
Abstract
Background
Although triple rule-out CT angiography (TRO) to simultaneously evaluate acute coronary syndrome (ACS), pulmonary embolism (PE), and acute aortic syndrome (AAS) is increasingly used in many institutions, TRO is inevitably associated with increased radiation exposure due to extended z-axis coverage compared with dedicated coronary CT angiography (DCTA).
Purpose
To determine the frequency of exclusion of findings of AAS, PE, and significant incidental non-cardiac pathology that may be the cause of acute chest pain when using a restricted DCTA field of view (FOV).
Material and Methods
We retrospectively reviewed CT images and charts of 103 patients with acute PE and 50 patients with AAS. Either non-ECG gated dedicated pulmonary or aortic CT angiography was performed using 16- or 64-slice multidetector CT (MDCT). We analyzed the incidence of isolated PE, AAS, or significant non-cardiac pathology outside of DCTA FOV (i.e. from tracheal carina to the base of heart).
Results
There were two cases of isolated PE (2/103, 1.9%) excluded from the FOV of DCTA. One case of PE was isolated to the subsegmental pulmonary artery in the posterior segment of the right upper lobe. In the second case, pulmonary embolism in the left main pulmonary artery was located out of the FOV of DCTA because the left main pulmonary artery was retracted upwardly by fibrotic scar in the left upper lobe due to prior tuberculosis. There was no case of AAS and significant non-cardiac pathology excluded from the FOV of DCTA. AAS (n = 50) consisted of penetrating atherosclerotic ulcer (n = 7), intramural hematoma (n = 5) and aortic dissection (n = 38).
Conclusion
As isolated PE, AAS, and significant non-cardiac pathology outside of the DCTA FOV rarely occur, DCTA may replace TRO in the evaluation of patients with non-specific acute chest pain and a low pre-test probability of PE or aortic dissection.
Triple rule-out CT angiography (TRO) to simultaneously evaluate acute coronary syndrome (ACS), pulmonary embolism (PE), and acute aortic syndrome (AAS) is increasingly being performed in many institutions equipped with 64-slice or greater multidetector CT (MDCT). The scan range for TRO and dedicated coronary CT angiography (DCTA) extends from the thoracic inlet to costophrenic angles and from the tracheal carina to the base of heart, respectively (1). Therefore, TRO is inevitably associated with increased radiation exposure due to extended z-axis coverage compared with DCTA, resulting in increased risk of radiation induced cancer. Multiple recent studies have indicated that TRO is valuable to evaluate patients with nonspecific acute chest pain in whom diagnosis of PE or AAS as well as ACS are simultaneously considered (1–7). One review article has suggested that most of PE and aortic dissection are identifiable on DCTA (8). However, this assumption has not been assessed in a systematic way. We hypothesized that isolated AAS or PE that is not in the field of view (FOV) of DCTA is uncommon.
Thus, the purpose of this study was to determine the frequency of exclusion of findings of AAS, PE, and significant non-cardiac pathology that may be the cause of acute chest pain when using a restricted DCTA FOV.
Material and Methods
Study population
Institutional review board approval was obtained and informed consent was waived for this study. This study was performed by retrospectively reviewing clinical and radiological data in a large university hospital. We identified 107 consecutive patients with acute PE between September 2006 and September 2009. A diagnosis of acute PE was made if there was an intra-luminal filling defect within the pulmonary arteries on contrast-enhanced CT in the absence of findings of chronic PE (i.e. an intra-luminal filling defect adherent to the wall of pulmonary arteries or abrupt narrowing or web in the pulmonary arteries). Four patients with acute PE were not included in this study because respiratory motion artifacts (n = 3) or poor contrast enhancement (n = 1) could not be excluded as a cause of the apparent filling defect in these cases. Thus, 103 patients with acute PE (men/women 57/46; mean age 57.7 ± 16.4) were included in this study. We also identified 50 consecutive patients (men/women 28/22; mean age 62.1 ± 15.2) with the diagnosis of AAS between September 2004 and September 2009. Acute aortic syndrome cases consisted of intramural hematoma (n = 5), penetrating atherosclerotic ulcer (n = 7), and aortic dissection (n = 38). A diagnosis of aortic dissection was made if there was an intimal flap traversing the lumen of aorta. A diagnosis of intramural hematoma was made if there was a crescent-shaped high attenuation in the aortic wall on pre-enhanced CT image without evidence of aortic dissection or penetrating atherosclerotic ulcer after enhancement. Penetrating atherosclerotic ulcer was considered to be present if there was an ulcer penetrating through the aortic wall accompanied by adjacent intramural hematoma. An aortic ulcer like outpouching in the absence of adjacent intramural hematoma (i.e. saccular pseudo-aneurysm) is often asymptomatic and can be an incidental finding, and such cases were not included in this study (9, 10). Only one case of saccular pseudo-aneurysm occurred during the study period.
