
Abstract
This study examined the effects of sound-field amplification (SFA) use for children who are deaf or hard of hearing (DHH) with additional diagnosed conditions enrolled in preschool and first and second grades in a rural district. Four focus children who are DHH with additional diagnoses were matched with hearing peers and observed for attending behaviors and latency in compliance to following routine directions with introduction of SFA. The study used a single-case multiple probe across participants design. All participants demonstrated improved attending behaviors and compliance to directions with SFA, with the focus children who are DHH with additional diagnoses showing stronger results than their hearing peers. Teachers indicated SFA was beneficial to the children who are DHH and they would use it again. SFA is an effective strategy to improve access to educational opportunities by increasing attending behaviors and promoting participation for children who are DHH with other diagnoses in special and general education preschool and first and second grades.
Keywords
Preschool and early elementary-age children rely on listening to obtain most of their input for learning. However, noise is inherent in the educational setting and teachers often compete to be heard against environmental and classroom noise. Children who have conditions predisposing them to either hearing loss (HL) or other learning difficulties may benefit from a more favorable listening environment than that required by children who have typical development. It is widely known that children demonstrate more effective learning behaviors if they can hear a clearer, closer, more consistent message (Boswell, 2006).
Noise in the Classroom
Noise levels in classrooms typically far exceed the acoustical recommendation for children with normal hearing (Cornwell & Evans, 2001). Even within unoccupied classrooms, noise levels frequently exceed noise thresholds recommended for learning (Leung & McPherson, 2006; Massie & Dillon, 2006). Not only do classroom noise levels affect young children’s speech reception, but signal-to-noise ratio (SNR) and reverberation affect reception. The SNR compares the level of a desired signal with the level of background noise, whereas reverberation is the decay as the sound is absorbed by the surfaces of objects in the environment (Johnson, 2000). Current recommendations are that background sound level in an unoccupied classroom should not exceed 35 dB (American Speech-Language-Hearing Association [ASHA], n.d.). In addition, distance from the sound source to the recipient is a critical factor in affecting speech perception (Crandell & Smaldino, 2000) with increased distance degrading message reception. When in close proximity, a teacher produces sound waves that transmit directly to a child with little interference from reverberation. Crandell and Smaldino (2000) discuss the impact of critical distance on message reception: The critical distance of the room refers to the point in the room where the level of the direct sound and the level of the reverberant sound are essentially equal . . . Beyond the critical distance, the direct sound from the speaker arrives at the listener initially, but is followed by reverberated signals . . . the reflected sound reaching the listener will contain a different acoustical content. (p. 366)
Although the critical distance of 0.9 to 1.8 m is ideal, it may not be achievable for all listening activities (Crandell & Smaldino, 2000). The distance between a child and the instructing teacher influences the speech perception of the child regardless of hearing ability. Speech perception can be increased by changing the child’s location to a place within the critical distance, relatively close to the teacher (Crandell, 1991; Crandell & Bess, 1986; Leavitt & Flexer, 1991). A child with HL should be situated where the primary signal is presented within the critical listening distance to gain full access to verbal instruction (ASHA, 2002; Anderson, 2010).
Sound-Field Amplification (SFA)
SFA aids acoustic accessibility to a teacher’s instruction for everyone in the room (Flexer & Long, 2003) and is critical for children diagnosed as deaf or hard of hearing (DHH). Although children who are DHH will often use personal hearing aids, these do not overcome the negative effects of distance, noise, and reverberation. Therefore, additional accommodations are needed. The purpose of SFA is to intensify the instructional sound source above environmental background noise, creating a favorable SNR throughout the classroom (Larsen & Blair, 2008). Amplification of the teacher’s voice produces a consistent signal regardless of the teacher’s distance from the student (Anderson & Goldstein, 2004). A favorable SNR for children who are DHH should equal or exceed +15 dB (Crandell & Smaldino, 2000), which is unachievable without intervention. A common example of a 15-dB gain in amplification would be the difference of the sound of a shower to that of a snow blower.
The benefits of SFA have been researched regarding effects on room acoustics with various populations. Numerous researchers have studied the benefit of using SFA systems to improve general listening conditions (e.g., Anderson & Goldstein, 2004; Crandell et al., 2001; Kazmierczak-Murray & Downes, 2015; Wilson et al., 2011). Research with amplification includes students with varying diagnoses such as those with Down syndrome (Bennetts & Flynn, 2002), emotional and behavioral disorders (EBDs; Maag & Anderson, 2006), and attention deficit hyperactivity disorder (ADHD; Maag & Anderson, 2007). Cornwell and Evans (2001) studied the attending factors of students with attending difficulties and their peers. All these studies found SFA beneficial.
Two studies on SFA with special populations of children conducted by Maag and Anderson (2006, 2007) were specific to speed of response to directions. Their initial study involved elementary-aged students with EBD; they subsequently studied three children, kindergarten through second grade, diagnosed with ADHD. The initial study demonstrated all participants increased their rate of compliance with task demands, whereas the second resulted in reduced time necessary to comply with task demands, both with the activation of SFA.
SFA Research for the Early Childhood Population
The need for early intervention for young children who are DHH is well established (Holstrum et al., 2008). As early as 1998, Bess, Dodd-Murphy, and Parker recommended providing families of children with unilateral losses and minimal HLs educational information regarding amplification as well as the creation of acoustically supportive environments such as SFA. Unfortunately, there has been little research on the use of SFA systems in academic settings for preschool-age children who are DHH (Nelson et al., 2013). When young children who are DHH have additional diagnoses, the research is even more sparse. This dearth of literature specific to SFA amplification for young children who are DHH emphasizes the need for increased study to further augment the current evidence base of classroom interventions.
