
Abstract
There is a wide spectrum of benign, non-cystic scrotal lesions that show characteristic histo-morphology and natural history. While sonography is the preferred modality for the diagnosis of both testicular and extratesticular masses, MRI is used as a problem-solving modality when sonographic findings are inconclusive. This article reviews the cross-sectional imaging features of benign, non-cystic, intra- and extratesticular lesions. Definitive diagnosis of benign scrotal lesions may lead to conservative management including testicular preserving surgery.
Testicular cancer is a common malignancy in young men, accounting for 1% of all cancers in men. It is a widely accepted urologic dictum that all solid intratesticular masses should be considered malignant and resected. However, recent literature indicates a high incidence of benign intratesticular lesions than previously reported (1). Extratesticular lesions commonly show benign behavior; distinction of testicular from extratesticular masses by imaging is thus considered important. Ultrasonography is usually the initial imaging modality used for the evaluation of scrotal masses. Grey-scale sonography in conjunction with Doppler studies may provide a specific diagnosis for most scrotal masses thus guiding further management. MR imaging is commonly used as a problem solving tool when sonographic findings are inconclusive. Identification of benign lesions is important as it can lead to non-surgical management or testicular-preserving surgery. It has been estimated that when indicated, MR imaging can reduce treatment costs by reducing unnecessary surgical procedures (2). In this review, imaging findings of a wide variety of benign, non-cystic, scrotal lesions (both intra and extratesticular masses) are presented along with an imaging pattern based algorithm (Table 1).
Classification of benign, non-cystic, scrotal masses
Intratesticular masses
Soft tissue masses
Leydig cell hyperplasia
Leydig cell hyperplasia is a rare condition that is characterized by bilateral, multifocal proliferation of the androgen-synthesizing interstitial cells of Leydig (3). Leydig cell hyperplasia is thought to occur due to a faulty hypothalamic-pitutary–testicular axis with resultant chronic Leydig cell stimulation (4, 5). In its primary form affecting boys, it is usually symptomatic and the patients usually present with precocious puberty (4). The primary form results from either a familial activating mutation of the luteinizing hormone receptor or congenital placental human chorionic gonadotropin (hCG) stimulation of the testes (6). hCG is structurally similar to luteinizing hormone and thus may also cause Leydig cell hyperplasia (4, 7). Secondary Leydig cell hyperplasia which affects adult patients is usually asymptomatic (7). This usually results from supra-physiological hormonal stimulation of the testes (8). Secondary causes of Leydig cell hyperplasia include cryptorchidism, congenital adrenal hyperplasia, hCG production by germ cell tumors or choriocarcinoma, pituitary abnormalities, Klinefelter's syndrome, exogenous hCG therapy, and antiandrogen therapy for prostate cancer (4).
Histologically, Leydig cell hyperplasia is characterized by an increased number of testicular Leydig cells (4) which insinuate between the seminiferous tubules (Fig. 1). This is in contrast to Leydig cell tumors that displace and compress the seminiferous tubules. Cells are usually arranged in multifocal nodules which often occur bilaterally and range in size from 1 to 6 mm (4). Leydig cell hyperplasia is not known to be a pre-neoplastic lesion (4).
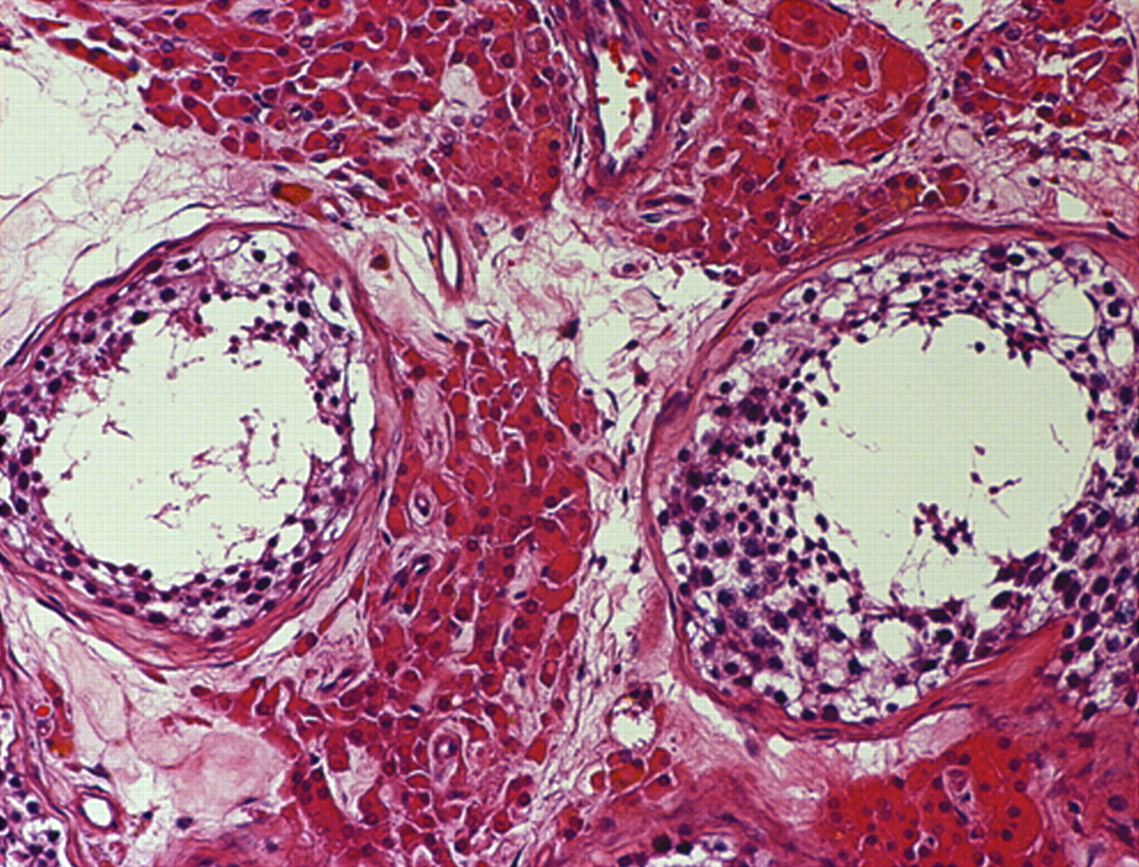
Photomicrograph of section of testicle reveals increased number of Leydig's cells in interstitium between normal seminiferous tubules
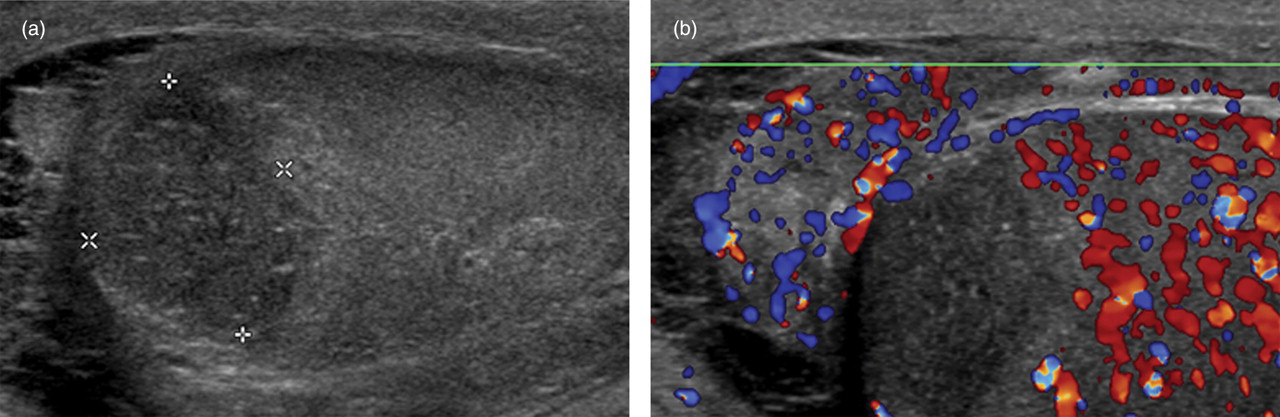
On sonography, Leydig cell hyperplasia commonly appears as multiple, usually bilateral hypoechoic nodules within the testicular parenchyma (Fig. 2a). Rarely a hyperechoic appearance has been described (8). The vascularity within the nodules is variable but usually increased (Fig. 2b). Few reports have described the MR imaging findings, which include multiple, bilateral solid lesions that are hypointense on T2-weighted images relative to normal testicular parenchyma, display contrast enhancement, and range in size from 1 to 6 mm. The nodules usually demonstrate avid contrast enhancement (more than the normal testis) (9). MRI can help by demonstrating the presence of bilateral and multifocal lesions (9).
