
Abstract
The importance of autopsy procedures leading to the establishment of the cause of death is well-known. A recent addition to the autopsy work flow is the possibility of conducting postmortem imaging, in its 3D version also called virtual autopsy (VA), using multidetector computed tomography (MDCT) or magnetic resonance imagining (MRI) data from scans of cadavers displayed with direct volume rendering (DVR) 3D techniques. The use of the data and their workflow are presented. Data acquisition was performed and high quality data-sets with submillimeter precision were acquired. New data acquisition techniques such as dual-energy CT (DECT) and quantitative MRI, then were implemented and provided additional information. Particular findings hardly visualized in conventional autopsy can rather easy be seen at the full body CT, such as air distribution, e.g. pneumothorax, pneumopericardium, air embolism, and wound channels. MRI shows natural deaths such as myocardial infarctions. Interactive visualization of these 3D data-sets can provide valuable insight into the corpses and enables non-invasive diagnostic procedures. In postmortem CT imaging, not being limited by a patient depending radiation dose limit the data-sets can, however, be generated with such a high resolution that they become difficult to handle in today's archive retrieval and interactive visualization systems, specifically in the case of full body scans. To take full advantage of these new technologies the postmortem workflow needs to be tailored to the demands and opportunities that the new technologies allow.
Keywords
Traditional invasive autopsy is today's state of the art in forensic and pathological investigation. Modern cross-section techniques can assist and supplement conventional autopsy providing improvements for the general workflow of postmortem examinations. The importance of autopsy procedures leading to the establishment of the cause of death is well-known. In forensic cases, the autopsy provides key information and guides the criminal investigation. Recent developments in postmortem imaging have led to an implementation of postmortem CT (pmCT) and postmortem MRI (pmMRI) for the benefit of forensic investigations. Different studies published over the past 10 years have demonstrated that in future a combination of autopsy techniques and cross-sectional imaging can augment the value of postmortem examinations for the jurisdiction (1–9). Contrary to the forensic field the autopsy numbers of clinical pathological examinations suffer from a continuous decline and that has become a serious issue (10–13). The recent addition of postmortem imaging to the autopsy workflow of forensic examinations and the experiences obtained therein may provide the scientific background for an implementation of postmortem imaging as a substitute for all the clinical pathological examinations that are unfortunately not performed anymore for different reasons. It may be considered for the clinical cases not undergoing a traditional autopsy. Depending on the country up to more than 90% of the deceased do not undergo a comprehensive postmortem examination. The negative consequences for medical education, quality assurance in medicine, public health, and mortality statistics are substantial as discussed by numerous authors (10, 12, 14, 15). Postmortem imaging has matured to a valuable postmortem examination method to acquire patho-anatomic details with a high spatial resolution. An increasing number of forensic institutes have started to install CT and MRI systems to use the imaging techniques for the purpose of quality improvements in the forensic field. However, it is the natural death that is significantly under-autopsied today and it seems obvious to us that clinicians should become aware of the potential and the recent progress of pmCT and especially pmMRI as a non- or minimal-invasive method for the investigation of the deceased patient. The aim is not to replace clinical autopsies but to complement or offer an alternative when autopsy is not agreed by next of kin and to re-establish a reliable base of data of cause of death in our society.
In the forensic field, on the other hand, the aim is to improve postmortem investigations and documentation by a combination of postmortem imaging and autopsy techniques. PmCT and pmMRI can support traditional autopsy in numerous ways. Findings can be visualized for the court room in a bloodless manner, the individual autopsy approach can be optimized based on the knowledge already obtained at imaging, several findings are provided that are only difficult or even impossible to demonstrate at autopsy (6) and the entire volume of the corpse is documented in real dimensions in an observer-independent manner allowing for innumerous virtual dissections without destroying key evidence. These data also provide the base for forensic reconstruction using real case data in real dimensions (16).
However, the useful combination of traditional autopsy and postmortem imaging faces problems. Looking at the infrastructure needed there are often two sites, a forensic institute and a radiological institute that have to be connected by sufficient corpse logistics. Furthermore, a sufficient data exchange has to be set up to allow both parties using the data. And in the end it is also the different expertise of radiologists and forensic pathologists that meets at interpretation of postmortem CT and MR images. Whereas the radiologist is used to assess the images in order to establish the diagnoses that can guide a future therapeutic strategy it is the forensic pathologist who searches the past within the images. These different views have to be combined to really use the potential of postmortem imaging for the benefit of forensic investigations. Furthermore, there is an increasing need to solve problems of data handling of whole body data-sets with slice stacks up to 10000 images. Postmortem imaging not being limited by any radiation dose restrictions or scanning time limits can make use of the theoretically possible spatial resolution in both modalities what boosts the data volume to be handled. Especially three-dimensional visualization gains importance in the forensic field as visualization is mainly for medical laymen (judges, lawyers, police representatives, next of kin, etc.) who very much benefit from not being limited to cross-sections presented as grey value images.
Facing these challenges it is crucial to establish optimized processes and work flows addressing the needs of both parties and probably even more important to align the different expertise focused on the important forensic questions, which often differ from the clinical ones. The aim of the present publication is to introduce the postmortem imaging activities as performed at the publications host center which were started in the year 2003 and improved ever since to what we today call a state of the art pipeline for postmortem imaging with special focus on visualization of postmortem imaging (PMI) data for forensic purposes. Using MDCT and MRI data from scans of human corpses presented with direct volume rendering (DVR) 3D techniques provide the foundation for a so-called virtual autopsy (VA). The modern imaging modalities can generate such large, high quality data-sets with submillimeter precision so that interactive visualization of these 3D data-sets can provide valuable insight into the corpses and enables noninvasive diagnostic procedures.
From the clinical viewpoint this development may also be interesting as performing the validation process on living patients normally has its limitations. It can in some cases be impossible to know if the acquired diagnostic information is correct as long as the patient is alive, as the real gold standard remains missing. Postmortem imaging has the potential to solve this problem as by validating postmortem imaging against autopsy also clinically obtained radiological diagnoses get substantial background from these postmortem activities.
The procedure and general workflow issues
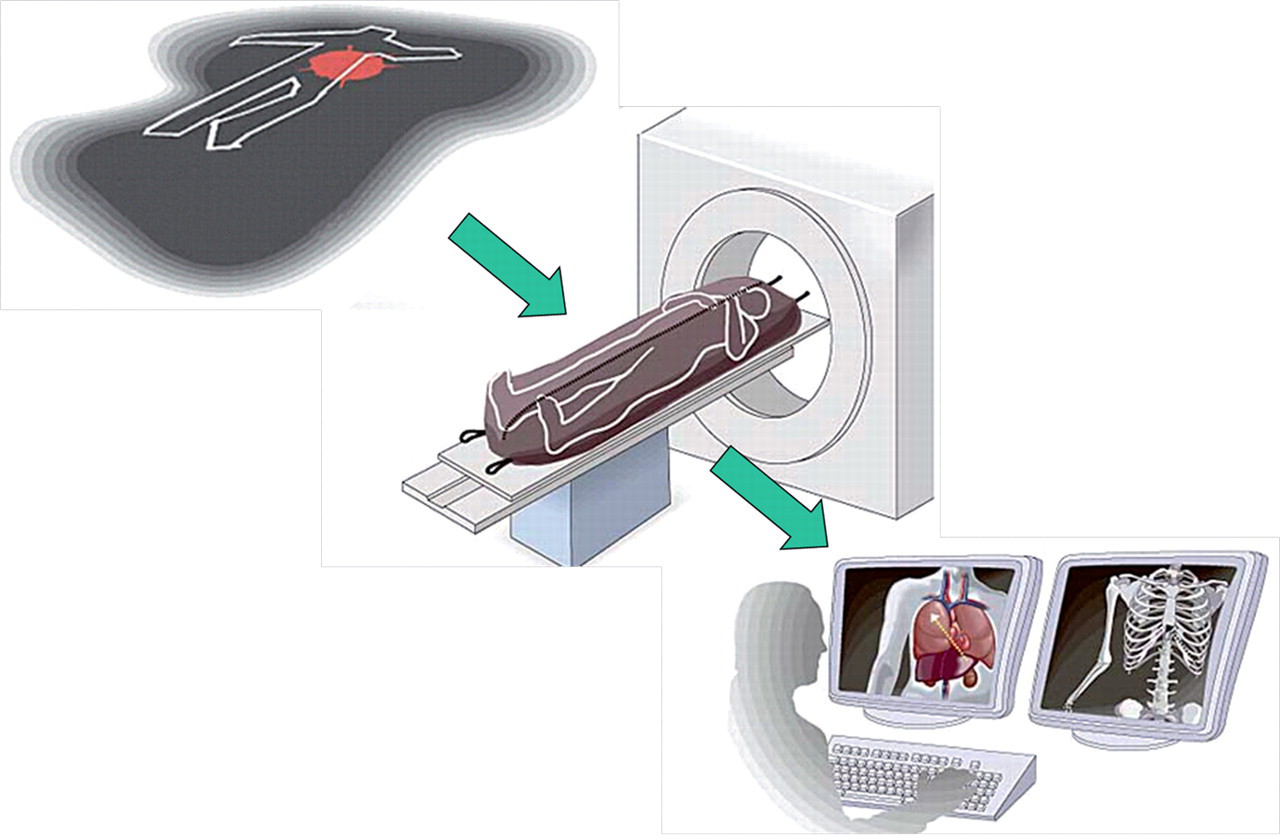
To be able to acquire sufficient pmCT image quality it is an advantage to have a scanner that can conduct a full body scan with submillimeter slices in extended field of view. The scan time is not crucial but if the scanning procedure is taking place at the radiology department it is easier to fit into the normal workflow if a fast scanner is used. Then examinations can be carried out early in the morning before the scheduled patients arrive. With thin slices and a small reconstruction interval up to 25 GB of data can be acquired in a single pmCT examination and that puts a lot of demands on the digital network, workstations, and the digital archive. The Center for Medical Image Science and Visualization (CMIV) at Linköping University Hospital in Sweden, in collaboration with the Swedish National Board of Forensic Medicine, has developed a procedure for postmortem imaging that is now routinely used for forensic casework (Fig. 1). This method has been in use since 2003 and has been applied to over 300 cases so far (mainly homicides). Our work has focused on optimizing the total workflow for pmCT and pmMRI up to developing a new type of software that can visualize full-body data-sets that could previously only be viewed in separate parts and with limited interactivity as well as to generate a three-dimensional visualization of quantified pmMR data of corpses.
