
Abstract
A variety of abdominal and pelvic tumors can present with rupture leading to hemoperitoneum/hemoretroperitoneum or peritonitis. Imaging plays an important role in the diagnosis of hemorrhage or peritonitis as well as in the detection of ruptured tumors or organs. In this article, we illustrate the imaging findings of ruptured tumors arising in the abdominal and pelvic organs while excluding those of ruptured tumors arising in the stomach and intestines. It is important for the radiologists to understand the mechanisms involved in tumor rupture and recognize the imaging features of ruptured tumors according to the organs involved because this will permit the exact diagnosis of ruptured tumors, thereby facilitating prompt and effective treatment.
While perforation is a condition in which a hole develops in the wall of organs, especially in the gastrointestinal tract, rupture is defined as a tear on the surface of organs or tumors, and is usually used in reference to solid organs. Rupture of solid organ tumors occurs either as a consequence of trauma or spontaneously. These conditions frequently lead to various degrees of hemoperitoneum or hemoretroperitoneum that may require prompt treatment, such as transarterial embolization or surgery. Occasionally, ruptured tumors result in peritoneal inflammation or dissemination of mucin in the peritoneal cavity. Therefore, both timely diagnosis and correct therapeutic decision-making are important and they are entirely dependent on the imaging diagnosis.
In the trauma patient or in the setting of acute abdomen, computed tomography (CT) has been widely used for the detection of blood in the peritoneal cavity or in the retroperitoneum; this imaging modality can provide a variety of information about bleeding such as source of bleeding, amount of bleeding, and the presence of active extravasation (1, 2). During image interpretation in cases of bleeding, particularly when the clinical history of trauma is not clear, the radiologist needs to be aware of the possibility of underlying tumors which can be the cause of bleeding since underlying tumors can affect the prognosis of patients and the treatment plan (Table 1).
Summary of ruptured abdominal and pelvic tumors
In this article, we illustrate the imaging findings of ruptured tumors occurring in various abdominal and pelvic organs.
Liver
When hemoperitoneum occurs in patients with hepatic masses, the most important clinical issue is to identify whether the tumor is the possible cause of hemoperitoneum. If the hepatic mass is the site of origin of the bleeding, the next step is characterization of the hepatic tumor. Rupture occurs more frequently in hypervascular hepatic tumors than in hypovascular hepatic tumors. Hepatocellular carcinoma (HCC), frequently seen as a hypervascular mass, is the most common cause of rupture associated with tumors in the liver. Rupture has been reported to occur in 3–15% of patients with HCC (2, 3). On the other hand, although rupture is a significant potential complication related to hepatocellular adenoma, it is infrequently encountered because of the rarity of the tumor (4).
Several theories, including disruption of a feeding artery, laceration of a superficial hepatic tumor due to minimal trauma, or an increased intratumoral pressure secondary to hepatic venous occlusion by tumor cells, have been suggested as the potential mechanisms for the development of spontaneous HCC rupture (3–5).
Imaging features of ruptured hepatic tumors reported in the literature have mainly been representative of HCCs. Given that hepatic tumors such as HCC, adenoma, focal nodular hyperplasia (FNH), and hemangioma usually appear as arterially-enhancing masses on CT, they may demonstrate similar cross-sectional imaging findings when a rupture develops. Moreover, differentiation of these ruptured hypervascular tumors can hardly be accomplished with imaging modalities alone especially when severe rupture occurs or dynamic scanning is not available.
On non-enhanced CT, high-attenuating areas representing clotted blood are evident close to the ruptured tumors (also known as the “sentinel clot sign”) (1–4). Sometimes, the observation of active extravasation of contrast material allows easy detection of bleeding tumors on enhanced CT (Figs. 1 and 2). Although arterially-enhancing masses showing contrast agent wash-out on subsequent delayed phase images are the typical imaging findings of HCCs, many HCCs can appear as low attenuating masses with focal parenchymal discontinuity when a rupture develops (Figs. 1 and 2) (3). This phenomenon may be due to compensatory arterial vasoconstriction during hypovolemic shock (5). Occasionally, intratumoral bleeding in hepatic tumors such as HCC, adenoma, or FNH can appear as a hemorrhagic mass with subcapsular hematoma formation on CT or magnetic resonance (MR) imaging (3, 4).

