
Abstract
Background
Since the first outbreak caused by the pandemic H1N1 2009 influenza in Mexico, the virus has spread widely across the world with meaningful morbidity and mortality. However, there are few data on the comparative investigations to assess the clinical and radiological features between the H1N1 patient and non-H1N1 patients.
Purpose
To assess the clinical and radiological features of patients infected by the pandemic H1N1 2009 flu virus at their initial presentation and to compare them with contemporaneous non-H1N1 patients with acute febrile respiratory illness.
Material and Methods
This retrospective study was approved by the ethics committee of the Armed Forces Medical Command, South Korea. From August to September 2009, 337 consecutive patients presented with an acute febrile respiratory illness in a tertiary military hospital. Reverse-transcriptase polymerase-chain-reaction tests were performed in 62 of these patients under the impression of H1N1 infection. Clinical and radiological features at their initial presentation were described for the H1N1 group (n = 35) and non-H1N1 group (n = 27) and compared between the two groups.
Results
Increased C-reactive protein level (97%) without leukocytosis (9%) or increased erythrocyte sedimentation rate (0%) was common in the H1N1 group at their initial presentation. On chest radiographs, 12 of 35 (34%) H1N1 patients had abnormal findings; nodules in 10 patients (83%) and consolidations in two (17%). Of the 28 H1N1 patients who underwent thin-section CT 16 patients (57%) showed abnormal findings; ground-glass opacities (GGOs) in 15 (94%), and nodules in 13 (81%). However, there were no significant differences between the H1N1 group and non-H1N1 group in terms of symptoms, laboratory results, or radiological findings (P > 0.05).
Conclusion
Patients with H1N1 infection show consistent clinical and radiological features at their initial presentation, however, clinical and radiological features of the H1N1 group are not significantly different from those of the non-H1N1 group.
In April 2009, an outbreak of influenza was reported in Mexico that was later found to be caused by the pandemic H1N1 2009 influenza virus. The virus has since spread to over 170 countries and territories, and on June 11, 2009, the World Health Organization (WHO) raised the level of pandemic alert to 6 (1). As of September 27, 2009 the total number of confirmed cases and deaths worldwide was 343,298 and 4108, respectively (2).
Appropriate and prompt diagnosis of the pandemic H1N1 2009 influenza virus infection is very important with respect to both the effective treatment of infected patients and proper interruption of the transmission of this disease in the community (3), and clinical and radiological features can be helpful in establishing the prompt detection of suspicious patients for the pandemic H1N1 2009 influenza virus infection and radiologists should be familiar with these clinical and radiological features.
In this context, several papers have been published on the clinical features and the radiographic findings of the pandemic H1N1 2009 influenza virus infection (4–13). However, there have been no comparative analyses between the pandemic H1N1 2009 influenza virus infection and other acute respiratory illness that should be differentiated from the pandemic H1N1 2009 influenza virus infection. Furthermore, with respect to the previous papers regarding the radiological features of the pandemic H1N1 2009 influenza virus infection, the number of the study population was either very small or the period between symptoms onset and radiological examinations was variable and the initial radiographs obtained at the time of their first clinic visit were not available (12). An even more problematic issue was that there was no laboratory evidence of confirmed pandemic H1N1 2009 flu virus infection in a considerable proportion of the study populations (12, 13).
Therefore, the purpose of this study was to assess the clinical and radiological features of patients with laboratory-confirmed pandemic H1N1 2009 flu virus at their initial presentation, and to compare them with features of other acute febrile respiratory illness patients.
Material and Methods
This retrospective study was approved by the ethics committee of the Armed Forces Medical Command, South Korea, which waived the requirement for informed consent.
