
Abstract
Objective:
To investigate whether acupuncture enhances knee joint muscle endurance effectiveness and time-dependent effects after anterior cruciate ligament (ACL) injuries.
Methods:
This randomized, single-blinded crossover trial included 20 males with ACL injuries. Participants were randomly divided into real acupuncture (RA) group and sham acupuncture (SA) group. RA was stimulated at ST32, ST34, ST36, SP10, and BL57; the SA received acupuncture 1–3 cm near these specific acupoints for 15 min. Both groups underwent RA and SA with a 1-week washout in between. Primary outcomes included kinetic and blood biochemical parameters. Kinetic variables (maximum torque, peak power, maximum average torque, average work, average power, total work, and joint stiffness) were assessed at six time points: pre-intervention and 3, 13, 23, 33, and 43 min postintervention. Blood biochemical markers (glucose, creatine, lactate, ammonia, carnitine, and glutathione) were measured at three time points: pre-exercise, postacupuncture, and postexercise.
Results:
Significant group × time interaction on isokinetic parameters, joint stiffness, ammonia, lactate, and glutathione (all P < 0.05). Post hoc tests revealed significant increases in isokinetic parameters and stiffness at post1-post3/post4, and ammonia, lactate, and glutathione increased significantly postexercise (all P < 0.05). Compared with the SA, the isokinetic parameters, stiffness, ammonia, lactate, and glutathione were significantly different (all P < 0.05). No significantly difference between groups in glucose and creatine kinase (all P > 0.05), and both increased with time (all P < 0.05).
Conclusion:
Acupuncture can immediately improve knee joint endurance in ACL injury patients, with time effects lasting 23–33 min after needle removal.
Keywords
Introduction
Anterior cruciate ligament (ACL) injury is among the most prevalent sports-related knee injuries. Conservative management represents the primary treatment strategy, particularly for partial ruptures. Despite conservative rehabilitation, persistent functional instability remains common in a subset of patients. 1 In patients with chronic ACL insufficiency, consistent neuromechanical deficits are evident, including impaired knee proprioception, aberrant quadriceps neuromuscular activation, and markedly reduced quadriceps muscle endurance.2,3 These impairments compromise dynamic knee stability, increase the likelihood of recurrent giving-way episodes, and accelerate the onset of post-traumatic osteoarthritis.4–6 Among these deficits, quadriceps endurance may represent a critical modifiable determinant of fatigue-resistant knee stability.
Acupuncture is a therapeutic technique in which fine needles are inserted into specific acupoints to regulate the flow of qi and elicit measurable neuromuscular responses. 7 Previous studies have indicated that acupuncture may exert acute effects on lower-limb performance, including reductions in analgesia and transient improvements in quadriceps force production and fatigue resistance.8–10 These effects exhibit a time-dependent pattern, typically peaking within minutes after stimulation and varying in duration across individuals.8,11 Preliminary studies suggest that acupuncture may facilitate rehabilitation after ACL injuries. For instance, electroacupuncture at acupoints BL39 and BL40 near the knee joint may reduce bone marrow edema and mitigate the severity of ACL injuries. 12 In addition, stimulation of the ACL hamstring reflex arc may contribute to proprioception recovery in individuals with ACL injuries. 13 Clinical evidence indicates that acupuncture may improve neuromuscular outcomes in patients with chronic ACL insufficiency.14,15 Collectively, these findings support the potential role of acupuncture as an adjunctive intervention in ACL rehabilitation, particularly given its reported time-dependent neuromuscular effects.
Deqi refers to sensations, such as soreness, numbness, heaviness, and distention, elicited by parasympathetic nerve stimulation at specific acupoints. 16 Similarly, postactivation performance enhancement (PAPE) is characterized by an acute increase in explosive neuromuscular force following high-intensity voluntary muscle contractions. 17 The underlying mechanisms include enhanced autonomic neural drive, high-threshold motor unit activation, and increased muscle temperature and water content, all of which collectively improve muscle contractility and performance. 18 Deqi and PAPE can enhance motor performance, and their effects are time-dependent. PAPE typically manifests 3–10 min postactivation, with effects lasting >15 min.17,19 Recent research has indicated that PAPE training can sustain improved vertical jump heights throughout volleyball session. 20 Acupuncture stimulation at the elbow can boost muscle endurance and explosive power for 7–21 min, 11 whereas stimulation at the shoulder acupoints can enhance muscle strength for 10–20 min. 21 Optimization of acupuncture to improve muscle strength is crucial for rehabilitation, especially if considering the decline in knee joint muscle endurance after ACL injury. Therefore, further research is needed to clarify the effectiveness and time-dependent effects of Deqi induced by acupuncture in ACL injury rehabilitation.