A 41-year-old man with a ruptured hepatocellular carcinoma (HCC). Hepatic arterial phase CT scan shows a partially enhancing mass in the subcapsular area of the right hepatic lobe (long arrows), perihepatic high-attenuation fluid (short arrows in a and b), and extravasated contrast material (arrowhead). A ruptured hepatocellular carcinoma was confirmed by pathology after a right hepatic lobectomy was performed

A 76-year-old man with a ruptured hepatocellular carcinoma (HCC). Axial enhanced CT scan obtained in the hepatic arterial phase shows high-attenuation fluid in the right perihepatic space (short arrows), a low-attenuated mass with surrounding parenchymal enhancement (arterioportal shunt; this was not seen in the portal venous phase) in the right hepatic lobe (long arrows), and extravasated contrast material in the mass (arrowhead). The low-attenuated mass was confirmed to be a ruptured HCC after a partial hepatectomy was performed
Hepatocellular adenoma is a rare benign neoplasm usually found in women who use oral contraceptives. Adenomas are hypervascular masses due to the presence of extensive sinusoids and feeding arteries (6). In addition, they may be predisposed to intratumoral hemorrhage or spontaneous rupture due to a paucity of connective tissue support (6). FNH is the second most common benign hepatic tumor after hemangioma. FNH is seldom associated with spontaneous rupture; this may be due to the presence of connective tissue within the tumor (2, 4).
Since arterially-enhancing tumors such as HCC, adenoma, FNH, and hemangioma share a similar imaging appearance, clinical information or history can help to differentiate between these ruptured tumors; for example, if sudden abdominal pain occurs in a young woman taking oral contraceptives, ruptured hepatocellular adenoma should be suspected as the cause of bleeding.
Hepatic hemangiomas are the most common hepatic tumors and can rupture spontaneously or due to trauma; however despite the high incidence of hemangiomas, hemangioma rupture is very rare (4, 7, 8). Some contributory factors have been suggested for spontaneous or traumatic rupture of hepatic hemangiomas and they include tumor size (6–25 cm), tumor location (right lobe), appearance (exophytic growth), ongoing medical therapy (steroid therapy), and pregnancy (2, 7, 8). Differentiation between ruptured hemangiomas and HCCs may be challenging unless triple phase CT is available (Fig. 3).

A 55-year-old man with a traumatic rupture of an exophytic hepatic hemangioma. (a) Pre-contrast CT scan shows a low-attenuated mass (long arrow) surrounded by high-attenuation areas representing clotted blood (so-called “sentinel clot sign”) (short arrows) in the left hepatic lobe. Hemoperitoneum is also seen in the perihepatic and perisplenic spaces. Our initial interpretation for this mass was a ruptured HCC because initially single phase enhanced CT was obtained (not shown). (b) On follow-up, a three-phase CT was performed after resorption of hemoperitoneum. The mass shows a centripetal enhancement pattern throughout the three phases (left, arterial phase; middle, portal phase; right, equilibrium phase) (arrows), which is a typical imaging finding of hepatic hemangiomas
Rupture is very uncommon in cases of hepatic metastasis and cholangiocarcinoma due to the histopathologic characteristics of abundant fibrous stroma and a relatively poor vascularity (2, 4, 9, 10). Hepatic metastases from lung carcinoma, renal cell carcinoma, and melanoma have been reported to be the most frequent causes of hepatic bleeding (4). Although ruptured hypovascular tumors share similar mechanisms as those in HCC rupture, tumor necrosis is thought to be the most important factor for the development of rupture (4, 9, 10). On imaging, ruptured tumors appear as protruding, low-attenuated subcapsular masses with discontinuity of the liver surface, and surrounding hemoperitoneum. Sometimes, intratumoral hemorrhage can be observed as a high-attenuation area on unenhanced CT and as a high signal intensity area on T1-weighted MR image, or as fluid-fluid level on both images (Fig. 4) (11).

A 59-year-old man with hemoperitoneum secondary to spontaneous rupture of hepatic metastases from small cell lung carcinoma. Enhanced CT scan shows multiple metastatic masses in the right hepatic lobe with one of these metastatic lesions showing a fluid-fluid level within the mass (long arrow). Note the high-attenuation hemoperitoneum (short arrows)
Pancreas and spleen
Although ruptured pancreatic tumors are rare, two noteworthy patterns of ruptured pancreatic neoplasms include rupture of the intraductal papillary mucinous neoplasms (IPMNs) and splenic rupture associated with pancreatic malignancies (12–15).
IPMNs, which are papillary-growing tumors with abundant mucin production within the pancreatic duct, encompass a wide spectrum of intraductal papillary neoplasms from adenomas to invasive carcinomas, with an incidence of rupture ranging from 11–15% (12, 13). Ruptured IPMNs present with one of the following two patterns (12, 13). The first pattern is fistula formation to adjacent organs such as the duodenum, common bile duct, and stomach induced by tumor cell invasion. The other pattern is free intraperitoneal rupture resulting in pseudomyxoma peritonei (Fig. 5). The latter situation develops as a result of an increased pressure in the main pancreatic duct or a cystic mass due to mucin accumulation. Although the majority of ruptured IPMNs are associated with carcinomas, adenomas are infrequently encountered in ruptured cases (12). In order to make a diagnosis of a ruptured IPMN on imaging, the identification of a fistula between the pancreatic cystic mass and adjacent structure and/or imaging findings of pseudomyxoma peritonei such as marginal scalloping of the liver are necessary. Occasionally, leakage of contrast agent from the pancreatic duct can be seen on pancreatic ductography (Fig. 5).

