
Abstract
Background
Accurately locating the epileptogenic focus in temporal lobe epilepsy (TLE) is important in clinical practice. Single-photon emission computed tomography (SPECT) and positron-emission tomography (PET) have been widely used in the lateralization of TLE, but both have limitations. Magnetic resonance perfusion imaging can accurately and reliably reflect differences in cerebral blood flow and volume.
Purpose
To investigate the diagnostic value of dynamic susceptibility contrast-enhanced (DSC) perfusion magnetic resonance imaging (MRI) in the lateralization of the epileptogenic focus in TLE.
Material and Methods
Conventional MRI and DSC-MRI scanning was performed in 20 interictal cases of TLE and 20 healthy volunteers. The relative cerebral blood volume (rCBV) and relative cerebral blood flow (rCBF) of the bilateral mesial temporal lobes of the TLE cases and healthy control groups were calculated. The differences in the perfusion asymmetry indices (AIs), derived from the rCBV and rCBF of the bilateral mesial temporal lobes, were compared between the two groups.
Results
In the control group, there were no statistically significant differences between the left and right sides in terms of rCBV (left 1.55±0.32, right 1.57±0.28) or rCBF (left 99.00±24.61, right 100.38±23.46) of the bilateral mesial temporal lobes. However, in the case group the ipsilateral rCBV and rCBF values (1.75±0.64 and 96.35±22.63, respectively) were markedly lower than those of the contralateral side (2.01± 0.79 and 108.56±26.92; P < 0.05). Both the AI of the rCBV (AIrCBV; 13.03±10.33) and the AI of the rCBF (AIrCBF; 11.24±8.70) of the case group were significantly higher than that of the control group (AIrCBV 5.55± 3.74, AIrCBF 5.12±3.48; P < 0.05). The epileptogenic foci of nine patients were correctly lateralized using the 95th percentile of the AIrCBV and AIrCBF of the control group as the normal upper limits.
Conclusion
In patients with TLE interictal, both rCBV and rCBF of the ipsilateral mesial temporal lobe were markedly lower than that of healthy control subjects. DSC-MRI can provide lateralization for TLE.
Keywords
Epilepsy is a common neurological disease whose incidence rivals only that of stroke; in China, from 3 to 6 in 1 million people suffer from epilepsy. A total of 25–50% of these cases is specifically temporal lobe epilepsy (TLE). Most refractory epilepsy is TLE, for which early surgical treatment is internationally advocated.
Accurate location of the epileptogenic focus preoperatively is the key to successful surgery, and methods of location are based on the long-held knowledge that cerebral blood flow (CBF) is increased in the region. The Wilder Penfield group (1) first described changes in CBF in focal epileptic seizures in the 1930s, and proposed an association between regional CBF and focal epileptic seizures. In the last decade it was shown that during TLE ictal, 97% of the epileptic foci are hyperperfused (2, 3). However, the perfusion pattern of the late phase is inconclusive. Certain studies using single-photon emission computed tomography (SPECT) (4) reported that the perfusion pattern varied over time after the contrast agent was injected. At present, the study of CBF in TLE interictal is focused on perfusion of the mesial temporal lobe.
Magnetic resonance imaging (MRI) is the most common and non-invasive method used in the diagnosis of TLE, and magnetic resonance (MR) perfusion imaging accurately and reliably reflects changes in CBF. The method has been widely used in the diagnosis of brain tumors and cerebral ischemic diseases, but rarely in TLE. SPECT and positron-emission tomography (PET) are currently the primary clinical tests for CBF changes in interictal TLE. Studies using SPECT and PET have confirmed that 50% of TLE interictal patients exhibit ipsilateral temporal lobe hypoperfusion (5, 6). However, due to the volume effect (that is, the loss of signal activity in small regions) and relatively poor resolution, the sensitivity of SPECT and PET is low. Using these tools alone for lateralization and localization in TLE remains difficult. In the present study, we explored changes in the perfusion parameters of the temporal lobes in interictal TLE using dynamic susceptibility contrast-enhanced (DSC)-MRI, and evaluated the value of this method for lateralization of an epileptogenic focus.