This study aimed to examine whether acupuncture at knee-specific acupoints acutely enhances knee muscle endurance in men with chronic partial ACL injury and whether these effects exhibit a time-dependent profile. It is hypothesized that acupuncture at knee joint-related acupoints can enhance knee muscle endurance in men after ACL injuries, with these changes being time-dependent. Furthermore, acupuncture-induced improvements in knee muscle endurance were expected to display a clearly time-dependent pattern across the poststimulation period, thereby informing optimal rehabilitation timing.
Materials and Methods
Trial design
This is a randomized, single-blind, crossover study. All participants received real (RA) and sham acupuncture (SA) interventions with 1-week washout interval, which was sufficient to prevent carryover effects.22–24 The study was approved by the Institutional Ethics Committee of Jilin Sport University (JLSU; Changchun, China; JLSU-IRB no. 2022002) and registered in the Chinese Clinical Trial Register (ChiCTR2200055658). The procedures took place in the biomechanics laboratory. All participants provided informed consent, and the trial complied with the Declaration of Helsinki.
Participants
Sample size calculation
An a priori power analysis was conducted using G*Power software (version 3.1.9.4; Heinrich Heine University Düsseldorf, Düsseldorf, Germany). Based on the medium effect size reported in White’s meta-analysis for acupuncture efficacy in knee dysfunction (Cohen’s d = 0.5), 25 a two-sided significance level of 0.05, statistical power of 0.8, and assumed within-subject correlation of 0.4 were adopted. 23 The analysis indicated that at least 16 participants were required. Twenty active, right-leg-dominant men with chronic (3–6 months postinjury), Magnetic resonance imaging (MRI)-confirmed partial ACL tears were enrolled. To minimize potential sex-based biomechanical heterogeneity, only males were recruited. Inclusion criteria required completion of conservative rehabilitation and medical clearance for sport. Exclusion criteria included concomitant injuries, surgical meniscal tears, prior knee surgery, or a history of needle sensitivity, needle phobia, or prior adverse reactions to acupuncture. Participants refrained from strenuous exercise, caffeine, and alcohol for 48 h pretesting as part of the standardized presession control conditions to ensure stable baselines. Demographics: age 24.37 ± 2.11 years; height 170.82 ± 8.08 cm; mass 66.25 ± 11.03 kg.
Randomization and blinding
An independent coordinator generated the randomization sequence using a computer-generated random number table via a sealed envelope. Stratified block randomization (5 blocks, block size: 4) was used to balance the treatment sequences. Participants were blinded to group allocation. Outcome assessors for isokinetic endurance and biochemical markers, as well as data analysts, were blinded throughout the study. RA and SA treatments were identical except for acupoint selection and needle depth. The acupuncturist was not blinded due to the nature of the intervention. Participant blinding success was evaluated after each session using Bang’s blinding index (BI). 26 The baseline assessments included anthropometry, isokinetic endurance, and blood biochemistry. Both treatments were administered in a crossover design with a 1-week washout. This study adhered to the Consolidated Standards of CONSORT guidelines (Supplementary Table S1) and the STandards for Reporting Interventions in Clinical Trials of Acupuncture (Supplementary Table S2).