A 61-year-old man with a ruptured intraductal papillary mucinous adenocarcinoma (IPMN). (a) Enhanced CT scan shows a large, cystic mass (long arrows) connected to a dilated pancreatic duct (short arrows). Omental soft-tissue masses suggesting peritoneal carcinomatosis (arrowheads) and low-attenuating peritoneal fluid are also seen. (b) Pancreatic ductography through a pancreatic drainage tube shows leakage of contrast media into the peritoneal cavity (short arrows)
Pancreatic malignancy rarely presents as splenic rupture; several cases of pancreatic adenocarcinomas, mucinous cystadenocarcinomas, and one case of adenosquamous carcinoma have been reported in the literature (14, 15). Additionally, we observed a case of splenic rupture caused due to non-functioning islet cell carcinoma (Fig. 6). Splenic infarction or ischemia secondary to thrombosis of the splenic vein caused by tumor invasion is regarded as the most important mechanism for the development of splenic rupture (14, 15). The presence of co-existing splenic abscess is likely when the tumor invades directly into the stomach or colon (Fig. 6) (16). On imaging, splenic rupture associated with pancreatic malignancy appears as pancreatic tail masses invading the splenic hilum in conjunction with hemoperitoneum or subcapsular splenic hematoma.

A 75-year-old man with a ruptured splenic abscess caused due to invasion by an islet cell carcinoma of the pancreas. Enhanced axial CT scan shows a large, enhancing mass with an irregular contour (long arrows) in the pancreatic tail invading the stomach and spleen, resulting in splenic infarction (double arrow) and splenic abscess formation (short arrows). Note the presence of pneumoperitoneum (arrowheads) and peritoneal fluid (not shown). The splenic abscess is assumed to be formed due to gastric invasion by islet cell carcinoma followed by rupture of splenic abscess, eventually leading to panperitonitis
Splenic rupture is associated with splenic neoplasms including metastasis from various primary malignancies, hamartoma, lymphoma, leukemia, and angiosarcoma (2, 14).
Gallbladder
In patients with gallbladder tumors, perforation of the gallbladder wall develops in one of the following two patterns. The first pattern is due to perforation of the tumor itself, and is extremely rare; we found only one case in which perforation occurred at the site of papillary adenocarcinoma of the gallbladder (17). The more common pattern is due to gallbladder perforation away from the tumor site. In the latter situation, acute cholecystitis with gangrenous change and necrosis of the gallbladder wall develops as a result of gallbladder outlet obstruction by a tumor (17). In a population-based study, the percentage of gallbladder cancer co-existing with acute cholecystitis was 2.3% among patients with acute cholecystitis managed with cholecystectomy, and the most common type of gallbladder cancer was adenocarcinoma (90.5%) (18).
Patients presenting with acute cholecystitis should be carefully examined with imaging for enhancing focal wall thickening or nodular lesion obstructing the gallbladder lumen, especially in the proximal portion of the gallbladder (Fig. 7). However, severe inflammatory changes in/around the gallbladder induced by perforation often make it difficult to detect an underlying gallbladder cancer preoperatively (Fig. 8). In addition, since gallbladder cancer patients presenting with acute cholecystitis are older (about 10 years older) than patients presenting with acute cholecystitis but without gallbladder cancer, radiologists need to be more cautious about interpretation of imaging in older patients who present with acute cholecystitis (18).

A 78-year-old man with gallbladder perforation due to gallbladder adenocarcinoma (courtesy of Dr Keum Nahn Jee from Dankook University Hospital). Coronal reformatted image shows an enhancing polypoid mass in the gallbladder neck portion (long arrows), pericholecystic fat infiltration (short arrows), and pericholecystic fluid (arrowheads). Also, note the presence of stones in the extrahepatic bile duct (thin arrows)

