
Abstract
Background
Imaging coronary venous systems to guide transcatheter cardiac interventions are becoming increasingly important, particularly in heart failure patients who are selected for cardiac resynchronization therapy (CRT). Failure of left ventricular (LV) lead placement during the procedure has been attributed to the inability to insert catheters into the coronary sinus and the lack of suitable side branches.
Purpose
To comparatively assess the value of a 64-detector MDCT examination in visualizing the cardiac veins and evaluating the morphological characteristics of the coronary venous system in patients with and without chronic systolic heart failure (SHF).
Material and Methods
A 64-detector MDCT examination of the heart was performed in 26 consecutive patients (five women, 21 men; mean age 57.80 ± 12.05 years; range 27–81 years) with chronic SHF. The morphological characteristics of the coronary venous system, such as the diameter, the distances between the venous tributaries, the angle and the tortuosity, were evaluated. The group was compared with a subgroup of 52 subjects without SHF (LV ejection fraction >40%) matched for age, sex, and the risk factors for coronary artery disease.
Results
The coronary sinus (CS), great cardiac vein (GCV), anterior interventricular vein (AIV), and posterior interventricular vein (PIV) were visualized in all 78 individuals. The posterior vein of the left ventricle (PVLV) (63/78), left marginal vein (LMV) (72/78), and the small cardiac vein (SCV) (50/78) were visualized in SHF and control patients (p = NS). The lengths between venous tributaries were higher (p > 0.05) and more dilated (P < 0.001 for CS, GCV, AIV, PVLV, LMV; p = 0.001 for PIV) in the cases with SHF compared with the control population. The angle between the CS-GCV axis and the venous branches was wider (p = 0.02 for LMV and PIV, p = 0.001 for PVLV) and did not have any correlation with the LV diameter in cases with SHF. There was no difference between the SHF and control groups in terms of the tortuosity of PVLV and LMV (p = NS).
Conclusion
The study demonstrated an increase in the diameters, lengths, and angulations with the CS-GCV axis of the coronary veins in cases with SHF. A 64-detector MDCT is a feasible tool for non-invasive evaluation of the coronary venous system and may provide considerable information regarding numbers and morphology of coronary veins before percutaneous transcatheter cardiac therapy.
Keywords
The number of percutaneous transcatheter cardiac interventional procedures related to the coronary venous system in cardiac arrhythmia and insufficiency has been growing rapidly for the last two decades (1–4). These therapeutic interventional procedures include cardiac resynchronization therapy (CRT), left ventricular (LV) lead pacing, percutaneous mitral annuloplasty, and transvenous myocardial cell transplantation (5–9). The morphological features of coronary venous structures, such as diameter, length and course, may vary (1, 10). Due to variations such as hypoplasia of the sinus and narrowing or atresia of the ostium and diverticulum, LV lead placement and effective biventricular pacing may result in failure in 10–15% of the cases (5–7, 11–13). Therefore, depicting the coronary venous anatomy in advance provides the electrophysiologist with a road map.
The coronary venous system can be evaluated with invasive cardiac venography, echocardiography, magnetic resonance imaging, electron-beam computed tomography, and recently, multidetector computed tomography (MDCT). Coronary venous system imaging with computed tomography was initially described in 1985; the coronary sinus was demonstrated as non-ECG-gated by a single slice scanner in this pioneering study (14). Coronary angiography with MDCT is a rapidly progressing branch in medical imaging. Advances in detector technology in the past decade have greatly improved the feasibility of imaging the coronary venous system. Various features of these veins have been studied in the literature in different patient groups. However, a literature survey on coronary venous anatomy shows only a few studies performed with a 64-detector MDCT (15, 16). Although there are a few studies performed with a 16-detector MDCT (13, 17) where the probable morphological variances in the cardiac venous system have been assessed, none have been performed with a 64-MDCT in this area, particularly in patients with chronic systolic heart failure (SHF). The aim of this study was to assess the value of a 64-detector MDCT in visualizing the cardiac veins and to evaluate the morphological characteristics of the coronary venous system in patients with and without chronic systolic heart failure.