Study population
From August to September 2009, 337 male soldiers who presented with an acute febrile respiratory illness (fever of 38°C or higher, and/or a new or worse cough, and/or shortness of breath) and were clinically suspicious to be infected with the pandemic H1N1 2009 flu virus infection, visited the emergency department and the outpatient clinic of a tertiary military hospital. In case a number of soldiers were from the same barrack, a nasopharyngeal swab for the confirmatory laboratory test was performed in a patient with the most severe clinical symptoms. Due to the large number of patients and a limitation of the laboratory capacity of our hospital, we were not able to perform confirmatory laboratory tests for the pandemic H1N1 2009 flu virus in all patients. Among the 337 patients, a nasopharyngeal swab was collected in 62 patients (mean age 20 years; range 19–22 years) either at the emergency department (n = 47) or the outpatient clinic (n = 15), and real-time reverse-transcriptase–polymerase-chain-reaction (RT-PCR) tests and viral cultures were performed in accordance with WHO guidelines to confirm the pandemic H1N1 2009 influenza virus infection in these 62 patients (14). Among these 62 patients, 35 patients (mean age 20 years; range 19–22 years) were confirmed to be infected with the pandemic H1N1 2009 flu virus (H1N1 group) and the remaining 27 patients (mean age 21 years; range 20–22 years) were confirmed not to be infected with the pandemic H1N1 2009 flu virus (non-H1N1 group). Oseltamivir phosphate (Tamiflu®, Roche, Basel, Switzerland) was administrated in the H1N1 group and patients in the non-H1N1 group were managed conservatively under the impression of seasonal flu infection, and all of them recovered after treatment. The mean interval between symptoms onset and ER visit were 1.72 days ± 1.43 (range 0–5 days) and 1.71 days ± 1.45 (range 0–5 days) in the H1N1 and non-H1N1 groups, respectively. These two groups (H1N1 group and non-H1N1 group) comprised the study population in this study. Clinical symptoms, laboratory results, and radiological features at their initial presentation were retrospectively described for each group and a comparison was made between the two groups.
Review of symptomatic and laboratory characteristics
Two of the authors (TJY and GJK) retrospectively recorded each patient's symptoms and laboratory results at their initial presentation using electronic medical charts. For review of the clinical features, initial symptoms such as fever, cough, sputum, rhinorrhea, sore throat, myalgia, headache, dizziness, vomiting, and diarrhea were recorded. The laboratory data collected were as follows: hematological analysis findings including white blood cell (WBC) count; red blood cell (RBC) count; hemoglobin level (Hb); hematocrit level (Hct); platelet count and neutrophil count; and biochemical analysis findings including creatine kinase (CK), erythrocyte sedimentation rate (ESR), and C-reactive protein (CRP) level.
Review of radiological features
Chest radiographs were available for all enrolled patients, and thin-section CT images were available for 55 out of 62 patients; in 28 H1N1 patients and all 27 non-H1N1 patients. All chest radiographs and thin-section CTs were performed on the day when the patients visited the emergency department or the outpatient clinic of our hospital.
Chest radiographs were obtained using digital radiographic equipment (TDR4600-F80; Gold Mountain Medial systems, Seoul, Korea) and a standardized technique: 110 kVp, 2 mAs, and a 180-cm film-focus distance for posteroanterior views. Thin-section CTs of the thorax were performed using a 16 channel CT scanner (Brightspeed; GE Healthcare, Milwaukee, WI, USA), with a 1.25 mm slice thickness, in the supine position. Scanning was performed during inspiration over a 6 s scan time, at 120kVp and auto mA.
All chest radiographs and thin-section CT images were evaluated in consensus by three chest radiologists (CMP, HJL, and JMG, who had 8, 10, and 16 years of thoracic radiology experience, respectively) who were blinded to the clinical information.
Each chest radiograph was assessed in terms of the presence of nodular opacity, consolidation, interstitial patterns, atelectasis, mediastinal abnormalities, and pleural effusion (15). Thin-section CT findings were interpreted by using the descriptors proposed by the Fleischner Society Nomenclature Committee, and were assessed in terms of the presence and extent of ground-glass opacity (GGO), nodule, consolidation, and reticulation: a GGO was defined as hazy increased opacity without obscuring the underlying bronchial and vascular structures (16). A nodule was defined as a rounded or irregular opacity measuring up to 3 cm in diameter. Consolidation was defined as a homogeneous increase in pulmonary parenchymal attenuation that obscured the margins of the vessels and airway walls. And reticulation was defined as a collection of innumerable small linear opacities that, by summation, produced an appearance resembling a net (16). To quantify the extent of each abnormality, thin-section CT scores were assigned based on areas involved. A score of 0–10 (None: 0, ≤10% involvement of the lobe: 1, 10% < and ≤20% of lobe: 2, etc.) was assigned to each pulmonary lobe (total overall score 0–60). This system is a modified method previously used in evaluating idiopathic pulmonary fibrosis (17, 18). In the present study, the left upper lobe was separated into the superior division and lingular division that corresponded with the right upper lobe and the right middle lobe, respectively. And, the involvement of superior division and lingular division were regarded as involvement of upper lobe and middle lobe, respectively. In addition, other abnormalities such as pleural effusion, lymphadenopathy, cavitation, calcification, and septal thickening were also evaluated.