A 70-year-old man with a perforated gallbladder adenocarcinoma. Coronal reformatted images show wall thickening and luminal narrowing of the gallbladder (long arrows). Note the presence of low-attenuation masses invading the liver (arrowheads) and pericholecystic fat infiltration (short arrows). During surgery, a 5-cm in size gallbladder mass and perforation of the gallbladder wall were identified. However, a cholecystectomy was not performed due to the presence of severe adhesion to the liver and omentum. Adenocarcinoma was confirmed with intraoperative biopsies of the gallbladder and hepatic lesions
Adrenal gland
Spontaneous rupture of various adrenal gland tumors including myelolipomas, pheochromocytomas, adrenocortical carcinomas, adenomas, and metastatic tumors has been reported (19–23).
Although the precise mechanisms for the development of spontaneous rupture of adrenal tumors are not clear, many cases of rupture occurred in larger tumors, exceeding 10 cm in size with or without tumor necrosis (19–22). Moreover, a considerable number of ruptured tumors tend to be non-functional, and present with acute abdominal pain (19, 21, 22). Therefore, it is assumed that as the non-functional tumors grow without causing symptoms, tumors tend to undergo necrosis which can increase the risk of rupture.
On imaging, a hematoma is located in or around the adrenal mass within the perirenal space. The presence of fat attenuation (−30 to −115 HU) in the adrenal mass is an important characteristic of myelolipoma (Fig. 9) (19). A ruptured pheochromocytoma can appear as a cystic lesion due to extensive cystic or necrotic changes (20). However, a ruptured adrenocortical carcinoma or adenoma also can be seen as a large, heterogeneous mass on imaging, owing to necrosis and hemorrhage (21, 22). The diagnosis of a large ruptured adrenal adenoma is rarely made on imaging because large adrenal tumors are usually regarded as malignant tumors (21, 22). Metastatic involvement of the adrenal gland is not uncommon, whereas a spontaneous rupture of an adrenal metastasis is a rare condition with reports about such events that have been found in cases of lung cancer and HCC (23). The rich sinusoidal blood supply may contribute to hematogeneous metastasis to the adrenal gland (23). Therefore, when spontaneous adrenal hemorrhage is observed in patients with lung cancer or HCC, rupture of the adrenal metastasis should be considered as the possible cause (Fig. 10).

A 53-year-old man with a ruptured adrenal myelolipoma. Coronal reformatted image from enhanced CT shows a small focus of extravasated contrast material (arrowhead) within a suprarenal mass with fat attenuation (long arrows). Also note the presence of intratumoral hemorrhage extending into the perirenal space (small arrows)

A 44-year-old man with a rupture of adrenal metastasis from HCC. (a) Enhanced CT scan shows an ovoid enhanced mass in the right adrenal gland (long arrow). The patient had multiple HCCs. This adrenal lesion was presumed to be a metastasis from HCC because the adrenal mass was newly developed with enhancement patterns similar to those of HCCs. Note the enhancing HCC (thin arrow). (b) Enhanced CT scan obtained 1 month later shows the development of right hemoretroperitoneum (short arrows) around a low-attenuation mass in the right adrenal gland (long arrow)
Sometimes, rupture of the adrenal tumor can be mistaken for splenic or renal rupture (21, 22). Therefore, identification of rupture of the adrenal tumor, seen as marginal defect on tumor and an intact renal cortical contour, can aid in the diagnosis of these conditions.
Kidney
In cases of spontaneous perirenal hemorrhage, the most common etiology is renal angiomyolipoma, followed closely by renal cell carcinoma (RCC) (24). Wilms' tumor (nephroblastoma) arises from metanephros (mesodermal precursor of the renal parenchyma), and sometimes rupture of the Wilms' tumor can occur (25, 26).
In angiomyolipomas, tumor growth induces a progressive increase in blood flow to the tumor, resulting in vessel dilatation and subsequent aneurysm formation; therefore, the presence of intratumoral aneurysms >5 mm in size and tumor size >4 cm have been reported as predictors of spontaneous rupture of angiomyolipomas (Fig. 11) (27). Although all ruptured RCCs are not of the papillary subtype, intratumoral necrotic changes frequently found in papillary RCC can cause fragility of the tumor, and can lead to tumor rupture (28). Necrosis and hemorrhage in Wilms' tumors may also be linked to tumor rupture (26).