Rural Services for Students Who Are DHH
Students who are DHH are likely to receive support from a teacher of the DHH (TODHH) via an itinerant model with student placement being in a general education classroom (Antia & Rivera, 2016), with such service delivery being particularly extensive in rural areas (National Deaf Center [NDC] on Postsecondary Outcomes, 2017). In rural communities, a TODHH can have extensive geographical areas to cover, resulting in students who are DHH receiving services directly from the TODHH 1 to 2 times per week to only once per month (Checker et al., 2009). If caseloads or geographical barriers result in such infrequent services provided directly by a TODHH, it becomes important for the TODHH to increase the skills of the classroom teachers who are working daily with students who are DHH. The NDC on Postsecondary Outcomes (2017) suggests that ensuring teachers in rural areas are trained in the use of technology is particularly important in meeting the needs of students who are DHH in those communities. Providing training to rural classroom teachers on the use of SFA systems is one means of addressing the unique educational needs of students who are DHH.
Purpose of the Study
The goal of this study was to determine how SFA affects learning behaviors of children who are DHH with additional diagnoses who attended preschool, first-grade, or second-grade classes in a rural school district. The research questions are as follows:
Furthermore, these research questions were being addressed in the context of a rural, itinerant TODHH providing training to the classroom teachers to use SFA.
Method
Participants
Prior to starting the study, approval was attained from the university’s institutional review board and informed consent was obtained for all participants. Pseudonyms are used to protect identities. Inclusion criteria for focus children for this study required children meet the state’s hard of hearing eligibility criteria, have an additional diagnosis, and be enrolled in preschool, first grade, or second grade. All students within the rural school district who met these criteria were included in the study. Inclusion criteria for the peers were hearing within normal limits and enrollment in the same class as the focus student with whom paired. A third criterion required being recognized, through general education teacher nomination based on teacher perceptions, as similar in personality to the focus students to increase the likelihood those with outgoing and/or introverted personalities would match. Peer participants matching these criteria were chosen randomly from each classroom, which resulted in mixed gender matching.
Focus participants and peers
Children who are DHH were recruited within a rural school district in a Western state. Four children eligible as DHH with additional diagnosis and served by an itinerant TODHH were the focus participants. Peer participants’ hearing was screened prior to the onset of the study to ensure it was within normal limits.
Susie
Susie, a 4-year-old White female identified as having HL at 30 months and later diagnosed with Usher syndrome, attended a community preschool. Diagnosed with a moderate to severe bilateral sensorineural HL averaging 53 dB HL (pure tone average [PTA]) with some conductive history, she wore hearing aids behind each ear. Susie’s aided speech reception threshold was 30 dB. She had a history of pressure equalization (PE) tubes in each ear to prevent accumulation of middle ear fluid. Her aided hearing allowed her to hear sounds within the speech range. Susie’s academic performance was at the level of her peers without disabilities; she had no language delay. Susie’s peer, Sonia, was a 4-year-old White female with typical development, who attended the same community preschool class.
Amelia
Amelia, a 3-year-old White female with an educational diagnosis of developmental delay due to Down syndrome and associated motor delays, attended a district early childhood special education (ECSE) class. She was diagnosed with a mild bilateral sensorineural HL, averaging 30 dB HL (PTA), at the age of 18 months without history of conductive HL. Amelia’s speech reception thresholds were 15 dB. She began wearing hearing aids at 2 years of age. She was consistently aided during school hours and was within the normal hearing range when aided. Amelia displayed a language delay of approximately 2 years; in her ECSE class, she was learning colors, numbers, and names of familiar objects as this educational experience was her first exposure to language and language concepts. Amelia’s peer was Amy, a 3-year-old White female who had developmental delays (a requirement for attendance in the ECSE classroom).
Martin
Martin, a 7-year-old second-grade White student with Stickler syndrome with HL diagnosed at age 14 months, was eligible as deafblind due to bilateral sensorineural HL averaging 43.7 dB HL (PTA) and accompanying vision impairment. Aided speech reception thresholds were 45 dB. He previously had unilateral cataract surgery. He was prescribed corrective lenses and hearing aids and wore both glasses and aids consistently, with the exception of having lost one hearing aid for 3 months prior to the study. Aided, his hearing was within the normal hearing range. Martin was delayed in language (approximately 3-year delay) as well as in academic skills such as math-related concepts (approximately a 1-year delay). Martin’s peer Mary was a 7-year-old White female who attended the same second-grade class.
Jason
Jason, a 7-year-old Asian and White male whose HL was identified at age 6 years, was in a general education first-grade class. He was diagnosed with a mild to moderate bilateral “cookie-bite”–shaped sensorineural HL (meaning he could not hear midfrequency sounds but could hear low- and high-frequency sounds) that averaged 43 dB HL (PTA) unaided with 45 dB speech reception threshold. He received amplification within 2 months of identification but was inconsistent with use and frequently lost his hearing aids. He was previously diagnosed with ADHD, which was addressed through a behavior plan associated with his Individualized Education Program (IEP). He was prescribed medication for his ADHD 4 months prior to the initiation of the study, which was consistently administered daily throughout the study. He wore two hearing aids with consistent amplification for the duration of the study. Aided acuity was within the normal hearing range. Jason’s language was within the typical range for his age; he was delayed approximately 1 year in academics. Jason’s peer, John, was a 6-year-old White male who attended the same first-grade class.
Teacher participants
Teacher participants were from the participating children’s classes. Each class had one teacher, with the exception of the private community preschool, which had two co-teachers. The teachers’ experience levels varied, but all were licensed educators with at least 5 years experience (see Table 1).
Demographics of Teacher Participants and Focus Participant.
Note. ECSE = early childhood special education.
Setting
This study was conducted in two educational settings: a public elementary school (three different classrooms) and a private community preschool, both located in a Western state in a rural, county-based school district with a recently declining enrollment of 7,000 students. This district was identified as rural by the state department of education as well as by the Rural Education Achievement Program (U.S. Department of Education, 2019). This county-based, rural school district covered 738 square miles. Data for 2012 to 2016 showed the total population of this school district as 47,426 in 19,928 households with a median income of US$59,769 (National Center for Education Statistics [NCES], 2019). Poverty was indicated as 16.1% of families with income below the poverty level and 18.6% of families with Food Stamps/Supplemental Nutrition Assistance Program (SNAP) benefits (NCES, 2019).