Statistical analysis
The statistical differences between the H1N1 group and non-H1N1 groups were analyzed using Fisher's exact test for the patients' symptoms, and the presence of radiological abnormalities. The statistical differences in the degree of fever, the laboratory results and the extent of radiological abnormalities were analyzed using an independent sample t-test. A P value of less than 0.05 was considered statistically significant. All statistical analyses were performed using the SPSS software package (version 16.0 for Windows, SPSS, Chicago, IL, USA).
Results
Clinical features of patients in H1N1 group
Symptomatic and laboratory data of the 62 study subjects are summarized in Tables 1 and 2. In the H1N1 group, all 35 patients presented with high fever (>38.0°C), with a mean temperature of 38.6°C ± 0.41. Common accompanying symptoms were cough (83%), sputum (63%), myalgia (57%), sore throat (46%), and headache (46%).
Patients' symptoms
* Data are numbers of abnormal patients divided by the total number of patients
† P values were calculated using the unpaired t-tests for fever and using Fisher's exact tests for other variables
Laboratory findings
*Data are numbers of abnormal patients divided by the total number of patients
† P values were calculated using the independent sample t-test
Leukocytosis was evident in only three patients (9%). Most of the patients in the H1N1 group (32 out of 35 patients) had a normal WBC count. Lymphocytopenia was a relatively common finding (26%). ESR was not elevated in any H1N1 patient although the CRP value was elevated in 97% of the H1N1 patients.
Radiological features of patients in the H1N1 group
Presence of a specific abnormality
Twenty-three of the 35 (66%) H1N1 patients had no abnormalities on chest radiographs (Fig. 1a). In the remaining 12 patients (34%) showing abnormal chest radiographic findings, nodular opacity was observed in 10/12 (83%) and was the most common radiographic abnormality (Fig. 2a). Consolidations, however, were found in just two of the 12 patients (17%).
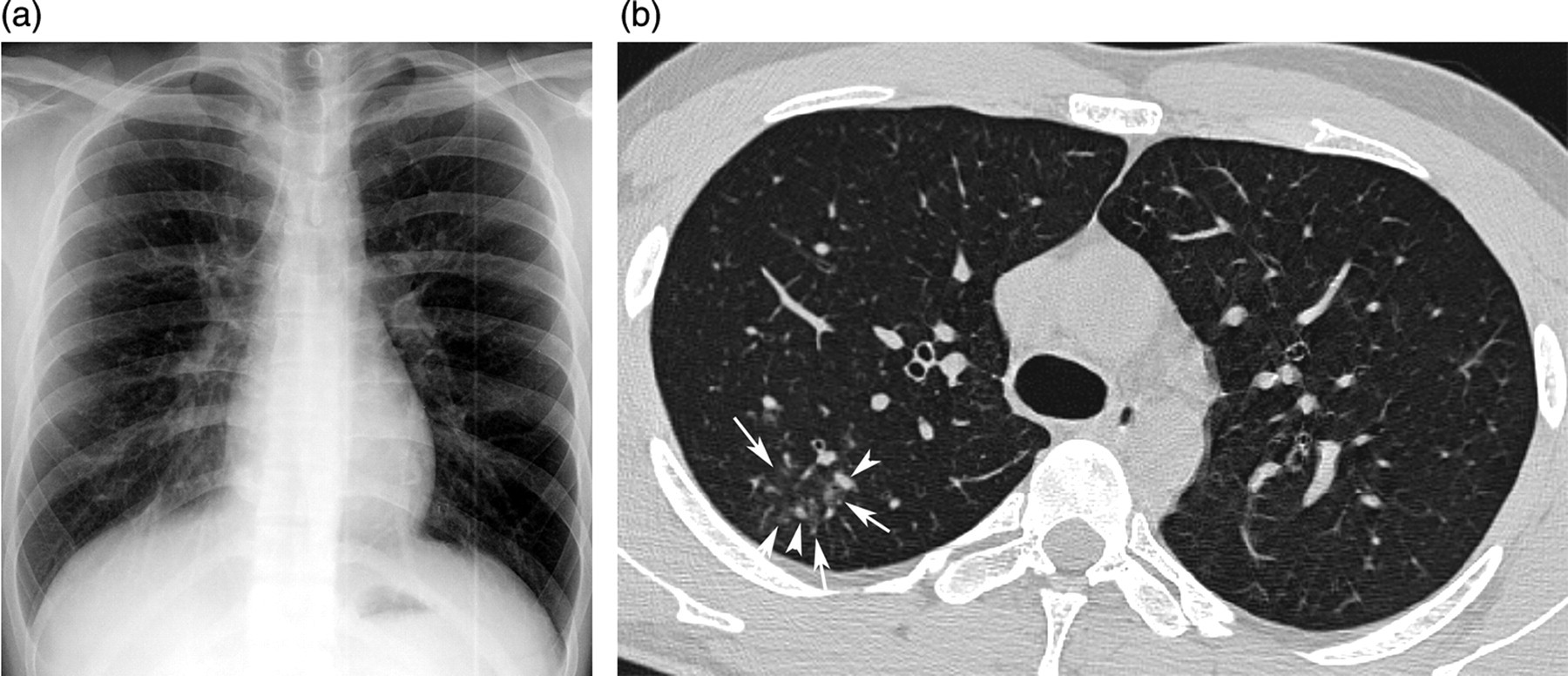
