
Abstract
Background
Although the screening of small, flat polyps is clinically important, the role of CT colonography (CTC) screening in their detection has not been thoroughly investigated.
Purpose
To evaluate the detection capability and usefulness of CTC in the screening of flat and polypoid lesions by comparing CTC with optic colonoscopy findings as the gold standard.
Material and Methods
We evaluated the CTC detection capability for flat colorectal polyps with a flat surface and a height not exceeding 3 mm (n = 42) by comparing to conventional polypoid lesions (n = 418) according to the polyp diameter. Four types of reconstruction images including multiplanar reconstruction, volume rendering, virtual gross pathology, and virtual endoscopic images were used for visual analysis. We compared the abilities of the four reconstructions for polyp visualization.
Results
Detection sensitivity for flat polyps was 31.3%, 44.4%, and 87.5% for lesions measuring 2–3 mm, 4–5 mm, and ≥6 mm, respectively; the corresponding sensitivity for polypoid lesions was 47.6%, 79.0%, and 91.7%. The overall sensitivity for flat lesions (47.6%) was significantly lower than polypoid lesions (64.1%). Virtual endoscopic imaging showed best visualization among the four reconstructions. Colon cancers were detected in eight patients by optic colonoscopy, and CTC detected colon cancers in all eight patients.
Conclusion
CTC using 64-row multidetector CT is useful for colon cancer screening to detect colorectal polyps while the detection of small, flat lesions is still challenging.
Keywords
Colorectal cancer, the second most common malignancy in the United States and Europe, is preventable if detected early at screening examinations (1, 2). The 5-year survival rate is 92% for patients with stage I colorectal cancer; in the presence of distant metastasis it decreases to less than 10% (3). While optical colonoscopy is the preferred method for colorectal cancer screening, it is invasive and inconvenient. The last decade has seen an increase in the use of multidetector CT colonography (CTC) for the non-invasive detection and evaluation of colorectal polyps (4–6) and positive health outcomes have been reported (7). CTC is a preferred option in the joint guidelines for colorectal cancer screening (8) and a meta-analysis that included 24 studies demonstrated a per-patient average sensitivity and specificity of 93% and 97%, respectively, for large polyps (>10 mm) (9).
In patients with colorectal neoplasms, flat lesions and laterally spreading tumors have been reported as relatively common and the incidence of flat lesions was approximately 10% in patients with advanced neoplasia (10, 11). Although the detection of small, flat polyps is clinically important and presents a challenge for colorectal cancer screening, the role of CTC screening in their detection has not been thoroughly investigated. Therefore, we evaluated the diagnostic capability and usefulness of CTC in the screening of flat and polypoid lesions by comparing CTC and optic colonoscopy findings.
Material and Methods
This retrospective study was approved by our institutional review board; patient informed consent was waived.
Patient population
Of 380 patients who underwent colorectal cancer screening at our institution between 2009 and 2010, for this study we enrolled 351 (236 men, 115 women) who underwent CTC and optic colonoscopy on the same day. Their age ranged from 25–79 years (average 51.4 ± 10.5 years). The target lesions were polyps of 2 mm or more in diameter that were detected by colonoscopy. Our Institutional Review Board approved the study and all patients gave written informed consent to undergo CTC study that exposed them to X-rays and required the injection of an antispasmodic agent immediately before CTC.
All patients underwent bowel preparation on the day of the examinations. It involved the administration of a bowel-cleansing agent (1600 mL of polyethylene glycol) followed by a 400 mL mixture of bowel-cleansing agent and water-soluble iodinated contrast medium (sodium and meglumine amidotrizoate) (Gastrografin, Bayer, Tokyo, Japan). In addition, a water-soluble iodinated contrast medium was administered orally for fecal and fluid tagging. In our institution, the CT and optic colonoscopy examination suites were located near to each other. First, the patient underwent optic colonoscopy after the bowel preparation. Immediately after the completion of total optic colonoscopy the patient was transferred to the CT suite and underwent CTC examination. Therefore, the bowel preparation was performed once on the day of the optic colonoscopy and CTC examinations.