From scene investigation over data acquisition to data visualization in a postmortem imaging workflow
In the beginning it was mainly the administrative effort that dominated the optimization process. The question of when and where to integrate postmortem imaging into the existing crime scene investigation (CSI) and forensic workflow had to be answered and also what kind of report shell be send to the judges (Fig. 2).
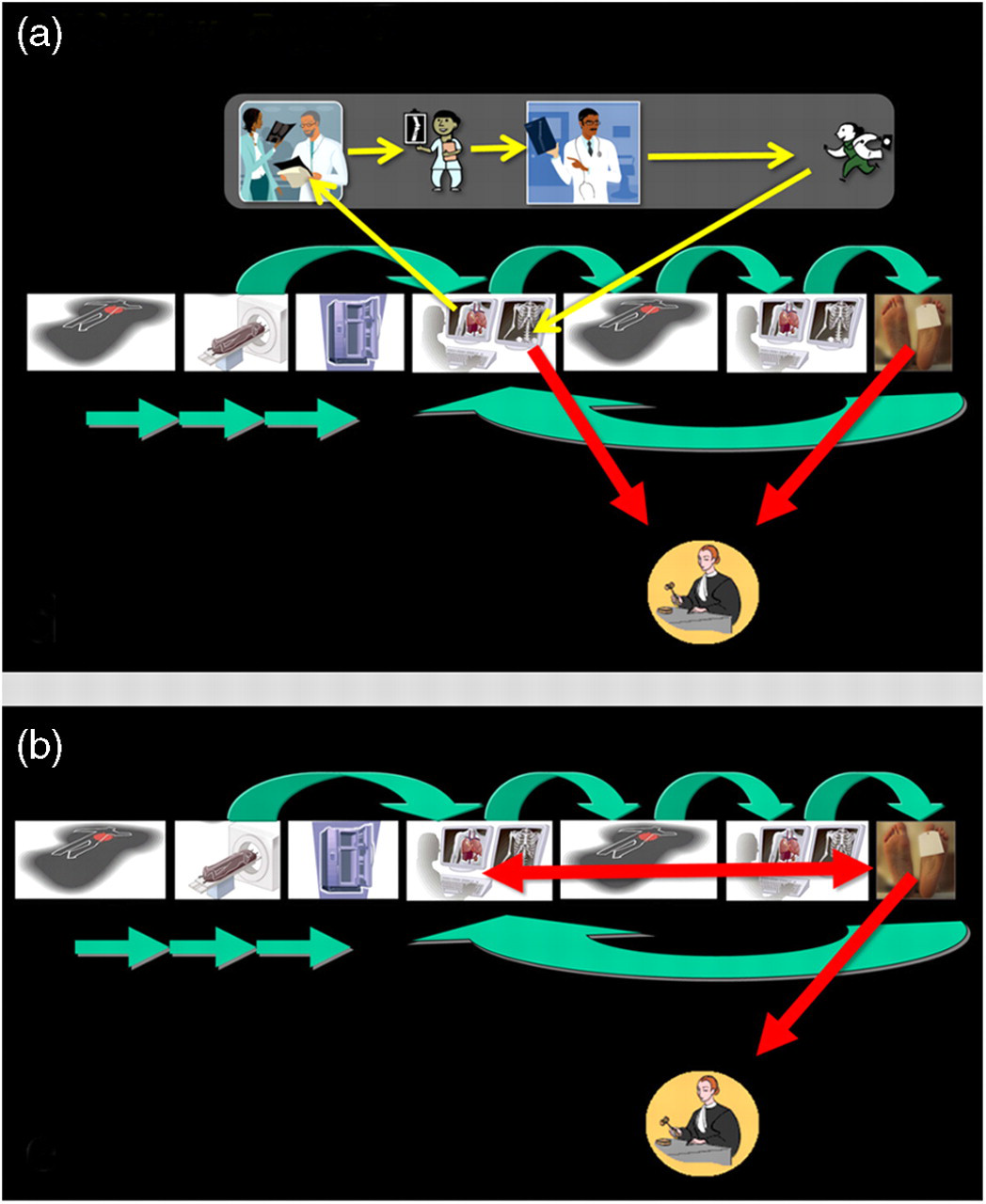
(a) When the postmortem CT examinations where introduced in the routine forensic workflow images were send to different subspecialties. As a result of this approach postmortem imaging suffered from high costs and a long waiting time on the report and in the end the judges were rather confused than satisfied! (b) Today three radiologists and one forensic doctor have specialized in postmortem imaging and only one common report summarizing the findings of pm imaging and autopsy leaves the forensic department. That facilitates assessment of the reports by the judges and prevents inconsistent information between several reports
The modalities and data acquisition
PmCT
In most cases, the forensic pathologist visits the crime scene and oversees the handling of the human corpse, which is placed in a sealed body bag before being transported to the forensic department and put in cold storage. The following morning, a full-body dual source CT (DSCT) scan is performed at CMIV (SOMATOM Definition Flash; Siemens Medical Solutions, Erlangen, Germany). Currently, both single- and dual-energy modes are used for forensic cases. A full-body data-set, if necessary in extended field of view (eFoV), is saved to have the entire body documented including the arms and elbows (120 kV, 250 Q ref. mAs, 128 × 0.6-mm collimation, rotation time 1 s, pitch 0.45, 512 matrix, voxel size 1 mm isotropic, B45 reconstruction kernel). Furthermore, a data-set reconstructed in an extended CT scale is saved when foreign bodies such as projectiles, fragments of knife blades, et cetera, are present. An additional ultra-high resolution scan of the dentition, with small field of view and overlapping slices, (z-Sharp™ technology, 120 kv, 182 mAs, 12 × 0.3-mm collimation, rotation time 1 s, pitch 0.9, 512 matrix, voxel size 0.24 mm isotropic, U70 reconstruction kernel, extended CT scale) is acquired to optimize dental visualizations (17–19). Ultra-high resolution scanning and reconstruction in extended CT scale allows for a low-artifact visualization of the dentition including fillings and restorations useful for forensic identification as well (Fig. 3) (17). Dual energy CT (DECT) distinctively improves soft tissue discrimination and visualization (3). DECT with two X-ray sources running simultaneously at different energies can acquire two data-sets showing different attenuation levels. DECT allows additional information about the elementary chemical composition of CT scanned material to be obtained. Compton scattering can be determined by using two different average photon energies, which correspond to two different tube voltages (80 and 140 kV). In other words, X-ray absorption is energy-dependent, e.g. scanning an object with 80 kV results in a different attenuation than scanning it with 140 kV. This physics phenomenon can help to discriminate between materials that have different atomic numbers but the same attenuation at a certain energy level. Colors can then be assigned according to changes in HU between the two energy settings, and the resulting color-mapped, dual energy image can differentiate between calcifications and iodine contrast. This technique can also be used to better visualize postmortem blood clots in vessels, and possibly bleeding in soft tissue. The material-specific difference in attenuation shown in the resulting image could facilitate classifications of different tissue types such as blood, soft tissue, tendons, and cartilage (Figs. 4 and 5).