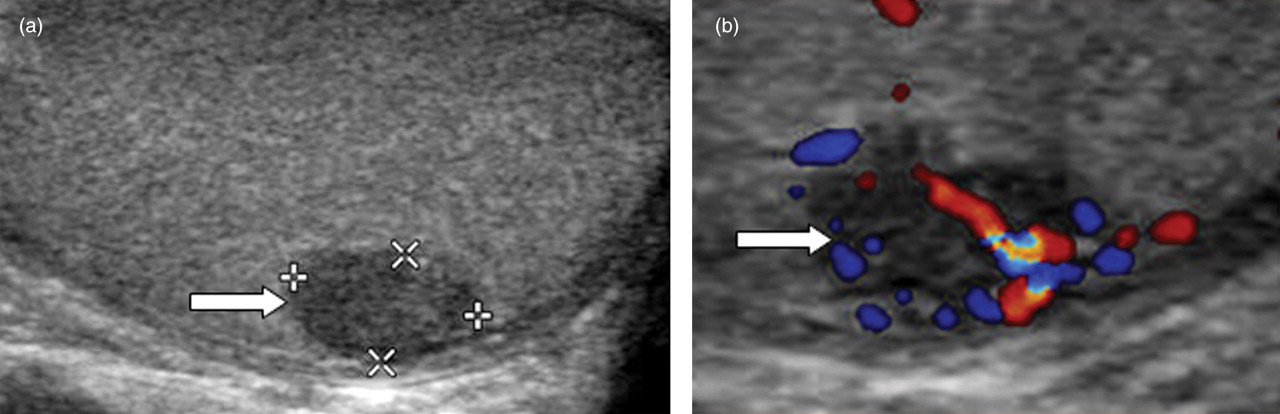
(a) 45-year-old man with incidental finding on sonography. Grey-scale sonographic image shows a small homogenous hypoechoic lesion in the periphery of the testicle (arrow); (b) Color Doppler sonographic evaluation shows increased vascularity within the lesion (arrow). The patient underwent inguinal orchiectomy for suspicion of tumor and final pathology showed benign leydig cell hyperplasia
Testicular adrenal rests
Testicular adrenal rests are benign corticotropin-dependent lesions that are often asymptomatic and occur frequently in male patients with congenital adrenal hyperplasia (CAH) but have also been described in patients with Cushing's syndrome and Addison's disease. Detailed microscopic examination suggests that adrenal rests are present in all male patients with CAH (10). The reported prevalence by ultrasonography, however, varies between 24% and 94%. Histologically, testicular adrenal rests consist of hyperplastic adrenal cortical tissue originating from aberrant adrenal tissue that descends with the gonads during embryonic migration (11).
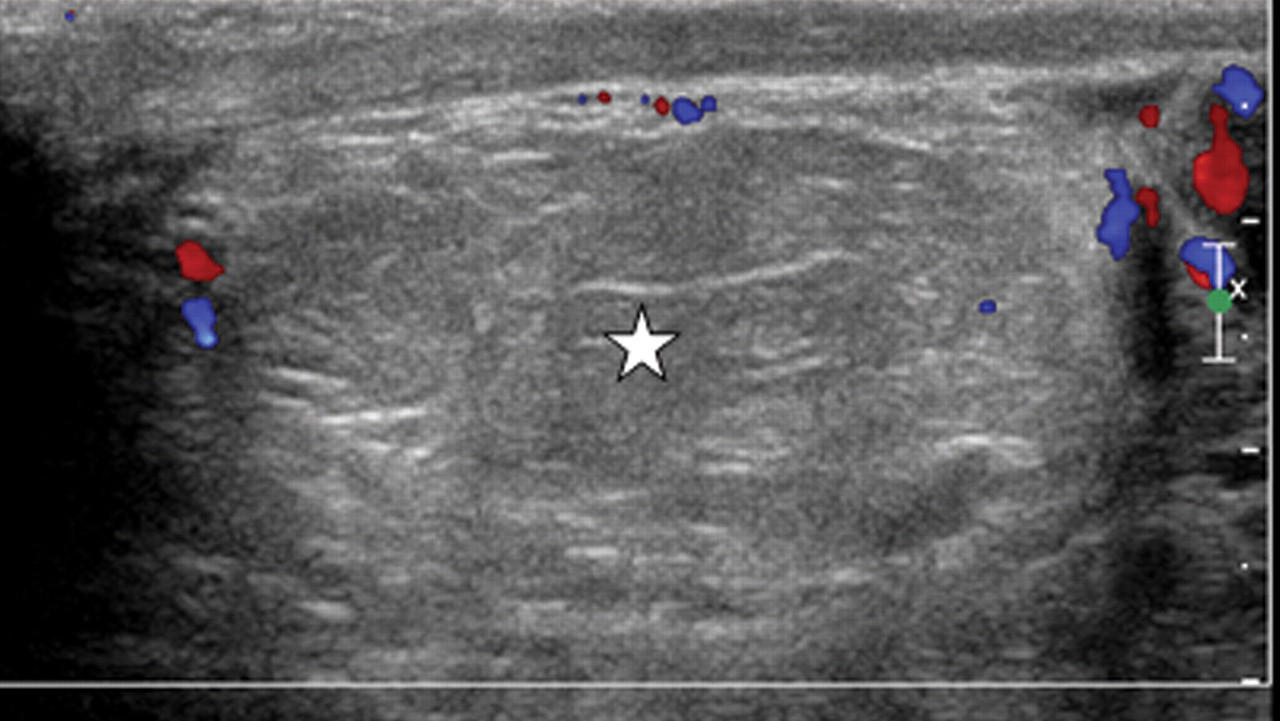
On ultrasonography, the testicular adrenal rests mostly appear hypoechoic although they may be heterogeneous or hyperechoic (Fig. 3a) (11–13). The adrenal rests are usually bilateral. The heterogeneous nodules may show calcification, a hyperechoic rim, or internal spoke-like echogenicity from vessels (10). The nodules may be associated with acoustic shadowing secondary to extensive fibrosis (10, 13). Most adrenal rests are located adjacent to the mediastinum of the testis, particularly in CAH patients (10). Color Doppler ultrasonography may show variable vascularity within these rests, however, it is usually increased (Fig. 3b) (10). A spoke-like appearance with multiple vessels radiating from the perimeter to the center of the mass has also been reported. Differentiating testicular adrenal tumors from other testicular tumors is important. Bilateral synchronous testicular tumors are rare with a prevalence of 1%, thus presence of bilateral lesions should prompt the diagnosis of adrenal rests. An important finding in adrenal rests is that vessels coursing through the lesion are not deviated and this is considered an important feature. MRI usually shows the nodules to be isointense to the normal testis on T1-weighted images, hypointense relative to normal testis on T2-weighted images, and diffusely enhancing on contrast-enhanced T1-weighted images (14).
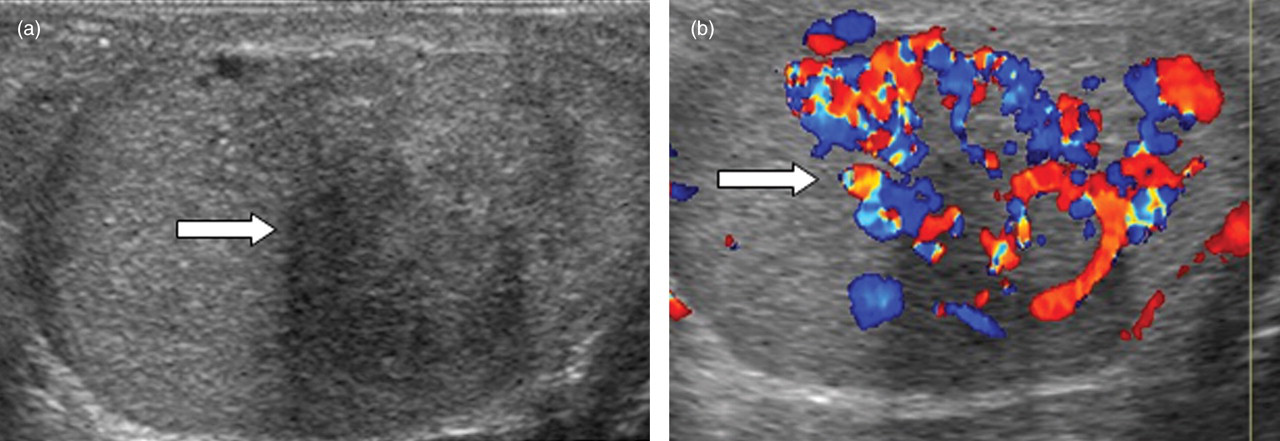
(a) 20-year-old man with congenital adrenal hyperplasia (CAH) and complaint of scrotal mass. Grey-scale sonographic image shows a heterogeneous lesion (arrow) with areas of posterior shadowing; (b) Color Doppler sonographic evaluation shows increased vascularity within the lesion (arrow). The patient is being managed medically for CAH
The intratesticular nodules of adrenal rests can gradually expand and destroy the testicular parenchyma, resulting in low testosterone production and infertility. The period from the initial detection of testicular abnormalities by sonographic examination until documented infertility can range from 0 to 10 years (15). Testicular vein sampling can show elevated cortisol levels compared with peripheral blood levels. Treatment with glucocorticoid replacement therapy can stabilize or repress these masses (14). If an adrenal rest tumor is unresponsive to steroid therapy, then partial orchiectomy may be considered (11).