ECSE classroom
The ECSE classroom, with centers including building materials, home making, tub and toy areas, a library, a sink, and circle area, was an exterior room with a bank of high windows facing the front of the school, sidewalk, bus lane, and parking lot. This room was 8.53 m × 8.53 m and had an additional 0.6 m × 1.21 m library area with a couch and floor pillows. The SFA speaker was placed on top of a low shelving unit near the circle area. This class enrolled 16 students, all eligible for special education, with one teacher and a paraprofessional.
First-grade classroom
The general education first-grade classroom was an interior 8.53 m × 8.53 m room located in the middle of an interior hall, bordering the multipurpose cafeteria. It had one partial set of sealed windows facing the hall. This class had a learning center with a kidney-shaped table, student groups of four tables with four to six chairs, a rocking chair, and a desk with a computer. The SFA speaker was placed atop a low shelving unit near where the teacher typically instructed. The class had 15 children with one teacher.
Second-grade classroom
The general education second-grade classroom, 8.53 m × 8.53 m, was an exterior room with a partial bank of small high hung exterior windows facing the playground and a partial set of sealed windows facing the hall on the opposite wall. The classroom had a learning center with a kidney-shaped table and chairs, and four groupings of student desks with chairs arranged in groups of four. There was an open floor area between two book cases, which was often used for group activities. The SFA speaker was placed on a low table near where the teacher typically instructed. The class had 16 students with one teacher.
Community preschool
The private faith-based preschool had 12 to 22 students (number attending varied due to unique student schedules) and two teachers and comprised two rooms, totaling 55.74 m2, with a coat room connecting them. The classroom used for this study was an elongated “L”-shaped room located on two exterior walls with both interior and exterior doors. It had a set of windows bordering the long side of the room and another set on the end. The SFA speaker was atop a low shelving unit. This preschool had the items discussed in the ECSE setting with the addition of a variety of independent Montessori-type exploratory jobs.
Materials
SFA equipment
Prior to intervention, Front-Row-to-Go SFA systems (https://www.gofrontrow.com/en/products/togo-system) were purchased by the school district and installed in each classroom. During intervention, the teacher wore a Behind-the-Neck Boom Microphone (890-88-300-00) connected to a body-worn transmitter (925T-216). Via FM radio wave technology, the teacher’s voice was transmitted across the room to the amplifier located on a single Column Speaker Receiver (925RS-216).
Speaker setup was accomplished by identifying the primary teaching locations of the teacher and electrical outlets. A single speaker was placed on a stand, at least 1.5 m from electrical equipment, at the ear level of the children. The volume of the teacher’s voice was determined to provide a positive SNR of approximately 15 dB greater teacher voice than room noise to each area within the classroom. A handheld transmitter (wireless microphone; 925H) was provided for class participation.
Teacher daily FM checklist
Teacher training within the intervention focused on using the SFA system accurately and appropriately. The teacher daily FM checklist served as a guideline for using the SFA system and ensuring correct activation of the system. The checklist reflected the procedure followed in teacher training along with troubleshooting and contact information. (See the supplemental material for the checklist.)
Listening Inventory for Education (LIFE)
One purpose of the LIFE (Anderson & Smaldino, 1998) is to determine efficacy of SFA use for a particular student in an educational setting. The LIFE Teacher Appraisal is a postexperience component composed of 16 questions themed to assess teacher’s perception of positive, negative, or no change in student’s attention, comprehension, or involvement in the educational process while using SFA. Items on the LIFE rate degree of perceived change on a Likert-type scale, from disagree (−2), to no change (0), to agree (+2) for all items except Question 16, noting the perceived total benefit to the student, which is weighted from +5 to −5.
The LIFE Scale total score ranges from −35 to +35 to reflect the extent of benefit of an intervention. The markers on the scale identify +35 as indicating strong support for positive change: use is highly beneficial, +17 indicating support for positive change: use is beneficial, 0 indicating there is no change: benefit of use not identified, −17 indicating support for negative change: use is unfavorable, and −35 indicating strong support for negative change: use is highly unfavorable.
Psychometrics for the LIFE were requested from the authors who reported the “original questions were developed and reviewed by a group of practicing educational audiologists who provided critique and feedback for improvement.” It was also reported “the areas covered by the LIFE were gathered from real experiences of many educational audiologists and have very high face validity. The LIFE is meant to be a comparative scale and so norms for the items were not developed” (K. Anderson & J. Smaldino, personal communication, December 15, 2011).
Experimental Design
A multiple probe research design across participants and behaviors was used (Horner & Baer, 1978; Kennedy, 2005). This design ruled out extraneous causes for children’s improvement in attending behaviors and latency in following directions and determined whether a functional relation existed between student behaviors and the intervention. Experimental control is demonstrated within a multiple probe design by collecting probe data across a minimum of three tiers and showing that when intervention is applied (in this case SFA), and only during intervention, a change in behavior occurs. The criteria for moving from probe condition to intervention were that probe data needed to be stable immediately preceding introduction of the intervention. In addition, intervention needed to result in a therapeutic change, demonstrated by at least two data points, signifying the intervention was having the desired effect (i.e., latencies decreasing or attending increasing) as evidenced by changes in level and trend as well as decreased variability, if relevant, in the first tier prior to implementation in the second tier. Subsequently, similar changes in data were required in the second and third tiers prior to introduction of the intervention for the third and fourth tiers. That is, prior to subsequent intervention in a later tier, at least two intervention data points needed to be at an improved level in comparison with probe condition data; response latencies needed to be lower than probe condition data and attending needed to be higher than probe condition data.