Material and Methods
Patient population
Twenty patients with TLE (12 men and 8 women; age range, 10–46 years; mean age, 23.2 ± 8.73 years) were enrolled in this study from June 1, 2010 to March 1, 2011 in the Department of Radiology, Xiangya Hospital, China (Table 1). All patients conformed to the International Classification of Epilepsies and Epileptic Syndromes issued by the plenary committee of the International League Against Epilepsy. Patients were excluded from the TLE group if they showed no evidence of TLE on electroencephalogram (EEG), and no mass lesions such as brain tumor, cerebrovascular diseases, or congenital malformations on conventional MRI.
Demographics and AIs of the case group
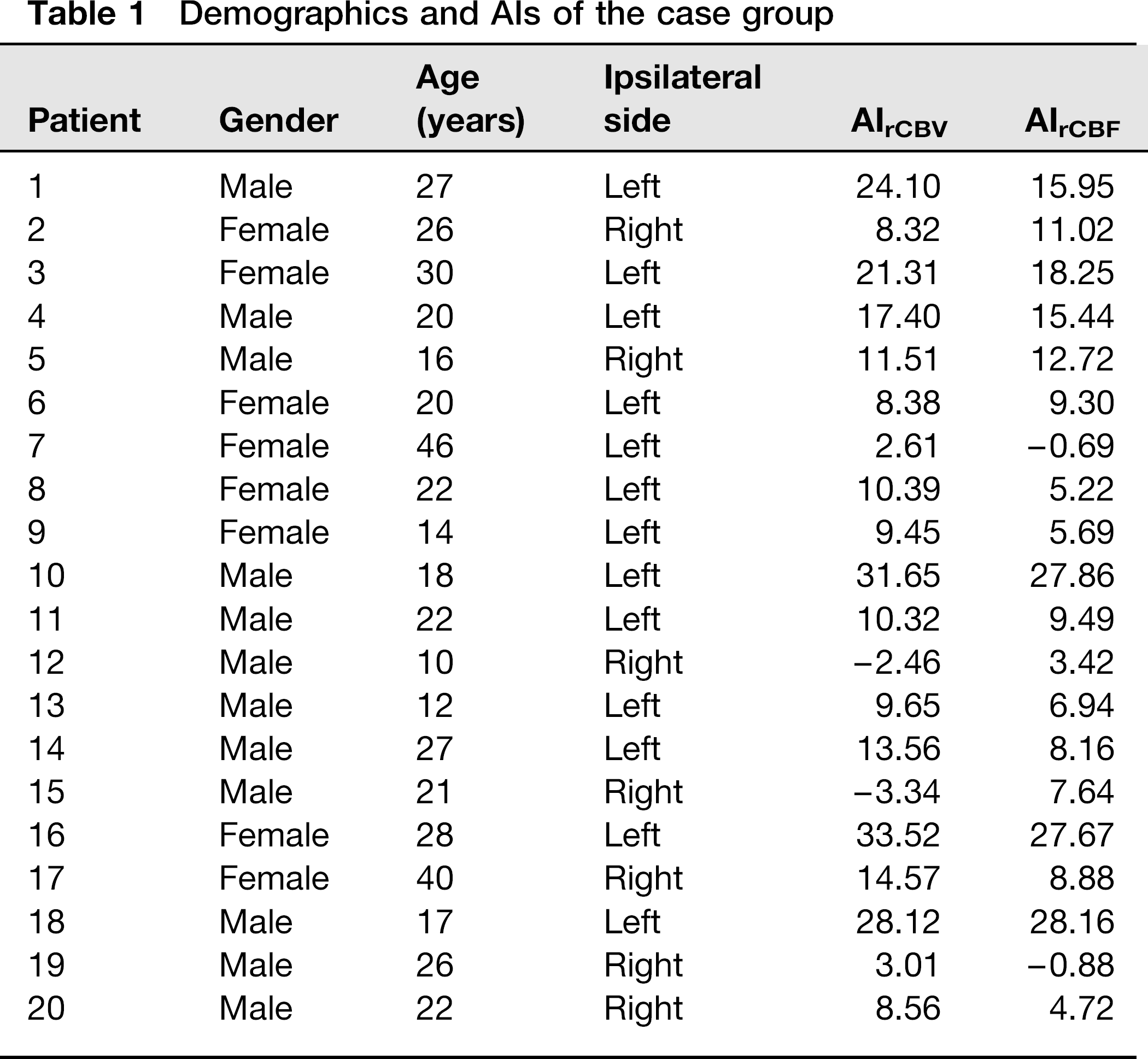
Unilateral TLE was diagnosed clinically by neurologists, based on combined comprehensive clinical symptoms and EEG. There were 13 left ipsilateral cases and seven were right. None of the patients had seizures during the 24 h prior to the MRI. The ipsilateral side was determined by clinical symptoms and the first abnormal onsets. The contralateral side defined as the side without seizures or the side after the first onset.
The control group consisted of 20 healthy volunteers (9 men and 11 women; age range, 22-53 years; mean age, 35.35 ± 9.75 years) with normal mental development. Exclusion criteria for the control group were a history of childhood febrile convulsions, central nervous system infection, or family history of seizures or epilepsy.
All participants or their families provided informed written consent. The Hospital Ethics Committee approved the study before the examination.
MRI protocol
The TLE patients and control volunteers were scanned on a 3.0T superconductive MR scanner (Signa HDX; GE Healthcare, Milwaukee, WI, USA) using a Medrad SCH 200 high-pressure syringe (Liebel-Flarsheim, Cincinnati, OH, USA) and the contrast agent gadolinium-diethyl triaminepentaacetic acid (Gd-DTPA; Guangzhou Kangchen Pharmaceutical, China).
