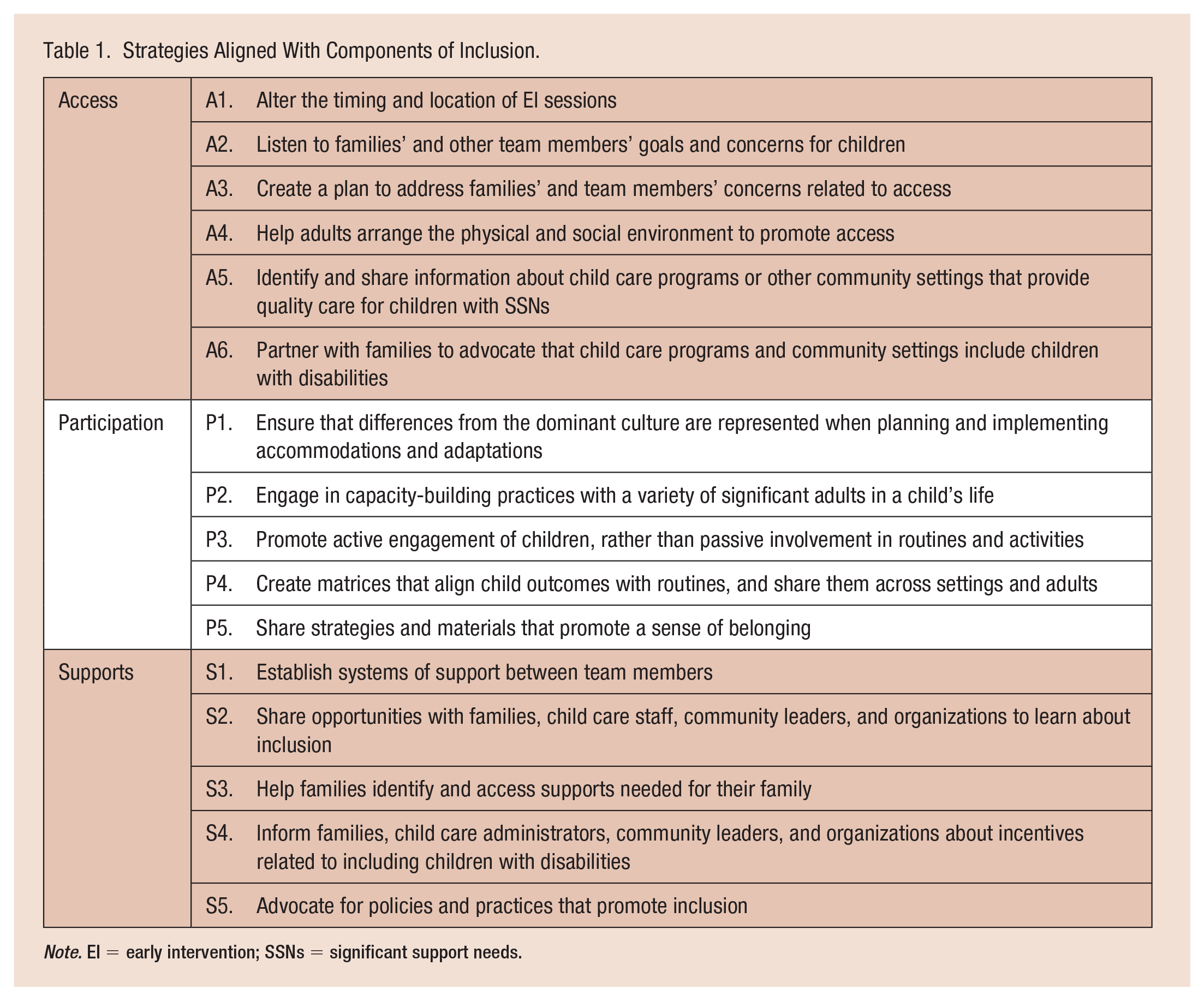
Note. EI = early intervention; SSNs = significant support needs.
