
Abstract
Photobiomodulation (PBM), a form of nonthermal light therapy utilizing nonionizing light in the visible, near-infrared, or infrared spectra, has both direct effects (at the level of the mitochondria, the primary chromophore in humans) and indirect effects (via modulation of downstream signal transduction and cellular responses). As a result, it is thought to stimulate energy production, reduce oxidative stress, and decrease inflammation. PBM has been clinically studied in a large number of conditions and disease states, and has the advantage of being generally safe and cost-effective. The effects of PBM in autoimmunity, fibromyalgia, muscular function, neurological conditions, long COVID-19, carpal tunnel syndrome, radiation dermatitis, and oral mucositis are reviewed in this article, and additional opportunities for research are identified.
Introduction
The use of light by humans as a therapeutic tool is a very old practice. Hippocrates (460–377 BC) recommended sun exposure (heliotherapy) routinely, and Sun Simiao of the Chinese Tang Dynasty (618–907 AD) described the importance of light therapy to strengthen the qi.1–3 The sanatoria of Europe, used to treat people with tuberculosis from the mid-19th century on, valued exposure to light and “sun baths.” 4 From these earlier practices of the therapeutic use of light to the development of the first lasers more than 60 years ago, the application of phototherapies in medicine has now advanced to include not just medical laser therapy or heliotherapy but also ultraviolet (UV) therapy, photodynamic therapy, and photobiomodulation (PBM), the subject of this article. PBM in simple terms is the therapeutic use of nonionizing forms of light in the visible, near-infrared (NIR), or infrared spectra, which may include lasers, LEDs (light emitting diodes), or broadband light. 5 The photons utilized in PBM are low energy, do not emit radiation (ionizing radiation), and do not emit heat.
Ionizing Versus Nonionizing Radiation
Radiation in the UV band and at lower energies is nonionizing.
Includes radio waves, microwaves, infrared radiation, and visible light (lower wavelength).
Energy is sufficient to move atoms in a molecule around, or cause them to vibrate, but not high enough to remove electrons from atoms.
Radiation to the right of the UV band on the electromagnetic spectrum (shorter wavelength) and at higher energies is ionizing.
Includes X-rays and gamma rays.
Energy is sufficient to knock electrons out of atoms (i.e., ionization). Due to effects on atoms, poses a health risk by damaging tissue and DNA (deoxyribonucleic acid).
In order for photons to have a therapeutic effect, they must be absorbed by some molecule (i.e., a chromophore) at the tissue level. In mammals, the principal site of photon absorption is thought to be the mitochondria. In particular, cytochrome C oxidase (CCO), complex IV of the mitochondrial respiratory chain, is light sensitive and serves as a chromophore in humans. Nitric oxide (NO) acts as a rheostat by reversibly binding to the heme in CCO, thus reducing mitochondrial respiration. Photons cause the uncoupling of bound NO from CCO, allowing oxygen to bind at this site instead, which then activates the electron transport chain.3,6 PBM appears to have more pronounced effects in tissues or cells that are diseased or damaged. It has been suggested that this may be a result of the fact that unhealthy or damaged cells, or those in a state of hypoxia, are more likely to have higher concentrations of NO. 6 As a result, PBM may selectively impact diseased cells while having a lower impact in healthy tissue. Additionally, because PBM may increase the bioavailability of NO, it is thought to improve endothelial function.
Because the primary chromophores for photons in humans would be located in the mitochondria, this also means that tissues with a higher concentration of mitochondria or higher metabolic activity would be likely to benefit more from PBM. 6 Consider skeletal muscle as an example, which has a 3%–8% volume of mitochondria per cell. Even more impressive, cardiac cells have a 30%–40% mitochondrial volume. 7 Neurons are also rich in mitochondria due to their extensive energy requirements; human neurons are thought to contain up to 2 million mitochondria per cell. 8 The liver and kidney also have high concentrations of mitochondria. 3
Aside from direct effects on mitochondrial respiration and adenosine triphosphate (ATP) production, PBM is also thought to modulate reactive oxygen species (ROS) production. It has been shown to modulate the activity of nuclear factor-kappa B (NF-κB). 6 In turn, NF-κB could then influence apoptosis, induce transcription of gene products that regulate neuronal repair or neurogenesis, or modulate production of inflammatory mediators and growth factors. 9 Importantly, these effects may be variable based on tissue conditions; PBM has been shown to activate NF-κB in quiescent (normal) cells while decreasing NF-κB in cells with active inflammation. 10 Some of the targets or mediators of PBM’s effects, such as NO, ROS, or cyclic adenosine monophosphate might also increase the expression of other downstream transcription factors or signaling pathways. Hamblin suggests that this is one of the reasons even brief PBM therapy may have longer-lasting effects that go beyond the acute exposure to light. 6 Additionally, it has been theorized that PBM may stimulate stem cell activity or differentiation. 11 These mechanisms combined highlight the concept that not only would PBM be working locally at the site of application, but that it might also have systemic effects at distant sites. 10