Optic colonoscopy protocol
After bowel preparation, we injected an antispasmodic agent (7.5 mg, Sesden; Mitsubishi Tanabe Pharma, Osaka, Japan) intramuscularly (i.m.) 10 min before colonoscopy and a sedative (7.5 mg, Horizon; Astellas Pharma, Tokyo, Japan) intravenously (i.v.) just before the colonoscopy. A board-certified endoscopist who had performed more than 5000 colonoscopies carried out the optic colonoscopy. The colonoscope (EC-590MP, EC-450WM5; Fujinon Toshiba, Tokyo, Japan) was first advanced into the cecum and then withdrawn toward the anus while checking for polyps in each colorectal region. Findings on the region and the size and macroscopic morphology of polyps were recorded on a designated form. The size of the polyps was measured with biopsy forceps inserted via the forceps channel, with the forceps pressed against the polyps closed (2 mm in diameter) and open (5 mm in diameter). Biopsy specimens were obtained of polyps measuring ≥6 mm in diameter and of polyps characterized as depressed plaques measuring ≤5 mm in diameter.
CTC protocol
The patient was placed on the imaging table in the left lateral decubitus position. To suppress intestinal peristalsis we injected another dose of an antispasmodic agent (i.m.) prior to CTC data acquisition. Rectal examination was performed to check for anal lesions, and a 21-F Nelaton catheter was introduced via the anus for insufflation. The insufflated bulb was not used with the Nelaton rectal catheter due to the cost. Carbon dioxide was administered with the patient in the left lateral decubitus or prone position using an automatic insufflator with a pressure measurement function. Average volume of carbon dioxide used for optimal bowel distension was 1958 ± 983 mL, and no complications were observed. After a scout radiograph was obtained to confirm sufficient dilation of the colon, CT images were obtained on a 64-row multidetector CT system (Aquilion 64; Toshiba, Tokyo, Japan) during 7–10 s breath-holding under expiration in the prone and supine position. The scan range extended from the diaphragm to the inferior edge of the pubis in both positions. The data acquisition protocol was: tube voltage 120 kV, tube current 100 mA, gantry rotation speed 0.5 s/rotation, slice thickness 0.5 mm, field-of-view 320 mm, beam pitch 0.83. The CT dose index was 5.7 mGy per position in our study, and our CTC protocol was considered a low-dose protocol according to the American College of Radiology guidelines (12). The mean range of data acquisition was 455 ± 29 mm. CT images reconstructed at a 0.5-mm slice thickness with 0.5-mm intervals were transferred to an image workstation (ZIO Station System N610 version 1.21b; Amin, Tokyo, Japan), and the images including multiplanar reconstruction (MPR), volume rendering (VR), dissected colon (virtual gross pathology [VGP]), and virtual endoscopic (VE) images were generated.
Image interpretation
Two experienced physicians (a board-certified radiologist and a gastroenterologist qualified as supervising physician), blinded to clinical data, interpreted the CTC images by consensus. The colon was divided into five regions: the ascending colon (including the cecum); the transverse colon; descending colon; sigmoid colon; and the rectum. The VR images were evaluated to check for insufficient dilation, wall deformation, and mucosal irregularities (Fig. 1). The VGP images were then used to identify regions harboring suspected lesions (Fig. 2). Dissected colon images were checked for polypoid lesions and morphological abnormalities by inspecting the image of each semilunar fold. All regions with suspected lesions were re-checked and then evaluated in the diagnosis-confirmation mode where regions with suspected lesions were inspected on VE and MPR images. In addition, the VE images were observed from two directions (from the oral and from the anal end of the colon) to check for lesions. When a suspected lesion was found, the region including the suspected lesion was checked again on the VGP image. The final diagnosis was based on findings identified on VE, VGP, and MPR images obtained in the prone and supine position. The region, size, and macroscopic morphological characteristics of each lesion were recorded. Findings on CTC images for lesions measuring ≥2 mm in diameter were compared with findings made by total optic colonoscopy as the gold standard. The sensitivity, specificity, and positive- and negative predictive value (PPV and NPV, respectively) per patient for polyps (>2 mm) were calculated in each region of colon (ascending, transverse, descending, sigmoid colon, and rectum). The reasons for missed lesions at CTC were assessed and classified as follows: invisible due to limitations of CTC (lack of spatial resolusion); inadequate bowel preparation; inadequate bowel distention; or misinterpretation of the observer. Furthermore, we visually evaluated which of the four reconstruction modes (MPR, VR, VGP, or VE) was appropriate for detection of flat and polypoid lesions on a 3-point scale: 3 = valuable, the lesion was easily and correctly detected; 2 = acceptable, the lesion was detected, but the detection was not easy; 1 = non-valuable, the lesion was difficult to detect.