Material and Methods
Patient population
Between November 2008 and February 2010, 26 consecutive patients (five women, 21 men; mean age 57.80 ± 12.05 [SD] years; range 27–81 years) with chronic SHF and low LVEF (≤40%) were enrolled for coronary MDCT angiography. All these patients were medically controlled by combination therapy with digitalis, diuretics, aldosterone-blocking agents, an angiotensin-converting enzyme inhibitor or angiotensin receptor antagonist, or β-blockers and were functional Class II or III according to the New York Heart Association. Patients with chronic SHF were compared with another subgroup of 52 patients without SHF (control group, LVEF >40%) selected from our cardiac MDCT data bank. The groups were matched in terms of age, sex, and risk factors for coronary artery disease (CAD) (Table 1). Exclusion criteria for MDCT were absolute arrhythmia (e.g. atrial fibrillation), renal dysfunction (serum creatinine >1.2 mmol/L), a history of allergic reaction to iodine-containing contrast media, and pregnancy. The study was approved by the ethics committee in the institution.
Demographic and clinical data of subject with SHF and control patients
Values are number with percentage in parentheses
SHF = systolic heart failure, CAD = coronary artery disease, NS = not significant
MDCT examination technique
Data were acquired using a 64-detector row spiral CT scanner (Aquilion 64-Slice CT System, Toshiba Medical Systems, Tokyo, Japan). The scan parameters were a detector collimation of 64 × 0.5 mm, a pitch of 0.2–0.45 (depending on heart rate), a rotation time of 400 ms, a tube voltage of 120 kV, and a current of 600–900 effective mAs. ECG-dependent tube current modulation was applied in regular heart rates. The scan direction was craniocaudal during a single midinspiratory breath-hold. The scanning range covered the entire heart from the level of the tracheal bifurcation to the diaphragm. A bolus of 80 mL of the iodine contrast agent iobitridol (Xenetix 350, 350 mg/mL; Guerbet, Villepinte, France) was injected intravenously via an antecubital vein at a flow rate of 5–6 mL/s using a dual-head power injector, followed by a 50-mL saline chaser (5 mL/s). The scan was started automatically by applying the ‘sure start’ technique (ascending aorta, threshold 160 HU). A beta-blocker (5–15 mL metoprolol) was given intravenously before the MDCT scan if the heart rate was greater than 70 bpm.
MDCT image reconstruction and analyses