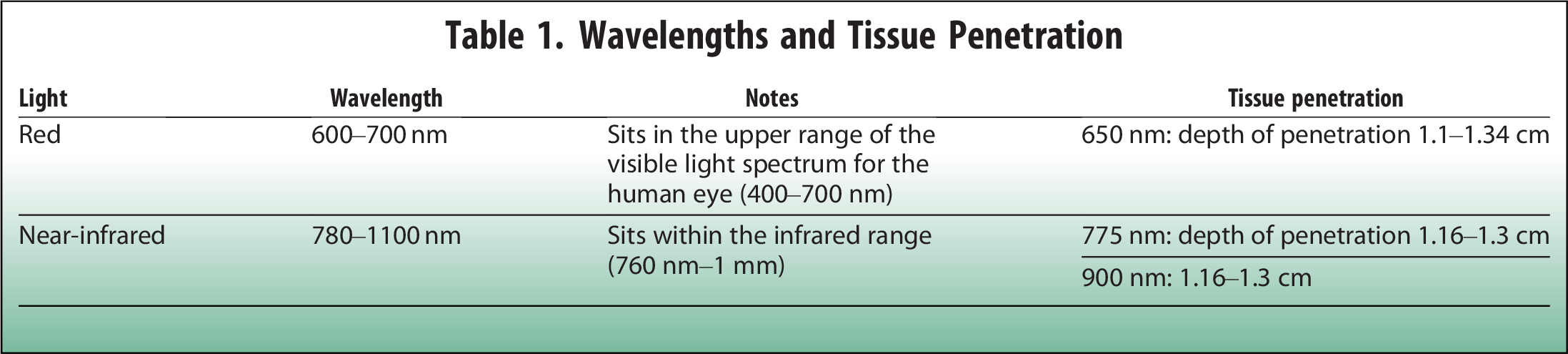
PBM parameters are seen in the sidebar. 12 The ability of a particular light source to penetrate and work at the tissue level is dependent on various factors, including scatter, tissue structures, source properties (such as coherence or treatment time), and wavelength.9,10 Wavelengths in the 600–1200 nm range are capable of interacting with CCO in the mitochondria. 9 Tissue penetration of red and NIR wavelengths of PBM are shown in Table 1. 13
Wavelengths and Tissue Penetration
PBM Parameters
Scatter in tissues is reduced as wavelength increases, so the penetration depth of NIR is thought to be maximal at ∼810 nm. At longer wavelengths, water becomes an important absorber of photons, so the penetration depth decreases again. 10 A small portion of light at 810 nm (on the order of 0.6%) may penetrate a tissue depth up to 2.5 cm. Roughly 78% of a low-power 820 nm light penetrates to a depth of 0.4 mm in epidermis; this drops to 58% at a depth of 1 mm and to 10% at 2 mm. These figures suggest that skin tissue alone may be sufficient to absorb or scatter all of the light from a low-power infrared light source. Higher power may yield greater penetration depth. Using a 15 W laser emitting 810 nm light continuously, 17% of energy has been shown to penetrate to 1.9 mm depth in human skin. Pulsing of infrared light may also improve penetration. Using a 15 W laser emitting 810 nm with a pulse frequency of 10 Hz, 69% of energy has been shown to penetrate to 1.9 mm depth in human skin. 9
A wide range of clinical trials has demonstrated beneficial effects of PBM for people with autoimmune, neurologic, and dermatologic conditions, as well as for muscle performance and fatigue. This article provides a sampling of these data and discusses the effects demonstrated with use of PBM in humans. While not an exhaustive review (a cursory search on PubMed of human clinical trials of PBM yields close to 2000 results), this at least provides an overview of some of the possible uses and breadth of evidence for the use of PBM.
Fatigue and Muscle Performance
A sampling of clinical trials of PBM for fatigue and muscular performance is seen in Table 2.
Clinical Trials of Photobiomodulation for Fatigue and Muscular Performance

BMI, body mass index; CKD, chronic kidney disease; CI, confidence interval; EFI, electromyographic fatigue index; HD, hemodialysis; PBM, photobiomodulation; rep, repetition; TTF, time to muscular fatigue.
These trials demonstrate the ability of PBM to impact muscular strength and reduce muscular fatigue.14–17 While the trials described above are quite small, meta-analyses seem to back these effects up.
In Vanin et al.’s 2018 meta-analysis of PBM for muscular performance and fatigue with exercise in healthy individuals, 39 randomized controlled trials (RCTs) with 861 total subjects were included. Overall, positive results were seen with the use of low-level laser and LED therapy, or the combination, in wavelengths ranging from 655 to 950 nm. Energy doses ranged from 20 to 60 J for small muscle groups, and 60 to 300 J for large muscle groups for included trials, with maximum power outputs of 200 mW per diode. For 12 trials that examined the effects of PBM in prolonging the time until exhaustion with exercise, there was a significant mean difference (MD) of 3.55 seconds with use of PBM (N = 348, 95% confidence interval [CI]: 1.09–6.00; P = 0.005). Eight trials also demonstrated that PBM increases the number of repetitions (reps) of an exercise performed, compared to placebo (N = 219; MD = 4.88; 95% CI: 0.14–9.62; P = 0.04). Additionally, 12 trials reported on blood lactate levels either immediately after or 5 minutes after exercise, finding that PBM had a significant benefit here as well (N = 337; MD = 0.14 mmol/L; 95% CI: −0.49 to 0.20; P = 0.41). The authors noted small sample sizes and risk of bias (including lack of allocation concealment) as limitations of this analysis. 18
In Bezerra et al.’s 2023 meta-analysis, 16 trials with a total of 340 individuals were included, assessing for the effects of PBM on strength, fatigue, and functional capacity in healthy subjects. Variable forms of PBM were used in the included trials. Wavelengths ranged from 655 to 905 nm, power from 100 to 200 mW, energy from 0.6 to 30 J per point, and time from 30 to 100 seconds per point. There was no change in strength as assessed by peak torque, a one-rep max test, or isometric and isokinetic strength with use of PBM, and no change in short- or long-term functional capacity with use of PBM in this analysis, with this data coming from nine trials. However, for four trials that assessed fatigue recovery, PBM was superior to placebo for the prevention of exercise-induced fatigue (MD = 5.87; 95% CI: 3.83–7.91). 19
Fibromyalgia
Trials on PBM have also been conducted in people with fibromyalgia (FM), assessing for effects on varied outcomes such as pain and stiffness, tender points, fatigue, and mood. A 2019 meta-analysis by Yeh et al. included 9 RCTs with 325 people with FM. Included trials utilized PBM, compared to placebo, with or without exercise programs. Wavelength ranged from 640 to 950 nm, while power ranged from 0.9 to 1000 mW in the included trials. Follow-up periods ranged from 2 to 10 weeks, except in one RCT, which followed subjects for 6 months.