Equipment
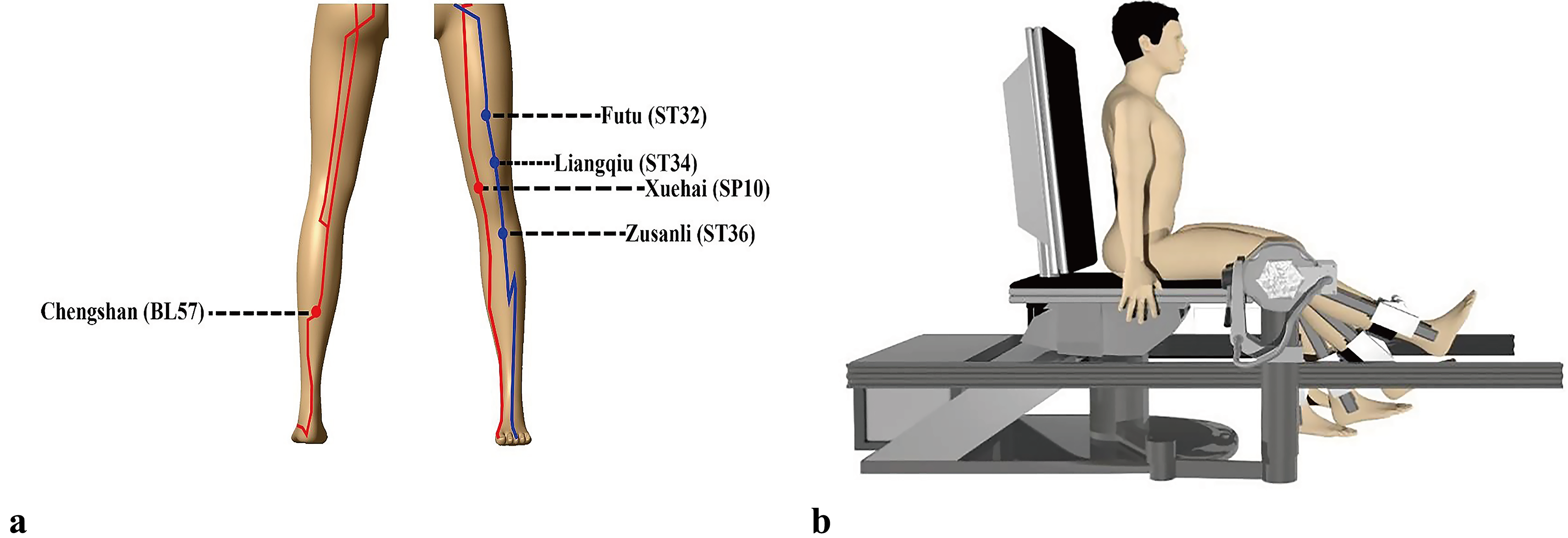
Kinetic data of knee flexion and extension were collected using a Con-Trex isokinetic dynamometer (Con-Trex MJ; CMV AG, Dübendorf, Switzerland; Fig. 1b). Blood biochemical parameters were collected using a Beckman Coulter AU5800 (Beckman Coulter Inc., Brea, CA, USA), Carnitine Assay Kit (Kainos Laboratories Inc., Tokyo, Japan), and Total Glutathione Assay Kit (Beyotime Institute of Biotechnology, Shanghai, China). Acupuncture used 0.25 mm * 40 mm disposable sterile needles (Suzhou Medical Appliance Factory, Suzhou, China). The acupuncturists selected experienced practitioners with relevant professional qualifications, performed the acupuncture part of the experiment, and completed the treatment as required. 21
Acupuncture points
Acupuncture interventions
The trial included two groups: RA and SA. The RA group received acupuncture at the Futu (ST32), Liangqiu (ST34), Zusanli (ST36), Xuehai (SP10), and Chengshan (BL57) sites (Fig. 1a), whereas the SA group received needling 1–3 cm adjacent to these points. All treatment procedures were performed by the same licensed acupuncturist with >6 years of clinical experience to minimize inter-operator variability. In the RA group, the participants were positioned comfortably, and the Ping Bu Ping Xie technique was used. Sterile needles were inserted and manipulated 90–180° with a 0.3–0.5 cm lift-thrust until Deqi was achieved and retained for 15 min. 27 In the SA group, needles were inserted to a depth of 5–30 mm at predefined non-acupoint locations positioned 1–3 cm lateral to the selected acupoints. This depth range was selected to ensure that all insertions remained within the subcutaneous tissue without penetrating muscle, accounting for individual variability in adipose thickness. Needles were retained for 15 min without manipulation to avoid eliciting Deqi sensations or inducing physiological activation. 28 To verify blinding success, Deqi sensations were assessed in both groups following each session.
Safety monitoring
Adverse events (AEs) were prospectively monitored during all intervention sessions in both the acupuncture and control conditions. An AE was defined as any unfavorable or unintended sign, symptom, or event occurring during the study, regardless of its presumed causal relationship with the interventions. All acupuncture sessions were conducted by the same licensed acupuncturist described in the intervention section. After each session, participants were systematically queried using a structured checklist and open-ended questions about discomfort or unexpected symptoms (e.g., localized pain, bruising, dizziness, fatigue, or nausea). Participants were also encouraged to report any concerns spontaneously at any time. Serious AEs were defined as those resulting in death, being life-threatening, requiring hospitalization or prolongation of hospitalization, or causing persistent or significant disability.