The retrospective reconstructions were performed in all cardiac phases with 50-m/sec intervals (from 20% to 80% of the R-R interval). Images were reconstructed with a section thickness of 0.5 mm, a reconstruction increment of 0.3 mm, a 512 × 512 image matrix, and a FOV of 180–240 mm. Data were transmitted to Workstation Vitrea 2 software (Vital Images Inc., Plymouth, MN, USA), and images were reconstructed with multiple postprocessing methods. Coronary venous anatomy (the coronary sinus [CS], great cardiac vein [GCV], posterior interventricular vein [PIV], anterior interventricular vein [AIV], posterior vein of the left ventricle [PVLV], left marginal vein [LMV], and the small cardiac vein [SCV]) was usually analyzed in images from the 70–80% R-R interval because the imaging quality is better in mid-diastole than in the systolic phase. To evaluate the coronary segments, transverse source images, multiplanar reformations, curved multiplanar reformations, maximum intensity projections, and volume-rendered images were used (Fig. 1a and b).
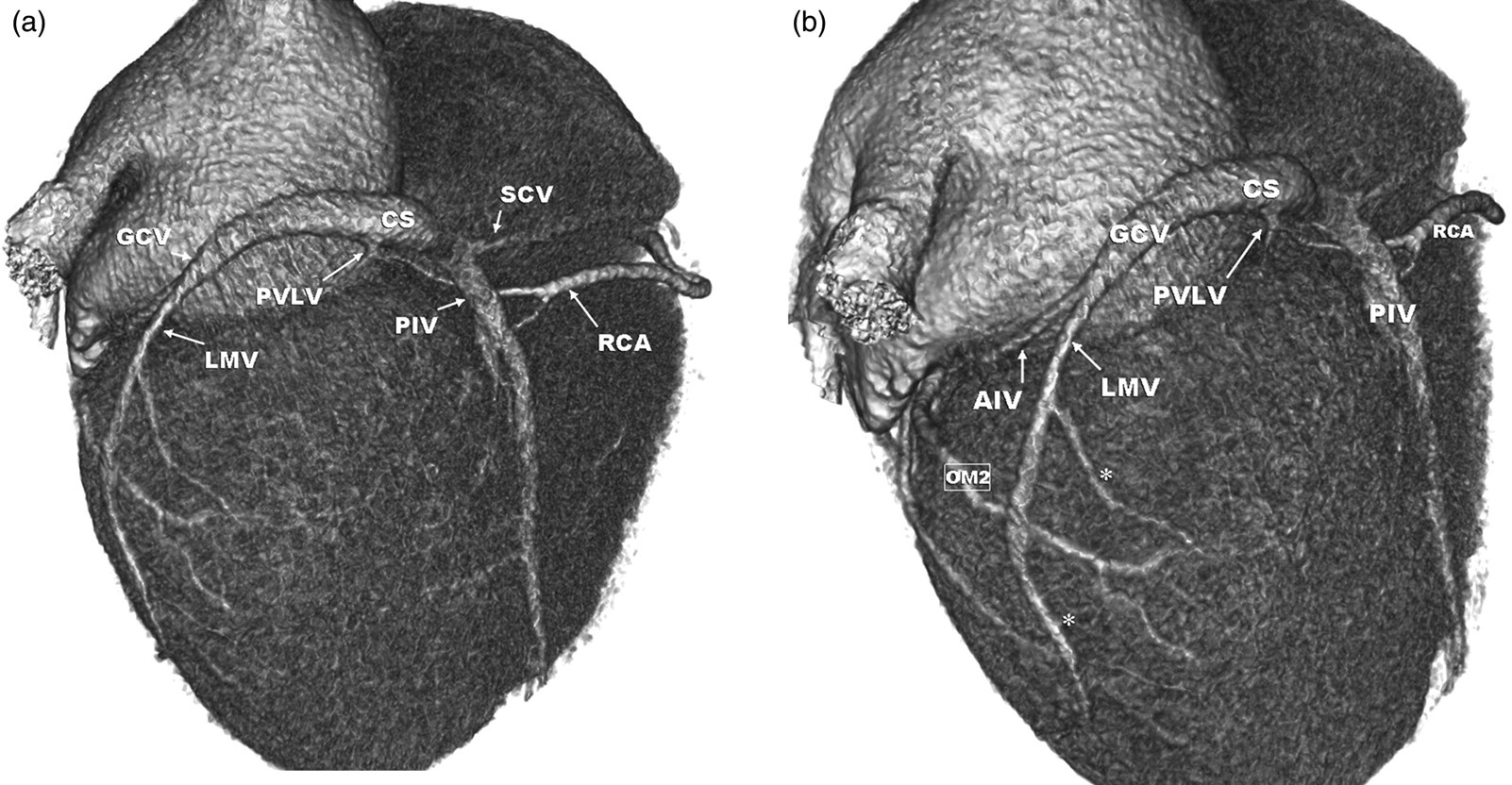
Volume-rendered reconstruction of the heart: (a) posterolateral view and (b) lateral view. The coronary sinus (CS), great cardiac vein (GCV), posterior interventricular vein (PIV), anterior interventricular vein (AIV), posterior vein of the left ventricle (PVLV), left marginal vein (LMV) with several distal branches (asterisks), and small cardiac vein are shown. Also note the right coronary artery (RCA) and obtuse marginal-2 (OM2)
The visibility of the coronary veins was evaluated semi-qualitatively using a four-point grading system for each coronary vein (grade 0, not visible; grade 1, visible with discontinuity; grade 2, visible with irregular borders; grade 3, visible as smoothly bordered vascular structure). The result of the evaluation for the presence of anatomic valves in accessing the coronary sinus was recorded. Multiplanar reformations were used to determine the diameter of the veins. The diameters of the ostia of the CSs at the superior-inferior and anterior-posterior directions were measured. The diameter of the veins was measured at the venous ostial level perpendicular to the main axis of the vein. The distances between the venous tributaries were measured on the curved multiplanar reformattings using electronic calipers (Fig. 2). The angulations of the venous tributaries (PIV, PVLV, and LMV) against the CS-GCV axis were measured using multiplanar reformations. The tortuosity in the PVLV and the LMV was assessed in the volume-rendered images. The number of turns in the trace of the vascular structure was recorded for tortuosity. The LMV and the PVLV were classified as being tortuous if the observers could visualize at least two turns.