In this analysis, use of PBM resulted in significantly greater improvement in Fibromyalgia Impact Questionnaire scores (standardized mean difference [SMD]: 1.16, 95% CI: 0.64–1.69), pain severity (SMD: 1.18; 95% CI: 0.82–1.54), number of tender points (SMD: 1.01, 95% CI: 0.49–1.52), fatigue (SMD: 1.4, 95% CI: 0.96–1.84), stiffness (SMD: 0.92, 95% CI: 0.36–1.48), depression (SMD: 1.46, 95% CI: 0.93–2.00), and anxiety (SMD: 1.46, 95% CI: 0.45–2.47) compared to placebo. Additionally, compared to exercise alone, the combination of PBM with exercise therapy provided additional reductions in pain severity, number of tender points, and fatigue level (SMD: 5.20, 95% CI: 3.85–6.55; SMD: 7.02, 95% CI: 5.29–8.76; and SMD: 1.35, 95% CI: 0.65–2.04, respectively).
Multiple Sclerosis
PBM has been proposed as an option in people with multiple sclerosis (MS) due to its ability to enhance cellular respiration and ATP formation, and modulate oxidative stress and cytokines. In a pilot-scale RCT (N = 15) in subjects with relapsing-remitting multiple sclerosis (RRMS), participants were randomized to either sublingual PBM treatment or PBM administered over the radial artery. Regardless of treatment site, wavelength was 808 nm, power was 100mW, and treatment time was 360 seconds twice weekly for 12 weeks (24 sessions). Blood samples were then analyzed to look at serum interleukin-10 (IL-10) and nitrite levels (serum nitrate and nitrite levels have been shown to be higher in people with MS). Nitrite levels were no different before or after PBM treatment. However, IL-10 increased in both the sublingual group (pretreatment: 2.8 ± 1.4 pg/mL; posttreatment: 8.3 ± 2.4 pg/mL) and the radial artery group (pretreatment: 2.7 pg/mL ± 1.4; posttreatment: 11.7 ± 3.8 pg/mL). The authors suggested PBM may be immunomodulating in people with MS. 20 In a separate analysis of the above treatment protocol by the same group, sublingual or radial artery PBM at the doses described had no effect on fatigue, as assessed by the Modified Fatigue Impact Scale (MFIS). There were no significant differences seen in either total MFIS scores or subscale scores (P < 0.05) with use of PBM at the doses described in subjects with RRMS. 21
In another clinical trial in people with MS, this time a randomized double-blind crossover study, PBM therapy did not impact muscle fatigue with an exercise trial, but did seem to support muscle recovery. Subjects received four sessions of PBM (40 J, 80 J, 120 J, and placebo), with muscle function assessed before and after. A subgroup from this first part of the trial also went on to complete a second part, in which they received an individualized dose of PBM (selecting the dose from best dose–effect seen in the first part of the trial for each participant), again for four sessions, and again with muscle function assessed before and after. As mentioned above, muscle fatigue was not significantly different with either PBM or placebo. However, in the first part of the trial, significant improvement in muscle force recovery (101.89%) was observed with the highest PBM dose compared to placebo (96.3%, P = 0.03). In the second part of the study using individualized doses, PBM treatment led to significantly better muscle strength compared to both baseline and to placebo (P = 0.01 and P = 0.02, respectively). 22 This suggests that patient response may be helpful in selecting an individually effective dose.
Autoimmune Thyroiditis
In chronic autoimmune thyroid disease, the immune system attacks the thyroid gland, leading to destruction and inflammation of the tissue over time. Autoimmune thyroid disease is actually the most frequent cause of hypothyroidism in iodine-replete populations. PBM has been proposed as a potential therapy for autoimmune thyroid disease, as preclinical data has shown it may lead to improved microcirculation in the thyroid tissue, and subsequent increases in thyroid hormone production. Because the thyroid sits superficially, it is also considered accessible for PBM purposes. 23
In a small 2010 noncontrolled clinical trial (N = 15), people with autoimmune thyroid disease who were being treated with levothyroxine were given PBM in a total of 10 sessions given twice weekly over 5 weeks. PBM was administered in continuous mode at 830 nm, fluence ranging 38–108 J/cm2, with 50 mW power, using either a point-focused technique (8 subjects) or a sweep technique (7 subjects). Ultrasound of the thyroid was performed at baseline and at 30 days post PBM. At the time of the second ultrasound, levothyroxine was also discontinued in all subjects and then reintroduced if needed. All participants experienced a reduced need for thyroid hormone replacement. In seven subjects (47%), there was no need for resumption of levothyroxine through nine months of follow-up after PBM. Overall levothyroxine dose significantly decreased from baseline to 9 months (from 96 ± 22 μg/day to 38 ± 23 μg/day; P < 0.0001). Echogenicity of the thyroid parenchyma by ultrasound also increased significantly (baseline = 0.99 ± 0.09, post PBM = 1.21 ± 0.19; P = 0.001). 23