Isokinetic parameters
The isokinetic outcomes included maximum torque, peak power, maximum average torque, average work, average power, total work, and joint stiffness. For each experimental trial, testing was conducted under standardized presession control conditions over two consecutive days to ensure consistent neuromuscular readiness. On Day 1 (familiarization), following instrument calibration, participants completed a 6-min jog at 8 km/h, sat with their right leg aligned to the dynamometer axis, and performed five flexion/extension repetitions at 30°/s. On Day 2 (experimental session), a pretest of five maximal concentric contractions at 60°/s was conducted with verbal encouragement. To minimize repeated-testing effects and acute fatigue, the protocol followed a fixed sequence: one pretest, a 15-min acupuncture intervention (applied to specific knee points), and five post-tests. Post-tests (identical to the pretest) were conducted at 3, 13, 23, 33, and 43 min after needle removal, with each separated by a 5-min seated rest interval. Each participant completed one pretest and five post-tests.
Blood biochemical parameters
Blood biochemical test parameters included glucose, creatine, lactate, ammonia, carnitine, and glutathione. In the experiment, all participants underwent two acupuncture interventions, and 10 mL of forearm venous blood was collected pre-exercise, postacupuncture, and postexercise, totaling 30 mL (Fig. 2). Blood lactic acid, ammonia, glucose, and creatine kinase levels were measured using a Beckman Coulter AU5800 analyzer (Beckman Coulter Inc., Brea, CA, USA).

CONSORT flow diagram.
Data processing
Knee joint stiffness was calculated as the change in the joint moment divided by the change in the joint angle. The joint moment was normalized to the body weight of the participant. A Contrex isokinetic dynamometer was used to measure the joint moment and angle during movement.
Statistical analysis
All analyses were performed using MATLAB 2020a (MathWorks, Natick, MA, USA). As all participants completed both trials of this randomized crossover design with no missing data, complete-case analysis was conducted. Potential sequence and period effects were tested in preliminary models. Neither sequence nor period effects were statistically significant (all P > 0.10); therefore, these terms were excluded from the final models to maintain parsimony. Consequently, a two-way repeated measures analysis of variance (ANOVA) (2 groups × 6 time points) was used to assess interactions for isokinetic parameters (maximum torque, peak power, maximum average torque, average work, average power, and total work) and knee flexion/extension stiffness. Similarly, a separate two-way repeated measures ANOVA (2 groups × 3 time points) was used to evaluate blood biomarkers (glucose, creatine kinase, blood ammonia, lactic acid, carnitine, and glutathione). Regarding model assumptions, Mauchly’s test was used to assess sphericity; when the assumption was violated (P < 0.05), the Greenhouse–Geisser correction was applied. Bonferroni post hoc tests were used to compare time points. Effect sizes (Cohen’s d, ES) were categorized as small (0.2–0.5), medium (0.5–0.8), or large (>0.8). 29 To verify within-session measurement consistency, the two-way mixed-effects intraclass correlation coefficient (ICC) was calculated based on repeated assessments in the control condition to ensure that no systematic measurement drift occurred during the testing protocol. Data are reported as mean ± standard deviation, with significance set at P < 0.05.
Results
Blinding and reliability
Bang’s BI was 0.73 (95% confidence interval [CI]: 0.51–0.94) in the RA group, indicating most participants correctly identified their allocation, whereas the SA group’s BI was 0.16 (95% CI: 0.02–0.31), consistent with successful blinding. Thus, blinding was effectively implemented, supporting the reliability of the efficacy results (Table 1). Within-session measurement reliability across the six repeated assessments in the control condition was low to moderate, with ICC values ranging from –0.07 to 0.46.
Bang’s Blinding Index Results
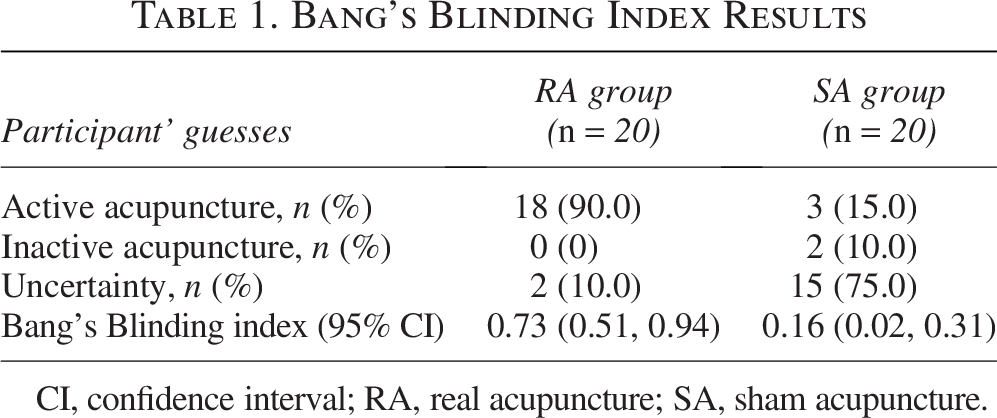
CI, confidence interval; RA, real acupuncture; SA, sham acupuncture.