CT technique
Dedicated pulmonary CT angiography and aortic CT angiography were performed on 16-slice multidetector CT (MDCT) (Somatom Sensation 16, Siemens Medical Solutions, Forchheim, Germany) or 64-slice MDCT (Light-speed VCT, GE Healthcare, Milwaukee, WI, USA). Scanning parameters of dedicated PE and aortic CT angiography were as follows: non-ECG gating, 120 kV, 200-400 mA, 0.625 mm collimation, 1.5 mm increment, 3 mm reconstruction, 32 cm field of view, and 0.35 or 0.40 s gantry rotation time. Contrast enhancement was performed with the intravenous injection of 60–100 mL of Ioversol (Optiray 350 mg/ml, Tyco healthcare, Montreal, Canada) based on the patient's body mass index. The scan range for dedicated PE and aortic CT angiography extended from the thoracic inlet to adrenal glands and from the thoracic inlet to femoral heads, respectively. A trigger delay of 5 s and bolus tracking of contrast material were used. Scanning was started when the contrast bolus arrived in the main pulmonary artery or ascending aorta (threshold >100 Hounsfield units [HU]) according to the targeting artery. Multiplanar re-formatted images such as volume rendering, maximal intensity projection or curved multiplanar re-formatted images as well as transaxial CT images were available in this study.
Image analysis
Two experienced radiologists (10 years of experience in cardiovascular imaging and 11 years of experience in body CT imaging) who were blinded to clinical information independently analyzed dedicated PE and aortic CT angiography images, retrospectively. If there was disagreement between the two readers about MDCT findings, a third reader's (10 years of experience in cardiovascular imaging) opinion was sought for final decision. Dedicated PE or aortic CT angiography images from the tracheal carina to the base of heart were used to simulate the FOV of DCTA. The imaginary upper and lower end of FOV of DCTA was identified by using a cross-reference tool on the PACS monitor. The cross-reference tool on a particular trans-axial CT image allowed us to obtain the corresponding horizontal line on the scanogram of the chest AP view. The upper end of the FOV of DCTA (Fig. 1) was defined as a horizontal line tangential to apex of tracheal carinal angle on the scanogram of the chest AP view. The lower end of the FOV of DCTA was defined as a horizontal line tangential to the cardiac base on the scanogram of the chest AP view. We analyzed the incidence of isolated PE and AAS excluded from the DCTA FOV. We recorded the largest pulmonary artery in which a pulmonary embolus was identified. The location of pulmonary embolus was classified as involving the main, lobar, segmental, or subsegmental pulmonary artery. We also analyzed the nature of the presenting symptoms and the presence of right ventricular enlargement and straightening of inter-ventricular septum in patients with PE. Right ventricular enlargement was considered to be present if the diameter of the right ventricle on transaxial CT image at the level of tricuspid valve was at least 1.5 times larger than that of the left ventricle on transaxial CT image at the level of mitral valve. Straightening of the inter-ventricular septum was considered to be present if there was a loss of normal bowing of inter-ventricular septum toward the right ventricle or abnormal bowing of inter-ventricular septum toward the left ventricle. In patients with AAS, the Stanford classification type of AAS was recorded. We also analyzed the presence or absence of carotid or subclavian artery involvement by a dissection flap that may be missed if DCTA rather than TRO is performed. We also analyzed the incidence of significant incidental non-cardiac pathology that may be the cause of acute chest pain. Significant incidental non-cardiac pathology comprised pneumonia, pericarditis, acute cholecystitis, acute pancreatitis, colonic diverticulitis, hiatal hernia, acute rib fracture, pneumothorax, and pneumomediastinum. Significant incidental non-cardiac pathology was considered to be present if a patient had consistent radiological and/or clinical findings on chart review. We also evaluated the incidence of significant incidental non-cardiac pathology excluded from the FOV of DCTA.