Ground-glass opacities and nodules in a 20 year-old man with pandemic H1N1 2009 flu virus infection. (a) Plain chest radiograph shows no abnormalities; (b) Thin-section chest CT image shows ground-glass opacities (arrows) in the right upper lobe of the lung. A few small nodules (arrowheads) are also observed around the ground glass opacities

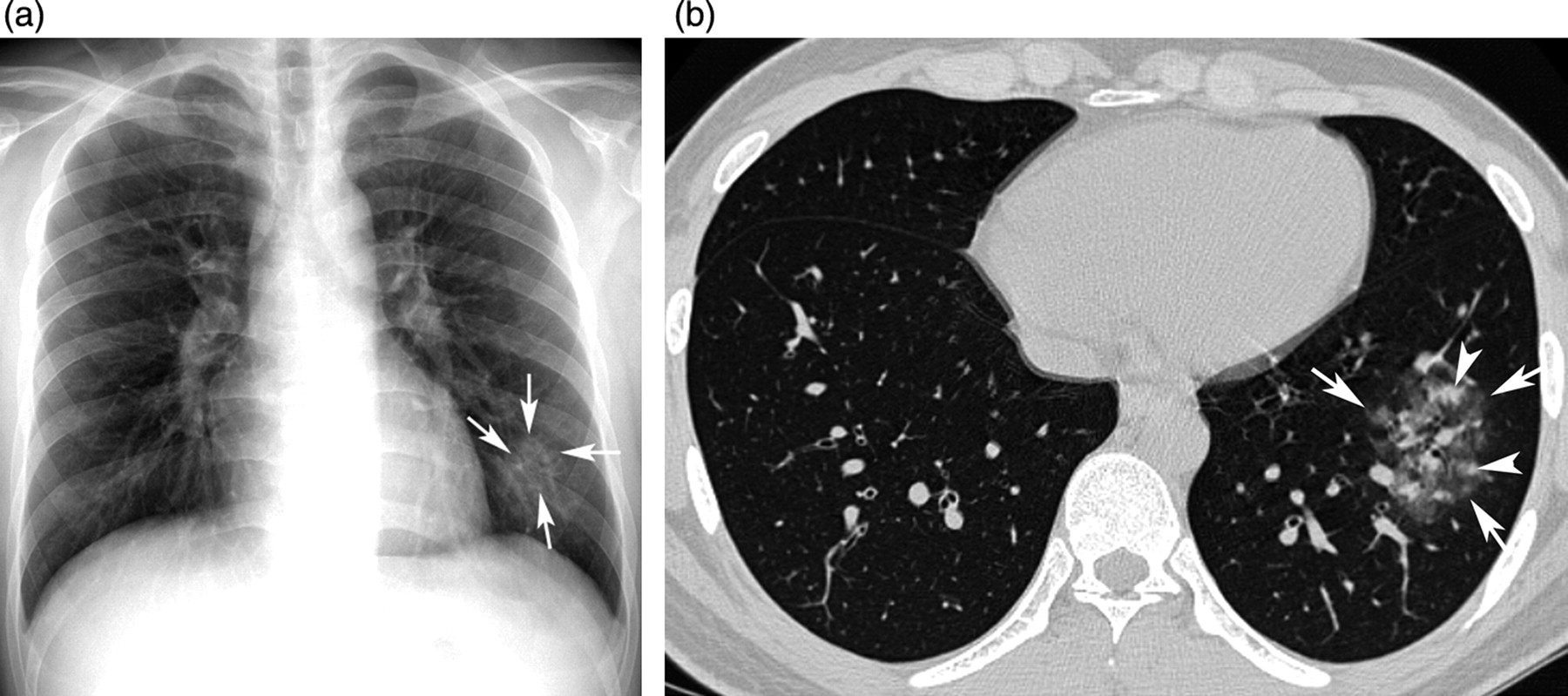
Ground-glass opacities in a 21 year-old man with pandemic H1N1 2009 flu virus infection. (a) Plain chest radiograph shows nodular opacities (arrows) in the right lung; (b) Thin-section chest CT image shows a few ground-glass opacities (arrows) in the right upper lobe of the lung; (c) Thin-section chest CT image shows multiple ground-glass opacities (arrows) in the right middle lobe and both lower lobes of the lung
Thin-section CT findings of the 28 patients in the H1N1 group are summarized in Table 3. Sixteen of these 28 patients (57%) had abnormal CT findings; 15 of the 16 (94%) had GGOs, and 13 (81%) had nodules (Figs. 1b, 2b and c). Consolidations and reticulations were uncommon and observed in 25% and 6% only of patients in the H1N1 group, respectively. Other abnormalities such as pleural effusion, lymphadenopathy, cavitation, calcification, or septal thickening were not found in any patient in the H1N1 group.
Presence of abnormality on thin-section CT images
*Data are numbers of abnormal patients divided by the total number of patients
† P values were calculated using Fisher's exact tests
‡Fisher's exact test was not applicable
UL = upper lobe involvement, ML = middle lobe involvement, LL = lower lobe involvement
Extent of a specific abnormality
The extents of a specific abnormality in the thin-section CT findings of 28 H1N1 patients are summarized in Table 4. The total extent score of the 28 H1N1 patients was 86 and the mean extent score in the 16 patients with abnormal findings was 5.38. GGOs and nodules contributed mostly to pulmonary parenchymal abnormalities (51 and 22, respectively) and scores for consolidations and reticulations were 7 and 6.
Extent of abnormalities in thin-section CT images
*P values were calculated using the unpaired t-tests
†Unpaired t-test was not applicable
UL = upper lobe involvement, ML = middle lobe involvement, LL = lower lobe involvement