Volume rendering method to check for insufficient dilation, wall deformation, and mucosal irregularities Virtual gross pathology image is used to identify regions harboring suspected lesions (arrow)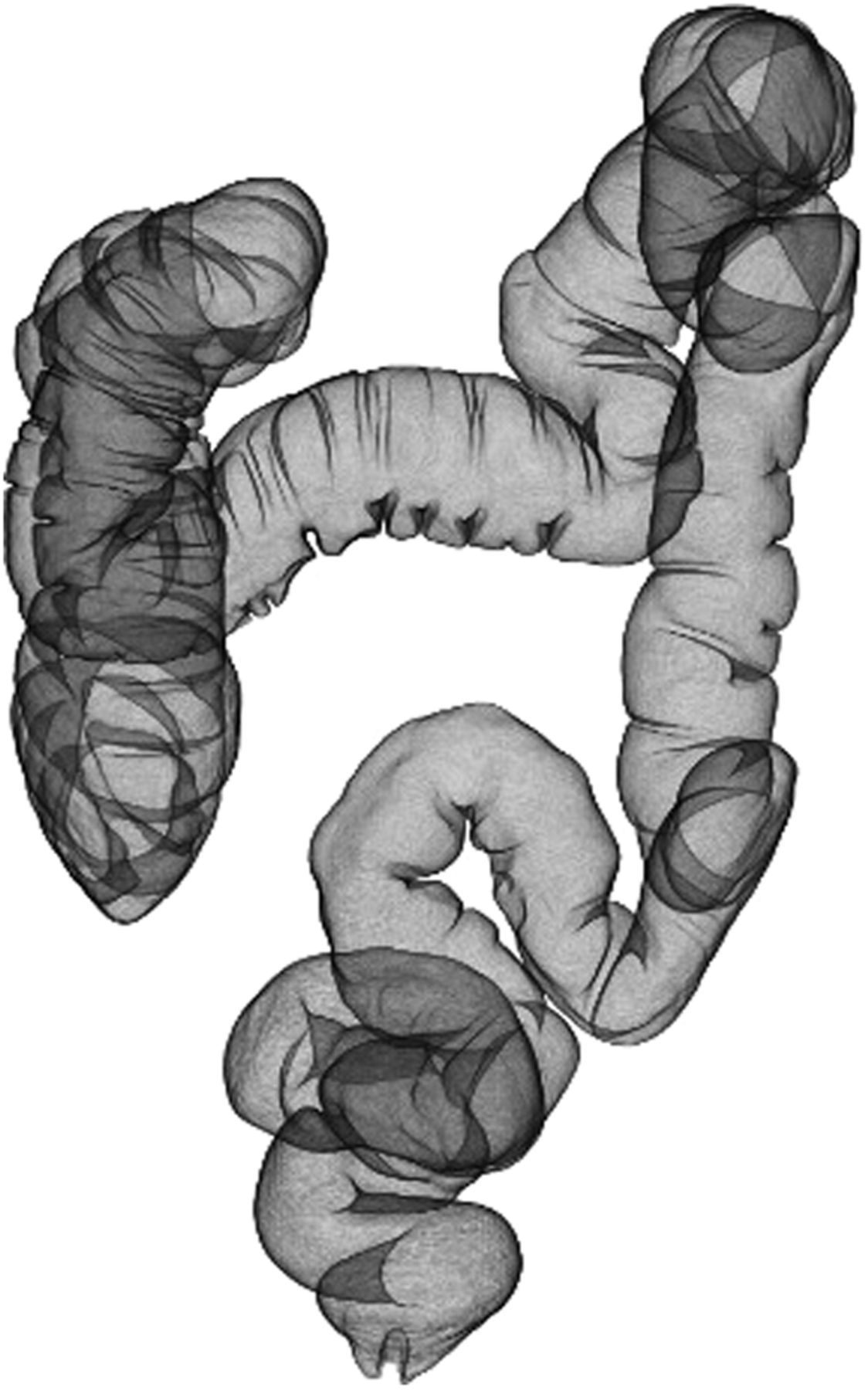

The lesions were classified into three groups based on size, i.e. 2–3 mm, 4–5 mm, and ≥6 mm. The maximum diameter of the lesion was measured on MPR images. Based on their macroscopic morphological characteristics, the lesions were first classified as flat or polypoid. The definition of flat lesions included mucosal elevation with a flat surface and a height not exceeding 3 mm (13, 14). Polypoid lesions were further classified as sessile, sessile-pedunculated (semipedunculated), and pedunculated. The detection sensitivity per lesion was evaluated based on its size and macroscopic morphological characteristics.
Statistical analysis
Statistical analysis was with the chi-square test to compare the detection capability rates among colon regions and the detection rates on CTC of flat and polypoid lesions. A P value of <0.05 was considered statistically significant. The results of visual evaluation of four reconstruction modes were compared with the Steel-Dwass test. We used software for statistical analysis (SPSS version 15.0; SPSS Inc., Chicago, IL, USA; and JMP 9.0.2; SAS Institute Inc., Cary, NC, USA).
Results
A total of 460 polyps measuring ≥2 mm in diameter were found in 209 of the 351 patients on optic colonoscopy; cancers were detected in eight patients. Of the 460 lesions: 243 (52.8%) measured 2–3 mm, 137 (29.8%) were 4–5 mm, and 80 (17.4%) measured ≥6 mm. Histopathologic study of biopsy or surgical specimens from 105 patients (135 lesions) returned a final diagnosis of hyperplastic polyps (9 lesions, 9 patients), tubular adenoma (118 lesions, 90 patients), and adenocarcinoma (8 lesions, 6 patients).
Capability of CTC for detecting colorectal polyps per patient
Detection capability rates of CTC in each region of the colon
*The cecum is included in the ascending colon
NPV, negative predictive value; PPV, positive predictive value
Detection rates per lesion based on the lesion size
The polyp detection rate was 46.5% (113/243), 74.5% (102/137), and 91.3% (73/80) for lesions measuring 2–3 mm, 4–5 mm, and ≥6 mm, respectively. It was significantly higher for polyps measuring ≥6 mm than for smaller lesions (P <0.01).