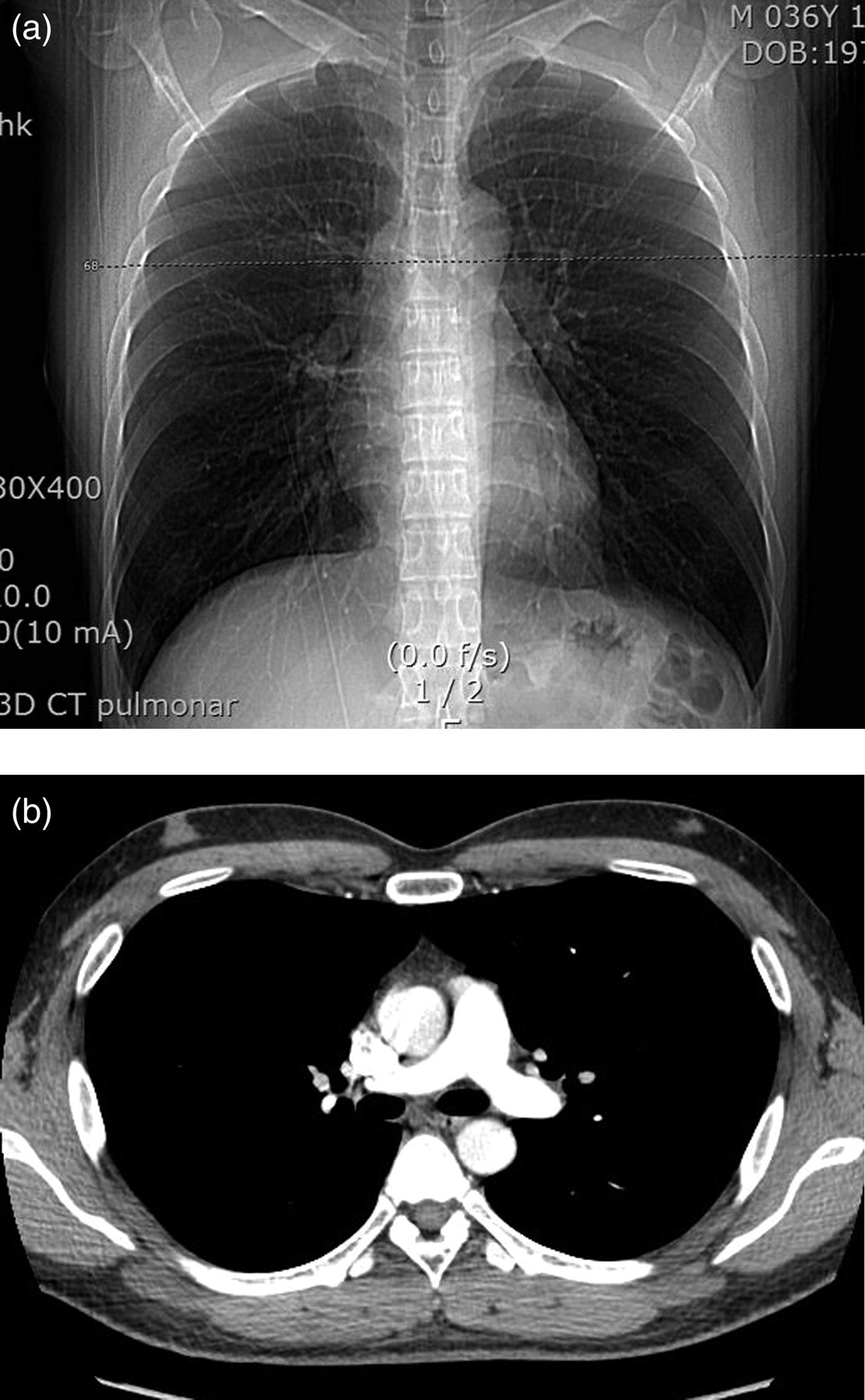
The imaginary upper end (a) of the field of view of dedicated coronary CT angiography is marked by a dotted line on the CT scanogram. Note transaxial CT image (b) corresponding to the dotted line in (a)
Statistical methods
Statistical analysis was performed using commercially available software (SAS version 4.1, SAS Institutue Inc., Cary, NC, USA). All data were expressed as mean ± standard deviation (SD) for continuous variables and percentages or frequencies for categorical variables. Interobserver agreement (kappa statistics) of each CT finding (i.e. isolated PE or AAS outside of the DCTA FOV, largest pulmonary embolus, right ventricular enlargement, straightening of inter-ventricular septum, and carotid or subclavian artery involvement by dissection flap) was calculated.