A 2013 trial by the same group also utilized a similar protocol to the one described above, but this time with a placebo control. Forty-three people with autoimmune hypothyroidism taking levothyroxine were randomized to either PBM or placebo for 10 sessions. PBM was administered at a wavelength of 830 nm, output power of 50 mW, and fluence of 707 J/cm2. As above, levothyroxine was discontinued in all subjects 30 days after PBM/placebo procedures. Mean levothyroxine dose requirements following the intervention were significantly less for the PBM group than for placebo (38.59 ± 20.22 μg/day vs. 106.88 ± 22.90 μg/day, P < 0.001), and lower thyroid peroxidase antibody levels and greater thyroid gland echogenicity via ultrasound were also seen with PBM (P = 0.043 and P < 0.001, respectively). 24 A separate analysis of the data from this trial also found that PBM decreases serum levels of transforming growth factor-beta (TGF-β1), a cytokine that may be anti-inflammatory in some contexts or associated with immune regulation. TGF-β1 levels were significantly higher in the PBM group than in the placebo group at 30 days postintervention (874.9 ± 541.7 pg/mL vs. −128.4 ± 832.8 pg/mL, P = 0.0379). 25
Long COVID-19 Symptoms
PBM has also been used in a handful of trials to address specific long COVID-19 (coronavirus disease 2019) symptoms. In Bowen and Arany’s 2023 open-label pilot study, 14 people with cognitive complaints (“brain fog”) of at least five months’ duration following COVID-19 infection were randomized to either transcranial PBM (using a helmet providing 1070 nm, power density of 24 mW/cm2, fluence of 20.2 J/cm2) or whole-body PBM (using a light bed providing 660 and 850 nm, treatment surface irradiance of 24 mW/cm2, fluence of 20.2 J/cm2). Subjects received 12 treatments lasting 14 minutes each, over a 4-week period. Use of both PBM devices led to significant improvements in cognitive batteries (Montreal Cognitive Assessment [MoCA], the Digit Symbol Substitution Test, the Trail Making Tests [TMTs] A and B, the physical reaction time, and a quantitative electroencephalography system [WAVi], P < 0.05 for all) in these subjects with long COVID-19 cognitive complaints. 26
Olfactory changes are also a common complaint among people with long COVID-19 symptoms. In a single-blind, randomized, controlled clinical trial, people with olfactory changes who were 1–12 months post COVID-19 infection (N = 81) were randomized to a control group, red light therapy, or infrared light therapy. Controls underwent 10 sessions of PBM with the device turned on, but without emitting any light. In the red light group (660 nm), subjects had 10 sessions of PBM at a dose of 4 J. In the infrared group (780 nm), again subjects had 10 sessions at 4 J (energy density 140 J/cm2). Regardless of the treatment/control applied, subjects were treated for 40 seconds at each nostril (intranasally), twice a week. All subjects also underwent olfactory training for 90 days and took prednisolone 40 mg for 7 days starting on the first day of the trial. People who received PBM demonstrated greater improvement in University of Pennsylvania Smell Identification Test scores compared to controls (+4.6 points, 95% CI: 1.5–7.8, P = 0.004). Response rates for subjects in the control, red light, and infrared groups were 26.1% (95% CI: 6.7–45.5), 43.5% (95% CI: 21.6–65.4), and 68% (95% CI: 48.3–87.7) respectively. 27
In another trial among people with dysgeusia related to long COVID-19, 70 people who had recovered from COVID-19 but had dysgeusia were randomized to either systemic (carotid) plus local PBM or simulated PBM as a control. PBM subjects were treated with red light at 18 spots on the lateral border of the tongue and over the parotid, sublingual, and submandibular glands (3 J per spot, energy density of 30.61 J/cm2, wavelength of 660 nm, power of 100 mW/cm2, 30 seconds per spot in continuous mode), as well as over the carotid artery (same parameters as above, at 60 J for 10 minutes). Subjects also underwent olfactory training for 8 weeks. At the conclusion of the trial, dysgeusia improved in both groups, but those receiving PBM had significantly greater improvement than controls (higher scores on total gustometry, P = 0.048).
Neurological Conditions
PBM has been clinically studied in people with Parkinson’s disease (PD), cognitive decline, and even dementia, with a variety of benefits having been demonstrated.
In a randomized controlled study in 38 people (ages 50–70) with functional declines and postural instability due to PD, subjects were randomized to either transcranial PBM or to a control group (standard of care only) for 12 weeks. At the conclusion of the trial, the PBM group had significantly better postural stability and function than controls (P < 0.05). 28 Another small trial (N = 12) randomized people with PD to either PBM (transcranial, intranasal, neck and abdominal, with parameters different for each application site) for 12 weeks or to a wait-list for PBM treatment 14 weeks later. Subjects were given a PBM device for home treatment, which was applied transcranially, intranasally, and at the neck and abdomen. Mobility, cognition, balance, and fine motor skills all significantly improved with PBM (P < 0.05 for all, with a variety of assessments used, including MoCA, step test, walking speed, spiral test, micrographia, nine-hole peg test, and tandem and single-leg stance) for up to 1-year posttreatment. 29
Turning to cognitive effects, PBM has been shown to result in cognitive benefits for people in a variety of clinical scenarios, from healthy older adults, to people with subjective cognitive concerns or mild cognitive impairment (MCI), to those with dementia.