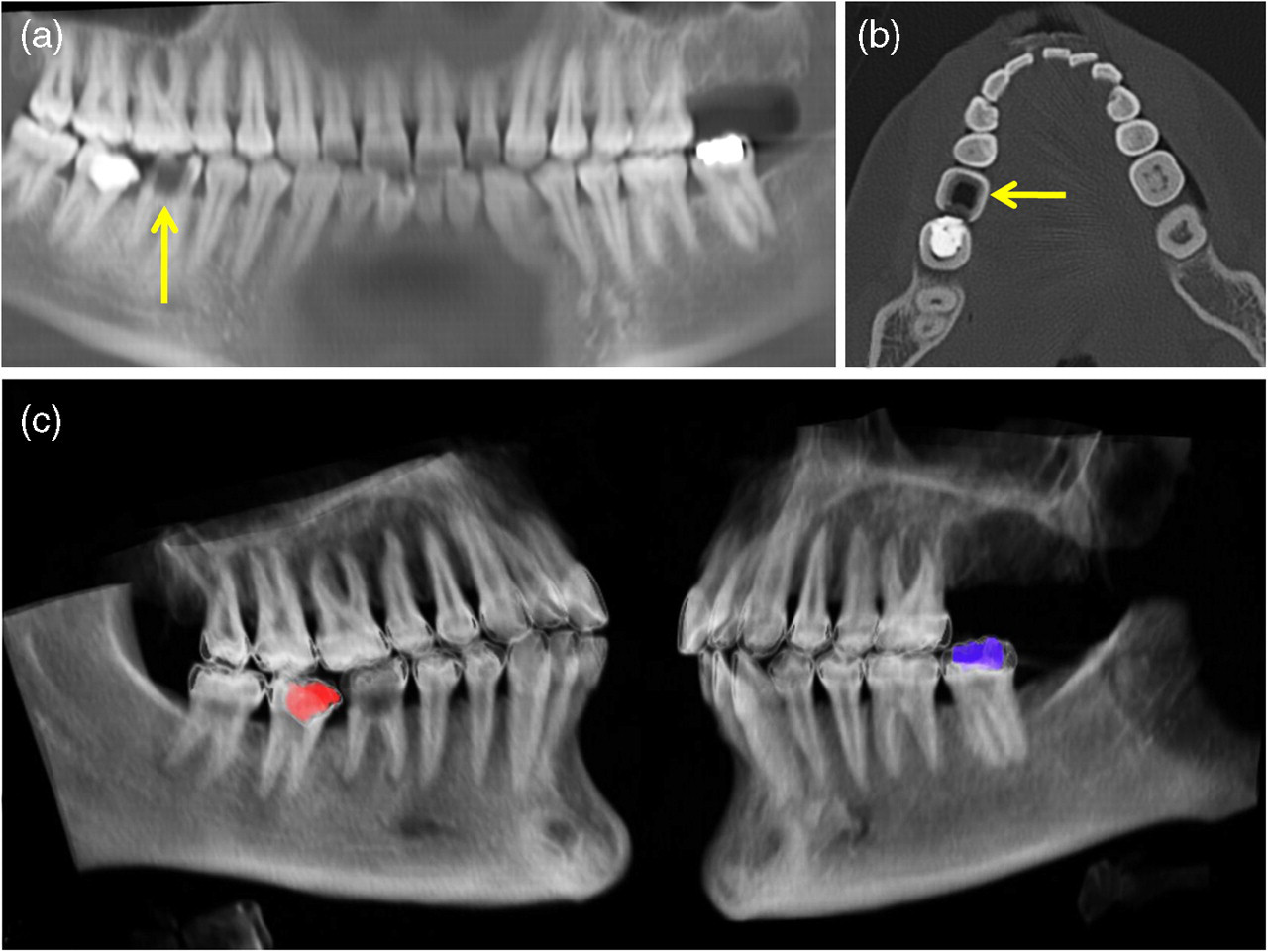
Dental documentation by ultra-high resolution extended scale CT. (a) Panoramic reconstruction gives an overview and provides hints for three fillings, two highly opaque on 37 and 47 and one low opacity filling (arrow) on 46. (b) Axial reconstruction at the level of both right lower jaw fillings shows the typical appearance of a ceramic filling on 46 (arrow). (c) Color encoding based on a published VR preset allows also differentiating the two highly opaque fillings (18). The right lower jaw one on 47 has to be a composite filling as always displayed in red whereas the left lower jaw filling on 37 has to be an amalgam filling as given in blue
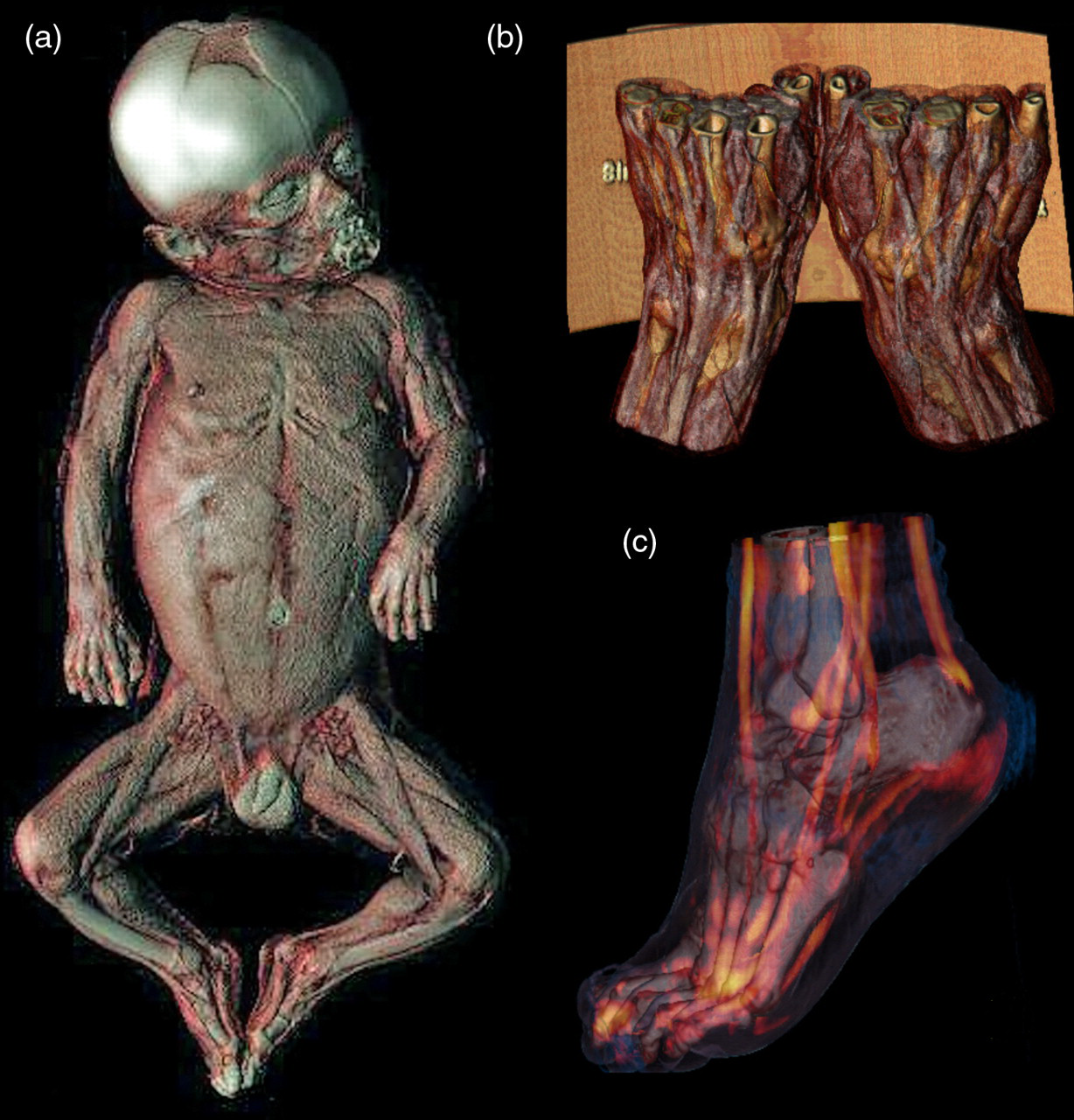
Enhanced soft tissue visualization by dual energy CT. (a) Note the brilliant three-dimensional musculature and lymph node visualization in an infant. (b) Tendons examined with DECT. Tendons and small vessels can be visualized without contrast agent administration. Ligaments between the carpal bones are also visualized. (c) Tendons in the foot examined with DECT
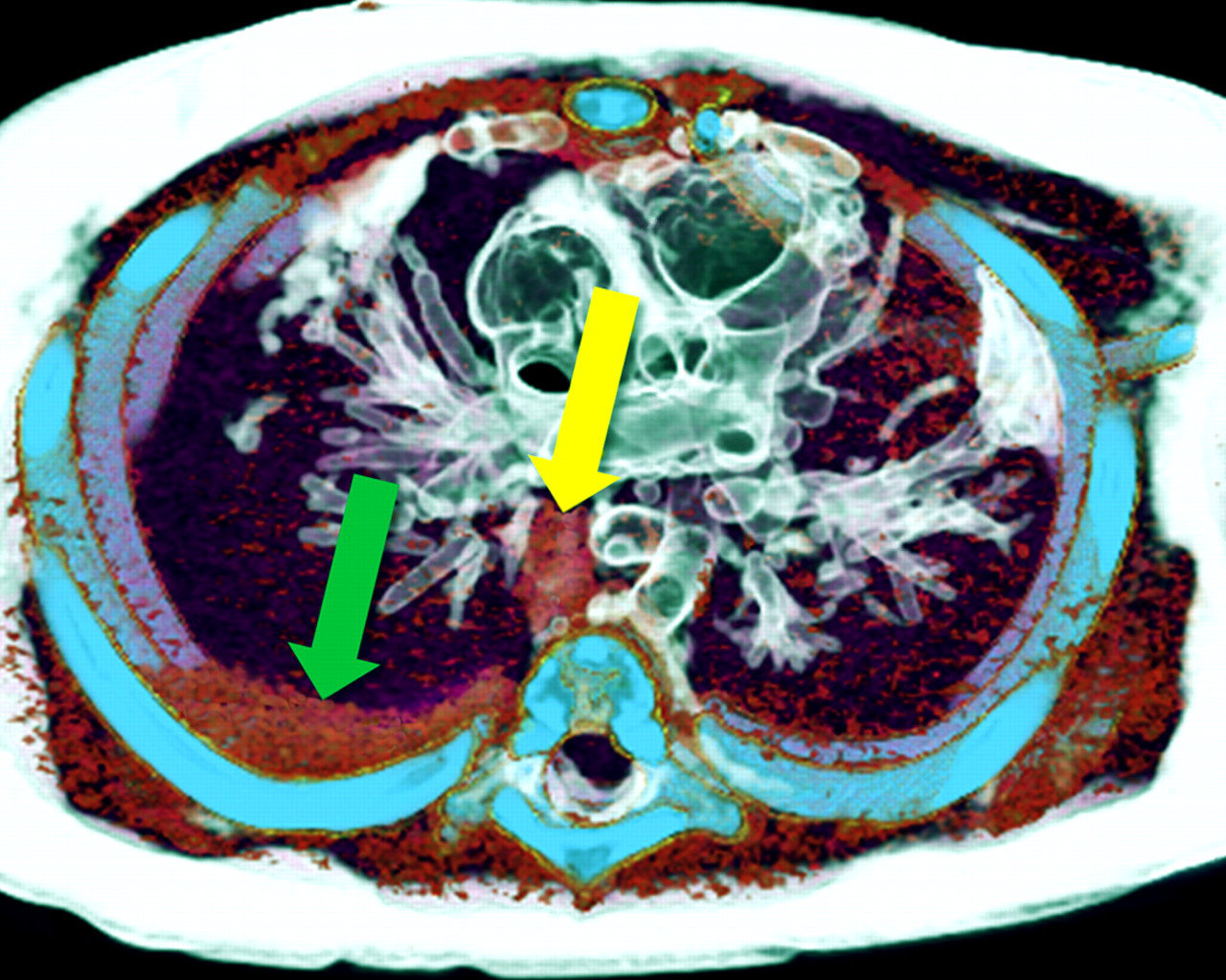
Dual energy CT of a small infant. Child abuse case with severe blunt trauma against the thorax region. Blood to the right of the aorta (yellow arrow) and in the right pleural cavity (green arrow)
The absence of any motion-related artifacts in combination with unlimited radiation exposure possibilities allows the acquisition of highly optimized data for DVR to display forensic finding in 3D. MDCT has been proven to be especially valuable in cases that present with forensically relevant findings in terms of skeletal alterations (Figs. 6 and 7) (20, 21), foreign materials (Figs. 8–10) (7, 22–24), gaseous findings (Fig. 11) (6, 25, 26), and postmortem CT angiography (Fig. 12) (27).