Inflammatory pseudotumor
An inflammatory/fibrous pseudotumor is an uncommon lesion usually found in an extratesticular location. It is characterized by nodular reactive proliferation of fibrous tissue and inflammatory cells, possibly reactive most often involving the tunica vaginalis. The etiology is not well understood but these lesions are thought to be a tissue reaction resulting from a variety of etiologies, such as previous trauma, surgery, hydrocele formation, infection, chemotherapy, radiation, and adjacent neoplasm. In this setting of tissue reaction, immunomodulation occurs, which results in the activation and proliferation of spindle cells, plasma cell infiltration, and an increased density of local capillaries (16). The association of inflammatory pseudotumors with infection has been well established, with case reports describing inflammatory pseudotumors secondary to Epstein-Barr virus, CMV, and Mycobacterium Avium-Intracellulare (MAI) (17). There have been two cases of a testicular inflammatory pseudotumor in the setting of HIV infection (18, 19). Though inflammatory pseudotumors are rare, a thorough evaluation of the patient for underlying illness or infection should be considered once diagnosed.
The imaging findings of intratesticular pseudotumors have only been described in isolated case reports. The lesion has been described as a hypoechoic and hypervascular mass (Fig. 4a, b).
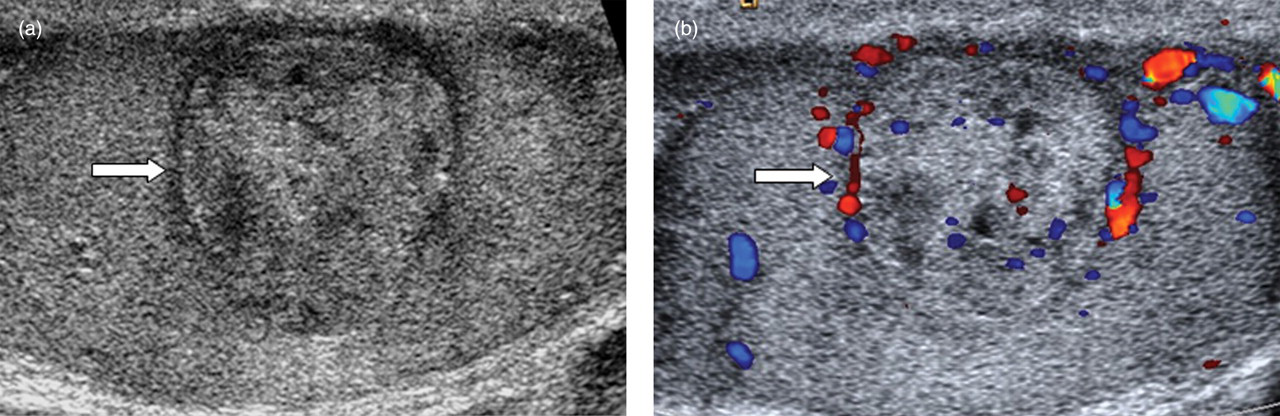
(a) 40-year-old man with testicular lump. Grey-scale sonographic image shows a well-defined heterogeneous lesion with a hypoechoic rim (arrow); (b) Color Doppler sonographic evaluation shows both internal and peripheral vascularity within this lesion. Surgical pathology performed due to suspicion of tumor revealed an inflammatory pseudotumor
Segmental testicular infarction
Segmental testicular infarction is rare and was often a diagnosis made following orchiectomy for a suspected tumor (20). The frequent use of color Doppler ultrasound has now allowed for a more confident assessment and diagnosis. Focal or segmental infarction can be caused secondary to a multitude of causes including small vessel ischemic disease, such as those with underlying vasculitis, intimal fibroplasia of the spermatic artery, sickle cell disease, and hypercoagulable states such as polycythemia, epididymo-orchitis, trauma, and inguinal hernia repair. Patients with a bell-clapper anomaly (an anomaly that leaves the testis free to swing and rotate within the tunica vaginalis) may also cause ischemia in the upper pole of the testis. Clinically segmental infarction usually presents with testicular pain.
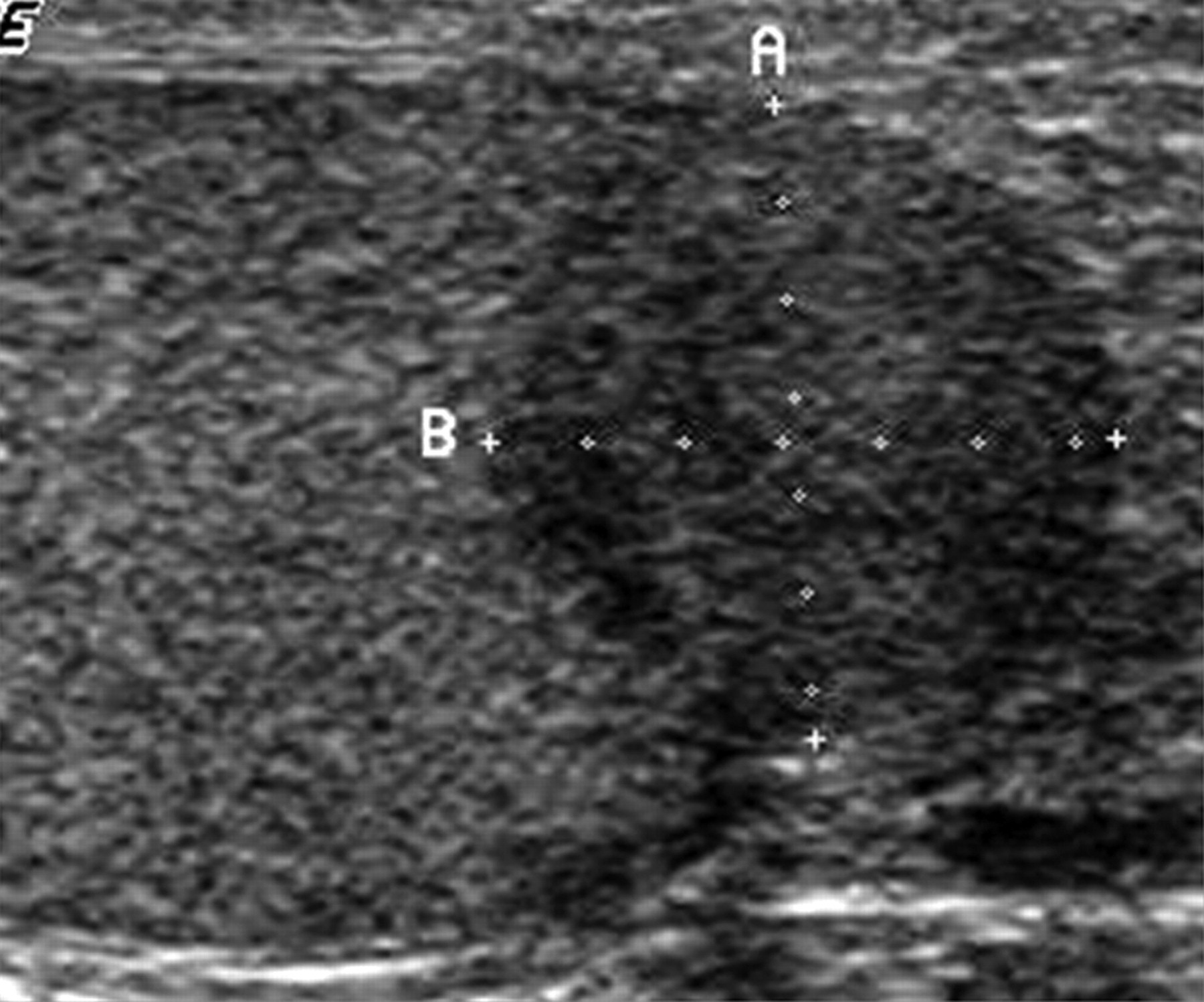
On ultrasonography, a segmental infarct usually appears hypoechoic and may be wedge-shaped commonly along the superior pole (Fig. 5a). The vertex of the infarct is usually directed towards the mediastinum. In the acute phase there may be associated focal expansion of the testis. Color Doppler sonographic imaging reveals poor or absent flow in this region, which is paramount in differentiating a segmental infarct from a tumor (Fig. 5b). These imaging findings along with negative tumor markers with short-term follow-up allow a confident diagnosis. Retraction of the tunica albuginea may also be noted in the area contacting the lesion, indicating a slight loss of lesion volume due to hyalinization and fibrosis occurring in the infarcted tissue (21).