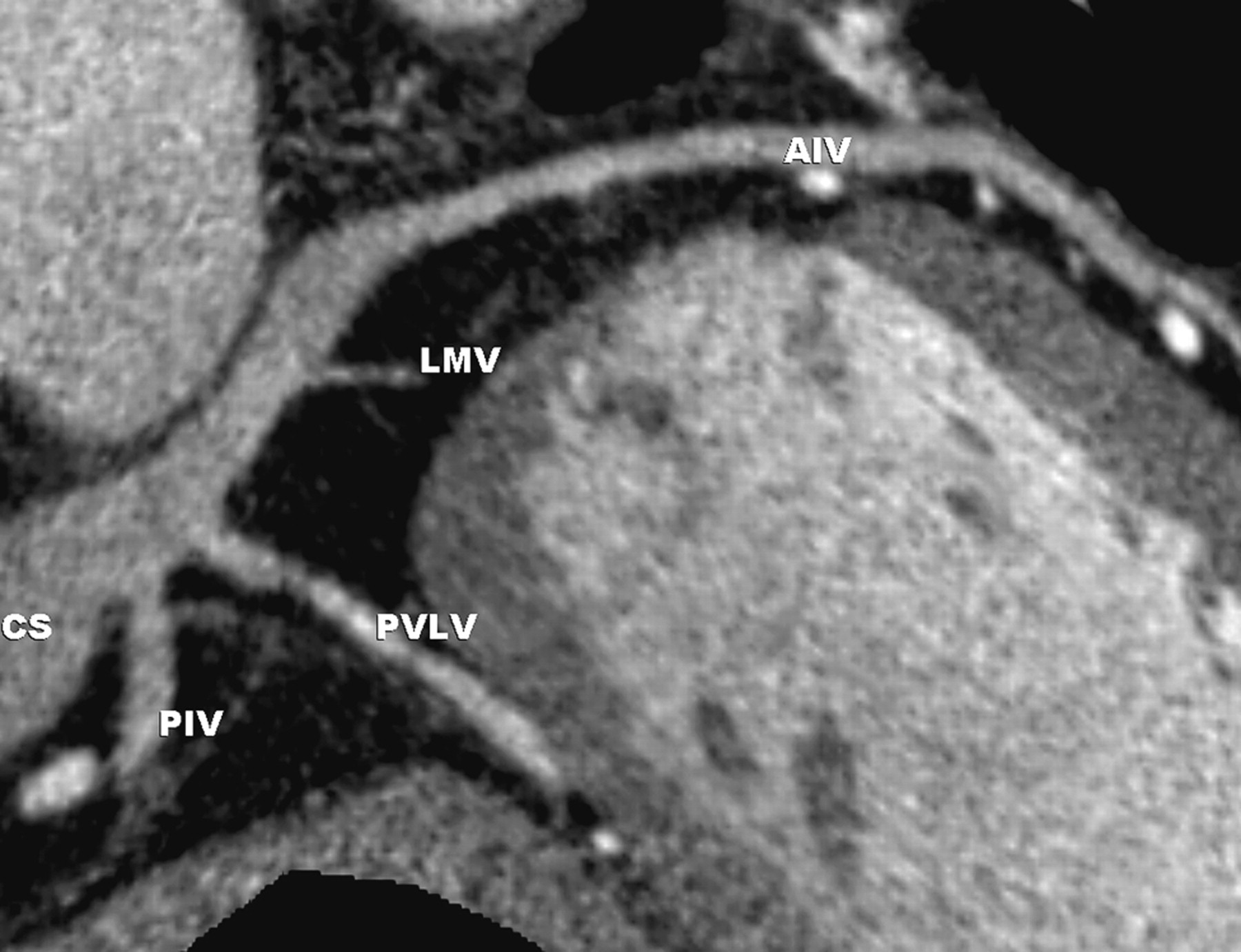
Measurements of the distances between the venous tributaries on the curved multiplanar re-formatting using electronic calipers. The coronary sinus (CS), posterior interventricular vein (PIV), anterior interventricular vein (AIV), posterior vein of the left ventricle (PVLV), and left marginal vein (LMV) are shown
Two radiologists (RC and NT) experienced in cardiovascular radiology interpreted the MDCT images. For visual analysis, the results of the consensus reading of both reviewers were reported. Two experienced cardiologists (SY and AA) blinded to the results of the cardiac MDCT acquired apical views of the left ventricle using a Vivid 7 (GE Healthcare, Waukesha, WI, USA) echo equipped with a 1.5–3.5 MHz transducer. Volumes were obtained from apical four- and two-chamber views, and the ejection fraction was calculated using the biplane Simpson method with dedicated software (Echopac v6.0, GE Healthcare – Vingmed Ultrasound, Horten, Norway).