Clinical and radiological features of patients in the non-H1N1 group
Tables 1 and 2 summarize the radiological features of the 27 non-H1N1 patients. In terms of the presence of specific radiological abnormalities, 15 of 27 non-H1N1 patients (56%) had no abnormalities on chest radiographs. In the remaining 12 non-H1N1 patients, eight had nodular opacities, and four had consolidations (Figs. 3a and 4a). Fourteen of the 27 non-H1N1 patients (52%) had abnormalities on CT examinations; 12 had GGOs (86%) and 10 out of 14 (71%) had nodules, which were the most common CT abnormalities in the non-H1N1 group (Fig. 3b). Consolidations were found in seven patients (50%) and reticulation in four (Fig. 4b).
Ground-glass opacities and nodules in a 21 year-old man presented with acute respiratory febrile illness by non-H1N1 causes. (a) Plain chest radiograph shows nodular opacities (arrows) in the left lower lung zone; (b) Thin-section chest CT image shows ground-glass opacities (arrows) in the left lower lobe of the lung. A few small nodules (arrowheads) are also observed around the ground glass opacities

Consolidation in a 22-year-old man presented with acute respiratory febrile illness by non-H1N1 causes. (a) Plain chest radiograph shows consolidation (arrows) in the left middle and lower lung zones; (b) Thin-section chest CT image shows consolidation (arrows) in the lingular segment of left upper lobe of the lung
Comparative analysis between the H1N1 group and non-H1N1 group
With respect to either clinical or radiographic characteristics, no significant differences were found between the H1N1 group and non-H1N1 group.
With respect to thin-section CT features, consolidations and reticulations tended to be observed more frequently in the non-H1N1 group than in the H1N1 group (50% vs. 25% and 29% vs. 6%, respectively). Abnormal lesions were located in the upper lobes with greater prevalence in the H1N1 group than in the non-H1N1 group (63% vs. 36%). However, these differences were not statistically significant. With respect to the extent of the specific radiological abnormalities, there were no significant differences between these two groups.