Dependent Variables and Data Collection
Attending behaviors
The operational definition for attending behaviors, as obtained from a behavior tracking form developed by Hunter (2004), included the student (a) watching the teacher’s activity appropriately, (b) observing their own copy, (c) watching a model being presented, (d) watching while waiting, (e) following a direction, (f) asking or answering a topic-related question, or (g) participating in the activity. Nonexemplars included (a) watching a peer unrelated to the activity, (b) moving around without purpose, (c) withdrawing from the activity, or (d) playing with a body part, clothing, or other irrelevant item. Nonexemplars were included for defining the types of behaviors that would not be coded as attending.
Videoed observations occurred at least once weekly for a minimum of 7 weeks for 15-min whole- or small-group sessions; observations occurred during consistent activities for each focus participant throughout the study. Videos were transferred to DVD and viewed to code attending behavior. Both focus and peer participants were coded either yes (l) or no (0) for presence of any of the attending behaviors at 15-s intervals, using a momentary time sampling data collection method. Coding was done by freezing the video at the 15-s interval, starting with the first available interval on the video from the following choices: 00, 15, 30, or 45 s taken from the time displayed on the video. The number of intervals in which attending behaviors were observed were summed and divided by the total number of possible opportunities (60) in the 15-min observation to produce a percentage of intervals of attending behaviors.
Latency in following directions
In the 15-min videoed observations, following directions was measured by recording the length of time it took to initiate an action in response to a routine direction. Latency for following directions was measured per direction from the conclusion of the last word of a direction given to the initiation of the student’s response to the direction. Directions were given during routine teacher-directed whole- or small-group activities. To ensure a consistent number of directions were observed for each participant, only the first 10 directions given during an observation session were coded. By observing participant response to the first 10 directions for all participants, there are no potential discrepancies in participant responding due to teachers varying the number of directions in a 15-min period. For example, if one teacher provided a greater number of directions in comparison with other teachers, there could be resulting participant fatigue and changes in latency to directions occurring later in the observation period due to the large number of directions, thus, affecting the average latency. Observing only the first 10 directions kept this variable constant across all participants.
Interrater reliability
Observations were videoed and scored by two independent observers trained to an interrater reliability level of .80 using a protocol that included a research summary, definitions, exemplars and nonexemplars, and practice. The primary observer was the first author who also trained the secondary observer, a doctoral student who was naive to the purpose of the study, to serve as the reliability observer. Interrater reliability is reported for each participant for both attending behaviors and latency in following directions. Interrater reliability was calculated for both dependent variables using the point-by-point approach employing this formula (Ledford et al., 2018): number of agreements ÷ number of agreements + number of disagreements × 100. The convention for interrater agreement used in applied research is achievement of a minimum of 80% agreement, based upon 20% to 33% of the observations for each participant (Kennedy, 2005) in each phase.
Interrater reliability met or exceeded these minimal standards across all focus participants. For the focus participants during the probe condition for attending behaviors, interrater reliability occurred in a minimum of 43% of sessions (across all focus participants) with a mean of 88% agreement (range = 80%–99%). During intervention for attending behaviors for the focus participants, interrater reliability occurred in a minimum of 37% of the sessions with a mean of 91.5% agreement (range = 80%–99%). Interrater reliability was similarly high for latency to responding to directions for all focus participants. During the probe condition for latency, interrater reliability occurred for a minimum of 43% of the sessions (across all focus participants) with a mean agreement of 95% (range = 80%–100%). Interrater reliability for latency occurred during a minimum of 37% of sessions across all focus participants with a mean agreement of 97% (range = 80%–100%).
For the peer participants during the probe condition for attending behaviors, interrater reliability occurred in a minimum of 43% of sessions (across all peer participants) with a mean of 89.4% agreement (range = 80%–95.5%). During intervention for attending behaviors for the peer participants, interrater reliability occurred in a minimum of 37% of the sessions with a mean of 92.4% agreement (range = 83.6%–97.7%). Interrater reliability was similarly high for latency to responding to directions for all peer participants. During the probe condition for latency, interrater reliability occurred for a minimum of 43% of the sessions (across all peer participants) with a mean agreement of 93.6% (range = 75%–100%). Interrater reliability for latency occurred during a minimum of 37% of sessions across all participants with a mean agreement of 95.8% (range = 80%–100%).
Procedure
Probe condition
Prior to the start of the probe condition, classroom noise levels were measured by the first author to correctly set the SFA system at the recommended volume of 15 dB above background noise. Consistent probe conditions occurred across focus participants to determine whether the targeted behaviors were occurring at a stable level prior to intervention (Kennedy, 2005).
Teachers provided a routine 15-min activity for each probe condition observation according to their usual schedules but without SFA. Activity sessions were videoed with the teacher, focus participant, and peer participant visible in the viewfinder. This allowed the probe condition to be established for both the studied variables, attending behaviors and latency of response to routine directions. The probe condition was established using a multiple probe approach for each of the dependent variables across participants at each of the four sites.
Intervention
Once a stable probe condition was established, the TODHH installed SFA equipment in the classroom according to manufacturer recommendations, in a staggered manner consistent with the research design. Classroom noise levels were measured with occupied noise levels ranging between 48 and 65 dB during unstructured times and 35 to 43 dB during whole group instruction. The system was set at a +15 dB signal above the classroom noise level occurring during structured activities, as measured halfway between the teacher’s primary teaching location and the SFA equipment. Structured activities were used as this was when data were collected.
Routine classroom activities continued to be presented with the addition of the SFA intervention. Attending behaviors and response to directions were assessed through data collected from 15-min videoed observations with SFA activation. Teachers were observed for fidelity in their use of the SFA system.
Procedural Fidelity
To ensure the intervention is responsible for changes to the dependent variables, it is essential the intervention be implemented as intended. Procedural fidelity is a measure of implementation of the defined intervention as well as the absence of intervention during the probe condition. The first author, the district’s itinerant TODHH students, individually trained each teacher on the use of SFA equipment in accordance with a teacher training protocol from the manufacturer’s operating procedures manual. All teachers were trained in the same manner to ensure their competency to correctly use the SFA system, checking off steps on the protocol as they were covered in the training. Teachers’ independent use of the system was a prerequisite to the activation of SFA during the study. Identification of equipment parts, operation procedures, demonstration of system use, practice to 100% independence, and an opportunity for questions were training components. Trainings were videoed to review for consistency. Following teacher training, teacher daily checklists were distributed and explained to serve as a procedural reminder and troubleshooting guide regarding system operation. The first author implemented this training with 100% fidelity and each teacher demonstrated 100% correct use of the system during training.