Safety results
No serious or minor AEs were observed or reported in either the acupuncture or control group throughout the study. Both interventions were well tolerated, with no withdrawals due to safety concerns.
Isokinetic parameters
Figure 3 shows the significant group × time interaction effects for all right knee flexion muscle performance metrics (all P < 0.01). In the RA group, maximum torque, peak power, and average power (Fig. 3a, b, e) increased significantly at post1–post3 versus pre-intervention (all P < 0.05, ES = 0.75–1.63), lasting up to 23 min. Maximum average torque, average work, and total work (Fig. 3c, d, f) improved at post1–post4 (all P < 0.05, ES = 0.80–1.81), persisting up to 33 min. Compared with the SA group, the RA group showed significantly greater peak and average power at post1–post3 (all P < 0.05, ES = 0.68–1.71) and higher maximum torque and maximum average torque at post1–post4 (all P < 0.01, ES = 0.90–1.98). Average and total work were higher in all post-tests (post1–post5; all P < 0.05, ES = 0.68–1.62). These results suggest that RA can enhance knee flexor strength and endurance in men with ACL injuries, with effects lasting 23–33 min.
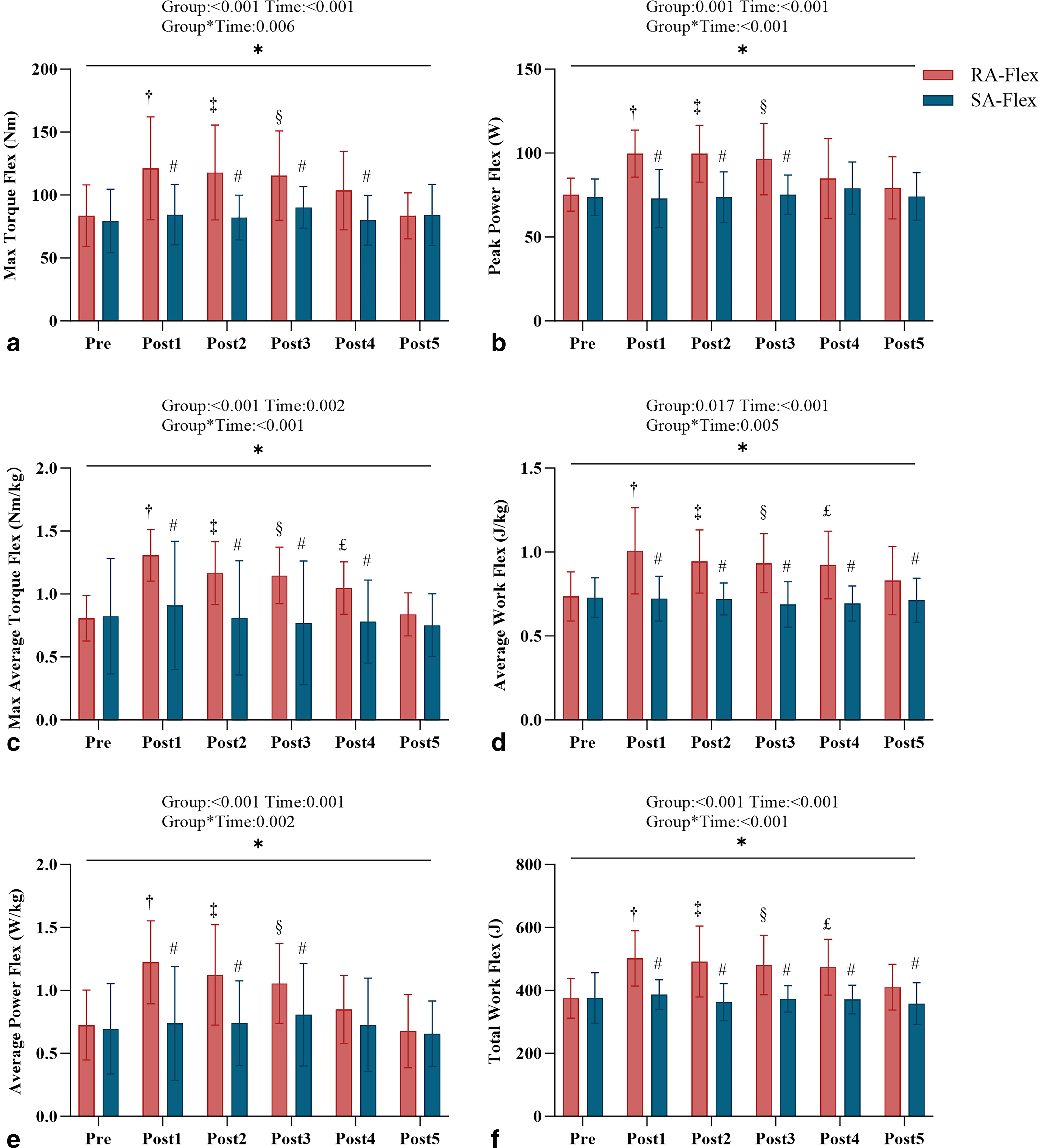
Comparison of flexion motion parameters of knee joint before and after acupuncture. Notes: maximum torque
Figure 4 shows the significant group × time interaction effects for knee extension performance and joint stiffness (all P < 0.05). In the RA group, maximum torque and maximum average torque (Fig. 4a, c) increased significantly at post1–post3 (ES = 0.81–1.70), whereas peak power, average work, average power, and total work (Fig. 4b, d, e, f) improved at post1–post4 (ES = 0.71–1.37), with effects lasting up to 33 min. Compared with SA, RA resulted in significantly greater improvements in torque, power, and work at most