MRI head scanning included: axial T2-weighted images (T2WI) with repetition time (TR)/echo time (TE), 4480/ 120 ms; field of view (FOV), 240; section thickness, 5 mm; intersection gap, 1.5 mm; and matrix, 384 × 256; axial T1WI with TR/TE, 1875/24 ms; FOV, 240; section thickness, 5 mm; intersection gap, 1.5 mm; and matrix, 320 × 256; axial fluid attenuated inversion recovery (FLAIR) with TR/TE, 8500/168 ms; FOV, 240; section thickness, 5 mm; intersection gap, 1.5 mm; and matrix, 320 × 256; and DSC-MRI and its corresponding T1WI (the same position and slice thickness).
DSC-MRI was acquired with gradient echo (GRE)-echo planar imaging (EPI) during the first pass with a bolus dose of Gd-DTPA (0.2 mmol/kg body weight). The scan position was parallel to the long axis of the hippocampus. Imaging parameters were: TR/TE, 1600 ms/14.3 ms; flip angle, 90°; FOV, 240 × 240 mm; section thickness, 5 mm; intersection gap, 1.5 mm; and matrix, 96 × 96.
A series of 60 multi-section sets were acquired in 96 s. The contrast medium was injected in the elbow at the fifth acquisition at 4 mL/s, and then a 20-mL bolus of saline was administered at 4 mL/s. The scan range, thickness, spacing, and FOV in T1WI were the same as those in DSC-MRI.
Data analysis
The DSC perfusion MR imaging was analyzed on perfusion software (Functool, GE Healthcare, Milwaukee, WI, USA). Processed maps were generated based on gamma variate fit. Relative corrected blood flow (rCBF) is defined as the volume of blood delivered to a given mass of tissue per unit time, thus representing instantaneous capillary flow in the tissue, estimated as the ratio of the integrated area to the time. Relative blood volume (rCBV) described the blood volume of the cerebral capillaries and venules (not arteries) per tissue volume, the integrated area of the signal intensity change. Gamma variate fitting was used to eliminate tracer re-circulation effect. The formula was: C(t) = DC + Cp(e / αβ) (t − AT)α e−(t − AT)/β.