DVR visualization of findings in a gunshot to the head in an infant. (a) Note the bony entrance defect on the forehead and a fracture line combining entrance and exit defect on the skull. The projectile remained within the subcutis. (b) DVR in soft tissue settings allows for a depiction of the gun shot channel through the brain and the intra-cerebral hemorrhage. Note also lead deposits (blue) and bone fragments (beige) along the wound channel
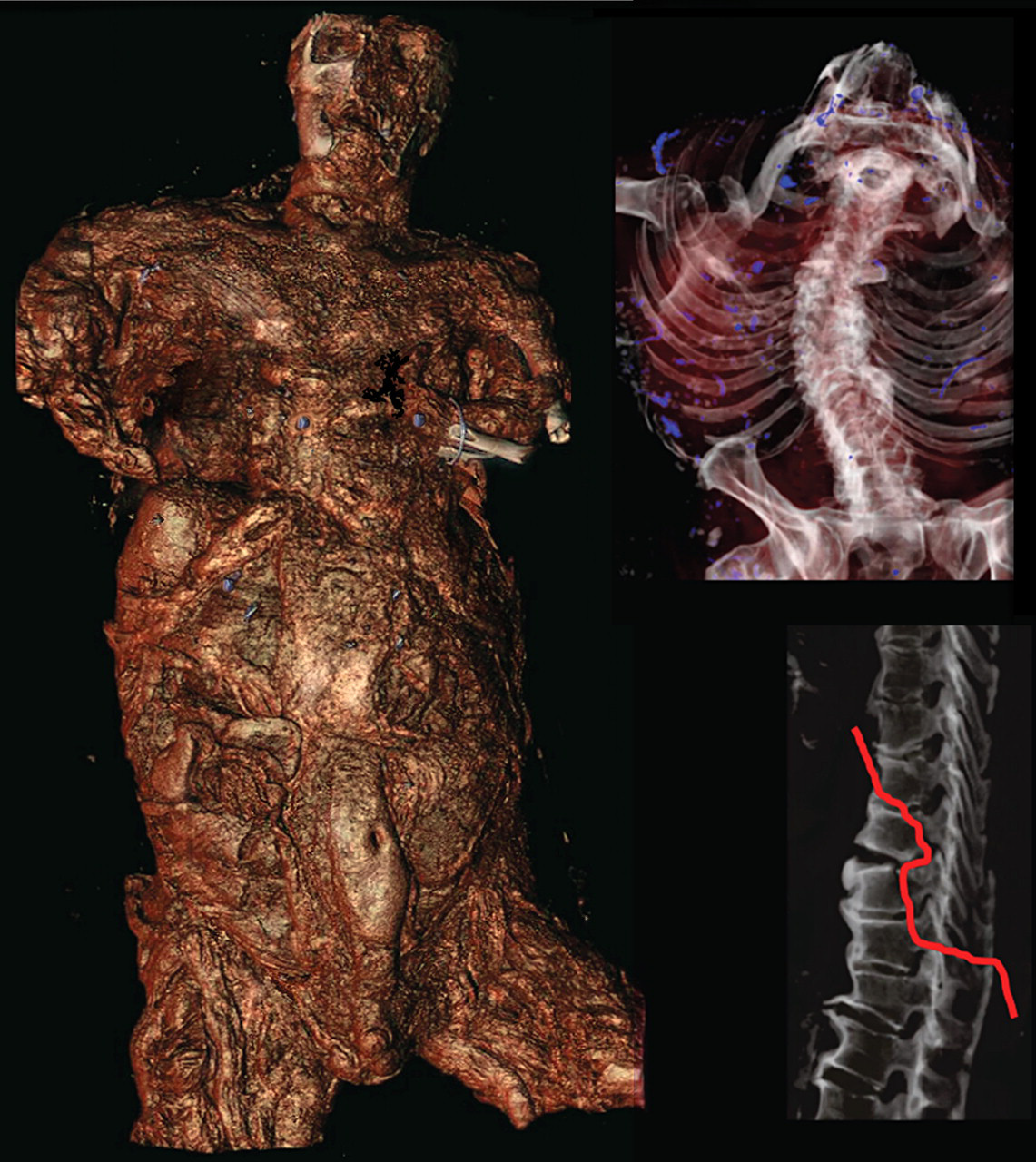
DVR in a burned corpse. Before the CT examination there was no suspicion of murder. Several fractures (red line in the right lover image) that could not be explained pointed the investigators in the right direction and after forensic and police investigation the case finally turned out to be a homicide
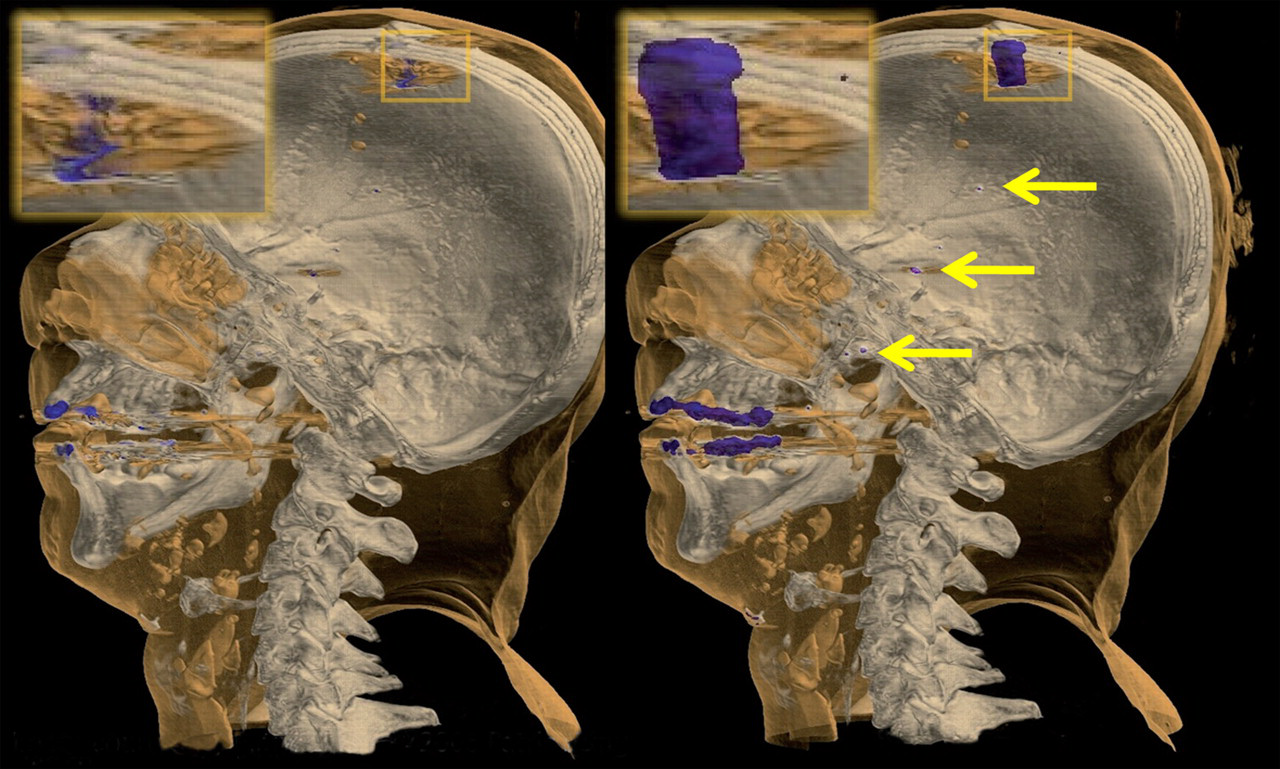
Foreign body visualization by DVR. A case of a gunshot wound to the head. A metal artifact reduction algorithm was used that specifically reduces artifacts from lead bullets in CT data-sets (24). Small lead fragments along the gun shot channel are made visible by enlarging their size in the image (arrows). This will together with other software tools be implemented in a newly developed radiological workstation that specifically addresses the forensic needs of visualization. Image courtesy of Patric Ljung
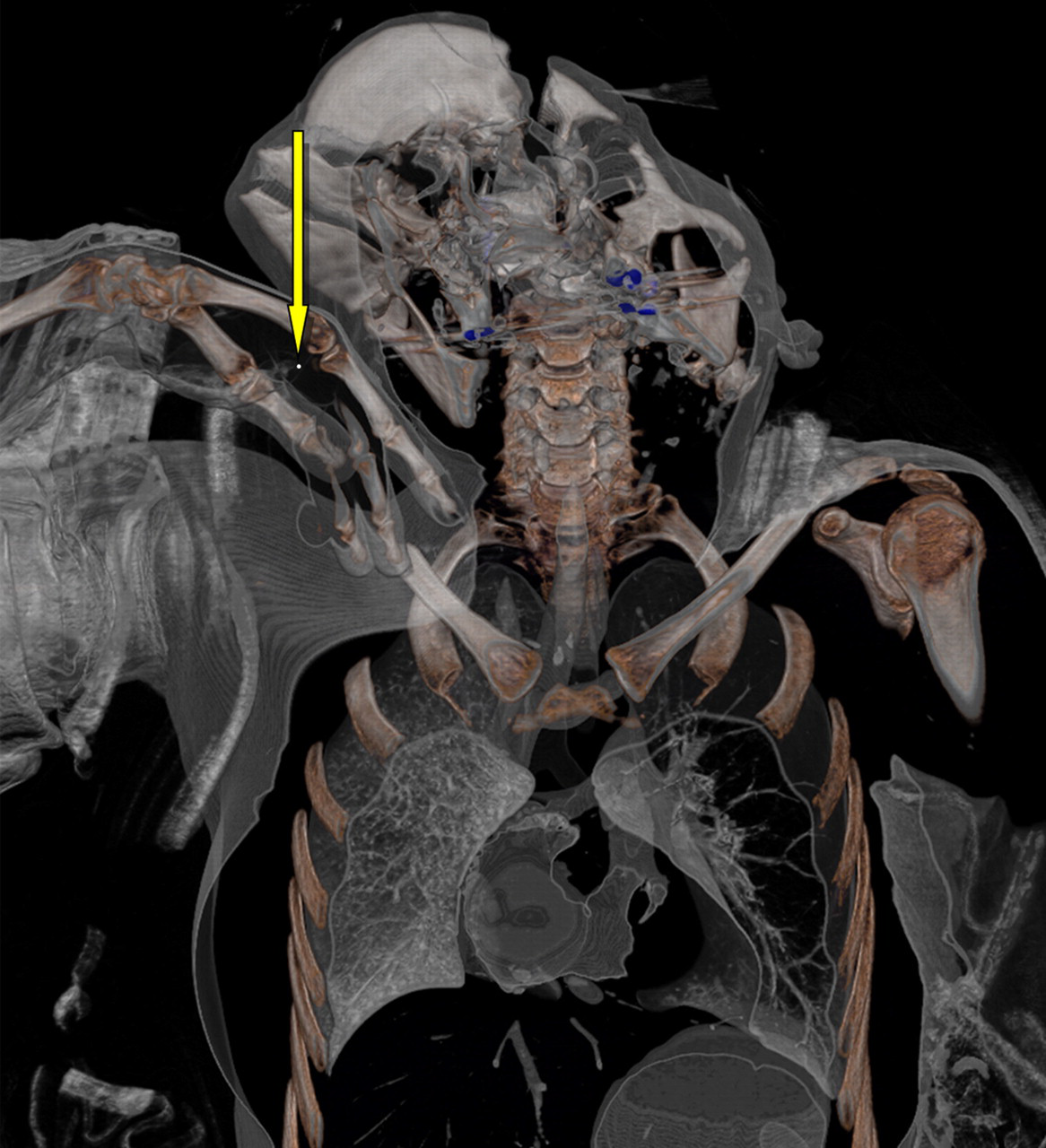
Foreign body visualization of a 10-centimeter thick volume rendering slab in the coronal plane. A case of gunshot wound to the head with massive destruction of the skull and soft tissues. In this case localization of 1 mm lead bullet fragment (yellow arrow) could easily be visualized with postmortem CT. At conventional autopsy these fragments as main forensic evidence are hard or even impossible to find in such zone of destruction. The second forensically important finding displayed is massive right atrial, right ventricular, and pulmonary artery gas embolism