During the intervention phase, teachers were observed by the first author, using the checklist in the supplemental material, for consistent use of SFA. The results of the teacher fidelity protocol indicated SFA use was 100% consistent during observations with equipment set appropriately in 21 out of 22 instances across teachers. Handheld microphone use varied by teachers as was expected given that teachers were taught to use it as appropriate, based on the activities occurring. It is also important to note the SFA was appropriately absent during probe condition sessions, demonstrating 100% compliance with probe condition procedures across all participants.
Social Validity
Social validity is defined as the “importance, effectiveness, appropriateness, and/or satisfaction various people experience in relation to a particular intervention” (Kennedy, 2005, p. 219). Social validity data were gathered using the LIFE (Anderson & Smaldino, 1998) to evaluate teacher perspectives of the efficacy the focus children experienced during intervention.
The 5-point Likert-type scale on the LIFE assessed teachers’ opinions about the SFA system and their perceptions regarding their children’s responses to SFA. Scores were totaled for collective teacher ratings. The two items noting the areas of greatest effect SFA had on the focus children who are DHH were the questions dealing with attention to whole group directions and following directions more quickly or easily. The items with the weakest teacher responses, or perceived efficacy for the focus children who are DHH, were two questions pertaining to speed in comprehending instruction and involvement in peer conversations. Use of the handheld microphone, which varied, might have affected peer conversations. Mrs. Sweet and Mrs. Young (the community preschool co-teachers for Susie) and Mrs. Evans (ECSE teacher for Amelia) used the SFA systems the longest (i.e., first two sites to receive intervention) and scored the highest efficacy ratings. Ms. Gold (second-grade teacher for Martin) and Mrs. Jones (first-grade teacher for Jason), whose classes were last for intervention, were the lowest scoring.
All teachers in the present study viewed SFA as beneficial. The scores of Ms. Gold (second-grade teacher for Martin) and Mrs. Jones (first-grade teacher for Jason), the lowest scoring teachers, were +13 and +22, indicating “support for change: use is beneficial.” Mrs. Sweet and Mrs. Young (community preschool co-teachers for Susie) and Mrs. Evans (ECSE teacher for Amelia) reported total scores for each of their focus children who are DHH of +34, +33, and +35, respectively, indicating “strong support for positive change: use is highly beneficial.”
Results
Attending Behavior
Susie
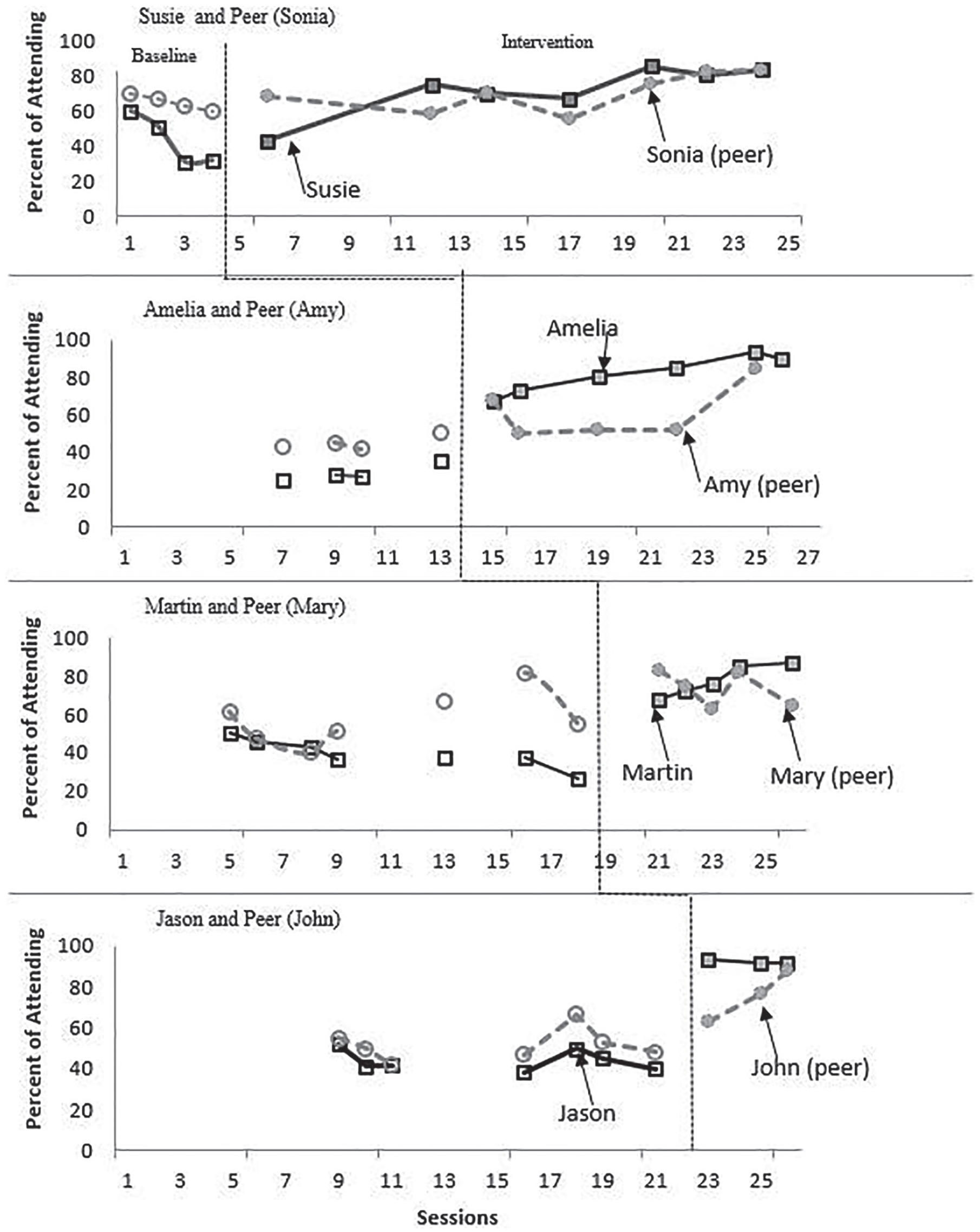
During the probe condition, there was a low degree of variability (see Figure 1) and a decelerating trend in Susie’s attending behavior. Upon intervention, there was a change in level as well as an accelerating trend. Only the initial intervention data point (i.e., one of seven data points) overlapped with the probe condition, resulting in 86% of nonoverlap.