A single operator blinded to clinical data of the subjects performed all measurements. The selection of region of interest was made with reference to Wolf et al. (7). The region of interest was hand-drawn with rCBV and rCBF maps at the same level of T1WI and included the amygdala, hippocampus, and parahippocampal gyrus. Generally, the mesial temporal lobe can be displayed over two or three levels (n). First the rCBV at the level of interest and the size of the region of interest were measured, and then the mean rCBV values of each side of the mesial temporal lobe was calculated with the following formula: (rCBV1 × area1 + … + rCBVn × arean)/(area1 + … + arean), where n = 2 or 3. Using the same method the mean rCBF values were calculated as well.
The asymmetry index (AI) was used to evaluate the perfusion changes in TLE interictal. The AI of the rCBV (or rCBF) is the absolute value of half the difference of the rCBV (rCBF) between the two sides over the total rCBV of the two sides, stated as a percentage. That is, the AIrCBV and AIrCBF of the control and case groups were calculated as:
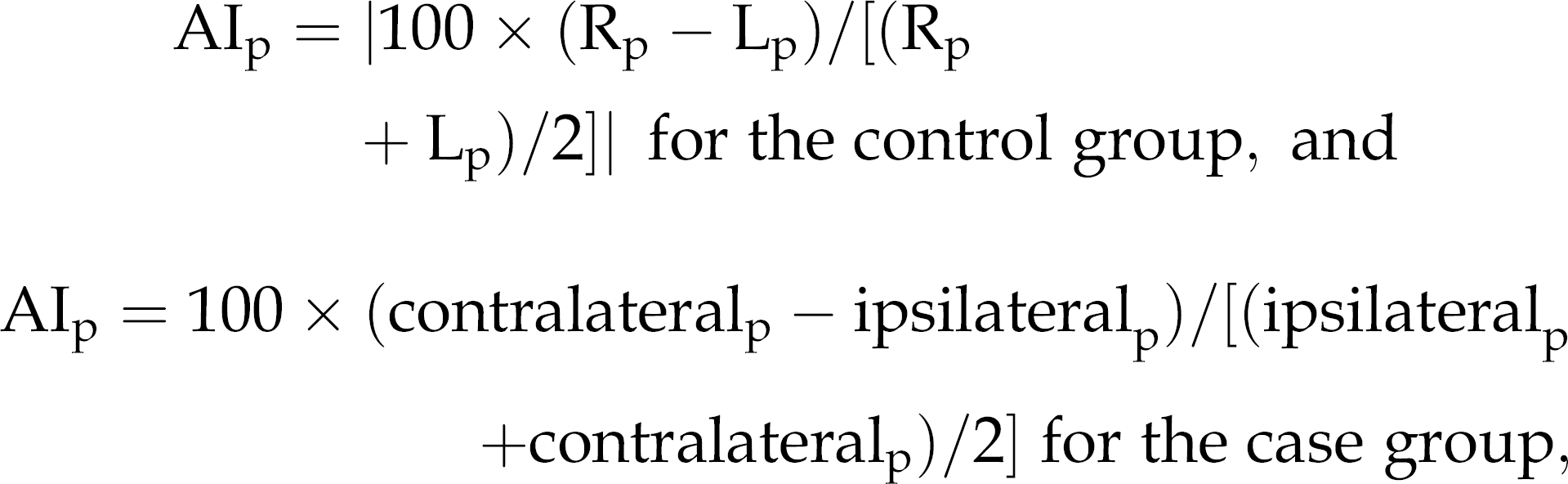
where p is rCBV or rCBF and R and L are the right and left temporal lobes, respectively.