Foreign body visualization by DVR. Localization of a knife together with self-inflicted cuts on the cervical neck region that could also be visualized pointed into the right direction – suicide. These findings can be presented to the jury in the court in a bloodless manner

DVR visualization in a case of lethal air embolism in an infant. Coronal volume rendering slabs reveal air filled cervical veins, superior cava vein, hepatic veins as well as air in all heart chambers and the aorta including aortic branches
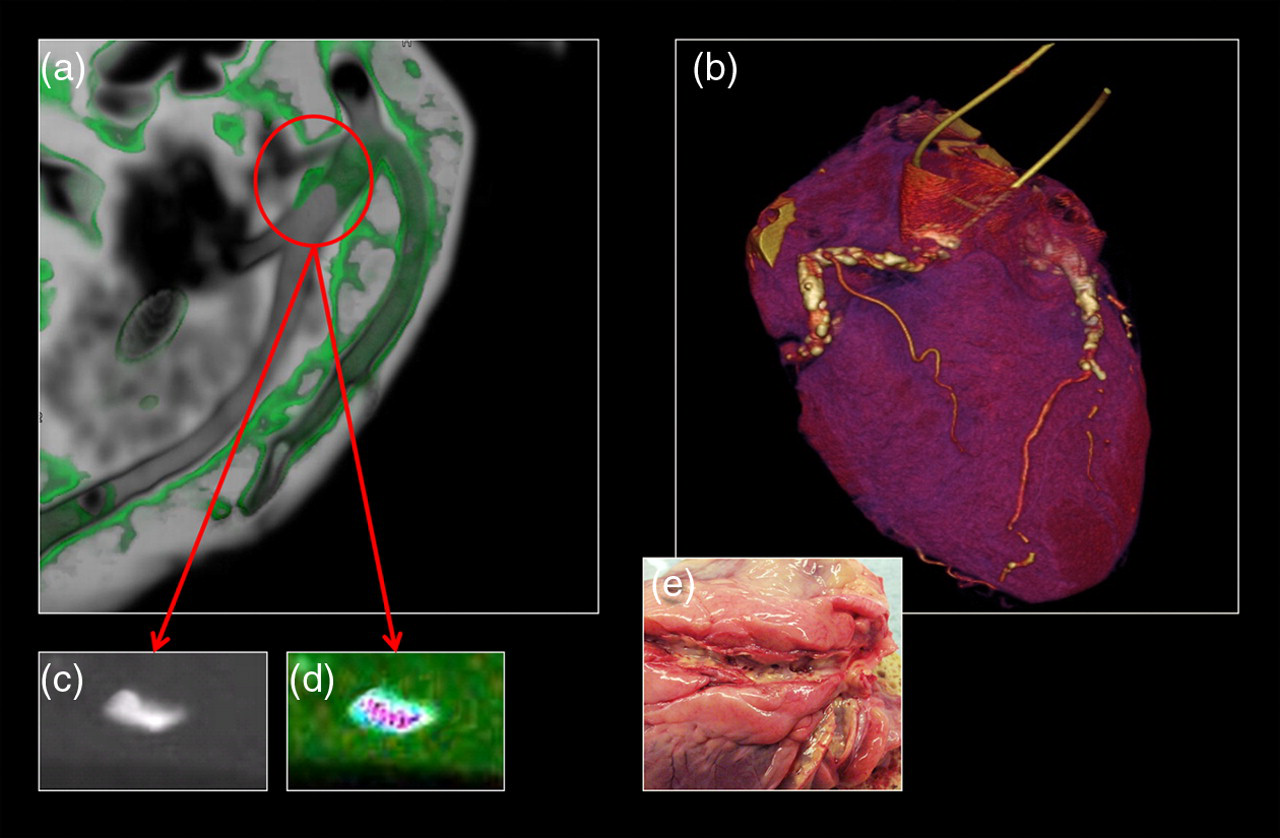
Postmortem CT angiography can give valuable additional information. Dual energy CT postmortem heart examination. In each coronary artery catheters have been introduced and diluted iodine contrast has been injected. (a) Left image showing single-energy multiplanar rendering. A plaque in the vessel wall can be seen (red ring). (b) DVR image of the heart. Coronary calcifications in the vessel wall are depicted white. (c) With only one energy level it is not possible to visualize several plaque components. (d) With multi-energy imaging (80, 100, 120 and 140 kV) several plaque components can be seen. (e) Autopsy depicts several ulcerations in the vascular wall
PmMRI
In selected cases, an MRI examination is also performed (1.5T scanner, Achieva; Philips Medical Systems, Best, Netherlands). Whole body scans were acquired in T1 (TR 450 ms; TE 18 ms) and T2 (TR 1200 ms; TE 80 ms) using the built-in volume coil (Q-body). Slice thickness for T1, 6 mm, gap 1 mm, resolution 1 × 1 mm and for T2, 7 mm, gap 1 mm, resolution 1.2 × 1.2 mm. Thereby, the soft tissue injury distribution pattern is documented in real dimensions and can be used for forensic reconstructions comparable to skeletal DVR reconstruction based on CT data (Fig. 13).