(a) 40-year-old man with suspicion of epididymitis. Grey-scale sonographic image shows a well-defined wedge-shaped hypoechoic area (between cursors) at the superior pole of the testis. A complex hydrocele is also noted. (b) Color Doppler sonographic evaluation shows complete absence of color flow in this area along with hyper vascularity in the adjacent testis and epididymis consistent with epididymoorchitis with segmental infarct. The patient was treated for epididymo-orchitis and follow-up sonogram decreased size of the infarct at the upper pole
Contrast-enhanced ultrasound (CEUS) has been recently noted to improve lesion conspicuity and help make a confident diagnosis (22). This is performed following injection of stabilized gas microbubbles (measuring >10 microns), which act as blood pool tracers and produce harmonic signals at low acoustic power. The ischemic testicular lobules, which are key to differentiate infarction from tumor are initially depicted as non-enhancing regions on the contrast-enhanced study even when the lesions are not wedge-shaped on grey-scale ultrasonogram. Perilesional rim enhancement is noted on CEUS within 2–17 days of initial presentation (22).
MRI helps to make a confident assessment of an infarct as the borders are well delineated. On T1-weighted images in MRI, infarcts are usually isointense to testicular parenchyma, unless hemorrhagic when foci of high signal may be noted on T1-weighted images. On T2-weighted images, the signal intensity is variable, however, usually of low signal intensity. On gadolinium-enhanced T1-weighted images, the infarct appears as a non-enhancing area (Fig. 6a–c). There may be rim enhancement surrounding the infarct in the acute/subacute stage (21).
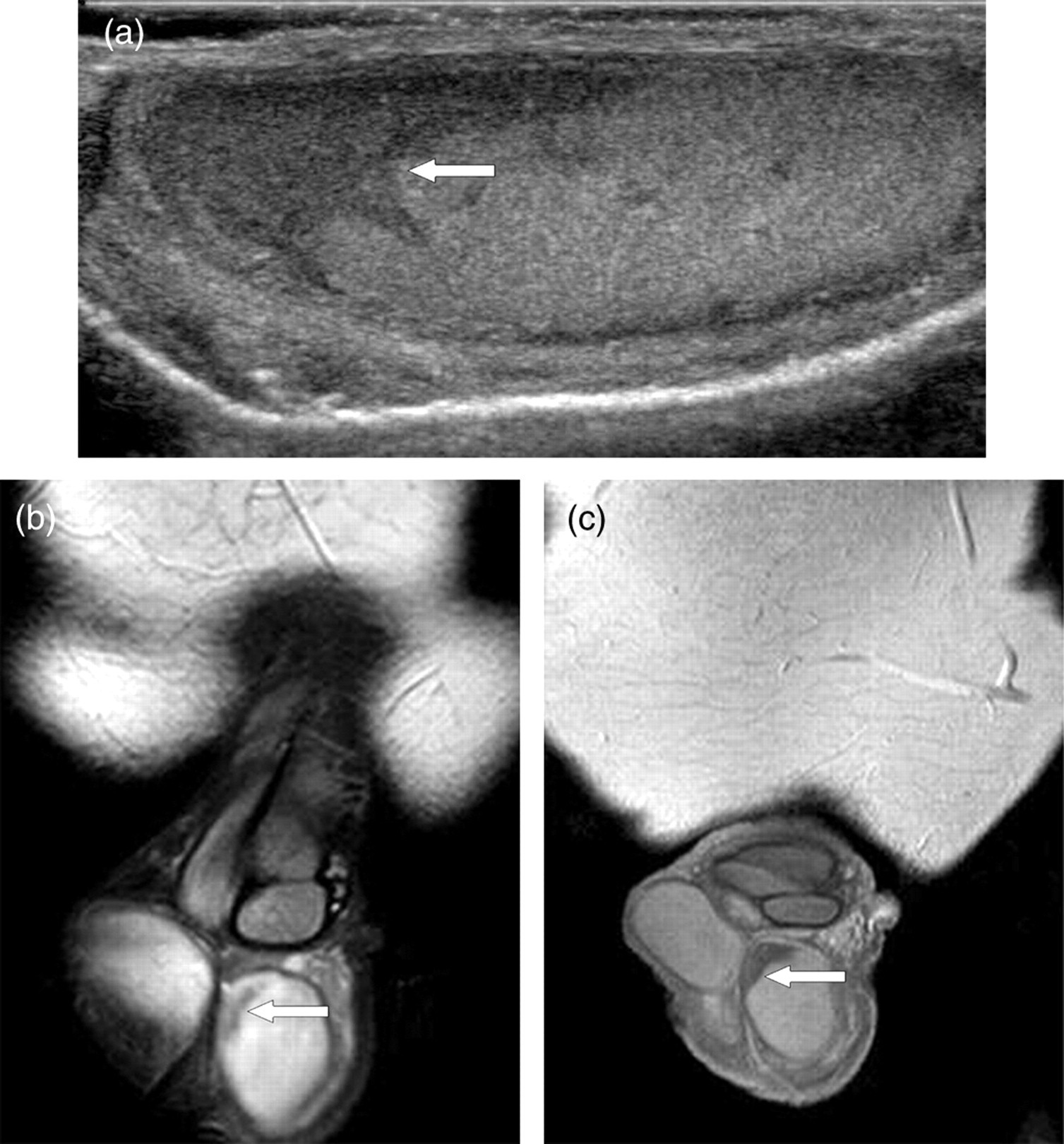
(a) 65-year-old man with chronic testicular pain. Grey-scale sonographic image shows a wedge-shaped hypoechoic area (arrow) at the upper pole of the testis; (b) Coronal T2-weighted MR image shows a hypointense area (arrow) at the upper pole of the testis corresponding to the sonogarphic abnormality; (c) Coronal postgadolinium T1-weighted MR image shows no enhancement in the area of infarct (arrow). The patient was diagnosed with chronic segmental testicular infarct with no change in imaging findings on follow-up
Scrotal masses with macroscopic fat
Testicular lipomatosis
Testicular lipomatosis (TL) is a recently described entity occurring exclusively in patients with Cowden disease (CD) in which rests of non-neoplastic lipomatous tissue (i.e. hamartomas) are seen in the testes (23). Cowden disease (also known as Multiple Hamartoma syndrome), is marked by increased cellular proliferation of ectodermal, mesodermal, and endodermal tissues (24). The pathognomonic mucocutaneous lesions of oral mucosal papillomatosis, trichilemmomas, and acral or palmar and plantar keratoses are present in 90–100% of patients with CD. Multiple benign and malignant neoplasms are associated with CD including cancers of the breast, thyroid, endometrium, and skin.
At sonography, TL manifest as multiple non-shadowing, uniformly hyperechoic small round foci of various sizes in both testes (Fig. 7). This appearance is virtually diagnostic of TL in the context of known Cowden disease. Similarly on MRI, multiple high-signal-intensity foci are seen in both testis on T1-weighted images (25). The differential diagnosis of bilateral masses in the testes include lymphoma, metastases, leukemia, and rarely, sarcoidosis or adrenal rests (26) However, these masses are typically hypoechoic on sonography and do not contain fat. The presence of these lesions can be used as a major diagnostic criterion for CD in adult males.