Results
Pulmonary embolism
Presenting symptoms of acute PE in 103 patients included chest pain (n = 42), dyspnea (n = 56), syncope (n = 4), and deep vein thrombosis (n = 15). The largest pulmonary embolus was demonstrated in main (n = 50), lobar (n = 24), segmental (n = 23) and subsegmental pulmonary artery (n = 6), respectively. There were two cases of isolated PE (2/103, 1.9%) that occurred outside of the FOV of DCTA. One case of PE presenting with deep vein thrombosis was isolated to the subsegmental pulmonary artery in the posterior segment of the right upper lobe (Fig. 2). In the second case, pulmonary embolism in the left main pulmonary artery in a patient presenting with dyspnea was located out of the FOV of DCTA because the left main pulmonary artery was retracted upwardly by fibrotic scar in the left upper lobe due to prior tuberculosis (Fig. 3). There was no case (0/42 patients) of pulmonary embolus occurring outside of the DCTA FOV among patients who presented with chest pain. The classification of the largest pulmonary embolus and isolated PE outside of the DCTA FOV was identical between two readers in all patients (100%; excellent interobserver agreement, kappa = 1.0). There were 19 and 17 patients with the right ventricular enlargement and straightening of inter-ventricular septum, respectively. There were two cases with disagreement in the interpretation of the presence of the right ventricular enlargement and straightening of inter-ventricular septum between the two readers (98.1%; excellent interobserver agreement, kappa = 0.927). The two cases with isolated pulmonary embolus outside of DCTA FOV did not demonstrate right ventricular enlargement or straightening of inter-ventricular septum.