A 34-year-old man with a ruptured angiomyolipoma of the right kidney. (a) Enhanced CT scan shows a fat-containing mass around the renal pelvis (long arrows) with a large right perirenal hematoma (short arrows). (b) Selective renal angiogram reveals an aneurysm (arrowhead) that was not identified on CT
On CT, ruptured renal tumors appear as heterogeneous soft-tissue masses accompanied by hemorrhage in the perinephric and/or subcapsular area. The renal surface where tumors occur is commonly seen as a cortical defect. The presence of intratumoral fat component is the typical feature of angiomyolipomas (Fig. 11) (24, 27). Owing to tumor necrosis and poor vascularization, papillary RCCs enhance poorly after contrast material injection; sometimes, these tumors can be mistaken for a renal cyst (28). Imaging findings of a Wilms' tumor cannot be distinguished from those of a RCC, especially in adult cases (26). However, careful inspection of images for identification of a soft-tissue mass within the hematoma is critical for making a diagnosis of RCC and Wilms' tumor (Figs. 12 and 13). In patients with right-sided Wilms' tumors, intraperitoneal tumor rupture into the Morrison recess is associated with a significant risk of peritoneal recurrence; peritoneal nodules and intraperitoneal fluid are the imaging findings of intraperitoneal tumor rupture (25). Recent advances in CT technology have improved the detection rate of small renal tumors. Nevertheless, repeat follow-up CT after resorption of perirenal hematoma can enable radiologists to identify a renal mass which was initially obscured by hemorrhage (24).

A 51-year-old woman with a ruptured renal cell carcinoma. Coronal reformatted image from the enhanced scan shows enhanced polypoid lesions in the defect area of the renal parenchyma (long arrows). Note the presence of a perirenal hematoma (short arrows). A ruptured papillary renal cell carcinoma was confirmed pathologically after a nephrectomy was performed
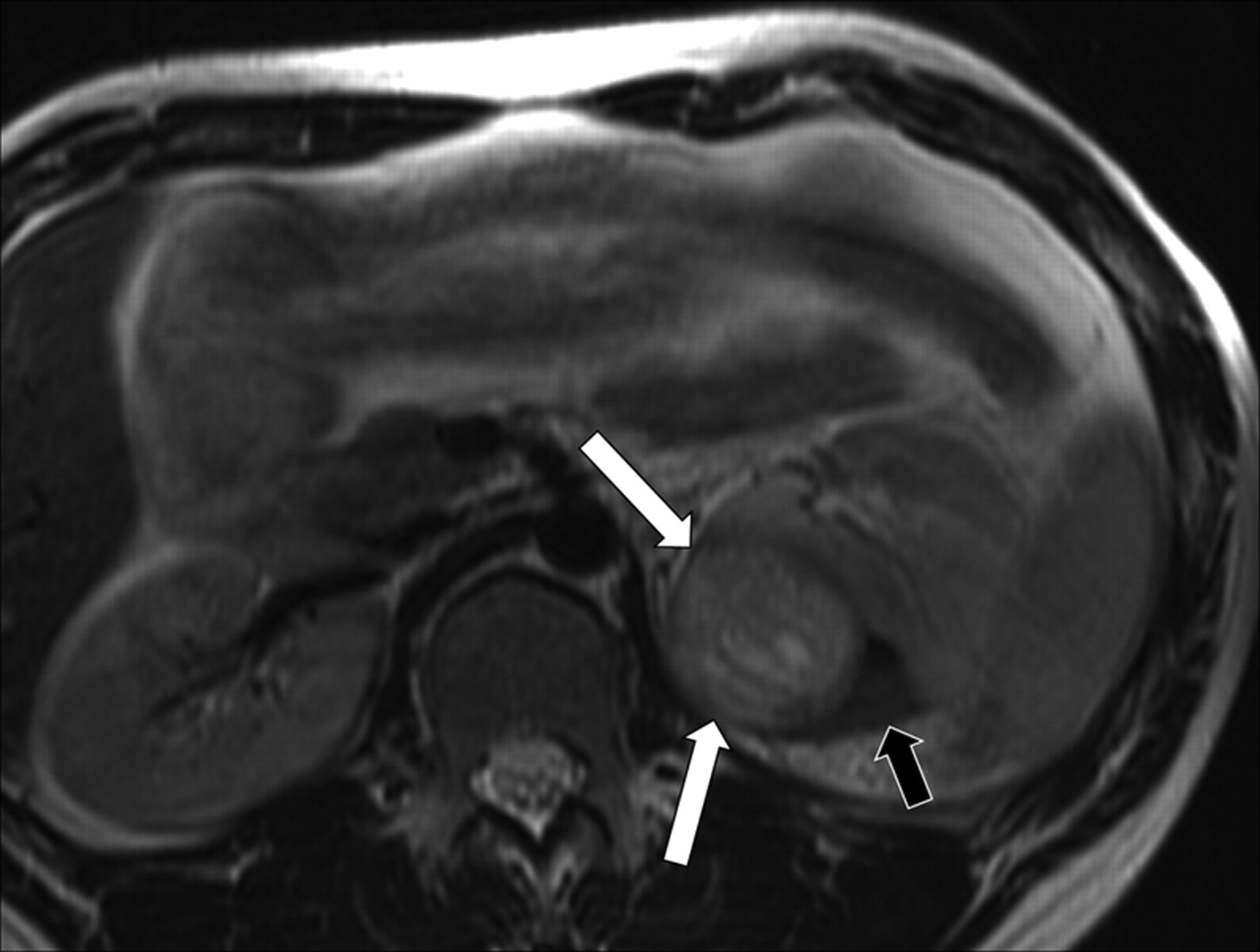