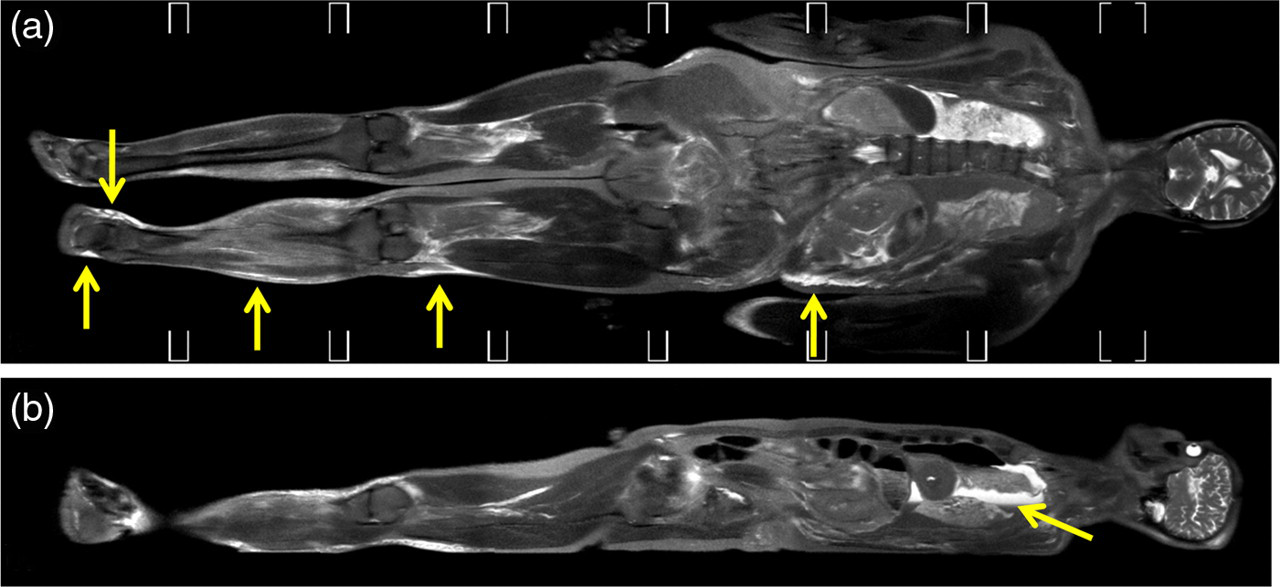
Whole body MR imaging in a fatal traffic accident (pedestrian). (a) Coronal T2-weighted image showing the left sided soft tissue hemorrhage distribution due to direct impact and also fracture hematoma (arrows). (b) Sagital T2-weighted image depicts a hematopneumothorax as the cause of death (arrow)
All children are routinely examined with MRI, because it offers superior visualization of the brain and malformations compared to DSCT (Fig. 14).
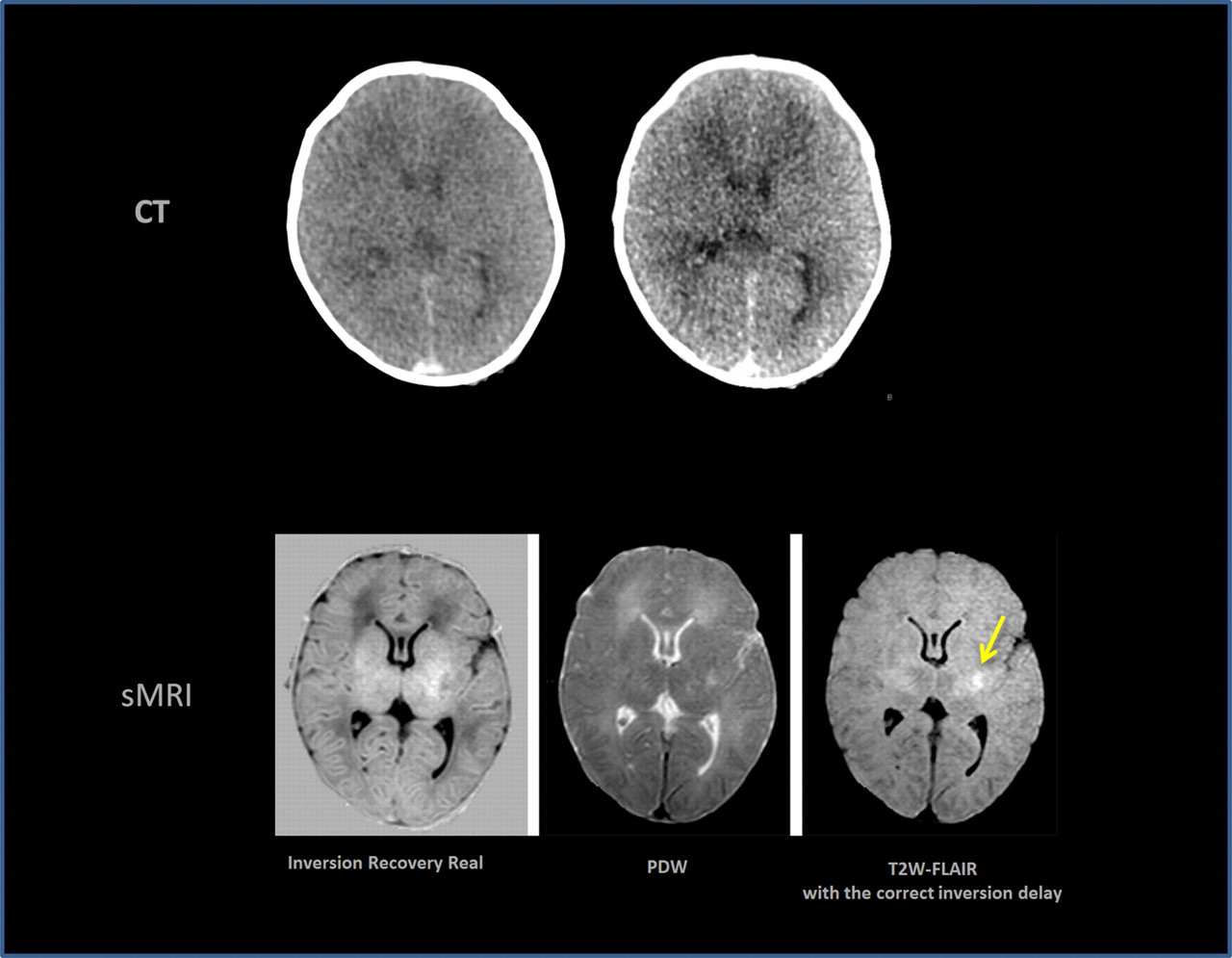
PmMRI in an infant compared to CT. CT and synthetic MRI of an infant's brain. The hemorrhage within the left sided putamen is not visible in the CT images but is clearly depicted in the MRI image (arrow)
In cases of suspected natural death also the heart is specifically examined using a SENSE cardiac or a SENSE torso coil. Short-axis images are acquired using conventional clinically used localizer settings (28) in T1 (TR 650 ms; TE 15 ms), 2 × T2 (TR 4000 ms; TE 70 ms and TR 4000 ms; TE 100 ms) and proton density (TR 4000 ms; TE 10 ms) weighting. Slice thickness 4 mm, resolution 0.7 × 0.7 mm (Fig. 15) (9, 29).