Though it may be a common practice for EI sessions to occur in the same location and at the same time each week, this is not required. In fact, several EI experts suggest that sessions occur at times and places that are most meaningful to families (McWilliam, 2010; Workgroup on Principles and Practices, 2008), which may change regularly; thereby, indicating the importance of altering the timing and location of sessions (A1). For example, returning to the vignette, Winston’s EIs might alter the timing and location of their sessions so that they vary within settings (e.g., one week during a meal and the next week during play time) and across settings (e.g., one week at home and the next at the library). When EIs provide services in a variety of natural environments, they can influence the child’s access within each of the targeted routines and settings.
It is important that EIs understand families’ and other team members’ goals and concerns so they can help address barriers related to children’s access (A2). In the vignette, Barb and Tara learned of Ellie’s concerns about Winston’s access to child care because of the rapport they had developed with her, by engaging in authentic conversations, and by listening to her priorities. Then, they intentionally addressed Ellie’s concerns by developing a plan with her (A3). Another way that EIs can help support access is ensuring that the environment (both the physical and social environment) provides children with SSNs with access to the same routines as their peers (A4). For example, if adults are intentional and planful in their scheduling for all children, then those with feeding tubes, like Winston, can sit at the table and receive their feedings during family and/or child care mealtime, rather than being excluded from meals because their feeding schedules do not align with the group meal or snack.
In the vignette, the EIs were able to identify child care programs that welcome children with disabilities (A5); however, this may not always be the case given that child care programs differ from public schools, as they are not required to serve children with disabilities. Although Title III of the Americans with Disabilities Act requires that child care programs grant equal opportunity to children with disabilities, some programs may not accept children with SSNs as their needs can be considered more extensive than is “reasonable” for the staff to accommodate, alleviating the program of their ADA obligation (U.S. Department of Justice: Civil Rights Division, 2020). EIs can help families advocate for their children’s access to child care by discussing ADA requirements, going with families to initial and recurring meetings at child care programs (Beneke et al., 2019), and informing child care staff of supports related to including children with disabilities (see “Supports” section of this paper). Due to structural barriers, not all families (including those with and without young children with disabilities) have access to child care or other community-based settings due to cost, transportation, or work schedules; therefore, it is important that EIs help families navigate these systems and find placements that match their unique circumstances (A6).
Participation
Before Winston’s first day of child care, Ellie and Jarod train his teachers to do the medical tasks he requires (i.e., gastrostomy tube feeding, suctioning his tracheostomy tube, inserting his tracheostomy tube) and discuss his If/Then emergency plan (Figure 2). They also ask Tara and Barb to do their joint session in Winston’s classroom during his first week so they can share intervention strategies with his teachers. When Tara and Barb arrive, the assistant teacher, Britni, and lead teacher, Aymen, invite Tara and Barb into the classroom. Tara asks Aymen how things are going with Winston, while Britni leads the children in a song. Aymen shares that he is an easy-going child and that his medical needs are not as difficult to manage as she initially thought; however, she is not sure how to help him engage in their typical routines. She draws their attention to Winston, who is sitting in a bouncer while the other children jump around and do the hand motions to a song. Tara offers to demonstrate how Winston can participate in singing songs, and Aymen accepts the invitation. Tara helps Winston out of the seat and props him up on her knee so that he is in an upright position next to his peers, facing Britni. She scaffolds his ability to do the hand motions by providing support under his elbow, which enables him to clap his hands. Aymen is surprised by how much Winston can do on his own, and Tara invites her to practice the strategy. Afterwards, Tara praises Aymen for helping Winston become involved in music and offers suggestions for age-appropriate supports (e.g., adapted chairs) they can use instead of a baby bouncer.