The 95th percentiles of AIrCBV and AIrCBF of the control group was used as the normal upper limits to lateralize TLE.
Statistical analysis
SPSS13.0 (Statistical Product and Service Solutions, Chicago, IL, USA) statistical analysis software was used to compare the bilateral rCBVs and the rCBFs of the case and control groups using the paired t-test. The AIrCBV and AIrCBF of the control and case groups were analyzed and compared using the independent sample rank-sum test (Mann-Whitney U test). The difference was considered significant when P < 0.05.
Results
The mean values for rCBV and rCBF of the bilateral mesial temporal lobe of the control group were almost symmetrical between the left and right sides; the difference was not significant (P > 0.05). Specifically, in the control group the rCBVs of the left and right sides were 1.55 ± 0.32 and 1.57 ± 0.28, respectively (t = 0.992, P = 0.334). The rCBFs for the left and right sides were 99.00 ± 24.61 and 100.38 ± 23.46 (t = 1.068, P = 0.299).
In the TLE case group, the mean rCBV and mean rCBF of the ipsilateral temporal lobe were significantly lower than those of the contralateral side (P < 0.05). Specifically, in the case group the rCBVs of the ipsilateral and contralateral sides were 1.75 ± 0.64 and 2.01 ± 0.79, respectively (t = 4.705, P < 0.05). The rCBFs for the ipsilateral and contralateral sides were 96.35 ± 22.63 and 108.56 ± 26.92 (t = 5.742, P < 0.05).
Since the AI values did not follow a normal distribution, the median and interquartile values were presented as well as the conventional mean ± standard deviation. The AIrCBV and AIrCBF of the temporal lobe of the case group and the control group were compared using the Mann-Whitney U test. The AIrCBV and AIrCBF of the case group were significantly higher than that of the control group (P < 0.05). Specifically, the median, quartile, and mean values of the AIrCBV of the case group were 10.36, 11.99, and 13.03 ± 10.33, respectively, and these values for the control group were 5.44, 10.12, and 5.55 ± 3.74 (U = 2.894, P = 0.003). The median, quartile, and mean values of the AIrCBF of the case group were 7.14, 7.11, and 11.24 ± 8.70, and the corresponding values for the control group were 4.83, 6.87, and 5.12 ± 3.48 (U = 2.38, P =0.017).
When the 95th percentile values of AIrCBV of the control group were used as the normal upper limit to lateralize TLE, the diagnosis threshold was set as 12.24. Eight patients (case no. 1, 3, 4, 10, 14, 16, 17, and 18) were accurately lateralized. The diagnostic sensitivity was 40% with a specificity of 95%. When the 95th percentile values of AIrCBF of the control group were used as the normal upper limit to lateralize TLE, the diagnostic threshold was 11.07; seven patients (case no. 1, 3, 4, 5, 10, 16, and 18) were accurately lateralized. The diagnostic sensitivity was 35% with a specificity of 95%. The epileptogenic foci of nine patients were correctly lateralized when we used the combined AIrCBV and AIrCBF of the control group as the normal upper limit. DSC-MRI diagnostic sensitivity was 45% and the specificity was 90%.
Discussion
Principles and techniques of DSC-MRI
Perfusion-weighted MRI is most commonly performed with either the DSC or arterial spin labeling (ASL) method. Only DSC perfusion MRI requires an exogenous contrast agent, and is used more often clinically. DSC-MRI is affected immediately with an intravenous bolus injection of paramagnetic contrast agent. When the agent passes the capillary, it interferes with the local magnetic field homogeneity, reducing the T2* signal intensity. The signal changes in these regions are reflected in changes in hemodynamic parameters, and thus information regarding microcirculation is obtained. Either spin-echo or gradient-echo sequences can be used for DSC imaging; the latter is sensitive to all blood flow information from capillaries and large blood vessels (8, 9). In the present study, we used GRE-EPI to acquire the original perfusion image.