A 19-year-old man with a ruptured Wilms' tumor. Axial T2-weighted MR image shows a mass in the left kidney with a high signal intensity (long arrows) and a subcapsular hematoma with a low signal intensity (short arrow). This mass was confirmed to be a ruptured Wilms' tumor after surgical resection was performed
Uterus
The uterus being a cavitary organ has morphologic features similar to the gallbladder; therefore, two patterns of rupture or perforation related to tumors can occur in the uterus like in the gallbladder. First, the uterine cervix can be obstructed by leiomyoma or cervical carcinoma, resulting in an accumulation of purulent material in the uterine cavity (pyometra). Accumulation of purulent material leads to thinning of the uterine walls which can predispose to the development of spontaneous uterine perforation (29, 30). Five cases of ruptured pyometra in cervical cancer have been reported in the literature (30). Ruptured uterine leiomyomas/leiomyosarcomas presenting as hemoperitoneum is the second pattern of rupture (31–33). Various degenerative changes including hyaline, cystic, and red degeneration as well as necrotic changes in leiomyomas can be the causes of rupture (31). In cases of leiomyosarcomas, tumor necrosis is presumed to be responsible for the rupture (32).
It may be difficult to make a correct preoperative diagnosis of pyometra using imaging modalities. A fluid-filled uterus with a focal defect in the wall is the hallmark of a perforated pyometra (Fig. 14) (29, 30). Perforation frequently occurs in the uterine fundus (30). Fluid collection accompanied by findings of peritonitis such as fat stranding and pneumoperitoneum can be observed (29, 30). More importantly, careful inspection of the uterine cervix for the presence of an obstructing lesion is necessary during interpretation of images of a perforated pyometra in elderly postmenopausal patients in order to exclude obstructing cervical masses. In CT findings of ruptured leiomyomas and leiomyosarcomas, large low-attenuating masses with a paucity of contrast enhancement due to degeneration or necrosis show a focal wall defect and hemoperitoneum (Fig. 15) (31). Sometimes, a hemorrhagic component secondary to thrombotic occlusion and infarction can be seen in ruptured uterine leiomyosarcomas (Fig. 15) (33).