As illustrated in this vignette, just because a child has access to a setting or routine, does not necessarily mean they can actively participate. Full participation in natural environments occurs when infants and toddlers are provided with individualized adaptations and accommodations that facilitate their engagement with peers and adults, and within age-appropriate activities (DEC/NAEYC, 2009). Five strategies (P1–P5) that EIs can use to promote the participation of children with SSNs are listed in Table 1 and described next.
Adaptations and accommodations should value differences from dominant expectations and routines (Love & Beneke, 2021). In other words, rather than reinforcing dominant conceptions of ability, behavior, or speaking, EIs should promote children’s strengths and culture when planning and implementing adaptations and accommodations (P1). EIs may do this by collaborating to understand families’ expectations for routines rather than imposing what EIs believe routines should look like, or by using greetings and other common words in a child’s native language when communicating with them and their families.
EIs also can influence a child’s participation in their natural environment by employing capacity-building practices with various caregivers (P2). These practices encourage the active participation of caregivers, focus on strengthening caregivers’ knowledge and skills, and help caregivers develop new knowledge and skills (DEC, 2014). Implementing capacity-building practices with caregivers of young children with SSNs has been effective for improving outcomes for both caregivers (e.g., responsiveness, use of strategies) and children (e.g., motor and communication skills) (Chen et al., 2007; Ciupe & Salisbury, 2020; Salisbury et al., 2018; Salisbury & Copeland, 2013). In the vignette, we illustrated how Tara engaged in one capacity-building practice (coaching) with the child care teacher; Table 2 includes descriptions of additional capacity-building practices that are commonly used in EI. Scenarios are provided on how each can be used to promote the participation of a child with SSNs. Noteworthy, Tara engages in coaching with a variety of important people in Winston’s