Relative DSC-MR perfusion parameters are more reliable because they are based on fewer assumptions (e.g. the linearity of δR2* signals in arteries with tracer concentrations) and they impose fewer methodological constraints than AIF quantification methods. Relative parameters are as useful as absolute measurements for investigating intrapatient effects. Measuring relative parameters involves monitoring perfusion between sequential observations or detecting localized hemodynamic conditions (10, 11). Interpatient parameters are more difficult to quantitate. Therefore, most researchers have used a ratio of lesion-to-normal tissue area within the same patient as a quantitative indicator. In this study, we used the AI of the bilateral temporal lobes of each patient individually to evaluate the perfusion changes in TLE interictal.
Changes in cerebral blood flow in TLE interictal
TLE originates in the temporal lobe and accounts for 25–50% of epilepsy. The studies of Fink et al. (12) and Breier et al. (13) have shown that the perfusions of the bilateral mesial temporal lobe in TLE are asymmetric, suggesting lateralization of the epileptogenic focus. We found that the AIs of the TLE case group were higher than those of the healthy control group.
The AIs of nine patients were significantly higher than those of the control group, which is in agreement with clinical practice experience, EEG, and the literature. Most of the literature has reported that hypoperfusion appeared in the ipsilateral mesial temporal lobe of TLE intericta (5, 6). In our study, in the control group the differences between the perfusions of the bilateral sides were not significant, but in TLE patients the ipsilateral perfusion was significantly lower than that of the contralateral side (Fig. 1), consistent with the literature.
Representative conventional MRI (a–c) and DSC-MRI (d–h) obtained from a patient with left TLE (patient 18). (a–c) Axial T1WI image; (d–f) rCBV map in corresponding levels; (g–i) rCBF map in corresponding levels. The left mesial temporal lobe showed hypoperfusion. Red, green, and blue areas indicate high, medium, and low measurement parameters, respectively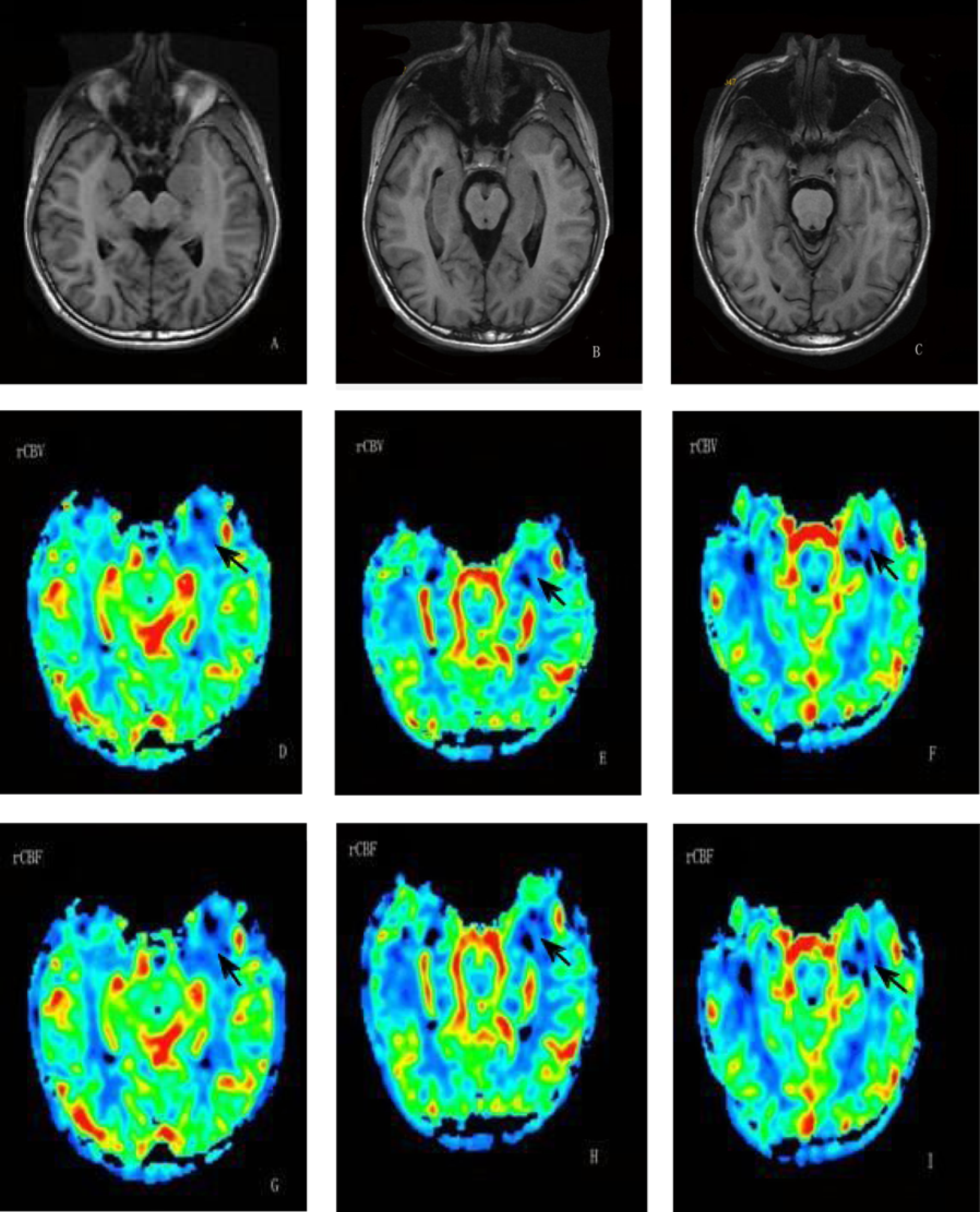