In a study of 55 healthy older adults, participants were randomized to either sham treatment or active transcranial PBM. After a washout period, subjects then crossed over to the opposite intervention, serving as their own control. Each treatment session included sham or active PBM (1064 nm laser applied to left forehead), functional near-infrared spectroscopy measurements, and the digital n-back task. Compared to sham, treatment with active PBM resulted in improved accuracy and reaction time during the n-back test (P < 0.001 and P = 0.004). Additionally, global efficiency, local efficiency, nodal efficiency, and functional connectivity significantly increased with use of PBM, especially in the frontoparietal region (P = 0.001, P = 0.003, P < 0.05, and P = 0.01, respectively). Improvements in the n-back test were positively associated with shifts in functional connectivity and nodal efficiency mainly in the left prefrontal cortex. The authors concluded that PBM may improve working memory by modulating functional brain network properties. 30
In a study of people with subjective cognitive decline (N = 58, ages 50–79, with memory complaints, but without MCI or dementia), participants were randomized to either sham or PBM treatment. The PBM device supplied light at 1064 nm, with power density of 250 mW/cm2, to the anterior prefrontal cortex (Brodmann areas 9 and 10), for 12 minutes daily for 6 days in a row. Use of PBM resulted in significant improvements in the n-back test compared to control, with both accuracy and reaction time showing improvements (88.6% vs. 79.6%, P = 0.001, and 544.80 ± 202.00 vs. 592.87 ± 222.05, P = 0.003, respectively). Measures of sleep function pre- and postintervention were unchanged. 31
In people with MCI, PBM has also shown to be efficacious. In Chun et al., participants of a small RCT (N = 26) were randomized to sham or veritas transcranial PBM treatment. Patients were provided a device for at-home use, completing 6 treatments a week for 12 weeks (72 treatments in total, each treatment lasting 11 minutes). The PBM device provided a power density of 277 mW/cm2, a wavelength of 808 nm, fluence of 3326 J/cm2, with a pulsed frequency of 42 Hz. Treatment with PBM resulted in a significantly greater increase in K-MoCA (Korean version of MoCA test) scores compared to sham control. At the completion of the trial, there was an MD of 5 points between groups (95% CI: 1.65–8.35, P = 0.005). 32
In Baik et al., researchers sought to determine if PBM has any impact on regional cerebral blood flow (rCBF) among people with MCI. Fourteen people with MCI were treated with a PBM device at the sternocleidomastoid (over the internal carotid) and superior trapezius (over the vertebral arteries) muscles, 30 minutes 5 times a week for 8 weeks (40 treatments in total). The device supplied light at 610 nm, with a power of 3.0 mW/cm2. Participants experienced significant improvements in rCBF Z-scores at the medial prefrontal cortex (P = 0.018), lateral prefrontal cortex (P = 0.025), anterior cingulate cortex (P = 0.000), and occipital lateral cortex (P = 0.018) from baseline to trial completion. Additionally, MoCA significantly improved (P = 0.000), as did the Verbal Learning Test, TMT, Boston Naming Test, and Rey Complex Figure Test (P = 0.003, P = 0.046, P = 0.001, and P = 0.012, respectively). 33