postintervention time points (ES = 0.65–1.68), and total work remained elevated through post5 (ES = 0.84–1.65). Joint stiffness during flexion and extension showed significant interaction effects (all P < 0.01; Fig. 4g, h), with flexion stiffness increased at post1–post3 (ES = 0.92–1.12) and extension stiffness at post1–post4 (ES = 0.98–1.06). RA produced greater stiffness improvements than SA, with benefits sustained for 23–33 min (ES = 0.65–1.37). These results suggest that RA may enhance knee joint kinetics in men with ACL injury.
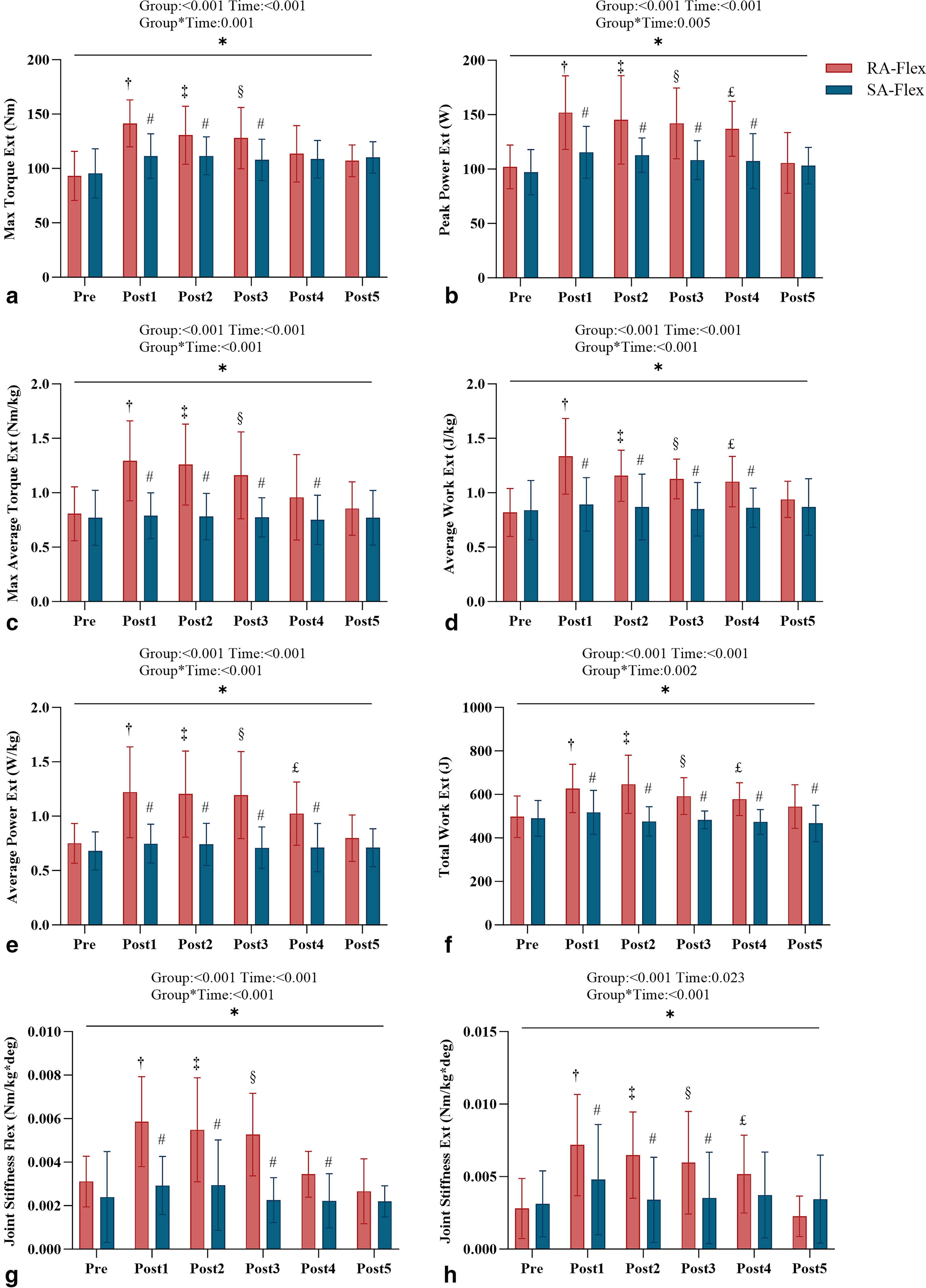
Comparison of extension motion parameters and flexion/extension stiffness value of knee joint before and after acupuncture. Notes: maximum torque
Blood biochemical parameters
Figure 5 shows the significant group × time interaction effects for blood ammonia, lactic acid, and glutathione levels during the knee experiment (all P < 0.05) (Supplementary Table S3). Compared with pre-exercise, blood ammonia, lactic acid, and glutathione (Fig. 5c, d, f,) all increased significantly after exercise (all P < 0.001, ES = 0.58–1.06), indicating that acupuncture can elevate these biochemical markers. Compared with the SA group, the RA group showed significantly lower postexercise blood ammonia and lactic acid levels (all P < 0.05, ES = –1.32–1.50), suggesting that RA may attenuate increases in these metabolites. No significant group × time effects were found for glucose (Fig. 5a), creatine kinase (Fig. 5b), or carnitine (Fig. 5e), though all increased significantly after exercise (all P < 0.05, ES = 0.56–1.44). Overall, RA effectively reduced exercise-induced increases in blood ammonia and lactic acid levels.

Blood biochemical parameters of RA and SA at different time points. Notes: glucose
Discussion