Percent intervals attending.
Sonia (Susie’s peer)
Sonia exhibited a decelerating trend in the probe condition, with a low degree of variability. During intervention, she showed a slight change in level upon introduction of SFA, gradually accelerating trend, and low variability. Inspection revealed two of seven data points overlapped with Sonia’s probe condition data (i.e., 71% of nonoverlap). She increased attending behaviors, benefiting from the use of SFA to some degree, but was less affected by SFA than was Susie.
Amelia
During the probe condition, Amelia’s data revealed a slight accelerating trend with low variability. After the SFA intervention was introduced, her attending behavior displayed an immediate change in level and an accelerating trend, without variability. There was no overlap of the data points between the intervention and the probe condition, resulting in 100% nonoverlap.
Amy (Amelia’s peer)
Amy exhibited a zero-celerating probe condition parallel to Amelia’s but roughly 20 points above, with a low degree of variability. During intervention, her behavior immediately changed in level and showed a slightly accelerating trend. One of five intervention data points overlapped with her probe condition for 80% nonoverlap.
Martin
During the probe condition, there was an initial but low degree of variability, with a slight decelerating trend. Upon intervention, Martin displayed an immediate increase in the level of attending behavior and a steadily, accelerating trend. None of Martin’s five intervention data points overlapped with the probe condition (i.e., 100% nonoverlap).
Mary (Martin’s peer)
Mary exhibited a somewhat accelerating trend in the probe condition. Upon intervention, there was an immediate change in the level of the data. However, visual inspection revealed almost complete overlap of four of the five intervention points with her probe condition data (i.e., only 20% nonoverlap).
Jason
Jason’s probe condition data were relatively flat. Upon intervention, there was an immediate increase in the level of attending behavior with a steadily accelerating trend. Furthermore, there were 100% nonoverlapping data points with the probe condition.
John (Jason’s peer)
John also exhibited a relatively flat probe condition, with a low degree of variability. Upon intervention, John demonstrated an immediate change in level with an accelerating trend. There were 67% of nonoverlapping intervention data with the probe condition (i.e., one of three data points overlapped)
Summary
Attending behavior increased for both focus and peer participants from the probe condition to intervention. These data demonstrated that all children who are DHH exhibited attending behavior less consistently than their matched peers did in the probe condition. All participants increased attending behavior in intervention.
Latency in Following Directions
Susie
During the probe condition, Susie’s latency for following directions showed a low degree of variability and a slightly decelerating trend (see Figure 2). Upon intervention, there was an immediate drop in the level of latency for following directions, a decelerating trend, with low variability. None of the eight intervention data points overlapped with the probe condition (i.e., 100% nonoverlap).

Response latency to directions.
Sonia (Susie’s peer)
Sonia’s data were zero-celerating in the probe condition. Upon intervention, she demonstrated an immediate drop in response latency, with low variability except for one data point. Two of eight intervention data points overlapped with her probe condition (i.e., 75% nonoverlapping data in intervention).
Amelia
During the probe condition, there was an accelerating trend with low variability. Upon intervention, the level of Amelia’s speed of compliance immediately showed a decrease in level and her performance showed a relatively flat trend, with low variability. There was no overlap of data points between the intervention and the probe condition, resulting in 100% nonoverlap.
Amy (Amelia’s peer)
Amy exhibited a variable probe condition. Upon intervention, there was an immediate drop in level representing a shorter response latency, with less variability in comparison with the probe condition. Also evident were four of six intervention data points overlapping with the probe condition (i.e., 33% nonoverlapping data).
Martin
During the probe condition, there was a low degree of variability and a slightly decelerating trend. Upon intervention, Martin’s data displayed an immediate and dramatic change in level resulting in a greatly reduced level of latency in following directions. None of the five intervention data points overlapped with the probe condition (i.e., 100% nonoverlap).
Mary (Martin’s peer)
Mary exhibited a decelerating trend in the probe condition, with a high degree of variability. Upon intervention, there was a countertherapeutic increase in level with a continued decelerating trend, with some variability. Furthermore, three of five intervention data points overlapped with probe condition data for this peer (i.e., 40% nonoverlap).
Jason
During the probe condition, Jason’s data revealed a low degree of variability and a slightly decelerating trend. Upon intervention, there was little immediacy of effect with the first intervention data point only 2 s less than the last data point of the probe condition. There was a slight decelerating trend and low variability. There was 67% of nonoverlapping intervention data with the probe condition (i.e., one of three data points overlapped).
John (Jason’s peer)
John exhibited a decelerating trend in the probe condition, with a high degree of variability. Upon intervention, there was little immediacy of effect, with the initial intervention data point slightly increasing in a countertherapeutic direction. Although John’s data demonstrated a more consistent decelerating trend in intervention compared with the probe condition. All three intervention points overlapped with the probe condition (i.e., 0% nonoverlap).
Summary
During the probe conditions, all focus children who are DHH had slower response latencies than their peers in following directions. Latency appropriately decreased for all participants in intervention, meaning they all responded more quickly with the SFA intervention. In intervention, three of the four focus children who are DHH demonstrated a faster response in comparison with their matched peers.