Clinical studies of PBM in MCI have generally been small in size, but a 2023 meta-analysis pooled results to examine effects on age-related cognitive impairment. Eleven RCTs were included. PBM was shown to have significant effects on global cognitive function (SMD = 0.51, 95% CI: 0.162–0.864, P = 0.004). Multiple wavelength PBM had significant effects, while single wavelength PBM did not (SMD = 0.648, 95% CI: 0.220–1.075, P = 0.003 vs. SMD = 0.385, 95% CI: −0.168 to 0.987, P = 0.172), and the effect for laser was greater than that seen with LED (SMD = 0.682, 95% CI: 0.37–0,994, P < 0.001 vs. SMD = 0.582, 95% CI: 0.269–0.895, P < 0.001). PBM applied in a clinical setting also outperformed home-use devices in this analysis (SMD = 0.468, 95% CI: 0.050–0.887, P = 0.028 vs. SMD = 0.616, 95% CI: −0.121 to 1.354, P = 0.101). The pooled effect of multimodality PBM was also greater with use of transcranial devices (SMD = 0.616, 95% CI: −0.121 to 1.354, P = 0.010). Cumulative treatment time was a moderator between use of PBM and improved and cognitive function. 34
Moving to studies in people with dementia, a small trial (N = 8) in people with dementia residing at home randomized subjects to either usual care or PBM (four people in each group) for 12 weeks. PBM was administered by a personal caregiver (such as the patient’s spouse or child) at home for 20 minutes 3 times a week, using a pulsed 810 nm light at 40 Hz intranasally and over the frontal and parietal regions of the head. Each treatment session provided 240 J, for a cumulative weekly dose of 720 J. At the completion of the trial, people in the PBM group experienced significant improvements in Alzheimer’s Disease Assessment Scale–Cognitive (ADAS-cog) and Neuropsychiatric Inventory (NPI) scores (group × time interaction: F1,6 = 16.35, P = 0.007, and group × time interaction: F1,6 = 7.52, P = 0.03, respectively). The authors noted that in this study, ADAS-cog scores in the PBM group improved by an average of −1.83 points after 6 weeks and −5.18 points after 12 weeks, and while the sample size was certainly small, these ADAS-cog improvements are greater than that seen in pharmacological trials of donepezil at 10 mg/day. Patients also underwent baseline and 12-week functional magnetic resonance imaging, indicating that PBM resulted in increased connectivity between the posterior cingulate cortex and lateral parietal nodes of the default mode network. There were no adverse events associated with PBM use in this small trial. 35
In another small trial in people with Alzheimer’s disease (N = 9), participants underwent 4 months of whole-brain PBM treatment (810 nm, 100 mW/cm2, 30 minutes per session, 6 sessions a week). At the completion of the trial, the mean change from baseline on the Mini-Mental State Examination was 3.2 (P = 0.02), and mean change from baseline on the ADAS-cog was −5.0 (P = 0.05). MoCA scores also improved from baseline by a mean of 1.9 (P = 0.12), as did NPI, by a mean of −4.2 (P = 0.47). These benefits were sustained in follow-up 2 months after completion of PBM, and there were no adverse events associated with use of the PBM device. 36
Carpal Tunnel and Osteoarthritis
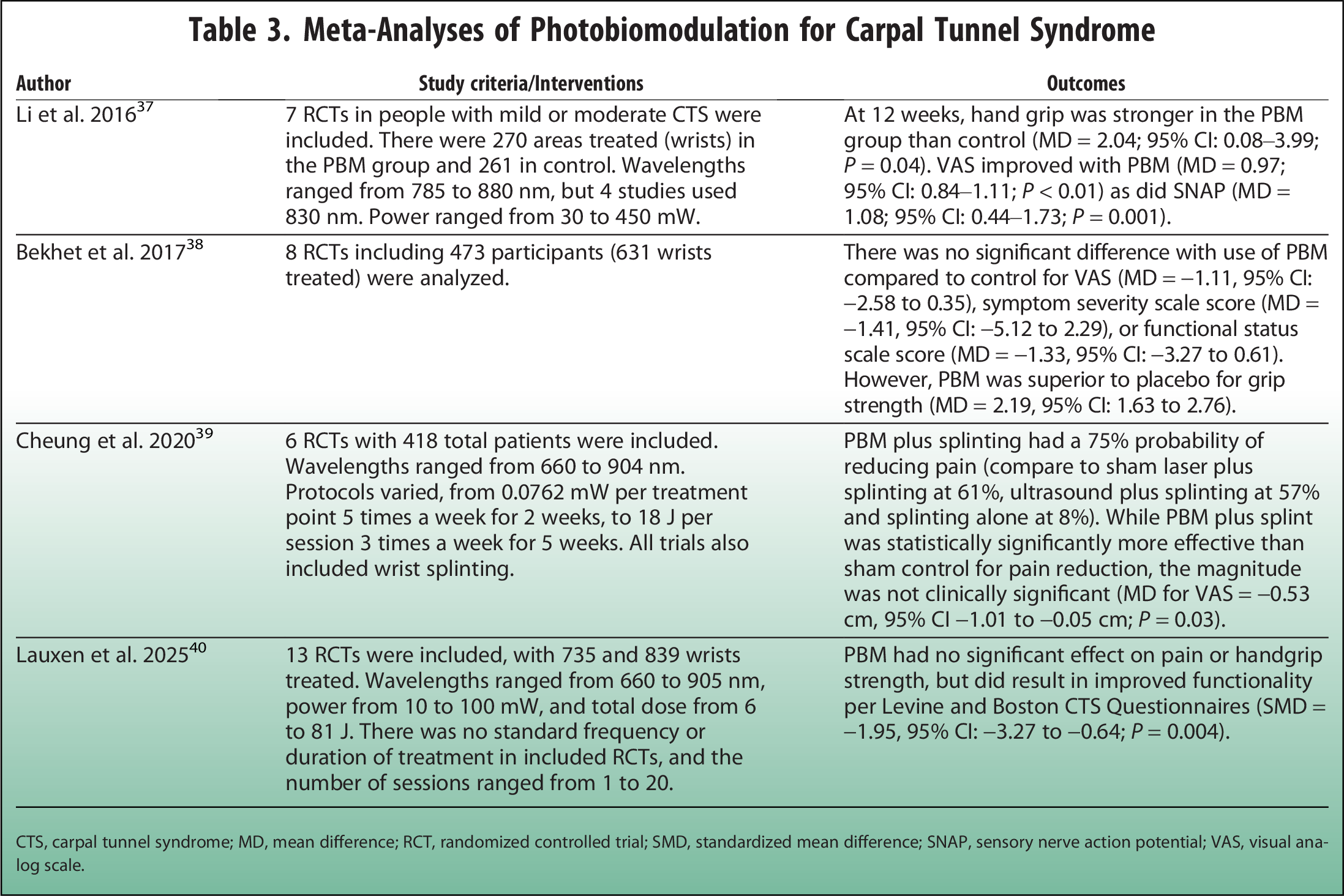
A number of clinical trials have been conducted in both people with carpal tunnel syndrome (CTS), and musculoskeletal complaints, including osteoarthritis (OA), demonstrating the benefits of PBM. As a result, there are meta-analyses available in both these areas that shed light on PBM’s effects (Table 3).
Meta-Analyses of Photobiomodulation for Carpal Tunnel Syndrome
CTS, carpal tunnel syndrome; MD, mean difference; RCT, randomized controlled trial; SMD, standardized mean difference; SNAP, sensory nerve action potential; VAS, visual analog scale.
Meta-analyses in people with carpal tunnel have demonstrated a variety of effects. Some indicated a benefit to hand grip, functionality, pain scores from visual analog scale (VAS), or sensory nerve action potential, while others found a lack of benefit in some of these areas.37–40 There would be a need for additional trials that help standardize doses and treatment protocols, to understand if there is an optimal PBM regimen for carpal tunnel.