In men with ACL injuries, 15 min of RA at ST32, ST34, ST36, SP10, and BL57 significantly improved isokinetic performance, joint stiffness, and blood biochemical markers of knee flexion/extension. RA produced greater and longer-lasting (23–33 min) enhancements in knee joint kinetics and joint stiffness than SA.
The maximum average torque, total work, peak power, and maximum torque of knee flexion/extension at post1 were higher than those at pretest after RA. Acupuncture could modulate muscle fiber conduction velocity via neuronal activation. 30 If nerves are stimulated, it could facilitate motor unit recruitment and firing rate. 31 Therefore, acupuncture may facilitate muscle fiber contraction and conduction velocities to increase the average peak torque and total work of knee flexors/extensors. In addition, acupuncture may increase the recruitment of high-threshold motor units and autonomic nervous drive through voluntary muscle contractions to induce the PAPE effect. 17 The acute enhancement of neuromuscular explosive power induced by PAPE can counteract peak force loss and improve motor unit power/work output. 18
The average work and power of knee flexion/extension at post1 were higher than those before RA. Muscle strength depends on the recruitment of motor units, whereas the regulation of motor neuron activity is influenced by spinal and supraspinal inputs. 32 Previous investigations found that increased reflex excitability at spinal and supraspinal levels can significantly enhance peak plantar Flex/Ext torque. 33 Neurophysiological measurements of the H-reflex signal indicated that acupuncture can improve spinal motor neuron excitability in patients with stroke. 34 Therefore, the increase in average knee power and work may be associated with reflex activity stimulating the spinal cord regions after RA, which enhances neurotransmitter and neuropeptide release to amplify motor excitability.