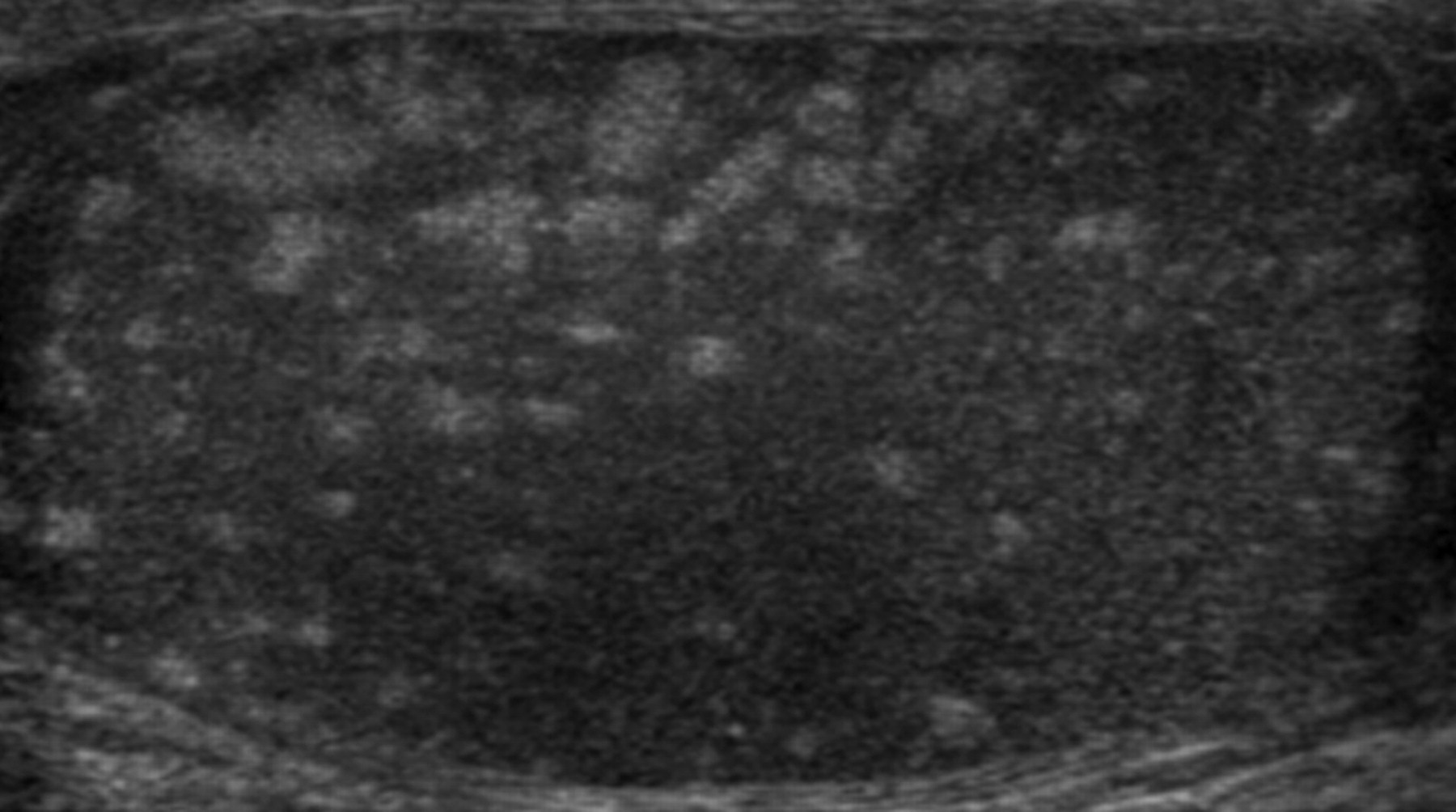
35-year-old man with Cowden syndrome. Grey-scale sonographic image shows numerous small echogenic foci/lesions within the testis consistent with lipomatosis
Lipoma
Intratesticular lipoma is an exceptionally rare condition (27, 28). However they are now being increasingly reported secondary to widespread use of scrotal sonography (2). On sonography, a lipoma usually consists of a homogeneously hyperechoic non-shadowing lesion without flow at color Doppler ultrasonographic imaging. The lesions follow the signal intensity characteristics of fat on MRI with no enhancement following contrast. Chemical shift changes confirm the presence of fat even when frequency-selective fat saturation techniques are not used.
Extratesticular lesions
Soft tissue masses
Adenomatoid tumor
Adenomatoid tumors (AT) that account for 30% of all para-testicular tumors, may originate from the epididymis, tunica vaginalis, or spermatic cord. ATs are the most common tumor of the epididymis and are the second most common benign para-testicular tumor following lipoma and occur more often adjacent to the lower pole of the testis (4:1). Adenomatoid tumors typically present as a painless scrotal mass and most are diagnosed in patients aged 20–50 years (29). ATs are typically unilateral and occur more frequently on the left side. When they grow non-invasively into the testicular parenchyma, they can simulate intratesticular disease.
Although the origin is still controversial, ATs are proposed to arise from vascular endothelium, the mesonephros or the Müllerian epithelium, although most recent reports consider them to be mesothelial in origin (30). AT is histologically composed of irregular tubules lined with flattened and cuboidal epithelioid or endothelioid cells that are well recognized with calretinin staining (Fig. 8). The stroma consists of hyalinized or loose collagen with varying amounts of smooth muscle and elastic fibers (30).
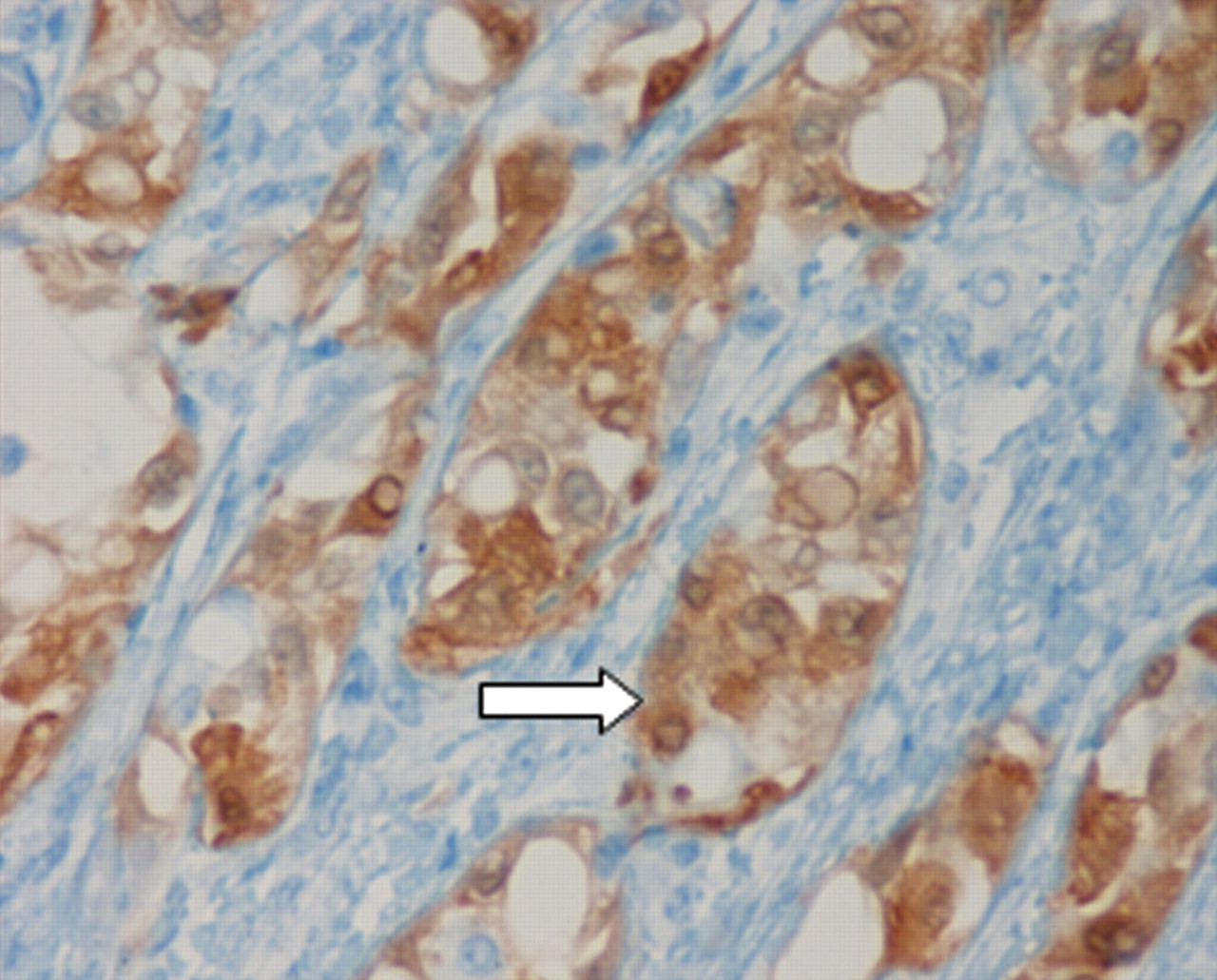
High power image of a Calretinin immunohistochemical study shows both cytoplasmic and nuclear positivity in the cells
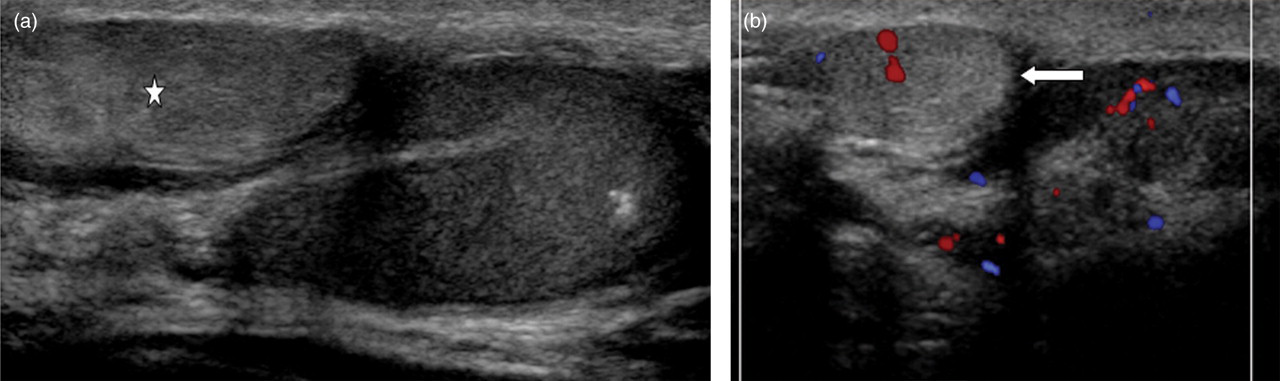
On ultrasonography, the AT appears as a well-circumscribed, solid extratesticular mass usually in the tail of the epididymis (Fig. 9). The lesion may show variable echogenicity but is commonly iso-hyperechoic (31). If the tumor arises from the tunica vaginalis or the tunica albuginea, differentiation from a testicular mass may be difficult on sonography (Fig. 10). MRI may then allow for precise localization of the origin of the mass and demonstrate enhancement features that enable a confident diagnosis and allow for conservative management (Fig. 11a and b) (32). On MRI, the lesion may show lower signal intensity relative to the testicular parenchyma on T2-weighted images. ATs may enhance after administration of gadolinium contrast material. Slow or decreased enhancement relative to the normal testis may also suggest a benign origin (33), although this finding can be variable.