Regarding OA, a meta-analysis of trials specifically conducted using 1064 nm wavelength PBM included 4 clinical trials, with Ns ranging from 40 to 90 participants. All four trials found a sustained reduction in OA knee pain (using VAS or Western Ontario and McMaster Universities Osteoarthritis Index) with a large effect, with follow-up ranging from six weeks to three months. One of the included trials demonstrated increased knee cartilage thickness, detectable six weeks after completion of a PBM protocol lasting three weeks. Protocols varied, providing treatment sessions ranging from 7 sessions given daily over the course of 1 week, up to 3 times a week for 12 weeks. Power ranged from 5 to 12 W, and total dose from 2400 to 3000 J. This meta-analysis also looked at use of 1064 nm wavelength PBM for other orthopedic conditions (such as neck or low back pain, or lumbar disc conditions), but noted that the largest effect sizes for pain reduction were seen with knee OA (average Cohen’s d effect size = 2.46). 41
Radiation Dermatitis and Oral Mucositis
Because PBM is generally cost-effective and noninvasive, it also presents an attractive option for wound care. PBM has been successfully demonstrated in many trials to assist with wound healing for people with varying conditions. This includes diabetic ulcers, oral surgery wounds, fracture healing, and pressure ulcers, among others.42–45 Effects seen with PBM that are pertinent to wound healing include resolution of inflammation, improved collagen synthesis, increased tensile strength, decreased time needed for healing, and reductions in wound size. 46
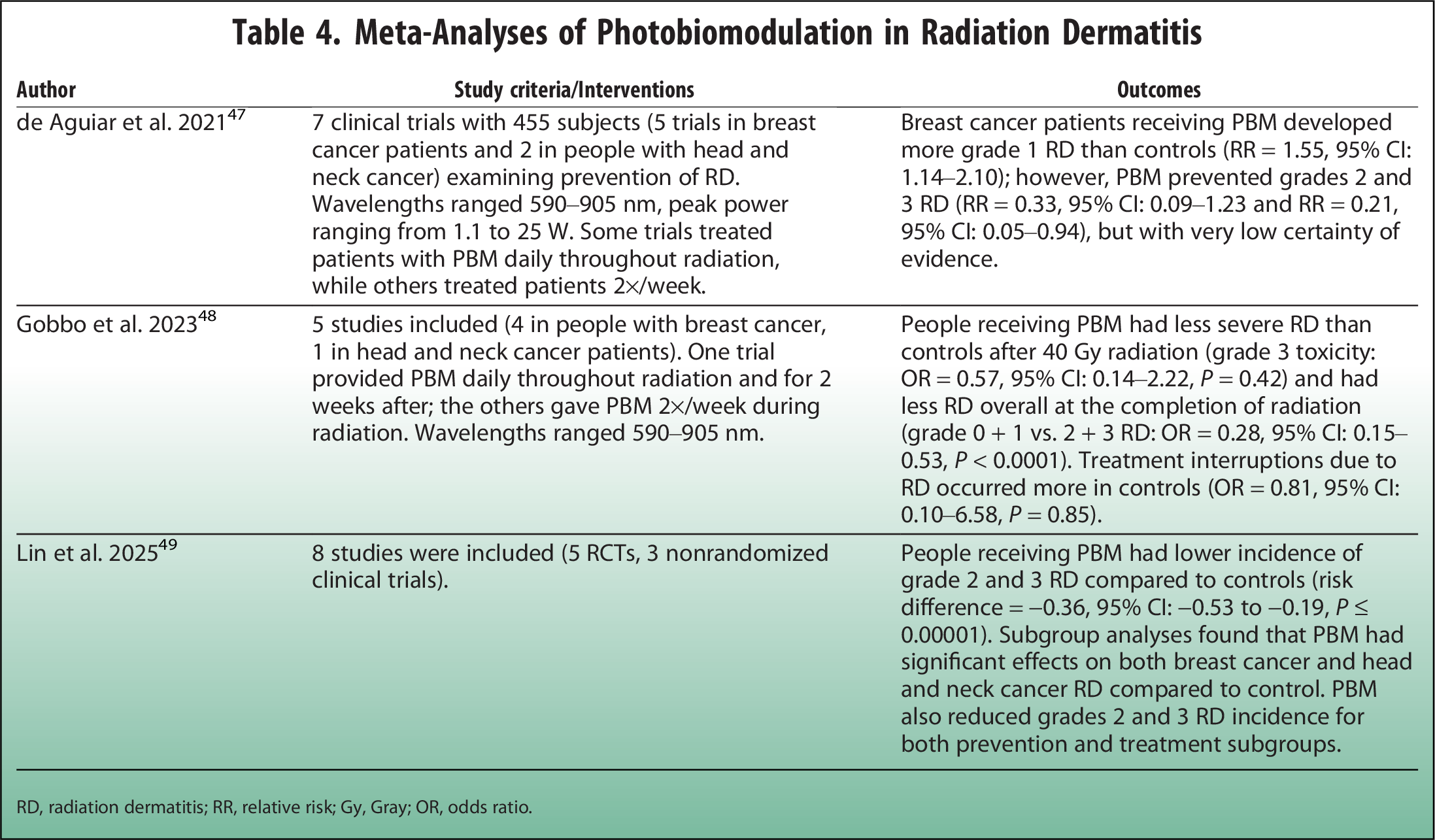
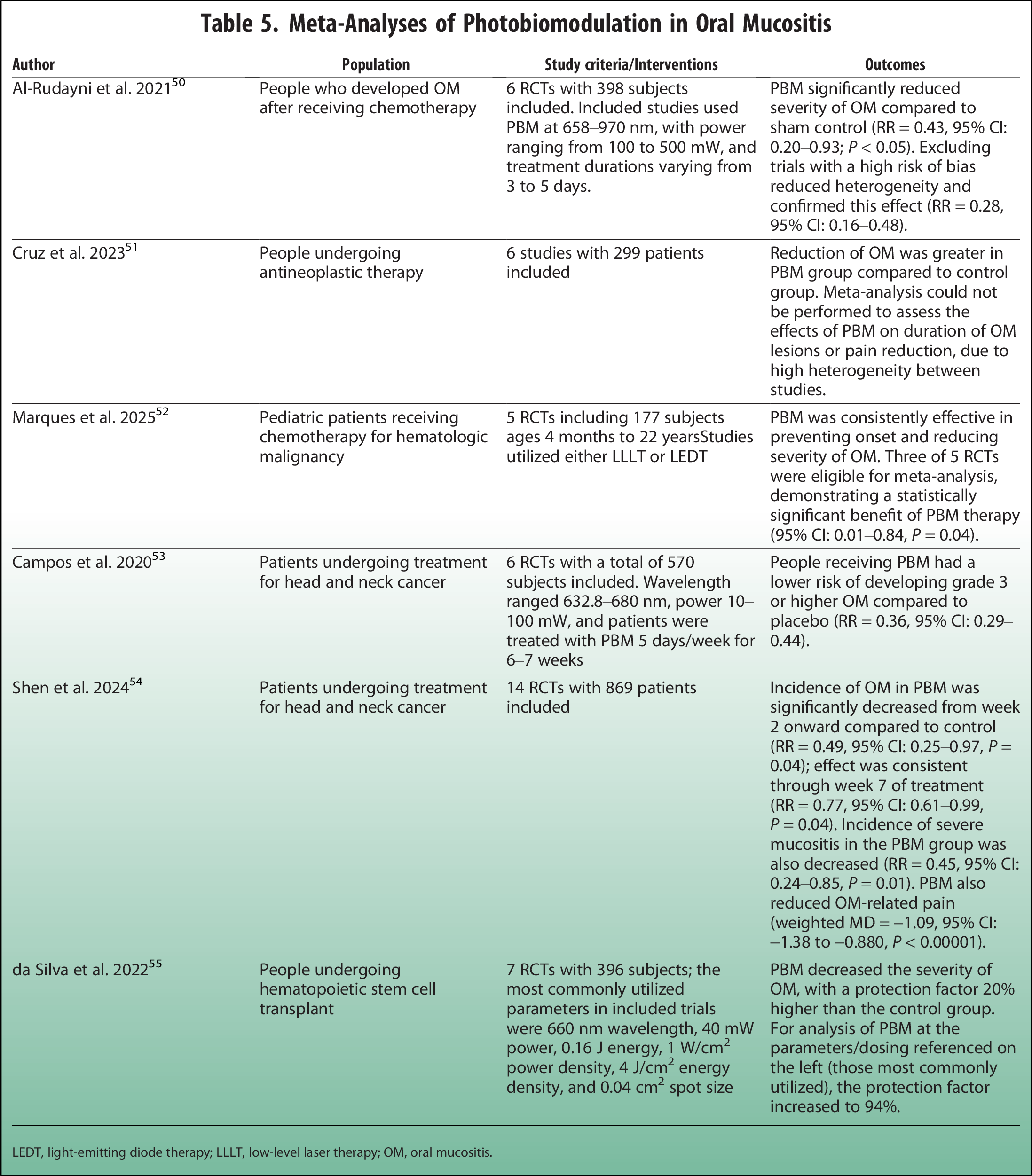
Related to its wound healing properties, PBM has also been shown to reduce radiation dermatitis and oral mucositis in oncology patients, with meta-analyses available in both areas (Tables 4 and 5).
Meta-Analyses of Photobiomodulation in Radiation Dermatitis
RD, radiation dermatitis; RR, relative risk; Gy, Gray; OR, odds ratio.
Meta-Analyses of Photobiomodulation in Oral Mucositis
LEDT, light-emitting diode therapy; LLLT, low-level laser therapy; OM, oral mucositis.
In meta-analyses of studies on radiation dermatitis, PBM was seen to reduce the occurrence of RD, including higher grade RD.47–49 In one analysis, PBM was seen to prevent treatment interruptions, and in another, it was effective for both RD treatment and prevention.48,49
In meta-analyses of studies in oral mucositis, a number of beneficial effects were demonstrated with PBM. These included a reduction in the incidence and severity of OM, as well as pain symptoms related to OM. Studies included people receiving chemotherapy treatment, people with head and neck cancer undergoing chemoradiation, and children and adults being treated for hematologic malignancy.50–55 Clinical trials of PBM for OM have been conducted utilizing both intraoral (such as the oropharynx) and extraoral (i.e., cheek, mandible, neck) delivery sites.
Discussion