life, such as his parents, sibling, grandmother, and even other EIs. She individualizes her approach based on each of their experiences, knowledge, skills, and preferences. When EIs engage in capacity-building practices with a variety of individuals, more people can develop the necessary skills to support the child, which in turn, promotes the child’s learning and development.
Capacity-Building Practices With Examples.
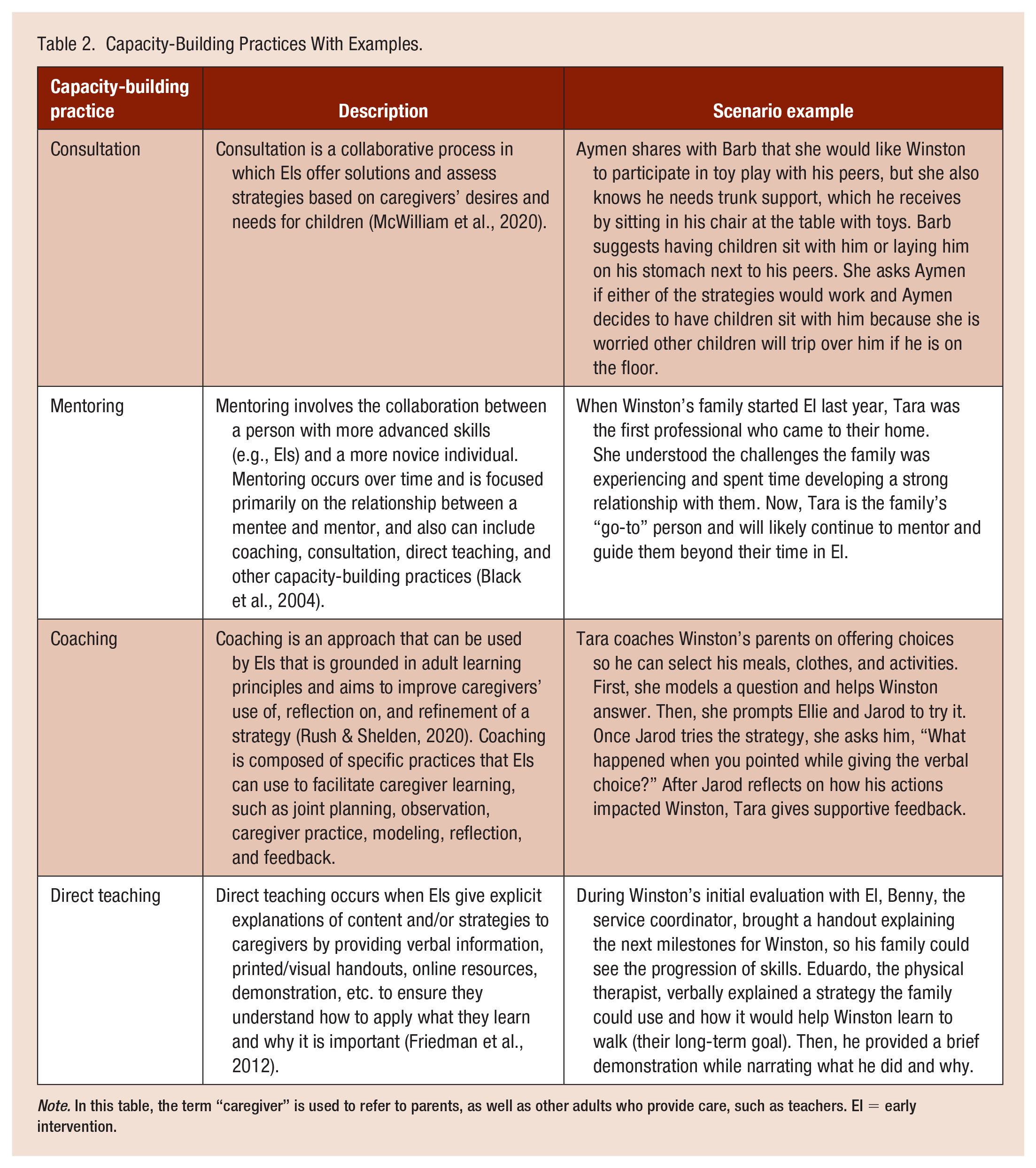
Note. In this table, the term “caregiver” is used to refer to parents, as well as other adults who provide care, such as teachers. EI = early intervention.
In the vignette, Aymen learned how to help Winston actively, rather than passively, engage in a music activity (P3). EIs can promote the active engagement of children with SSNs in other routines as well. For example, EIs can encourage the participation of children with feeding tubes during meals by recommending that teachers and other caregivers give them play food, utensils, and/or food approved by their doctor. As another example, EIs can help caregivers identify accommodations that enable children with SSNs to participate in chores and classroom jobs like their same-age peers, rather than repeatedly offering them an easy job, or no job at all, due to their disability. Another way EIs can promote the participation of children with SSNs is to work with the team to create a matrix of child outcomes next to everyday routines in which they can be incorporated (P4), which can be shared across team members and settings to support generalization and ensure that multiple and varied opportunities to participate are provided. Caregivers of children with SSNs have reported the benefits of learning to embed intervention in their typical routines and intentionally planning and documenting this process (Salisbury et al., 2018). A matrix is a planning tool that encourages different people to work on the same skills across various parts of the day; it provides a visual reminder of the child’s goals and it promotes high expectations for children with SSNs. EIs can develop a matrix (see Figure 3) or use an existing one, such as the Outcomes Routines Matrix developed by McWilliam (2020).