After RA, knee flexion/extension joint stiffness at post1 was higher than before. ACL injuries often result in knee stiffness and joint instability. 35 Previous studies have indicated that increased muscle co-contraction enhances knee stiffness, 36 and promoting co-contraction of knee flexor-extensors improves joint stiffness and mechanical impedance. 37 Thus, knee stiffness may be closely related to the coactivation of the agonist and antagonist muscles. In addition, acupuncture may enhance muscle blood flow and local water content, 38 which may indirectly facilitate PAPE production. 17 Acupuncture-induced muscle contraction through mechanisms, such as radial bulging, fiber rotational force, and increased longitudinal passive contraction can enhance the strength and contraction speed of the agonist muscles.18,39 Therefore, the observed increase in knee flexor and extensor strength may be attributed to the acupuncture-induced PAPE, which contributes to greater joint stiffness and mechanical stability.
RA and SA elevate postexercise blood ammonia, lactate, and glutathione levels. Compared with SA, RA induced lower ammonia and lactate levels and higher glutathione levels. During short-term high-intensity exercise, cells generate lactic acid via glycolysis to supplement adenosine triphosphate when oxidative phosphorylation is insufficient.40,41 Elevated lactate levels are often accompanied by increased blood ammonia levels, indicating metabolic stress and muscle fatigue. 42 Previous studies have shown that acupuncture can promote the production of nitric oxide to induce the relaxation of vascular smooth muscle and enhance blood flow in muscle tissue, 43 which can accelerate the clearance rate of lactate and ammonia to reduce postexercise blood ammonia and lactate levels. 44 This is consistent with our findings. Meanwhile, acupuncture has been confirmed to activate the antioxidant enzyme system, 45 inhibiting the excessive production of reactive oxygen species and reactive nitrogen species 46 to alleviate oxidative stress. This may explain why glutathione levels in the RA group were higher than in the SA group. Therefore, acupuncture can effectively improve the metabolic state after exercise to alleviate fatigue.
This finding holds significant clinical implications, as it indicates that effective acupuncture interventions can markedly enhance muscle endurance and joint function within a specific timeframe. Therefore, greater consideration of temporal factors is essential when developing acupuncture rehabilitation protocols. In formulating rehabilitation plans, therapists can leverage this effect window to design exercise regimens. Following acupuncture interventions, exercise training should be scheduled within the 23- to 33-min effect window to promote muscle activation and improve training outcomes. Previous research has found that long-term repeated acupuncture may lead to a gradual reduction in the analgesic effect of acupuncture. 47 However, further studies are needed to explore whether repeated acupuncture can prolong the duration of increased muscle endurance.
Limitations
This study has limitations. The lack of electromyography and hemodynamic measures restricts mechanistic insight into neurophysiological adaptations. In addition, the exclusive recruitment of male limits generalizability, necessitating future inclusion of female subjects. Furthermore, the absence of long-term follow-up and a no-treatment control group prevents the assessment of treatment sustainability and the ruling out of placebo effects, respectively.
Conclusion
This study demonstrates that acupuncture immediately enhances knee endurance in patients with chronic ACL injuries, with benefits persisting for 23–33 min and modulating blood biochemical markers. Consequently, acupuncture should be considered a viable adjunctive modality in ACL rehabilitation protocols. It effectively improves fatigue resistance and lower limb strength, thereby facilitating functional recovery in this specific population.
Authors’ Contributions
I.-L.W. designed the study. I.-L.W. and F.-F.L. wrote and revised the article. I.-L.W. performed the statistical data analysis. L.J.C., J.Y.S., and L.-C.W. performed the experiments. F.-F.L., Y.S., and L.J.C. prepared the figures and tables. J.Y.S., Y.S., and L.-C.W. reviewed and edited the article. All the authors have read and agreed to the published version of the article.
Footnotes
Acknowledgment
The authors would like to thank all the study participants.
Author Disclosure Statement
The authors declare no conflict of interests.
Funding Information
This research was supported by a grant from the Hubei Normal University (GRANT_NUMBER: HS2021RC010).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Ethical Considerations
The trial was approved by the Institutional Ethics Committee of Jilin Sport University (JLSU; Changchun, China; JLSU-IRB no. 2022002) and registered in the Chinese Clinical Trial Register (ChiCTR2200055658).
Data Availability
Data are available from the corresponding author upon request.
Supplemental Material
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.