Isolated subsegmental pulmonary embolism in the posterior segment of the right upper lobe in a 70-year-old woman. An intra-luminal filling defect of low attenuation (arrow) is noted in the subsegmental pulmonary artery in the posterior segment of the right upper lobe on contrast-enhanced transaxial CT image at the level of distal trachea. There was no evidence of pulmonary embolus in the remainder of pulmonary arteries
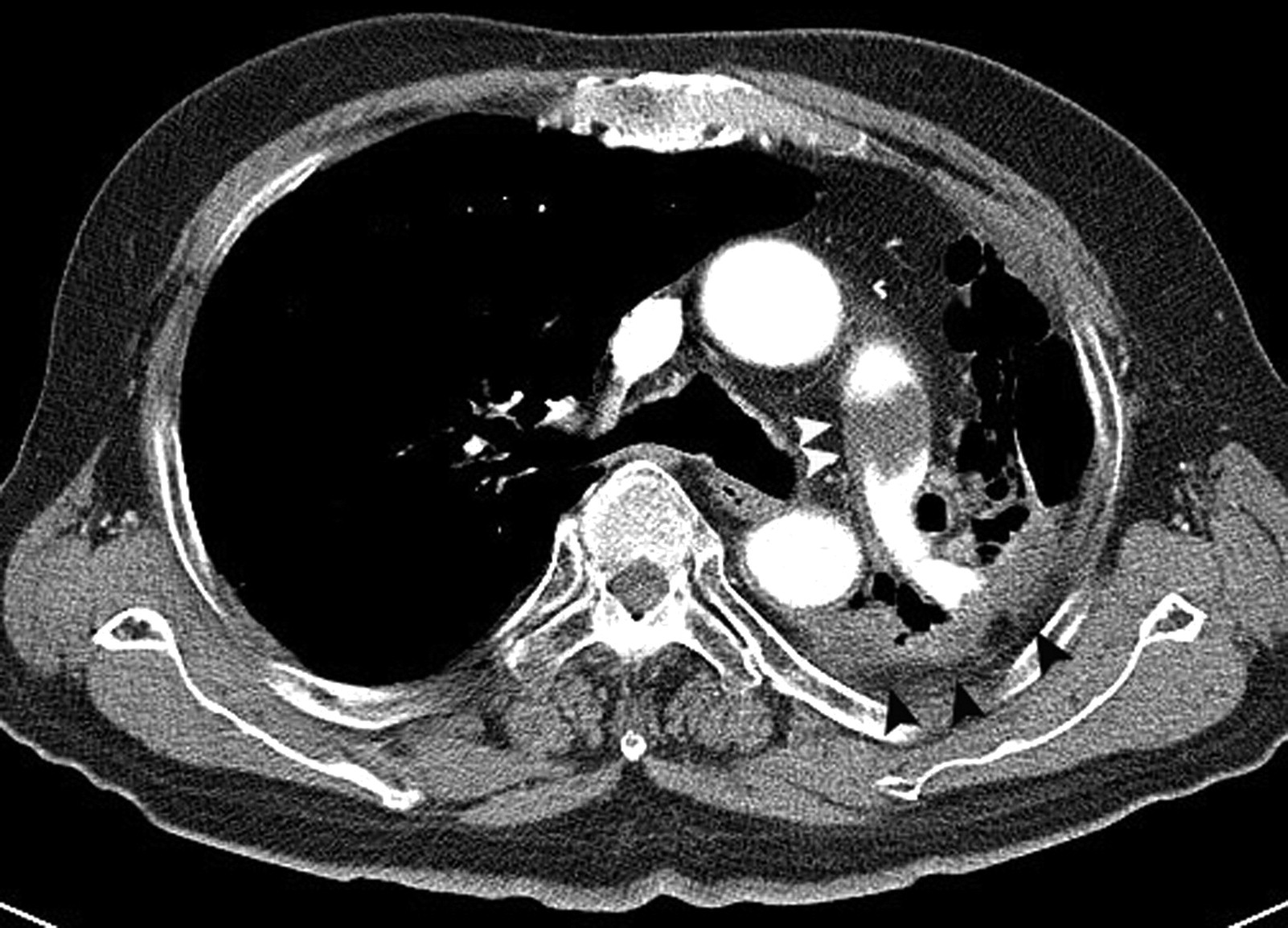
Pulmonary embolism excluded from the field of view of dedicated coronary CT angiography in a 72-year-old man. Pulmonary embolus (white arrowheads) is seen in the left main pulmonary artery on a contrast-enhanced transaxial CT image at the level of the left main pulmonary artery. Fibrotic consolidation (black arrowheads) due to previous tuberculosis is also noted in the left upper lobe
Acute aortic syndrome
Stanford type A and B aortic dissection was found in 20 and 30 patients, respectively. All of these patients presented with acute chest pain. There was no case of AAS (0/50) which was only visible outside of the DCTA FOV (Figs. 4 and 5). The extension of a dissection flap into the carotid or subclavian artery was identified in five patients with Stanford type A aortic dissection. Interpretation of isolated AAS outside of the DCTA FOV and the extension of dissection flap into the carotid or subclavian artery was identical between the two readers in all patients (100%; excellent interobserver agreement, kappa = 1.0).