Statistical analyses
SPSS 11.5 statistical software (SPSS Inc, Chicago, IL, USA) was used for the statistical analysis of the data acquired in this study. Data were expressed as either mean (±SD) or frequencies. Correlations between different parameters were assessed using Pearson correlation analysis. The continuous variables in the patients with or without heart failure were compared by Student's t-test, and chi-squared test was used for comparison of categorical variables. P values less than 0.05 were considered as statistically significant.
Results
MDCT coronary angiography was successfully completed without any complications in all the patients. No patients reported any discomfort due to the MDCT examination or the use of contrast material. The CS, GCV, AIV, and PIV were assessed in all patients (78/78). The PVLV (63/78), LMV (72/78), and SCV (50/78) were assessed in SHF and control patients (p = NS). The LMV was present as a single vessel in 16 patients (21%), double in 43 patients (55%), and triple in 19 patients (24%). The difference in LMV counts between the two groups was not significant (p = 0.6). The Marshall vein and the Thebesian valve were identified in nine (five SHF patients and four normal controls) and 23 (13 SHF patients and 10 normal controls) cases, respectively. There was no significant difference between the visualization of the veins in either group (p = 0.18). The traces of the veins could be evaluated without any interruption except for the SCV. Because of the small size of the SCV and minimal motion detected on the right heart contour, the SCV was visualized as grade 2 in 11 subjects. The diameter of the branches and angulations of the venous tributaries against the CS-GCV axis and the distances between the main venous tributaries are summarized in detail in Table 2. For the quantitative measurements, inter- and intra-observer agreements were assessed in all patients, and the percentages of agreements were 93% and 96%, respectively.
Quantitative measurements in venous anatomy from MDCT
SHF = systolic heart failure, CS = coronary sinus, GCV = great cardiac vein, AIV = anterior interventricular vein, PIV = posterior interventricular vein, PVLV = posterior vein of left ventricul, LMV = left marginal vein
The diameters of all coronary veins were statistically significantly different between the heart failure and the control groups (Table 2). There was also a statistically significant difference between the two groups in the distances between the main venous tributaries. There was a statistically significant difference between the two groups in the branching angles. The branching angles of coronary venous tributaries relative to the CS-GCV axis were generally obtuse (>90°), particularly for the PVLV and the LMV, and the angles were almost unanimously wider in the heart failure group. The turn counts in PVLV and LMV ranged between 1 and 4, and there was no statistically significant difference between the groups regarding the tortuosity in the PVLV and the LMV (p = NS).
The anterior-posterior and the superior-inferior diameters of the coronary sinus ostium were positively correlated with LV diameter (r: 0.384, p = 0.001 and r: 0.443, p < 0.001, respectively). There was also a positive correlation between the LV diameter and the diameter of the GCV (r: 0.365, p = 0.001), the AIV (r: 0.299, p = 0.008), the PIV (r: 0.263, p = 0.02), and the PVLV (r: 0.403 p < 0.001). The distances between the main venous tributaries were also positively correlated with the LV diameter (PIV-AIV distance r: 0.412, p < 0.001; PIV-PVLV distance r: 0.331, p = 0.003; PIV-LVM distance r: 0.370, p = 0.001; LMV-AIV distance r: 0.330, p = 0.003). There was no correlation between the branching angles of the coronary venous tributaries and the diameter of the LV (PIV angle r = 0,115, p = 0.3; PVLV angle r = 0,217, p = 0.056; LMV angle r = 0,142, p = 0.2).
Discussion
There were four main findings in this study: (a) 64-detector MDCT is a feasible non-invasive modality for assessing the coronary venous anatomy; (b) the venous anatomy was longer and more dilated in the cases with SHF compared to that of the control population; (c) the angle between the CS-GCV axis and the venous branches was wider and did not have any correlation with the LV diameter in cases with SHF; and (d) there was no difference between the SHF and the control groups in the tortuosity of PVLV and LMV. The present report is the first in the literature to report the last two findings. These findings play a significant role in the pre-procedure evaluation of cases with SHF and for candidates for CRT.
Echocardiography does not contain any X-ray acquisition to image the coronary venous system. However, echocardiography is operator-dependent, and it is not possible to visualize the distal venous branches with this method (11, 18, 19). Although it is possible to image the structures of the coronary venous system with relatively larger diameters such as CS and GCV in high contrast and spatial resolution clearly by contrast-enhanced electron-beam CT, visualization of the distal venous tributaries is poor with this technique, as it is for echocardiography (20). Besides, there are no reports in the literature showing that electron-beam CT can reveal small cardiac veins or the Thebesian valves (1). During invasive cardiac venography, the operator reaches the CS via a catheter and injects contrast media into the venous system, either directly or after balloon occlusion (21). In many cases, even the distal branches can be easily visualized with this technique. However, the disadvantages of this invasive method include balloon-related trauma risk of the coronary sinus and the use of high-dose iodine contrast material. Additionally, invasive cardiac venography gives information only about the lumen and, in contrast to echocardiography and CT, lacks imaging of entire anatomic structures such as the ventricular wall and the LV diameter.