Discussion
The findings of this study include strong results for use of SFA for early childhood age children who are DHH with additional diagnoses and who were receiving their educational services in a rural district. The district TODHH (i.e., the first author) successfully taught classroom teachers in this rural area use of the SFA system with high fidelity, which resulted in increased attending and decreased latency in compliance to directions.
SFA proved to be effective in improving their behavior for attending and for latency to compliance with directions. Intervention was also effective for their peers’ attending behavior, but not as effective as for the focus children who are DHH. This finding is in agreement with Cornwell and Evans (2001), who studied attending behaviors using SFA for participants who presented with difficulty attending and being easily distracted and who demonstrated clear improvement in attending behaviors with introduction of SFA for participants with ADHD. The results for Jason, the student in the current study diagnosed with ADHD, coincide.
Latency to compliance with directions was derived from the limitations of Maag and Anderson’s (2007) research. They suggested future research set session lengths with latency for each session graphed over weeks, as opposed to the individual data points they graphed over a few days. The present study fulfilled that suggestion adding to the literature. Findings include strong results for all focus children who are DHH with additional diagnoses, and for three of four of their peers for latency of response to directions for classroom routines with SFA intervention. Jason (the student with ADHD) and his peer, John, received SFA in the last week of school, which may have affected their results. The peers’ results for latency of response, although improved, were not as definitive as the focus participants.
The results of this current study concur with the findings of both of Maag and Anderson’s (2006, 2007) and Palmer’s (1998): SFA decreased the latency of compliance for children in following directions. Children who are DHH with additional diagnoses complied more quickly following directions given with SFA as compared with their peers. All focus children who are DHH improved their participation and compliance to directions in general and special education classrooms. In comparison, peers did not demonstrate as strong a response, although positive responses were noted for all. Peer responses were greater in attending than in speed of response to directions.
This study demonstrated clearly that children of early childhood age, preschool to 8 years, benefit from SFA intervention. SFA was highly effective for the children who are DHH who fall within the critical language-acquisition period from birth through 7 years. Results demonstrated improved attending behavior and responsiveness to teacher’s directions. Increased attending behavior with SFA provided these young learners access to expand their language and develop understanding. As a result, these early childhood focus children who are DHH responded faster to teacher’s directions.
SFA was effective for early childhood peers across settings. There was a greater effect on increasing attending behaviors than reducing the response time to teachers’ directions for peers. The effect was not as great as it was for the focus children who are DHH in any educational setting. Given the improved attending behaviors and compliance to directions for children in general education as well as those with HL and other special concerns, renovation of acoustic conditions such as adding SFA in all classrooms could potentially benefit learning for all.
Limitations
One way to view study results is in light of What Works Clearinghouse (WWC, 2017) standards to determine the quality of a study. The current study provides three demonstrations of experimental control across both attending and latency in responding to directions for focus participants and meets WWC standards with reservations for a multiple probe design due to having only four probes in some probe conditions. In a multiple probe design, a total of five baseline probes are needed to meet WWC standards.
In terms of external validity, the study included a small number of focus participants, which limits the generalizability of the results. Also related to the focus participants, it is a potential limitation that the additional diagnoses varied, and the effects of those diagnoses likely affected the participants in different ways. It is also a limitation that this study occurred very late in the school year and the last intervention sessions were occurring on the last days of school. The number of intervention sessions was limited for the focus participants Martin and Jason and their peers due to intervening in the final days of the school year.
Another potential weakness is the community preschool was located at a different site, which presented unique characteristics in room dimensions, proximity to extraneous sound, and teacher vocal qualities. However, this study was intended to overcome such differences by demonstrating SFA intervention was effective regardless of teacher, construction, and location differences. SFA equipment and accompanying teacher training were identical in all sites. Results demonstrated SFA was effective in each location, overcoming site differences.
For all sites, it is a potential limitation that reverberation times were not taken for the purpose of SNR calculation. Reverberation is the decay as the sound is absorbed by the surfaces of objects in the environment, whereas reverberation time is expressed as the time required for a signal’s magnitude to decrease by 60 dB. The direct effects of reverberation interference, speech recognition, and speech intelligibility assessment were not a part of this study; therefore, reverberation times were not taken. Given the classroom sizes in the present study are considered smaller than most typical classrooms, reverberation was not considered to be a significant contributor to noise in comparison with larger spaces.
The fact that SFA was not always used as recommended by the manufacturer could be another limitation. Speakers were attached to manufactured stands, an alternate recommendation, and placed on table or bookshelf tops rather than being wall mounted, which is the primary recommendation of the manufacturer to provide permanency. However, as the children were small in stature, their ears were commensurate with the speaker heights. A related concern is that teachers at two sites made changes to speaker settings and placement. Ms. Gold (second-grade teacher for Martin) moved the speaker to the front of the room where she primarily teaches, and Mrs. Jones (first-grade teacher for Jason) turned the volume down to +10 dB based on student feedback, rather than the higher recommended SNR setting of +15 dB. Participating teachers may have been more compliant had the study been conducted earlier in the school year. The stress of the end of the year was reported anecdotally by two of the five teachers.
An additional limitation of the study is that the directions teachers gave varied according to their routines and, as a result, the directions varied in length, complexity, and motivation. However, being overly prescriptive with the types of directions would have changed the natural routines of the settings. Overall, teachers balanced the types of directions they gave. One possible strategy to overcome the potential bias of direction types could be to code the latency of all directions during the observation period rather than just the first 10 directions. However, coding all directions could lead to increased variability across teachers in number of directions given, which could affect the overall results if there was great discrepancy across teachers.
Finally, the social validity measures used might be a limitation. Due to familiarity and access, the original LIFE rather than the more current, revised LIFE (Anderson et al., 2011) was used. Teachers were asked to complete the LIFE addressing only the focus participants. Social validity results might have been strengthened if the teachers had also addressed the peer participants. Similarly, teachers could have been asked open-ended questions about the effects of SFA for the peer participants. Social validity could also be enhanced by asking the teachers how likely they would be to continue to use SFA and to highlight any barriers they thought might interfere with continued use.