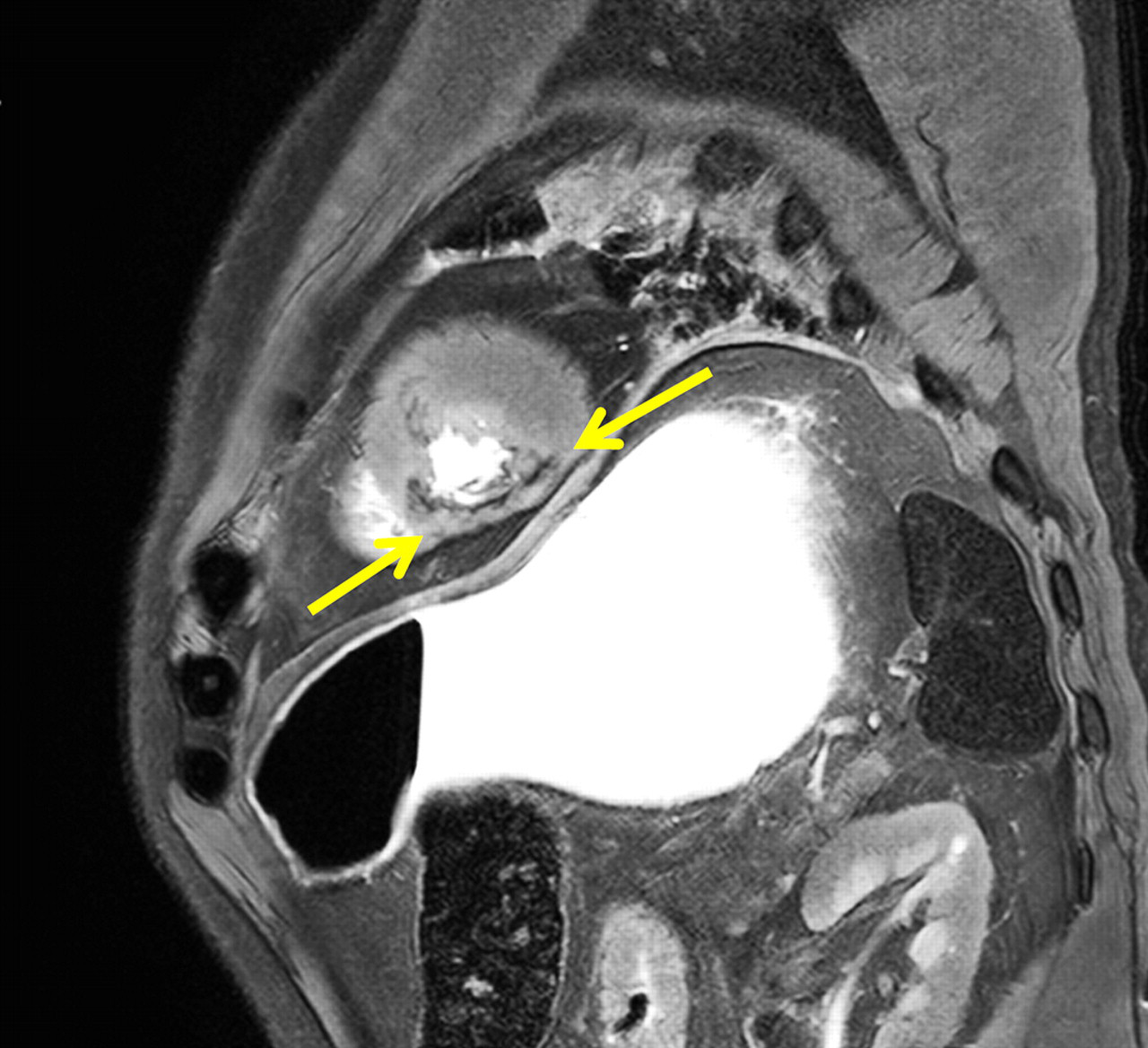
Postmortem cardiac MR imaging in a case of myocardial infarction. T2-weighted short axis image demonstrates a chronic infarction within the inferior wall and the posterior septum (arrows). Note the shrinking of the inferior wall as well as the corresponding concentric hypertrophy of the anterior and lateral wall
As a groundbreaking new approach the so-called IQpmMR (isotropic quantified postmortem magnetic resonance) data acquisition was implemented (30). IQpmMR enables sophisticated 3D postprocessing such as re-formatting and volume rendering. The body tissues can be characterized by the combination of the three quantified values of T1 relaxation time, T2 relaxation time and proton density. The values of T1, T2 and PD can be given as coordinates in a T1-T2-PD space where similar tissue voxels form clusters. Implementing in a volume rendering software enables color encoding of specific tissues and pathologies in 3D models of the corpse similar to CT, but with distinctively more powerful soft tissue discrimination (Fig. 16). From IQpmMR data any image plane at any contrast weighting may be calculated or 3D color-encoded volume rendering may be carried out.
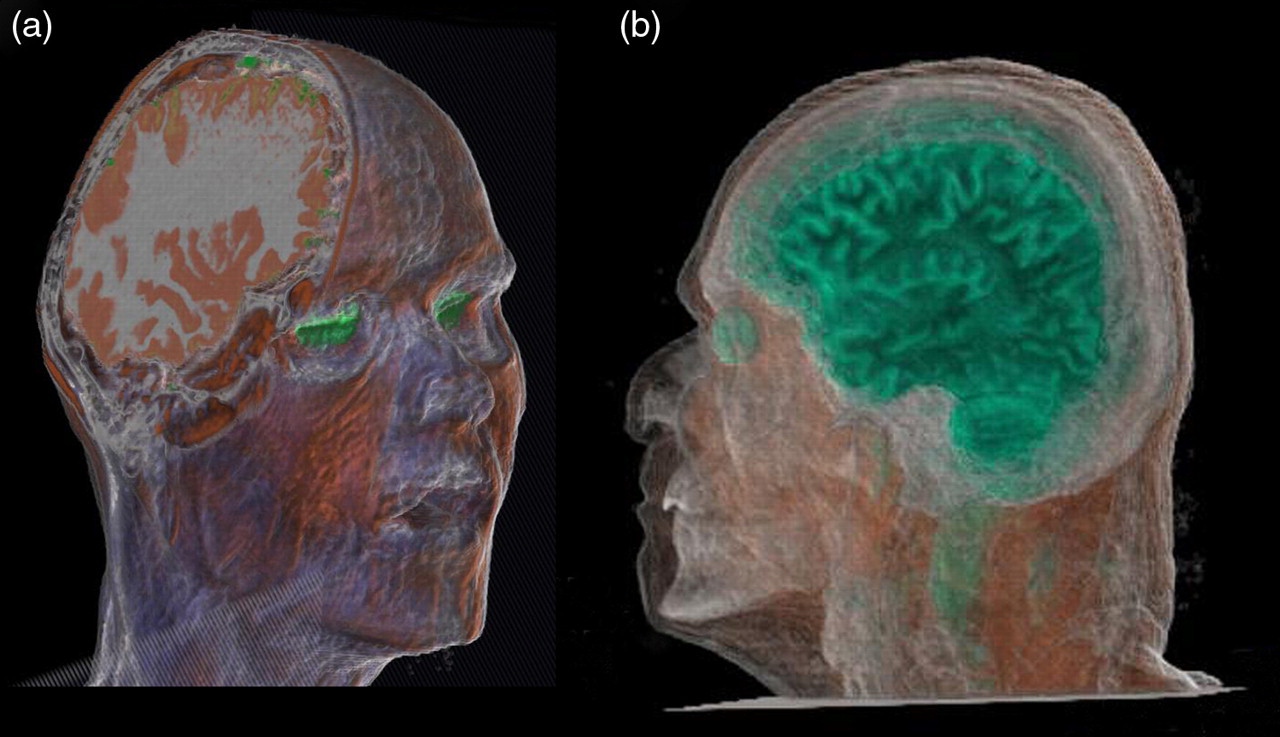
Visualization of isotropic quantified postmortem MR data (IQpmMR) by DVR techniques to selectively demonstrate cerebral structures. (a) The entire cranial volume is represented including the skull, which became astonishingly possible in MRI by the use of IQpmMR. (b) Another data-set but with more translucent rendering
Preliminary results indicate that this new approach will enable future computer aided diagnosis that for example checks corpses for a hemorrhage distribution based on the knowledge of its T1-T2-PD vector behavior in a high spatial resolution (Fig. 17).
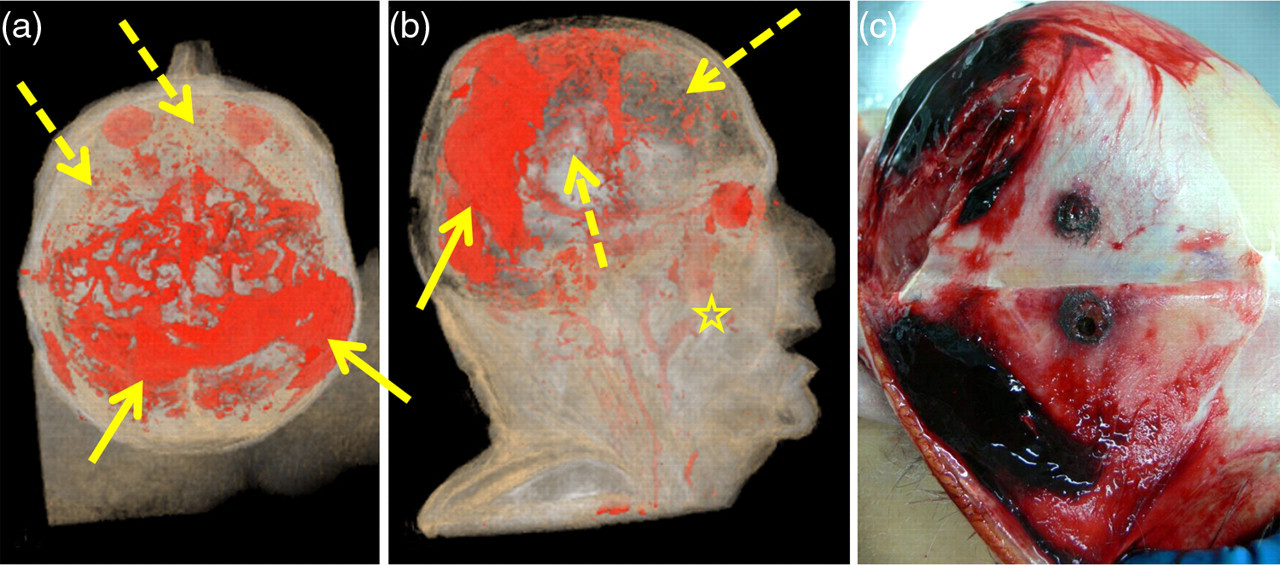
Use of IQpmMR data for DVR techniques to selectively demonstrate the hemorrhage distribution in a gunshot case. (a) Craniocaudal and (b) right lateral view on a IQpmMR based rendered 3D model selectively depicting extra vascular blood accumulations. Note distended subcutaneous fracture hematoma (arrows), subarachnoidal bleedings (dashed arrows) and also blood accumulation in the sinus and pharynx (asterisk). Note also the overlapping signal behavior of vitreous fluid as also given red although other tissues were intended to have low opaque visualization. (c) Autopsy appearance of the large subcutaneous hematoma well correlating to (a) and (b)
For both MDCT and MRI the cadaver remained in the body bag throughout the entire pm imaging procedure to ensure the security of forensic evidence, such as fibers and body fluids, and of course to avoid contamination of the radiological equipment.