Discussion
With respect to symptoms in patients with the pandemic H1N1 2009 flu virus infection, we found that high fever (fever ≥38°C), cough, and sputum were the most common clinical features. These results are in concordance with most previous reports, which have also reported that the signs and symptoms of pandemic H1N1 2009 flu virus infection were similar to those of seasonal flu although they did not perform a comparison analysis between the pandemic H1N1 2009 flu infection and seasonal flu infection (6, 9–11). Indeed, in the present study, we found that the initial symptoms of the H1N1 group were similar to and were not significantly different from those of the non-H1N1 group with other acute febrile respiratory illnesses, who were thought to be infected by seasonal flu and were managed conservatively or with antiviral agents, all of whom recovered after treatment.
It has been known that laboratory results, with the exceptions of serology and culture, are not diagnostic for flu infection; leukocyte counts were shown to be variable, and were frequently low or normal during the early stages of this viral infection (19). In the present study, we found that 91% of patients of the H1N1 group did not show leukocytosis. This result can be explained by the fact that the patients in our H1N1 group were in the early stages of pandemic 2009 H1N1 flu at their initial presentation. The other interesting laboratory results from our study was that the CRP level was elevated in 97% of patients while ESR level was within normal limits in all patients of the H1N1 group. We believe that elevated CRP combined with a lack of leukocytosis or elevated ESR may be characteristic of patients with flu virus infection, and these findings could be helpful to differentiate them from bacterial pneumonia.
According to recent papers describing the radiological features of pandemic H1N1 2009 flu infection, chest radiographs were abnormal in 42% of infected patients (12, 13). Patchy consolidations were the most common radiographic features and the incidence of these findings occurred in 50–57% of patients with abnormal radiographic findings (12, 13). In the present study, chest radiographs were abnormal in 34% of patients with H1N1, which was slightly less than that of previous reports (12). In terms of specific radiographic abnormalities, nodular opacities (83%) were the most common abnormal findings in the present study and consolidations were relatively uncommon (17%). With respect to thin-section CT features, 57% of H1N1 patients showed abnormal findings in the present study, and GGOs (94%) and nodules (81%) were the most common CT abnormalities with consolidations occurring in just 25% of H1N1 patients with abnormal CT findings. However, in the previous two studies, multifocal consolidations were the most common CT abnormalities of H1N1 patients, and nodules were rare in their studies (12, 13). These differences might be explained by the fact that radiological examinations including chest radiographs and thin-section CTs in the present study were performed at their initial presentation and probably in the early stages of the disease, whereas in previous studies, chest radiographs and CT examinations were performed in various periods after symptoms onset, particularly at a progressed state of the disease (12, 13). Furthermore, Agarwal et al. included a considerable amount of patients who were not confirmed with pandemic H1N1 2009 flu through confirmative laboratory tests (12).
Knowledge about whether there is any difference between the H1N1 group and non-H1N1 group manifesting as acute febrile respiratory illnesses could be clinically relevant and important both in terms of the diagnosis of H1N1 flu infection and ruling out other causes of acute febrile respiratory illnesses in clinical practice, although there are other confirmative methods such as RT-PCR tests and viral cultures for the diagnosis of the pandemic H1N1 2009 flu virus infection. Unfortunately, there were no significant differences between the H1N1 group and non-H1N1 group in terms of initial symptoms, laboratory variables, and radiological features in the present study. In particular, with regard to radiological features, there were no significant differences between the H1N1 group and non-H1N1 group in spite of an effort to quantify the extent of specific abnormalities.
There are several limitations in this study. First, due to the large number of patients and limitations in laboratory capacity of our hospital, we were not able to perform confirmatory laboratory tests for the pandemic H1N1 2009 flu virus in all patients manifesting with acute febrile respiratory illness, possibly resulting in selection bias. Second, all patients in our study were young, healthy soldiers with no concomitant chronic diseases affecting their immunity. This homogeneity of our population may be helpful in terms of understanding the clinical characteristics of pandemic H1N1 2009 flu virus and may add to the validity of this comparative study. However, there may be limitations in applying the results of our study to the larger general population or population with high risks for complications such as patients with concomitant chronic diseases, women who are pregnant, or older patients.
In conclusion, patients with H1N1 infection show consistent clinical and radiological features at their initial presentation, however, their clinical and radiological features of H1N1 group are not significantly different from those of non-H1N1 group.
Footnotes
ACKNOWLEDGEMENT
This study was supported by a grant from Bayer Schering Pharma AG.