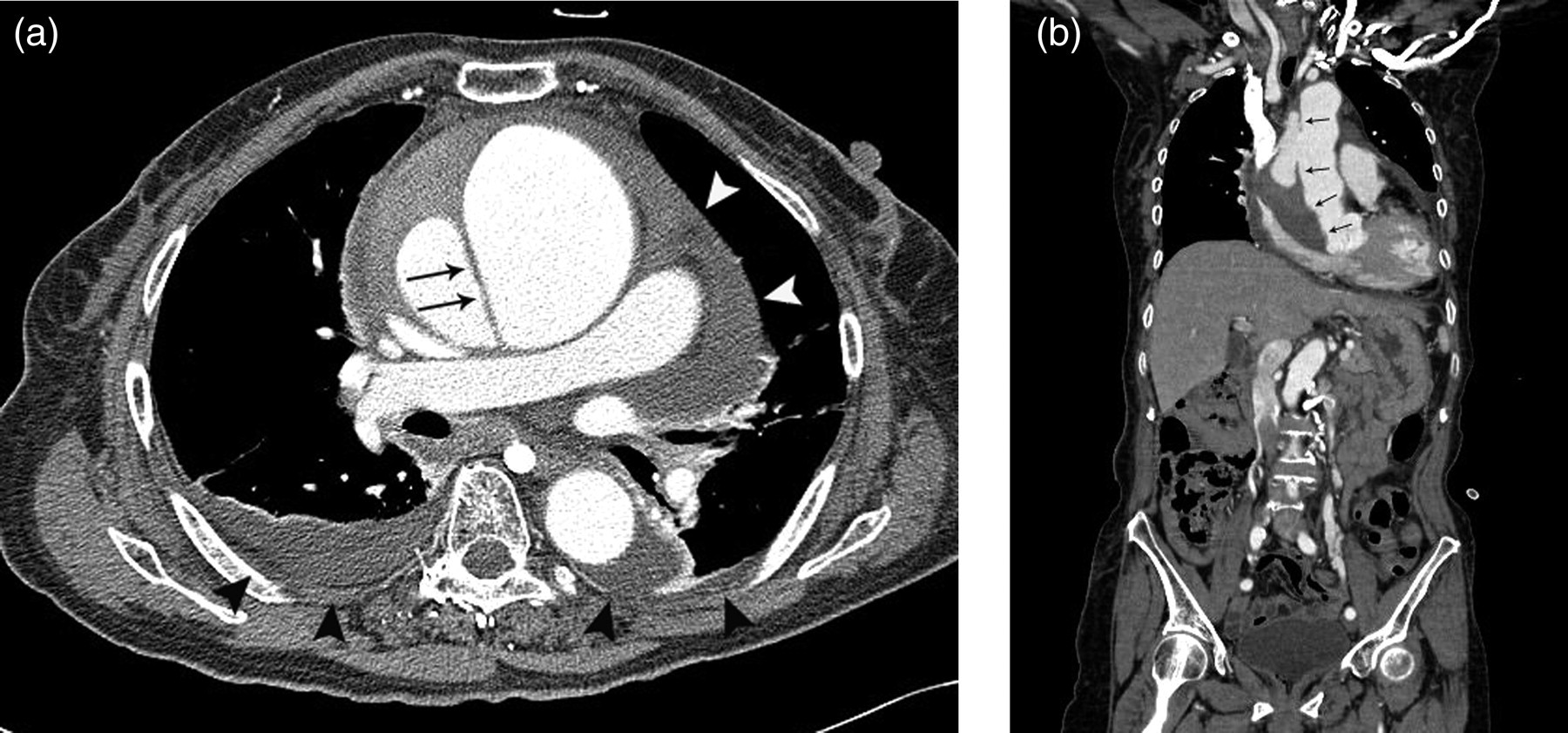
Stanford type A aortic dissection visualized in the field of view of dedicated coronary CT angiography in a 71-year-old woman. (a) Intimal flap (arrows) is noted on a contrast-enhanced transaxial CT image at the level of the right main pulmonary artery within the field of view of dedicated coronary CT angiography. Note both hemothorax (black arrowheads) and hemopericardium (white arrowheads) suggesting aortic rupture; (b) Intimal flap (arrows) extends into the field of view of dedicated coronary CT angiography as seen on a coronal multiplanar re-formatted image

Stanford type B aortic dissection visualized in the field of view of dedicated coronary CTA in a 67-year-old man. (a) Intimal flap (arrows) is noted on a contrast-enhanced transaxial CT image at the level of the left atrium. This image is within the field of view of dedicated coronary CT angiography; (b) Intimal flap (arrows) extends into field of view of dedicated coronary CT angiography as seen on a coronal multiplanar re-formatted image
Significant incidental non-cardiac findings
There were nine cases (5.9%, 9/153) with significant incidental non-cardiac findings that could be the cause of acute chest pain, including hiatal hernias (n = 5), pneumonia (n = 2), pneumomediastinum (n = 1), and an acute rib fracture (n = 1). All of these findings other than the one case of hiatal hernia were demonstrated in patients with a diagnosis of PE. All significant incidental non-cardiac findings were identified within the FOV of DCTA.