50-year-old man with palpable lump. Grey-scale sonographic image shows a hypoechoic mass (between cursors) in the region of tail of epididymis consistent with an adenomatoid tumor
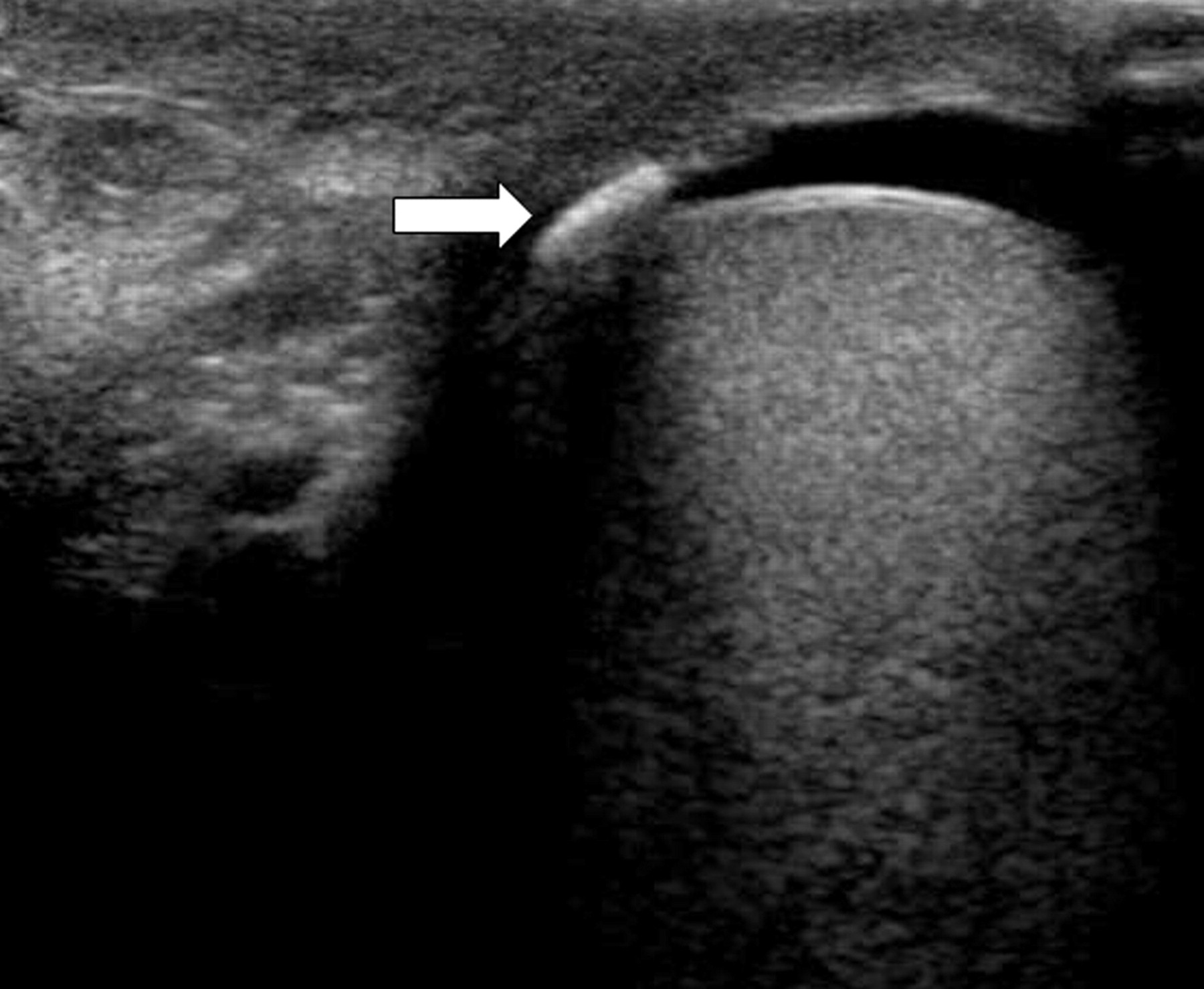
Grey-scale sonographic image shows a hypoechoic mass (star) at the lower pole of testis. On sonogram, it was difficult to exactly define whether the lesion was intra or extratesticular. MRI was then performed
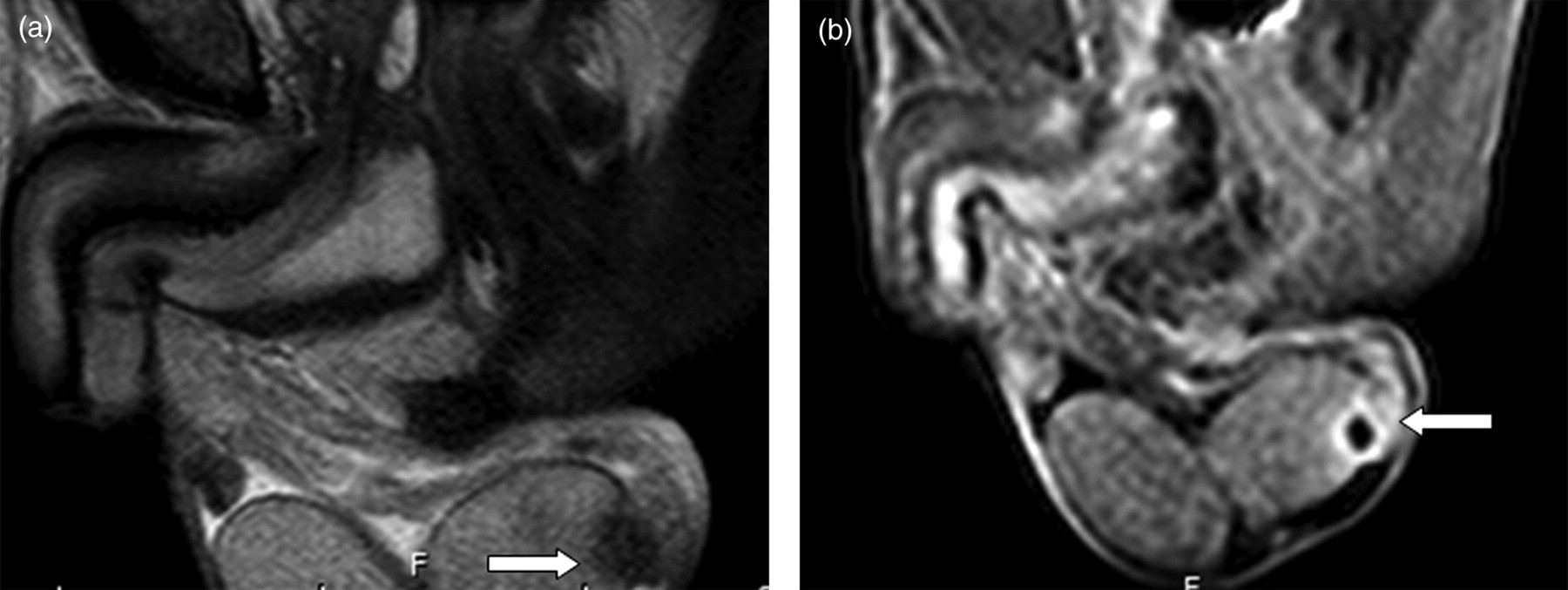
(a) Sagittal T2-weighted MR image showing a hypointense epididymal mass (arrow) that is separate from the testicle; (b) Sagittal post-contrast T1-weighted MR image demonstrates ring enhancement around the lesion (arrow). An extratesticular adenomatoid tumor was diagnosed and patient was spared surgical excision
Sperm granuloma
A sperm granuloma (SG) forms as a foreign body giant cell reaction to extravasated sperm. They may occur as a result of prior surgery, trauma, or infection. The reported incidence is up to 42% of men who have undergone vasectomy and 2.5% of the general population in an autopsy series. Although most SG is asymptomatic, some manifest as painful nodules. SG is histologically characterized by deposits of sperm surrounded by connective tissue and epithelial cells. Granulomatous inflammation and lymphoid cells are also seen (34).