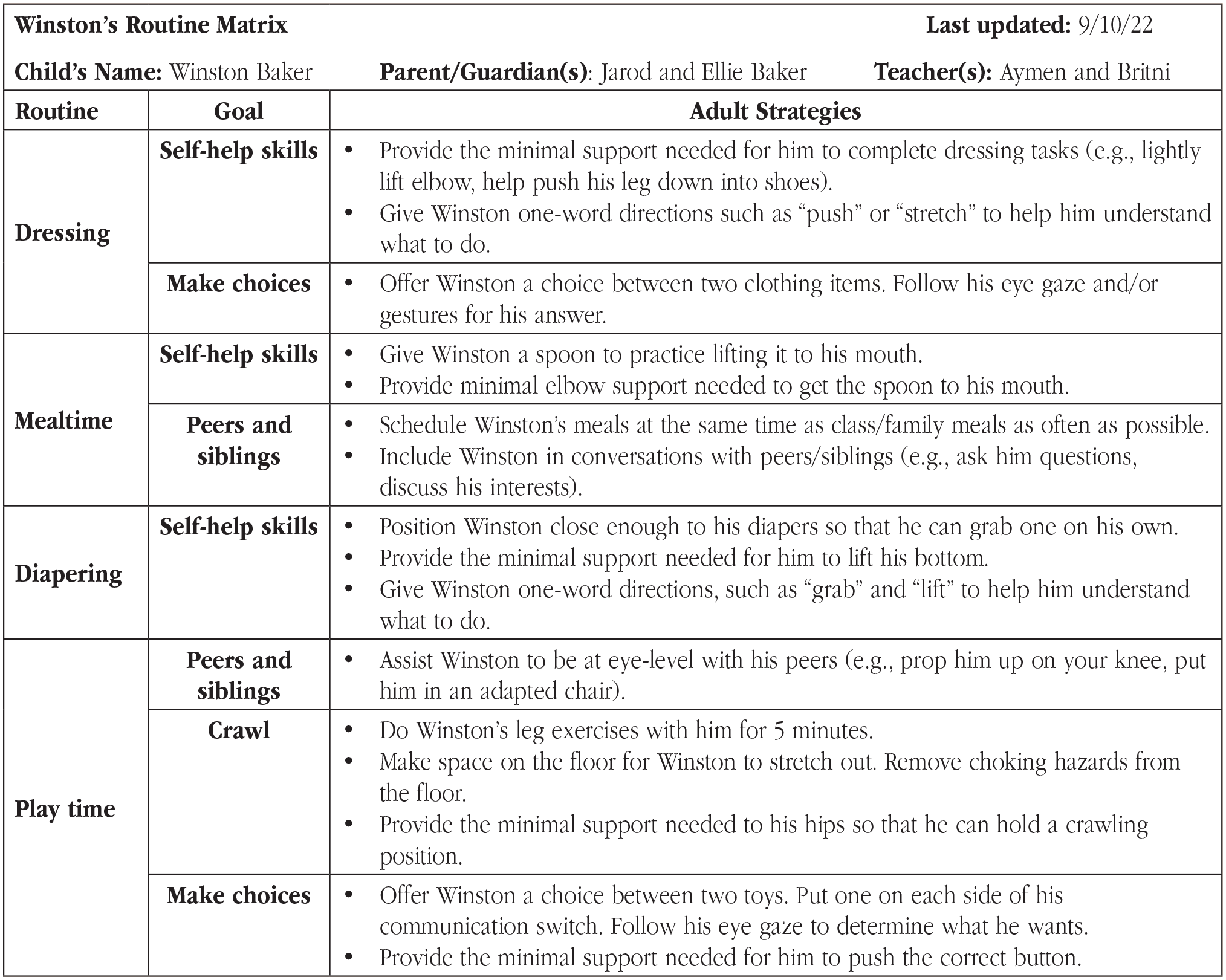
Winston’s Routine Matrix.