A 77-year-old woman with a perforated pyometra. Enhanced sagittal reformatted image shows a fluid-filled uterus (long arrow) and passage of endometrial fluid into the peritoneal space (short arrows) through a defect (arrowhead) in the uterine wall. A hysterectomy specimen revealed a perforated pyometra induced by endometritis. Presence of a cervical tumor was not seen

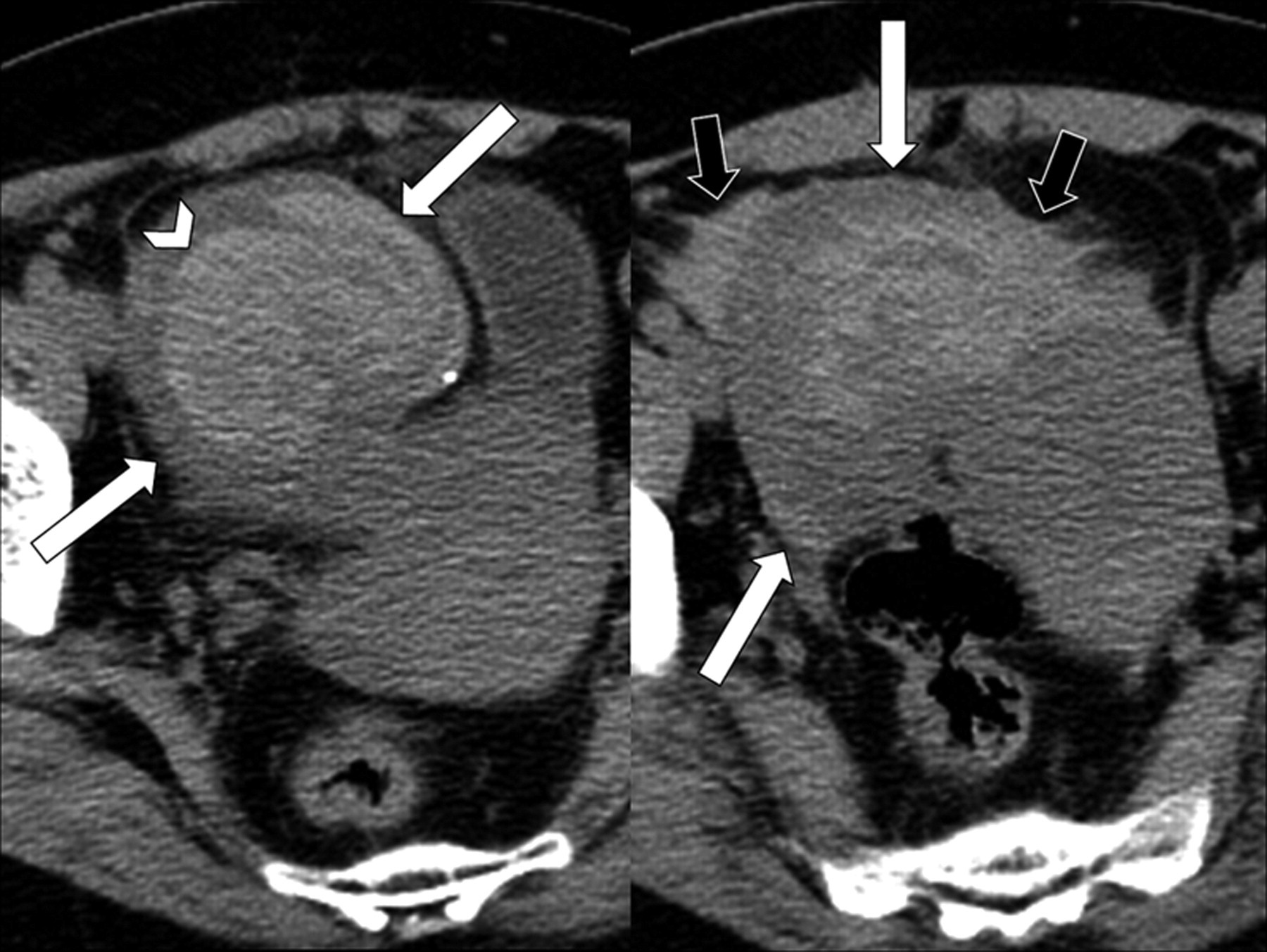
A 54-year-old woman with a ruptured uterine leiomyosarcoma. Pre-contrast CT scan (left) shows a large, solid, and cystic mass (long arrows) with hyperdense hemorrhagic components (arrowhead) in the uterus. Note the presence of peritoneal fluid (short arrow). Coronal reformatted image from an enhanced CT (right) shows a large, solid, and cystic mass (long arrows) with a focal defect in the left lateral wall (thin arrow). Note the presence of a large amount of peritoneal fluid (hemoperitoneum) (short arrow). This mass was confirmed to be a ruptured leiomyosarcoma with cystic and hemorrhagic components after a hysterectomy was performed
Ovary
The most common cause for spontaneous hemoperitoneum due to ovarian masses is the rupture of an ovarian cyst (34, 35). Therefore, the rupture of ovarian tumors in which cystic components are frequently found, is theoretically possible. In cases of teratomas and granulosa cell tumors (GCTs), rupture can occur occasionally, and the incidence of rupture in teratomas has been reported to be 1–4% and that in GCTs to be 10–35% (36, 37).
Teratomas, which consist of mature or immature tissue originating from the three germ cell layers, can rupture with leakage of the sebaceous material into the peritoneum, eventually causing peritonitis (36). On imaging, ruptured teratomas can be suggested by the presence of high-density ascites and a distorted contour of the tumor in addition to the findings of peritonitis such as omental infiltration (Fig. 16) (36). GCTs arise from the sex-cord stromal cells of the ovary and are estrogen-producing tumors. Although GCTs most commonly present with abnormal uterine bleeding, more than 10% of patients are first examined for acute abdomen secondary to rupture (37). Imaging findings of GCTs vary widely, ranging from solid masses to unilocular or multilocular cystic lesions; the pattern of a solid mass with cystic components has also been observed (37, 38). Interestingly, evidence of hemorrhage has been reported in 60–71% of GCT cases and it is a characteristic finding (37, 38). Ruptured GCTs may contain hemorrhagic components and they can be diagnosed when hemoperitoneum is observed on imaging (Fig. 17). Prognosis of ruptured GCTs is less favorable compared to that of intact tumors (37).