The reason for ipsilateral hypoperfusion of TLE interictal is not very clear. It has generally been considered to be due to neuronal loss and cortical atrophy (14), but may be related to epileptic discharge (15) because TLE EEG is still visible in TLE interictal. Hippocampal sclerosis was also reported to be closely related to TLE and could be cause or result, or one promotes the other (3). Studies has shown that the CBF of the ipsilateral hippocampus in TLE interictal was reduced (6, 16), and conventional MRI of the majority of these patients showed hippocampal sclerosis or atrophy. In addition, the change in the hippocampus structure may be related to TLE hypoperfusion. The mesial temporal lobe of TLE interictal has shown not only ipsilateral hypoperfusion, but also bilateral hypoperfusion or normal perfusion (17). In our study, most patients showed ipsilateral perfusion reduction, while some showed roughly equal perfusion bilaterally.
Evaluation of DSC-MRI for lateralization of interictal TLE
Ren et al. (16) and Brien et al. (18) have applied DSC-MRI to lateralization in TLE interictal. The former showed that the rCBV of the ipsilateral hippocampus was reduced significantly; nine patients with TLE were lateralized accurately in their study. Brien et al. (18) found that the lateralization accuracy of rCBF was 100% (10/10). In both of these studies, the sensitivity of DSC-MRI in TLE lateralization was significantly higher than the 45% of our study. Several reasons may account for this. First, the severity of the diseases was different – the patients in their studies had serious hippocampal sclerosis and received surgical treatment, while in our study only one patient showed hippocampal sclerosis on conventional MRI.
In addition, between the present study and those of Ren et al. (16) and Brien et al. (18) there were differences in the optional measurements performed. We selected the mesial temporal lobe as the region of interest, while the latter studies measured the local blood flow on both sides of the hippocampus, and the methods were very sensitive to the perfusion reduction of the hippocampus. The mesial temporal lobe was our focus because structures in this region are also subject to TLE attack. The entorhinal cortex and amygdala play an important role in the origination and expansion of epilepsy. Stereotactic electrode tests have shown that the abnormal electrical activity of TLE might originate in the amygdala and isolated damage in this structure was observed. Furthermore, choosing the mesial temporal lobe as the region of interest should capture the perfusion change in TLE more comprehensively. While the vast majority of PET and SPECT studies of TLE chose the mesial temporal lobe as the region of interest, there have been no reports pertaining to changes in the region using DSC-MRI in TLE interictal.