Finally, participation involves children with SSNs feeling a sense of belonging within their natural environments (P5). In the vignette, Tara helped establish that Winston belongs with his peers and that he deserves age-appropriate supports. By sharing this perspective with the teacher, Tara reinforced a conversation she recently had with Ellie, in which she encouraged the family to replace infant materials with age-appropriate ones that serve the same function (e.g., replace baby teethers with oral motor tools), and to reinforce to others that Winston is a capable toddler and not a “baby.” EIs also can affirm the use of adapted materials for all children in a setting by allowing other children to use adapted materials, which helps reduce the stigma that can emerge when one child uses different materials (Parkalian, 2021). For instance, another toddler in Winston’s child care class may notice him using his yes/no switch to make choices. Tara can encourage Aymen to let Winston’s peer use the yes/no switch to make choices too, so they can share the experience. As another example, adults can let all children practice cutting using adapted scissors. Other ways EIs can promote a sense of belonging for a child with SSNs is by promoting the use of materials that include people with disabilities, (e.g., toys, books, posters, curriculum) and by encouraging caregivers and teachers to talk to children about similarities, differences, disabilities, and supports. For example, a child care teacher can read books that include pictures of children with disabilities and have conversations about each person’s unique strengths and commonalities (e.g., “Winston likes to swim like Susan does in Susan Laughs. Who else in our class likes to swim?”) (Willis, 2000). A sense of belonging also applies to children’s other identities, such as race or gender. Thus, these conversations should include discussions about other differences that young children notice as well (Lalvani & Bacon, 2018). By promoting a child’s sense of belonging across settings, EIs can help eliminate social stigmas related to disability and differences, and promote a more inclusive society (Beneke et al., 2019).
Supports
When Winston entered the EI system last year, his service coordinator helped the family develop a Care Map of their support systems to highlight the importance of various individuals in his life (see Figure 4). The Care Map highlights who is on the team, their role, and how to contact them, which is helpful for the family as well as the other team members. Winston’s teachers received a copy of the Care Map when they learned he would be in their classroom. Recently, Aymen reached out to Winston’s physical therapist, Eduardo, because she wanted ideas on how to help Winston crawl (instead of roll) across the floor. Eduardo shared a video with Aymen that demonstrated a technique she could use to facilitate skill development, and then put the link in the shared document (Figure 1) so that other team members could see the same technique. By sharing the strategy across individuals, everyone knew how to encourage Winston to crawl, and Winston received more opportunities to practice the skill.