A 17-year-old woman with a ruptured teratoma of the right ovary. Axial CT scan shows a large, lobulated mass (long arrows) containing intratumoral fat and calcifications in the pelvic cavity. Focal fat infiltration and fluid (short arrows) are seen around the mass. This mass was pathologically confirmed to be a ruptured mature cystic teratoma
A 52-year-old woman with a ruptured granulosa cell tumor of the right ovary. Pre-contrast CT images show a well-defined, cystic mass (long arrows) with an internal hemorrhagic portion (arrowhead on left image) in the pelvic cavity. This hemorrhagic component did not show contrast enhancement on the enhanced scan (not shown). High-attenuation fluid representing hemoperitoneum (short arrows on the right image) is seen around the mass (long arrows). The mass was pathologically confirmed to be a ruptured granulosa cell tumor arising in the right ovary
Discussion
The majority of ruptured tumors that have been described above are rarely encountered in our daily practice. Moreover, a variety of extremely rare cases of ruptured tumors have been reported in the literature. In this section, we briefly discuss the other rare cases of ruptured tumors.
Cases of ruptured hepatic angiomyolipoma and hepatic epithelioid hemangioendothelioma have been reported in the literature (39, 40). A ruptured angiomyolipoma appears as a large, exophytic mass containing fat density and soft-tissue density portions (39). A ruptured epithelioid hemangioendothelioma has an appearance similar to that of a hemangioma, appearing as peripheral nodular enhancement with delayed centripetal enhancement (40). In these two cases, hypervascular components of the masses might be considered as the cause of spontaneous rupture. Similarly, primary angiosarcoma of the liver can present with rupture (2).
Rare cases of ruptured solid pseudopapillary tumor, islet cell tumor, and mucinous cystadenocarcinomas of the pancreas have been reported (41–43). In solid pseudopapillary tumor, necrosis and hemorrhage are found frequently, and eight cases (2.7%) of ruptured solid pseudopapillary tumors have been reported in the literature until 1994 (41). A few cases of islet cell tumor rupture have been found; they present as an enhanced solid mass or a large cystic mass (42). In pregnant women, tumor activity may be increased during pregnancy and pregnancy may precipitate rupture of the mucinous cystic neoplasms of the pancreas due to hormonal dependency of the tumors (43).
Very rare cases of ruptured multilocular cystic nephroma and renal angiosarcoma have been reported in the literature (44, 45). However, the imaging findings are non-specific and include a cystic mass containing a hemorrhagic component and a perirenal hematoma, respectively.
Cases of ruptured cystic ovarian tumors have mainly been observed, even though rupture of solid ovarian tumors can occur. Several cases of ruptured ovarian tumors including cystadenoma/cystadenocarcinoma, endometrioid carcinoma, Sertoli cell tumor, and metastatic tumors have been sporadically reported (34, 35, 46, 47). Rapid tumor growth, trauma, sudden increase in intra-abdominal pressure, and torsion are known to be the contributing factors for rupture (34). Sometimes, ruptured tumors may show hemorrhage into cystic lesions presenting as a fluid-fluid level on imaging (35).
In the earlier sections, we described a variety of ruptured tumors, with a main focus on CT imaging findings. However, in many cases of acute abdomen, ultrasonography has played the role of the primary imaging modality, especially in patients with suspected gynecologic diseases (2). For an ultrasonographic diagnosis, the detection of hemoperitoneum or hemoretroperitoneum may be the most important finding of ruptured tumors. Hemoperitoneum appears as echogenic fluid mainly located in the hepatorenal fossa, paracolic gutters and pelvic cul-de-sac (2, 48). Moreover, ultrasonography has been reported to be an excellent modality for visualization of hemoperitoneum, with a sensitivity of 63–99% (49). Perinephric or subcapsular renal hemorrhage is a usual finding of ruptured renal tumors as demonstrated by ultrasonography (24, 28). Although ultrasonographic identification of a ruptured tumor itself may be possible in some cases and is usually depicted as a non-specific complex heterogeneous mass, however it would be more difficult than identification of hemorrhage. However, recent advances in sonographic contrast agents may help in detection of ruptured tumors as well as hemorrhage, as can be observed in the improved detection of traumatic abdominal solid organ injuries (49). Although magnetic resonance (MR) is not frequently used as the first-line imaging technique for the evaluation of hemoperitoneum/hemoretroperitoneum, MR imaging is an excellent method for discriminating an underlying mass from a hematoma as was seen in our case (Fig. 13) (2).
Conclusion
Tumor rupture is a rare phenomenon in the majority of tumors. The detection of an underlying tumor becomes challenging due to hemorrhage or inflammation which develops after tumor rupture. A wide spectrum of tumors arising in various abdominal and pelvic organs can present with rupture. A number of these tumors exhibit characteristic findings on imaging that allow an accurate diagnosis of the underlying cause of rupture. Recognition of the causative tumors along with imaging findings and characteristic patterns of rupture will facilitate a prompt diagnosis and effective treatment.