Discussion
Rapid diagnosis of life-threatening causes of acute chest pain is extremely important to improve patient outcome. There is substantial potential value in developing a non-invasive imaging study that permits expeditious triage of patients with non-specific acute chest pain because of the significant clinical overlap in presentation among serious conditions such as AAS, ACS, and PE (2, 11–14). A TRO protocol that can simultaneously evaluate life-threatening causes of acute chest pain may address this issue but carries a higher radiation exposure than DCTA. Although the radiation dose of TRO can be reduced by scanning the part of the chest above the FOV of DCTA with a non-gated protocol or by using strict automatic tube modulation, the radiation dose of TRO is often 50% higher than that of DCTA due to extended z-axis coverage of the former technique (8). Although one review article has suggested that most of PE and aortic dissection may be identifiable on DCTA, there was no study that formally addressed this assumption (8). The FOV of DCTA includes approximately the lower two-thirds of the entire thorax, excluding only the upper one-third. Because approximately two-thirds of the total pulmonary arterial blood flow is directed into the lower lungs which is included in the FOV of DCTA, isolated pulmonary embolus in the upper lobe would be expected to be uncommon. In our study, there were only two cases of PE (2/103, 1.9%) identified out of this FOV. There is debate as to whether isolated subsegmental PE should be treated (15–17). One study suggested that treatment with anticoagulation may be unnecessary in patients with asymptomatic subsegmental PE and good cardiopulmonary reserve (15). In addition, the right ventricular enlargement and straightening of the inter-ventricular septum which may indicate massive embolic burden and poor prognosis (18, 19) were not identified in our two cases with PE outside of the FOV of DCTA. Therefore, the presence of isolated PE out of the FOV of DCTA may indicate a small embolic burden and a benign clinical course. In the second case, pulmonary embolus in the left main pulmonary artery was not identified within the FOV of DCTA because the left main pulmonary artery was retracted by tuberculous scar in the left upper lobe. In patients without a fibrotic scarring in the upper lobe, the main pulmonary arteries would be often located within the FOV of DCTA. Therefore, most central pulmonary emboli except for those located in the anterior trunk supplying the right upper lobe would be detected on DCTA. It is important to recognize that fibrotic changes in the upper lobe may lead to upward retraction of main pulmonary artery and other vessels, causing a false-negative diagnosis for PE when performing DCTA. Similarly, the scan coverage of DCTA may be extended in patients with an unusually high position of the main pulmonary arteries or aorta on the chest radiograph. For example, the top of aortic arch lies above the medial ends of the clavicles in patients with a cervical aortic arch (20). The scan coverage of DCTA may be extended to avoid the false-negative diagnosis of AAS in patients with a cervical aortic arch.
There was no case of isolated AAS (0/50, 0%) outside of the DCTA FOV in our study. Although the entry tear site in Stanford type B aortic dissection is outside of the FOV of DCTA (i.e. descending thoracic aorta just distal to the origin of the left subclavian artery), there was a long flap extension from the entry tear site in all Stanford type B aortic dissections in our study, even on CT image performed immediately after symptom onset (21). In patients with aortic dissection, a lengthy intimal flap extending from the entry tear site may result from underlying pathology (e.g. aortic degenerative change) in the aorta (22). This progression of the intimal flap may continue until reaching a reentry tear or the occurrence of aortic rupture in patients with aortic dissection or intramural hematoma (21). All patients with Stanford type A aortic dissection and intramural hematoma were identified within the FOV of DCTA. The intimal flap was invariably demonstrated within the FOV of DCTA due to some degree of retrograde extension of entry tear in the ascending aorta, irrespective of the entry tear site. There was no case of penetrating atherosclerotic ulcer (0/7) found out of the FOV of DCTA. This presumably is due to the fact that the most common site of penetrating atherosclerotic ulcer with intramural hematoma is the middle or distal portion of descending thoracic aorta (9, 23). Because the present study comprised the small number of penetrating atherosclerotic ulcer cases (n = 7), further study is necessary to elucidate the frequency that penetrating atherosclerotic ulcer would be visible with a DCTA FOV.
One study has pointed out the importance of on-site radiologists when performing aortic dissection CT angiography (24). The scan range of aortic dissection CT angiography is from the thoracic inlet to both femoral heads. However, the study suggested that further scanning of the lower abdomen and pelvis (i.e. unjustified radiation exposure) should be stopped by on-site radiologists in patients with no evidence of aortic dissection when scanning the thorax and upper abdomen (24). Similarly, it is advisable for on-site radiologists to check DCTA immediately in order to detect PE or AAS that could be completely evaluated by additional scan coverage during the same CT examination.
One study indicated that diagnostic tests for at least two of the three diagnoses (i.e., ACS, AAS, or PE) were necessary in 22% (n = 139/626) of patients presenting with non-specific acute chest pain. Of these, diagnostic tests for ACS and PE and ACS and AAS were necessary in 19.3% (n = 121/626) and 2.2% (n = 14/626), respectively (25). However, the clinical situation in which ACS, AAS, and PE would need to be simultaneously excluded is rare (i.e. only 0.6% [n = 4/626] of patients presenting with non-specific chest pain). Therefore, this study suggests that TRO in the true sense is uncommonly necessary in real clinical situations. This is the reason why we considered two clinical scenarios for this study, ACS and PE or ACS and AAS.