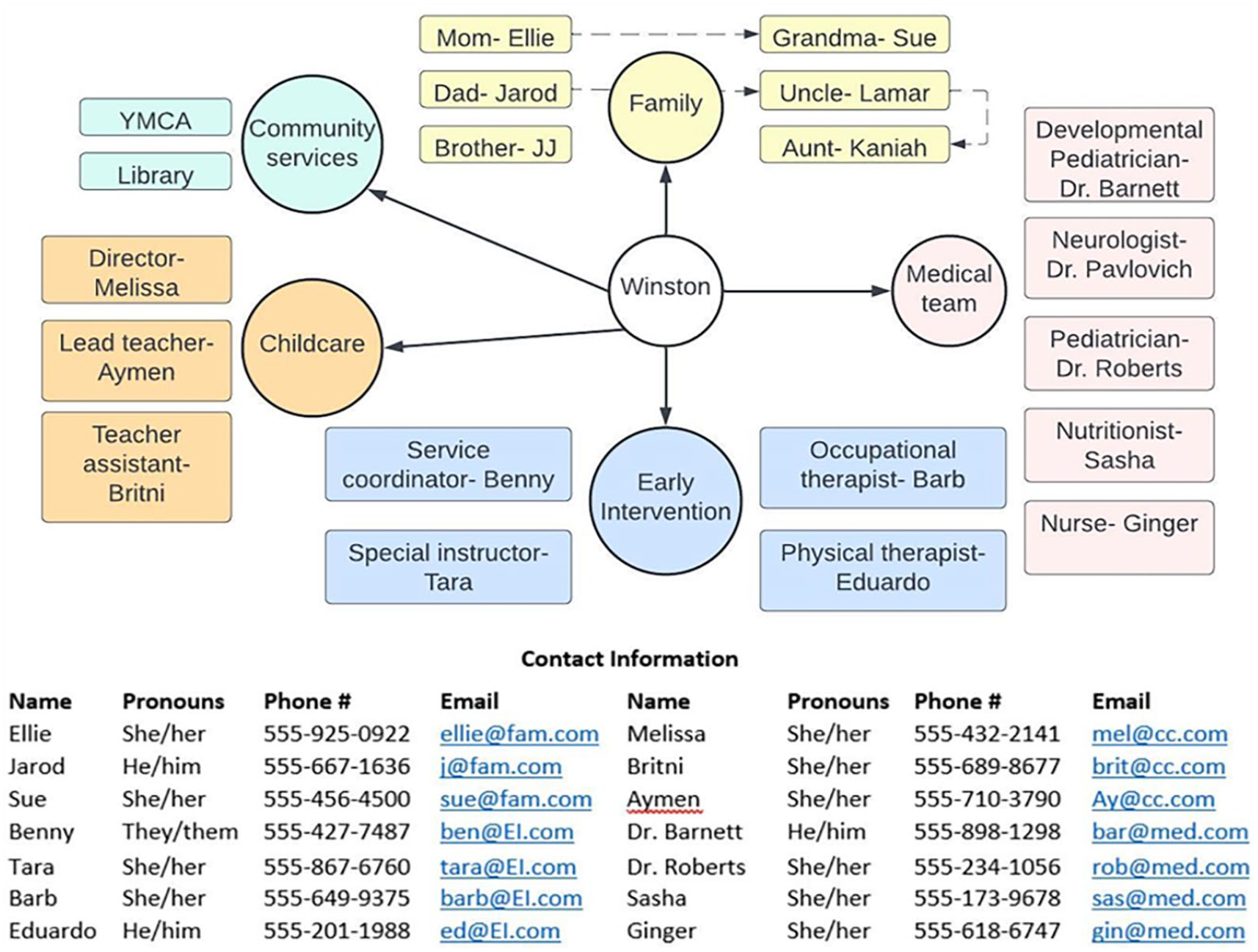
Winston’s Care Map.
A key component of inclusion is that adults who serve children with disabilities have access to supports for their inclusion efforts through high-quality professional development, coordination of care, communication, and policies (DEC/NAEYC, 2009). We provide five strategies in Table 1 (S1–S5) that EIs can use to develop systems of support on a child’s team. In the vignette above, Winston’s EI team demonstrated how they coordinate their services, communicate, and use one another as resources to best serve Winston and promote his inclusion (S1). Importantly, the team’s priorities are consistently established by Winston’s family’s expressed goals and values as recommended by Love and Beneke (2021). Other ways that EIs can help establish systems of support between significant adults in a child’s life is to invite those not typically included to EI meetings (e.g., child care teachers, babysitters) and to agree on ways to share information (e.g., communication notebooks, video-recordings, copies of EI session notes, sending meeting minutes).
In addition to promoting coordination of care and communication, EIs can share opportunities with others to increase their knowledge about inclusion of children with SSNs and gain support from like-minded individuals (S2). For instance, EIs can encourage others to learn about and join organizations dedicated to the inclusion of people with disabilities (e.g., TASH, DEC), connect with support groups, or attend webinars about inclusion. In addition, EIs can share opportunities to get involved in Communities of Practice (CoPs) such as DEC’s EI CoP (https://www.dec-sped.org/earlyinterventioncop) or they can start their own to help others learn about important issues affecting children with disabilities and their families (Williams & Ostrosky, in press). EIs also can consider the specific supports that individual families need and help them obtain the supports (S3). For example, due to the complexity of Winston’s medical needs, he receives nursing care 8 hours a day. Although his family was told about home nursing care by his physician following his injury, other families may hear about it for the first time from their EIs or may want help setting up home nursing care. As another example, EIs who support families of children with SSNs can share information about developmental disability services in their state, provided under the Developmental Disabilities Assistance and Bill of Rights Act (2000), which emphasizes the importance of community-based services for individuals with disabilities (e.g., adaptive equipment, residential services, employment support). These services often require an extensive application process and have long waitlists; therefore, EIs can emphasize to families the importance of getting on waitlists so their children have access to supports as an adult, even if they do not need the services now.