Finally, we chose the temporal lobe over the hippocampus because there is a greater susceptibility to artifact in 3.0T MR, and the local anatomy of the hippocampus is very complex. The DSC-MRI parameters of the local hippocampus are easily influenced by volume effect, and expanding the regions of interest can improve accuracy of the data.
Some authors have focused on the ASL method in the study of TLE interictal. Wolf et al. (8) studied 12 patients with TLE interictal and found that the AI of bilateral perfusion of the mesial temporal lobe of the case group was higher than that of the control group. Young et al. (19) studied 10 patients with TLE using ASL and found that the perfusion of the ipsilateral mesial temporal lobe was reduced. The AIs of four TLE patients were significantly higher than those of the control group and the ipsilateral side was accurately determined. Although ASL-MRI may provide valuable information for TLE lateralization, DSC-MRI has a higher signal-to-noise ratio and reflects blood flow information more comprehensively than ASL-MRI. The additional rCBV information to be gained from DSC-MRI (e.g. time to peak, mean transit time, and bolus arrival time) is also valuable, as it is highly reliable for small changes in perfusion (20). However, the drawback of DSC-MRI that ASL-MRI does not share is that it requires injection of a contrast agent, which increases the burden of patients. Both methods have their advantages in practical applications.
Advantages and disadvantages of DSC-MRI application in TLE
For TLE lateralization, SPECT and PET are currently the principle imaging modalities used, and not DSC perfusion MRI. Amorim et al. (21) found that the sensitivity of SPECT used for ictal TLE surpassed that of interictal TLE, where the sensitivity was low (32.3–55.3%). In the present study, the results using DSC perfusion MRI showed that the AIs from nine TLE interictal patients were significantly higher than those of the healthy volunteers, and the ipsilateral side could be determined accurately. The data indicated that DSC-MRI, like SPECT, could provide information for TLE lateralization.
MRI requires a high degree of patient cooperation, which limits the application of DSC-MRI in TLE ictal. It is also very difficult for MR to capture the late phase of TLE. SPECT is therefore more useful than DSC-MRI in TLE ictal and its late phase. However, our study confirmed that DSC-MRI could determine the asymmetry perfusion change in the bilateral mesial temporal lobes in TLE interictal, and find the lateralized epileptogenic focus accurately. Compared with SPECT, DSC-MRI also has a higher resolution, which allows the identification of small changes in perfusion, and when integrated with conventional MR, it can lateralize accurately.
PET studies have shown that hypometabolism and hypoperfusion are important findings for localizing the epileptogenic focus in TLE interictal. However, one study using PET reported that changes in CBF did not match changes in metabolism, which may decrease the sensitivity of PET in TLE lateralization (22). Otha et al. (23) also reported that the accuracy of 15O-H2O PET for TLE lateralization was low. This evidence suggests that it is difficult to use PET alone for TLE lateralization. In contrast, according to Young et al. (18) there is high consistency between MRI perfusion and PET perfusion. However, the cost of PET is very high and limits its application. DSC-MRI may be a viable clinical alternative to PET, for its high resolution and lower cost.
Our study was limited in that the diagnosis of unilateral TLE by neurologists rested on combined comprehensive clinical symptoms and EEG, and the lack of pathology may influence the sensitivity ratings. Furthermore, the only parameters we compared were the rCBV and rCBF. Other DSC-MRI parameters, such as mean transit time, may be important to consider.
In conclusion, the present study demonstrates that both rCBV and rCBF of the ipsilateral mesial lobe in TLE interictal are significantly reduced compared to the contralateral side, and DSC-MRI can provide lateralization for TLE.