Sperm granulomas are generally well-circumscribed, hypoechoic, solid masses at sonography (Fig. 12a and b). SGs may be multiple and can range in size from microscopic up to 4 cm, but most are less than 1 cm. Calcification occurs in less than 10% of cases (35). Although they can occur anywhere in the ductal system, they are most common at the cut ends of the vas deferens (36, 37).

(a) 50-year-old man with palpable scrotal abnormality. Grey-scale sonographic image shows a heterogenous lesion in the region of spermatic cord; (b) Color Doppler sonographic evaluation reveals no internal or peripheral vascularity in the lesion. The patient had history of vasectomy and a diagnosis of sperm granuloma was considered likely. The patient however opted for surgical excision and surgical pathology confirmed presence of sperm granuloma
Scrotal calculi
Scrotal calculi are free-floating calcifications within the tunica vaginalis and are also referred to as scrotoliths or scrotal pearls. It is postulated that these result from torsion of the appendix testis/epididymis or inflammatory deposits on the tunica vaginalis that have separated from the lining. Histologically these correspond to fibrinoid deposits around a central nidus of hydroxyapatite (38). Hydroceles are often seen in association.
On sonography, scrotal calculi appear as echogenic lesions with posterior acoustic shadowing and are usually mobile (Fig. 13). Multiple calculi may be seen measuring upto 1 cm.
65-year-old man with hard palpable nodule on testis. Grey-scale sonographic image shows a discrete echogenic foci with posterior shadowing consistent with a scrotolith and a small hydrocele
Fat-containing lesions
Lipoma
Lipomas account for most of the extratesticular tumors. These commonly arise from the spermatic cord and account for about half of all cord tumors (39). Lipomas can vary in size and do not show any age predilection (36).
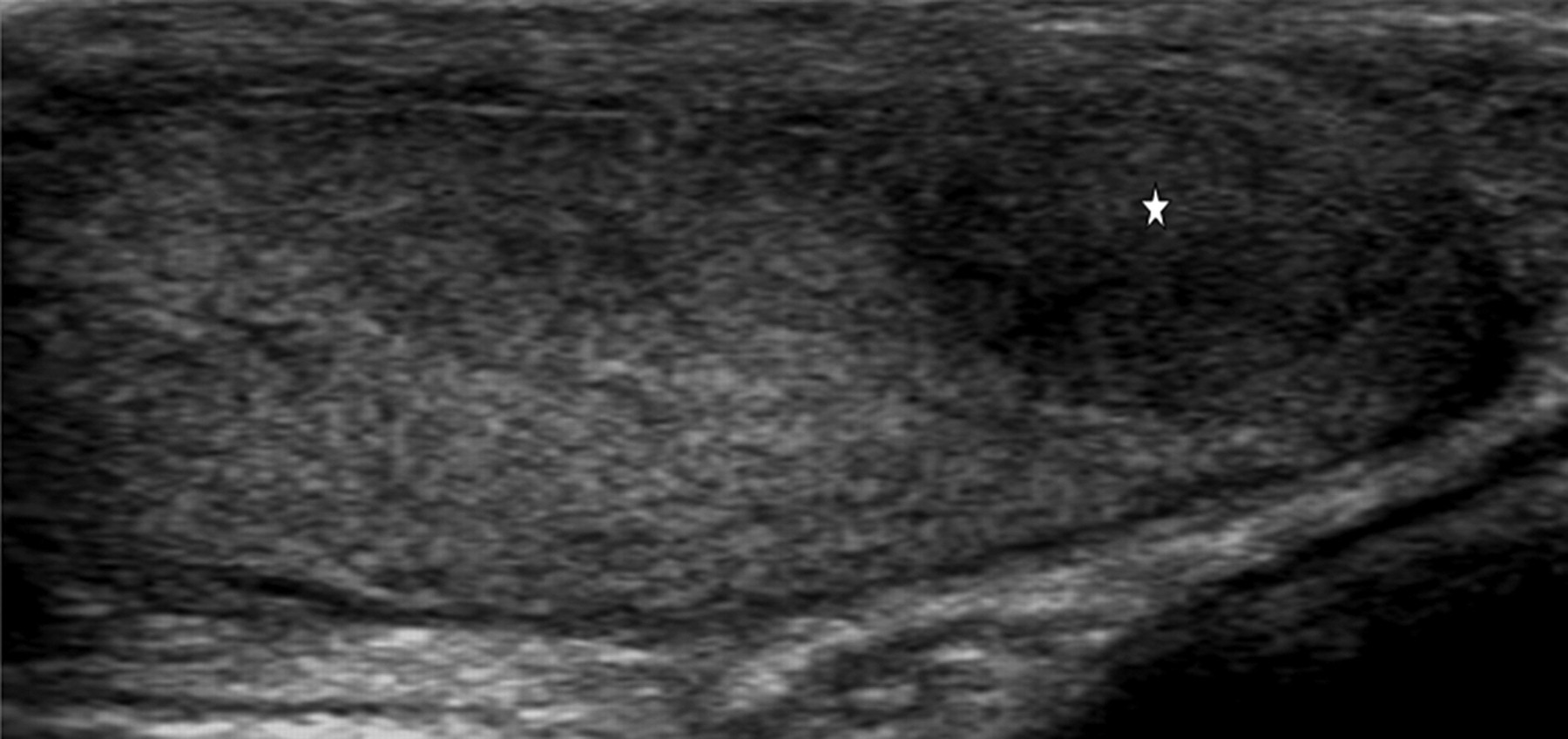
On ultrasonography, lipomas are usually well-defined and echogenic (Fig. 14); uncommonly they may appear hypoechoic (40). Lipomas contain various amounts of fibrous, myxoid, or vascular tissue, and the greater structural complexity presumably increases the echogenicity. No internal color flow is seen on Doppler ultrasonographic examinations. Lipomas must be distinguished from inguinal hernias with herniation of fat. This can be done by finding the superior edge of lesion or having the patient perform the Valsalva maneuver (Fig. 15a and b). When sonographic findings are equivocal, MRI can be helpful for making a definitive diagnosis. Lipomas have signal intensity similar to that of subcutaneous fat, on both T1- and T2-weighted images without enhancement (Fig. 16a and b). Hemorrhagic lesions may also have high signal intensity with these pulse sequences, so a fat-suppressed sequence must be performed to confirm the diagnosis (41).
55-year-old patient with scrotal mass. Color Doppler sonographic sonographic image shows a homogenous hyperechoic mass (star) superior to the testis without color flow consistent with lipoma

(a) 45-year-old man with scrotal mass. Grey-scale sonographic image shows a hyperechoic mass above the testicle (star). The superior margin of the lesion is not visible; (b) Coronal reformatted CT shows a fat (F) containing inguinal hernia (arrow) which simulated a lipoma on ultrasound

(a) Axial T2-weighted MR image showing a lesion that is isointense to the subcutanous fat (arrow) in the region of the left spermatic cord; (b) Axial fat-saturated post-contrast T1-weighted MR image demonstrating low signal intensity within the lesion without any region of enhancement (arrow). A spermatic cord lipoma was diagnosed based on these findings
Angiomyolioma
Angiomyolipoma (AML) is a benign mesenchymal tumor that is usually found in the kidneys. These are composed of a mixture of fat, smooth muscle cells, and tortuous, thick-walled, small to medium-sized blood vessels. Extra-renal lesions such as liver, lung, large bowel, bladder, and skin have also been reported. These tumors may arise sporadically or in the setting of tuberous sclerosis. There have been few case reports of intratesticular AML not associated with Tuberous Sclerosis (42).