Another way that EIs can support the inclusion of children with SSNs is by sharing information about policies and incentives related to the inclusion of people with disabilities (S4). For example, child care programs or other businesses that make accommodations to support the inclusion of children with SSNs may be eligible for tax credits or tax deductions (U.S. Department of Justice: Civil Rights Division, 2020). By sharing this information with families, child care administrators, community leaders, and organizations, more businesses may be motivated to make changes in their admission procedures. In addition to sharing information about policies and incentives already in place, EIs can advocate for new policies that support the inclusion of children with SSNs across environments (S5). For example, EIs can advocate to their statewide EI program, policymakers, and program administrators that their compensation includes time spent consulting with a child’s family, child care teacher, and other significant adults beyond the typical 60-min session (i.e., between session consultation). Also, EIs can help advocate for supports for child care teachers such as lower adult-child ratios, higher compensation, nursing staff, or mental health consultants. Supports for child care teachers are critical given the current child care crisis in the United States (e.g., underpaid staff, teachers leaving the profession, lack of quality centers, lack of spots for children). EIs can learn about disability-related policies on the Council for Exceptional Children’s policy agenda page at https://exceptionalchildren.org/policy-and-advocacy/policy-agenda and take action by visiting the Legislative Action Center at https://exceptionalchildren.org/takeaction, where individuals can personalize messages to members of the United States Congress.
Through EI, Ellie and Jarod have learned about supports they can use and gained experience in advocating for supports for themselves and others. During a recent parent support group meeting in their community, Jarod facilitated a discussion about the local YMCA and learned about other parents’ concerns related to staff training. Jarod asked Tara if she would go with him to a meeting at the YMCA, and she agreed. Together, they learned that the director of the disability services at the YMCA was currently looking for people to provide training to the staff. Tara and Jarod decided to use this opportunity to support others and offered to provide professional development about the inclusion for young children with SSNs.
Conclusion
Families of young children with SSNs, like Winston’s, may experience exclusion from environments in which children without disabilities typically participate. EIs can work with significant adults in a child’s life to promote the key components of inclusion: access, participation, and supports by using the strategies described. Likewise, by striving for high-quality inclusion across environments, EIs can influence more people, and therefore, society at large to become more inclusive. Children with SSNs will likely receive services and supports through adulthood; therefore, it is crucial that significant adults are prepared to use strategies and access resources that support a child’s inclusion during and beyond EI.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported in part by two grants from the Office of Special Education Programs, U.S. Department of Education: Early Childhood Intervention Doctoral Consortium (ECiDC) (grant no. H325H190004) and Trauma-Informed Early Intervention, Early Childhood Special Education, and Social Work (TI3) (grant no. H325K210076).
Author Biographies
Crystal S. Williams is a doctoral candidate in the Deaprtment of Special Education at the University of Illinois Urbana-Champaign and a practicing early intervention provider. Her research focuses on high-quality early intervention services, particularly for families of children with significant support needs.
Grace E. Sawyer is a master’s student in the Department of Special Education at the University of Illinois Urbana-Champaign. Her studies focus on early intervention, early childhood special education, and trauma-informed care.
Jonathan R. Alexander is a PhD student in the Department of Special Education at the Univeristy of Hawaii at Manoa, a social worker, and a MCH LEND faculty member. His research focuses on integrating families, policy, and advocacy for Native Hawaiian, indigenous, and diverse families who have children with extensive support needs.
Michaelene M. Ostrosky is the Grayce Wicall Gauthier Professor of Education in the Department of Special Education at the University of Illinois Urbana-Champign. Her research focuses on early childhood special education with a particular interest in inclusion, social emotional competence, peer relationships, and challenging behavior.