Visualization – image analysis
In preparation for the physical autopsy, the forensic pathologist and the radiologist conduct a collaborative MPR and DVR session. They can obtain a clear survey of the entire body quickly, and localize fractures and air pockets. The full-body procedure permits fast localization of foreign objects such as metal fragments or bullets. Another important aspect is the high resolution of the data, which, in a seamless visualization, allows details such as dental information to be extracted for identification purposes (Fig. 3). After scanning, the body is moved to the forensic department for conventional autopsy. A personal computer connected to a beamer system is installed within the autopsy room and allows visualizing the pmi scanning data during autopsy (Fig. 18). In periodical consensus sessions the past cases are discussed and the forensic personnel informs about the autopsy results and possible discrepancies to pm imaging. To further strengthen the collaboration and information exchange between different personnel groups a new visualization tool has been developed at CMIV, the ‘Visualization table’. Multiple users can interact collaboratively and simultaneously, working with large and complex data to gain deeper understanding and insight into the functions and processes inside the body (Fig. 19).

A personal computer connected to a beamer system is installed within the autopsy room and allows visualizing the PMI data during autopsy. Police and CSI personnel attending the autopsy is then presented the pmi results parallel to the autopsy and questions can be addressed from autopsy to PMI data and vice versa. And if more specific radiological information is needed later, new contact to the radiologists is made. In periodical consensus sessions the past cases are discussed and the forensic personnel informs about the autopsy results and possible discrepancies to PMI

The Visualization Table is a unique new medical visualization tool that allows people to explore the inside of a human body. Except for the added value in the autopsy room it is also a powerful tool for educational purposes and science communications, suitable for a wide range of environments such as schools, universities, museums, and Science and Technology centers
Guide and checklist for working with PMI data of forensic cases
General thoughts
Forensic examinations of bodies are mainly performed to address five major demands, which should be always kept in mind when trying to gather information from MDCT or MRI data-sets for forensic purposes (of course, there are always exceptions!). Although each case can individually be very different and challenging the following five general goals should be addressed:
What is the atrium mortis (cause of death leading to the manner of death)? Are there relevant forensic traumatic or pathologic findings on the skeleton and soft tissues (see the following case groups)? Are vital reactions present, which can prove that the victim was still alive when the incident occurred (circulatory, gastrointestinal and respiratory system or consciousness?) How is the potential for forensic reconstruction of the event based on the findings? How is the potential for a visualization of the findings using DVR at the court room?
Tables 1–8 give advice from the viewpoint of forensic needs based on the recently published literature. It cannot be all-embracing for every single case, but can give ideas about what to look for. Moreover, any finding that can somehow be related to the mentioned five points but is not noted here might be important and should individually be discussed.
Identification clear? If not, check for the following
Severe blunt trauma (falls from great height, pedestrians in traffic accidents, etc.)
Sharp forces. Check the data for
Children – suspicion of shaken baby syndrome or sudden infant death syndrome
Advantages and disadvantages of postmortem imaging
In a comparison of both techniques there are several points to be discussed. Table 9 gives an overview on the main advantages and disadvantages of PMI compared to a traditional autopsy.
Postmortem imaging by pmCT and pmMRI
Although it is an additional effort it may help to save time in complicated cases. PMI can be a complement to standard autopsies, enabling broad, systematic examinations of the whole body that are normally difficult and time consuming at autopsy, for example, an examination of the entire skeleton or searching for the presence of air in the body (Figs. 7 and 11).
It is non-invasive. Once an invasive traditional autopsy has taken place, the body cannot be reassembled in its original state, thus precluding other forensic pathologists from conducting a fresh analysis on the same body. Using whole-body PMI data-sets a virtual dissection can be performed numerous times by numerous experts.
A traditional autopsy may be rejected by family members, perhaps due to religious beliefs that prohibit the desecration of the remains of a deceased person. For example, Orthodox Judaism prohibits disturbing dead bodies except when such action may save others, and decrees that practices such as organ removal should be avoided. Islam is likewise opposed to desecrating or even exposing the body of a deceased believer.
Autopsy protocols and photographs used as evidence in criminal cases can be difficult for jurors to understand. On one hand it is specific medical information that is to be understood by medical laymen and the information comes hidden in bloody pictures. PMI visualizations instead are typically clearer focused on the specific finding and probably more important, they are bloodless (Fig. 6).
Although the storage of PMI data poses a few problems in terms of size of the data, tissue specimens obtained at autopsy are more difficult to store indefinitely because the body has to be re-assembled when leaving the forensic institute.
With potential global pandemics such as bird flu (avian influenza A) and swine flu (the H5N1 virus) posing an increasing threat, the practice of eviscerating the victims can pose serious health risks to coroners, pathologists, and medical examiners. Using PMI, these risks are minimized.
Shortcomings
In MDCT the soft tissue discrimination is low. Energy-resolved CT (DECT) has the potential to resolve this problem (Figs. 4 and 5) to certain extend. However, the soft tissue discrimination potential of the human eye in combination with the sense of touch of an experienced forensic examiner will never be reached by CT.
The huge amount of data resulting from the high resolution whole body scans is a problem to analyze. But better and faster postprocessing programs have to solve this. This is especially the aim of CMIV's research efforts. The possibility of handling large slice stacks in DVR is a prerequisite of a successful implementation of PMI in a forensic environment as postmortem scans are not limited to a certain body region, e.g. in a traffic accident it is the entire injury distribution of the victim from head to toe that needs to be documented and visualized in 3D (Fig. 13).
Whole-body MRI is still a time-consuming investigation and today's clinically optimized sequences do not perform well on cold bodies. Synthetic MRI is a promising development as it solves several problems simultaneously. Once having a whole body IQpmMR data-set acquired on the MR scanner all possible non-contrast agent enhanced sequences may be synthetically calculated in all possible plane directions (30). That allows optimizing the image contrast in terms of adaptation to the individual core temperature at time of data acquisition. Although the initial IQpmMR sequence will take 2–3 times as long as a usual mean clinical sequence would be the overall time saving is distinctive and the examination possibilities after the actual data acquisition become almost endless.
Postmortem imaging with MDCT and MRI did not give any color documentation of the body. By implementing a colored DVR technique based on the IQpmMR data this shortage will be addressed (Fig. 17).
The absence of micro morphology (histology and chemistry) may be addressed by implementing an image-guided biopsy procedure to obtain necessary tissue specimen and body fluids (43, 44).
Postmortem gas formation in its beginning stages can be difficult to distinguish from other types of gas (bowel gas, gas in wound channels, etc.). Therefore, it is important to execute the postmortem imaging examination soon after death has occurred.
Conclusions
The Center for Medical Image Science and Visualization (CMIV) at Linköping University Hospital in Sweden, in collaboration with the Swedish National Board of Forensic Medicine, has developed a procedure for virtual autopsy that is now routinely used for forensic work since 2003. This method has been applied to over 300 cases so far, mostly homicides. The procedure is based on a continuous interaction between the forensic pathologist, the radiologist, and the police. For acquisitions of data at CMIV new promising tools have been used such as dual energy CT and IQpmMR (isotropic quantified postmortem magnetic resonance). The overall goal of the VA procedure is that it can be applied to every victim of any kind of incident as an add-on to conventional autopsy in the forensic setting and that it can serve as an alternative postmortem examination technique in non-forensic clinical pathology, a discipline that severely suffers from declining autopsy rates since decades now. This goal is, however, far from reached and several challenges remain to be addressed before the full envisioned potential of the VA could be realized.
Footnotes
ACKNOWLEDGEMENTS
The authors would like to express their gratitude to Lotta Nordén-Pettersson (Department for Forensic Medicine, RMV, Linköping) for the reliable support in case management as well as to Elisabeth Wålin, Peggy Florhed-Hermansson, Ann-Charlotte Skiölt, and Nobar Ashjian (Department for Forensic Medicine, RMV, Linköping) for their experienced assistance at autopsy and their support in logistic aspects of the study. Furthermore, we would like to thank the team of forensic examiners around Johan Berge, MD, at the Department for Forensic Medicine in Linköping for varying contributions that not least enabled the collaboration, and Professor Anders Unnerman and his colleagues for successful research regarding data management and visualization research (Division for Visual Information Technology and applications, Linköping University). We are also grateful to Petter Quick, Annika Hall and Johan Kihlberg (CMIV) who performed the data acquisitions mostly at flexible time band. This study was supported by grants from the national scientific visualization program in Sweden.