On sonography, AML typically appear as well-defined hyperechoic lesions but may also appear heterogenous (Fig. 17a). Vascularity on color Doppler may be vary from none (primarily fat-containing lesion) to extensive (due to presence of vascular component) (Fig. 17b).
(a) Grey-scale sonographic image shows an oval echogenic lesion (star) superior to the testicle in the spermatic cord; (b) Color Doppler sonographic evaluation shows small amount of color flow within the lesion (arrow) which represented an angiomyolipoma
Both intra- and extratesticular lesions: granulomatous diseases
Sarcoidosis
Sarcoidosis is a multisystemic disorder characterized by non-caseating epitheloid granulomas. The reported incidence of genital involvement at postmortem is 4–4.5%, but only 0.5% of these patients had clinical symptoms (43). Sarcoid most commonly involves the epididymis; solitary testicular involvement is uncommon (44). Testicular sarcoid can present with a mass, which may be painful.
On sonography, sarcoid appears as a hypoechoic focal lesion/s within the testicle (Fig. 18). A diagnosis of sarcoidosis can be confidently made only if there is clinical evidence of sarcoid, if the intratesticular lesions are multi-focal or if there is associated epididymal involvement. Without these associated symptoms or features, tissue biopsy for pathological evaluation may be required (45). On MRI, the lesions are of low-signal intensity on T2-weighted images. Enhancement following contrast material administration is usually noted (46). The diagnosis of sarcoidosis should be considered if there is involvement of both the testis and the epididymis, particularly in African-American patients. The differential diagnosis for infiltrative processes involving the epididymis and the testis includes epididymo-orchitis, sarcoidosis, lymphoma, tuberculosis, and leukemia.
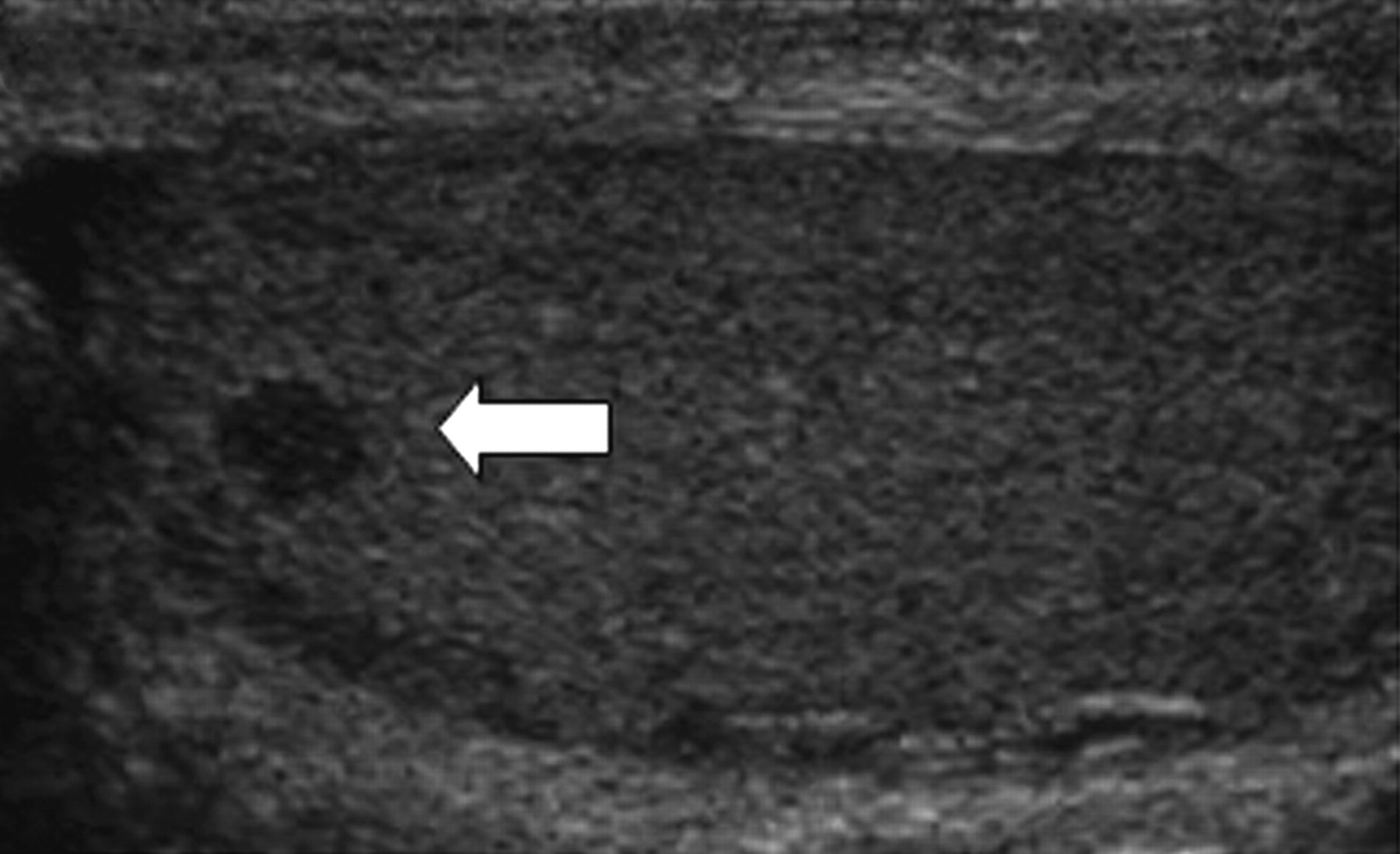
50-year-old man with incidental finding. Grey-scale sonographic image shows a focal hypoechoic lesion within the testicle (arrow). Similar lesions were also seen in the other testicle. Review of clinical charts revealed sarcoidosis and the lesions were followed conservatively with a presumed diagnosis of testicular sarcoidosis
Tuberculosis
Tuberculosis is the most common opportunistic infection in patients with human immunodeficiency viral infection. Tuberculous orchitis is an uncommon entity that may present with or without co-existent systemic disease. Extension from the lower urinary tract and hematogenous dissemination are postulated pathways of epididymal infection. Involvement of testis is almost always secondary to spread from epididymis.
On ultrasonography, a nodular or diffusely enlarged heterogenous epididymis is usually the earliest imaging finding. The testis is involved by direct extension from a tuberculous abscess. In advanced disease, nodules without Doppler flow may be seen in the testis/epididymis or the tunica vaginalis (Fig. 19a and b). These nodules represent tuberculomas with cystic necrosis. The entire testis may also be enlarged and diffusely heterogenous. There is usually an associated pyocele with internal debris. Sinus tracts to the scrotal skin and calcifications also may be seen. Orchiectomy may be needed if there is no reponse to antituberculous therapy or the diagnosis remains uncertain.

(a) 55-year-old man with history of treated genitourinary tuberculosis. Color Doppler sonographic image shows a focal heterogenous lesion with macrocalcification and no vascularity consistent with a calcified granuloma (arrow); (b) 35-year-old man with low-grade fevers and draining abscess from the skin. Grey-scale sonographic image shows heterogeneous echo texture (arrows) of the testis with small calcifications, areas of necrosis (star) and a pyocele. Culture reports revealed acid fast bacilli consistent with Mycobacterium tuberculosis
Conclusion
Benign intra- and extratesticular non-cystic lesions are being increasingly identified on imaging. Review of this text would allow a confident diagnosis of common benign intratesticular solid masses such as adrenal rests, Leydig cell hyperplasia, segmental infarcts, lipomatosis that are associated with characteristic imaging findings as well as clinical and demographic features. Lesions of Leydig cell hyperplasia are usually bilateral and hypoechoic, in contrast lipomatosis, which is also bilateral, is associated with echogenic lesions and occurs in association with the Cowden syndrome. Segmental infarcts are usually unilateral, wedge-shaped and at the upper pole and show decreased flow on Doppler imaging allowing for differentiation from a testicular tumor. Extratesticular benign lesion such as a lipoma is usually echogenic and located in the region of spermatic cord whereas adenomatoid tumors which are also hyperechoic on sonography usually occur in the tail of the epididymis. In cases where sonographic findings remain indeterminate, MRI can help to make a confident diagnosis esp by identifying site of origin of the mass, content within the mass such as fat in lipomas as well as presence or absence of contrast enhancement. A confident and correct diagnosis of a benign lesion may allow for conservative management or testicular preserving surgery.