The opacification of the cardiac venous system and even its distal branches was acceptable in this study with a 64-detector, as in a previous report with a similar equipment (15). PVLV and LMVs, which are frequently used in percutaneous transcatheter cardiac therapeutic procedures, are located on the posterolateral wall of the heart. Demonstration of their existence and their numbers, as well as revealing their morphological features such as the diameter, the distances between the venous tributaries, the angle and the tortuosity provides very useful information prior to the intervention (22). Studies with imaging techniques over the last 10 years have shown that the prevalence of PVLV and LMV is between 13% and 100%, and 38% and 96%, respectively (1, 13, 15, 20–23). Our results were close to the upper limits of these studies. In one recent study in which 16-detector MDCT was used, Christiaens et al. reported that 64% of the patients have a single LMV, whereas 32% have two, and only 2% of the patients had triple LMVs (24). In this context, our results were quite different from theirs because many more LMVs were identified with the 64-detector CT. This difference may easily be attributed to the higher resolution.
Stimulating the lateral wall of the left ventricle during CRT may be difficult because of the absence or low caliber of LMV and PVLV, which causes the high failure rate of this procedure. The increase in the diameters of the veins, including CS, in cases with SHF should allow an easier catheterization of both the CS and the other venous structures during CRT. Similar results were obtained in the former MDCT study performed in patients with SHF, and Chen et al. (13) reported that the coronary venous diameters and total coronary venous length were larger in patients with SHF. In another study done with a 16-detector MDCT, the LMV in particular is reported as more dilated in cases with SHF (17).
According to our results, the diameters and the lengths of the coronary veins increased with the diameters of the LVs. In a recent MDCT study, it was reported that there is a positive relationship between the LV diameter and the distance between PIV-AIV, but not with the other venous distance intervals (24). Christiaens et al. performed this study in cases with normal EFs and reported that there was a relationship between the LV/mitral annulus diameter and the superior-inferior diameter of the CS. The LV is usually enlarged, particularly in cases with SHF, and this can lead to changes in the orientations of the coronary veins. The relationship between the LV wall and the coronary veins (the diameter, course, and tortuosity) can be depicted simultaneously (unlike with invasive cardiac venography) with MDCT in three dimensions prior to CRT. This knowledge may be helpful in reducing the failure rates in the procedure.
A change is observed in the axis of the heart due to the enlargement of the heart chambers in SHF. The inevitable result of these changes in the axis and shape of the heart is a change in the orientations of the coronary veins (13, 24, 25). To the best of our knowledge, this is the first time that a significant increase was observed in the angle between the CS-GCV axis and PIV, PVLV, and LMV using a 64-detector MDCT in cases with SHF. These angles were usually obtuse (>90°). However, the increase of the angles was not related to the LV diameter. The reason for the absence of any relationship between the increase in the angles and left ventricular diameter is likely because an increase in the left ventricular diameter does not necessarily accompany SHF.
In our study, the tortuosity of the PVLV and LMV in patients with SHF has been investigated for the first time in the literature. We found no significant differences between the groups regarding the tortuosity for each vein. This finding indicates that, although the change in the cardiac morphology in SHF leads to increases in the venous length and calibers, it does not lead to a difficulty in LV lead placement caused by tortuosity in LMV and PVLV.
The limitations of this work are similar to those of other venous cardiac MDCT studies. The first is the relatively low opacification of the coronary veins because of the timing of the acquisition that is needed to visualize coronary arteries. The exclusion of patients with atrial fibrillation that is determined to be a contraindication is another limitation. New-generation dual-source MDCTs may overcome this problem.
In conclusion, 64-detector MDCT is a feasible tool for non-invasive evaluation of the coronary venous system before percutaneous transcatheter cardiac interventions. There is an increase in the calibers, lengths, and angels with the CS-GCV axis of the coronary veins in cases with SHF. This information related to the changes in the venous morphology due to changing cardiac anatomy in cases with SHF prior to CRT is important for finding the suitable vessel and the success of the procedure.