The studies discussed above have demonstrated the utility and feasibility of PBM in a variety of clinical conditions. People with autoimmune conditions (such as MS or autoimmune thyroid disease) have been shown to obtain benefits from PBM. PBM may impact fatigue or muscular performance. It has also been shown to reduce pain and mood complaints in people with FM. Likewise, it may help reduce pain in people with CTS or OA. It has also been shown to provide positive effects in people with neurological conditions, including PD and dementia. It has successfully been used in people with taste and smell changes and cognitive complaints related to long COVID-19. Additionally, many trials have been conducted in people undergoing treatment for cancer, with PBM having been shown to reduce both RD and OM.
As the studies described above demonstrate, there are a large number of parameters or doses of PBM being used clinically. There seems to be a lack of consensus on optimal wavelength, dosing, and treatment regimen. There is a need for studies across all the areas mentioned above that compare or standardize PBM dosing and parameters. This would help clinicians develop the most effective recommendations, so patients can derive maximum benefit when receiving PBM therapy, and would assist those trying to assess a PBM device for efficacy and safety.
PBM should not be applied over the eyes. 56 Clinicians should keep in mind that the protective eyewear provided with consumer-direct PBM devices may be of poor quality and may need to be replaced with better quality eyewear. 57 PBM is also contraindicated for direct application over tumor tissue. Additionally, caution is advised around the thyroid gland unless under medical supervision. It is thought that the because of the thyroid’s important role in regulating metabolism, it may be especially vulnerable to the effects of treatments such as PBM, which are energy modulating. PBM tends to be quite well tolerated, with generally <10% of people noticing mild and short-term side effects such as fatigue or mild headache in some studies. Again, this is an area where tailoring the use of PBM for the specific individual may become important. 56
As consumer-grade PBM devices become both more popular and more widely available, the concerns discussed above become even more important. Given the lack of consensus on optimal PBM parameters for various conditions, it may also be difficult for consumers to understand whether the wavelength, energy density, or mode of a specific device will be sufficient to have the intended effects. Consumer-grade PBM devices may also lack consistent or uniform power output, so doses at a target tissue may simply be ineffective. For example, in one study of five randomly selected consumer-direct PBM devices, the stability of power output was seen to be variable, affecting the accuracy of dose delivery. 57 Additional standardized, well-designed trials on PBM are especially important in this context, to help clinicians guide patients in the selection of appropriate and effective treatment.
Advantages of PBM include its noninvasive nature. It is also generally cost-effective, well tolerated, and can be administered long term. Because of its broad effects in reducing inflammation and pain, modulating the immune response, and stimulating tissue regeneration or healing, there are a large number of clinical scenarios that could likely be addressed with this rather simple and accessible therapy.
Footnotes
Author Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.▪