Only limited information is available as to how to optimize CT protocols (i.e. DCTA versus TRO versus dedicated PE or aortic CT angiography) based on the specific presentation to the emergency department. One study reported that the presence of isolated pulse or blood pressure differentials or any combination of three variables (i.e. pulse or blood pressure differentials, significant mediastinal widening on chest radiograph, or aortic chest pain [i.e. severe tearing or ripping chest pain of sudden onset]) indicates high pre-test probability (>83%) of aortic dissection. The presence of one of last two variables was indicative of intermediate pretest probability (31%) of aortic dissection. The absence of three variables indicated low pretest probability (7%) of aortic dissection (26). A previous TRO study reported a low prevalence of PE (1.5%) and AAS (0.5%) in patients with undifferentiated acute chest pain and low to intermediate risk for ACS (27). In our study, isolated PE and AAS outside of the FOV of DCTA rarely occurred. Therefore, DCTA may replace TRO in the evaluation of patients with non-specific acute chest pain, but a low pretest probability of PE or aortic dissection.
There is a significant difference in contrast administration for TRO and DCTA that could affect the detection of PE. Adequate contrast enhancement of pulmonary arteries, the aorta, and coronary arteries is mandatory in TRO to simultaneously evaluate ACS, PE, and AAS. The total time necessary to administer the contrast material in TRO consists of scan time, trigger delay time, and pulmonary transit time (i.e. time for the contrast media to travel from pulmonary arteries to the aorta). Typical pulmonary transit time is approximately 11 s (4). In contrast, targets of ordinary coronary CT angiography are the coronary arteries and aorta, not the pulmonary arteries. Theoretically, the total time to administer the contrast material consists of scan time plus trigger delay time when performing coronary CT angiography for purposes other than the evaluation of non-specific acute chest pain (5). Therefore, pulmonary transit time should be taken into account when performing DCTA in patients with nonspecific acute chest pain, so that a false-negative diagnosis of PE can be avoided. One study indicated that contrast attenuation of pulmonary arteries in TRO (363 HU [253–424]) is significantly higher than that of dedicated PE CT angiography (235 HU [182–269], P = 0.001) if 100% contrast material with a high flow rate (5 mL/s) is used to opacify pulmonary arteries (28). In fact, several TRO studies used a dilute contrast material of variable concentration (30–70%) to cover the pulmonary transit time (1, 6, 7). These studies suggest that a dilute contrast medium can be also used to opacify pulmonary arteries when performing DCTA. However, further studies are required to adequately address this issue.
Recent studies have indicated that various non-cardiac findings other than ACS, AAS, and PE can rarely be the cause of chest pain in patients who undergo DCTA (29–31). In particular, incidental non-cardiac pathology (1.3%, 5/395) such as pneumonia (n = 3), cholecystitis (n = 1), or pneumothorax (n = 1) were identified as the etiology of acute chest pain in patients with low to intermediate risk for ACS in one recent study (31). In our study, there were nine cases (5.9%, 9/153) of such findings, which consisted of hiatal hernias (n = 5), pneumonia (n = 2), pneumomediastinum (n = 1), and an acute rib fracture (n = 1). All of these findings were identified within the FOV of DCTA. The results of our study suggest that the frequency of excluding findings of extra-cardiac pathology when using a restricted DCTA FOV is low.
This study has several limitations. First, it is retrospective with a small number of patients, possibly leading to bias. Second, a DCTA and TRO are ECG-gated whereas the cases used in this study were not. Non-ECG gated PE or aortic CT angiography was inevitably used in this study because incidence of AAS and PE identified on DCTA or TRO is extremely rare (i.e. both DCTA and TRO are mainly used for excluding ACS). For example, there were only three cases of PE (1.5%, 3/197) and one case of AAS (0.5%, 1/197) out of 197 patients with non-specific acute chest pain who had undergone TRO in the previous study (27). Third, the comparison of radiation dose between DCTA and TRO was not performed in this study. However, the previous study confirmed that the radiation dose of TRO is approximately 50% higher than that of DCTA due to extended z-axis coverage (8). Fourth, the DCTA was assumed to extend from the tracheal carina to the bottom of the heart in this study. However, some centers may not reconstruct a wide FOV as a matter of protocol. Also, some scanners cannot do this for technical reasons when operating in DCTA mode. Therefore, this study assumed an idealized situation where all the lung area in x-y axis is reconstructed.
In conclusion, as isolated PE, AAS, and significant non-cardiac pathology outside of the DCTA FOV rarely occur, DCTA may replace TRO in the evaluation of patients with non-specific acute chest pain and a low pre-test probability of PE or aortic dissection.