Implications for Practice
There are specific implications for students who are DHH and living and receiving services in rural areas. The NDC on Postsecondary Outcomes (2017), in its research brief on “Serving Deaf Individuals in Rural Communities,” indicated delivery of services in rural areas can be affected by a variety of factors (e.g., resources, geographical barriers, and lack of adequately prepared teachers and support staff). It is important that school personnel are taught to use technology appropriately to meet the needs of students who are DHH (NDC on Postsecondary Outcomes, 2017). Ensuring appropriate use of SFA in rural school settings can be one strategy to facilitate curriculum access for students who are DHH. As in the present study, itinerant teachers are often used to meet the educational needs of students who are DHH in rural settings (NDC on Postsecondary Outcomes, 2017). It is key for itinerant teachers of students who are DHH to ensure appropriate use of technology such as SFA.
The success of this research indicates SFA implementation can be a valuable learning strategy. SFA can enhance access to the general education curriculum. It potentially enhances social emotional development as a result of better attention, increased understanding, and improved opportunities to participate in surrounding activities. Therefore, SFA can promote learning and development for children with and without disabilities in general and special education settings.
Specifically, SFA was highly effective in improving attending behaviors and latency of compliance to directions for early childhood children with additional diagnoses. Jason, a student with ADHD and HL, confirms the use of SFA has beneficial effects for children with ADHD, HL, or a combination of the two. Similarly, results were dramatic for Amelia, who had an HL and Down syndrome, and revealed more consistency for the peer student with developmental delays, supporting the recommendation for SFA use in ECSE programs. Half of the focus population, and four of the eight children studied in this research, were preschool participants. Their results emphasize the value of SFA for preschool children with HL to access linguistic and educational opportunities that preschool programs afford.
Although the value of SFA was supported by this study, cost of the system for multiple classrooms might be problematic for many rural districts that frequently face insufficient funding for initiatives (Preston et al., 2013). In the present study, the SFA was approximately US$1,000 per room. Although US$1,000 might seem costly for one student, SFA actually can benefit many, if not all, students in the classroom. In addition, the cost may be offset in financial savings resulting from declines in teacher absenteeism due to decreased vocal strain and declines in special education referrals (The Institute for Enhanced Classroom Hearing, n.d.). Moreover, the use of SFA systems is far less expensive in comparison with making acoustical modifications (e.g., changing ceiling tiles, adding sound-absorbing panels, changing windows, addressing heating, ventilation, and air conditioning noise), and results in enhanced, positive listening environments for all students (The Institute for Enhanced Classroom Hearing, n.d.). Even though the benefits of SFA are supported, rural district administrators might have to be creative with their budgets to meet all district needs (Preston et al., 2013). As a result, a special initiative such as providing SFA across classrooms might require assistance from outside the district (e.g., grants, funding from the state education agency) to ensure the needs of all students are being met.
Implications for Future Research
Further investigation of the effects of SFA on academic achievement or language development through pre/postassignment comparison would warrant study for the early childhood population who are DHH and have additional diagnoses. The purpose of SFA is to provide auditory access to academic curriculum; yet, few studies (Flexer et al., 2002; Maag & Anderson, 2007; Wilson et al., 2011) have been conducted measuring the effects of SFA directly on academic achievement for this population. The current study was conducted to assess two prerequisites for learning: attending behaviors and latency of compliance to directions in classroom routines for young children who are DHH with additional diagnoses and their hearing peers. Further investigation measuring the effects of SFA on preacademic performance in this population is warranted.
Another suggested topic for future research involves SFA and computerized whiteboard technology. One question is whether teachers use the SFA aspect of the board. Investigation into training that occurs in conjunction with this technology is warranted; are teachers consistently trained on the SFA aspect of this technology? Another question is whether personnel are available to set and maintain the systems. Teachers with SFA or computerized whiteboard technology with built-in SFA often report they are not using SFA. Research is needed to determine specifically what teachers’ reactions are to hearing their voices and reasons why teachers do not use SFA after installation or stop use after a trial period.
Conclusion
All student participants demonstrated improvement in attending behaviors and compliance to directions with SFA. Focus children who are DHH with additional diagnoses produced stronger results than their peers to the activation of SFA. Teachers indicated SFA was beneficial to the children who are DHH and they would use it again. One teacher, Mrs. Sweet, identified a critical aspect of the benefits of using SFA in the classroom, “The speaker was so good for Susie and her needs, but the microphone was good for all the children, and I think she felt good that she wasn’t singled out. It was for everybody!” The benefits of SFA for early childhood children who are DHH and their peers clearly enhance and improve opportunities to participate in class routines.
This study makes a contribution in documenting appropriate delivery of services by rural district itinerant TODHH students through work with classroom teachers. These teachers used the SFA system appropriately to improve the behaviors of the focus participants. Given the dearth of previous studies on the effects of SFA, especially for young children who are DHH with other diagnoses, this study contributes to the literature. Children who are DHH in the foundational early childhood ages were highly successful in improving attending behaviors and complying more quickly to directions with SFA. SFA is an important strategy to expand access to educational opportunities by increasing attending behaviors and promoting participation for children who are DHH with additional diagnoses in preschool, first-grade, and second-grade settings. It is particularly important that these improvements resulted through training on use of an SFA system delivered by a rural itinerant TODHH to the participants’ classroom teachers.
Supplemental Material
Teachers_Daily_FM_Checklist – Supplemental material for Young Children With Hearing Impairment and Other Diagnoses: Effects of Sound-Field Amplification
Supplemental material, Teachers_Daily_FM_Checklist for Young Children With Hearing Impairment and Other Diagnoses: Effects of Sound-Field Amplification by Lois Furno, MaryAnn Demchak and Ann Bingham in Rural Special Education Quarterly
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.