Detection rates per lesion based on morphological characteristics
Comparison of detection rates between flat and polypoid lesions for different size ranges
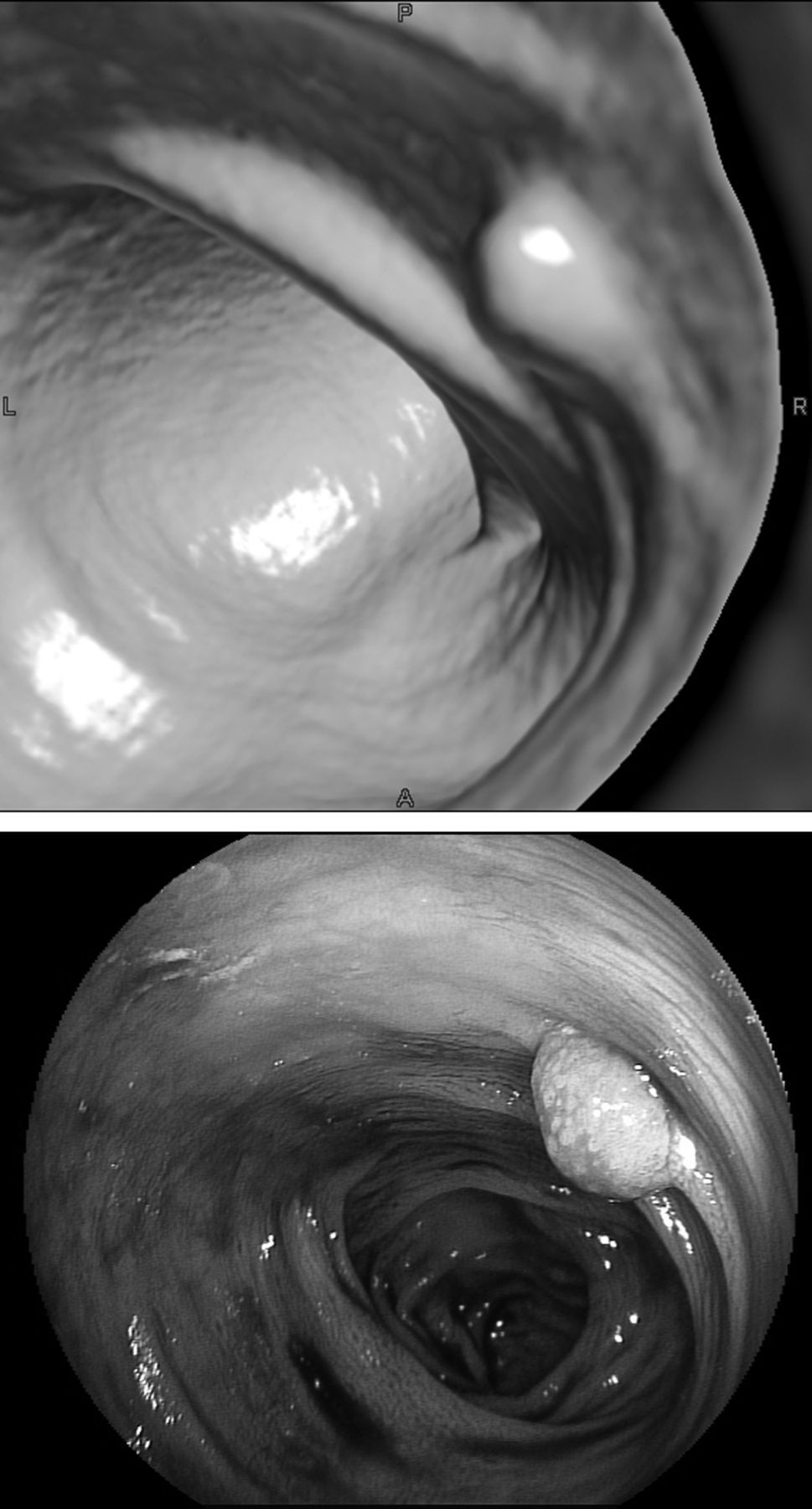
A 41-year-old woman with polyp in sigmoid colon. Virtual endoscopy image (a) shows polypoid lesion measuring 5 mm. This coincides with optic colonoscopy finding (b)
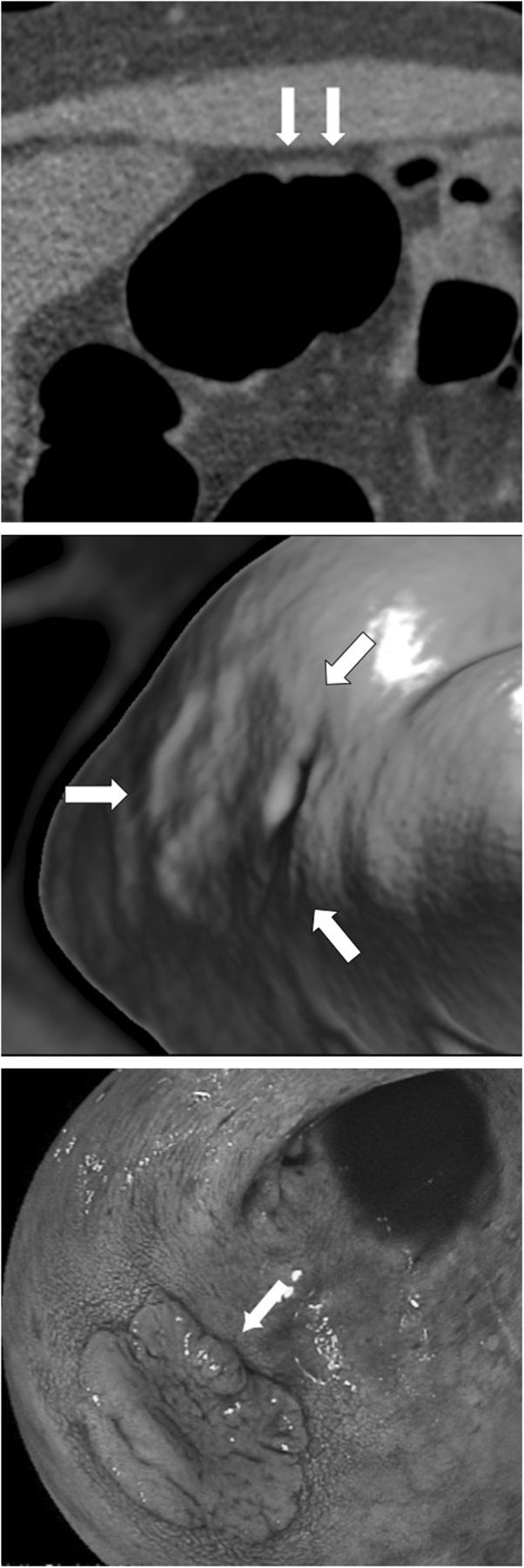
A 54-year-old woman with flat polyp in descending colon. MPR image (a) shows flat lesion of uniform soft tissue density (arrows). Virtual endoscopy image (b) shows flat lesion (arrows). This coincides with optic endoscopy (arrow) (c). Histopathological examination confirmed that lesion was carcinoma in adenoma
Evaluation of the 22 flat lesions missed at CTC
Evaluation of the 150 polypoid lesions missed at CTC
Visual evaluation of four different reconstructions
Degree of polyp visualization with four reconstruction modes at CTC
Score 3, valuable; 2, acceptable; 1, non-valuable
MPR, multiplanar reconstruction; VE, virtual endoscopy; VGP, virtual gross pathology; VR, volume rendering
Multiple comparisons of polyp visulalization among four reconstruction methods
MPR, multiplanar reconstruction; NS, not significant; S, significant; VE, virtual endoscopy; VGP, virtual gross pathology; VR, volume rendering
Discussion
As most colorectal cancers are thought to develop from adenomatous polyps (11), screening for early-stage cancer and pre-neoplastic lesions can significantly improve disease outcomes. Automated colonic insufflation and fecal tagging are advances in CTC and in average-risk populations, CTC performed every 5 years may be a reasonable alternative for the screening suggested by the joint guidelines issued by three medical societies of the United States (8). As the reported sensitivity and specificity of CTC for the detection of adenomas or cancers measuring >10 mm were 90% and 86%, respectively, its diagnostic capability is sufficiently high for screening an average-risk population (6). However, the detection of flat polyps is important at colorectal cancer screening because small flat lesions are more likely to be stage T3/T4 than polypoid lesions that tend to be stage T1 (15). In our study the detection sensitivity for flat polyps (>2 mm) was 47.6%, for polypoid lesions it was 64.1%. Although the detection of flat polyps by CTC is compromised by the lack of direct mucosal visualization, this disadvantage may be overcome by techniques such as bowel preparation and colonic distension. According to Ignjatovic et al. (11) routine fecal tagging lowered the examination failure rate from 4% to <1%.
In different colon regions, both the sensitivity and specificity of CTC were relatively high and we observed no significant regional differences. Our findings were comparable to findings reported previously (9, 16, 17) and the quality of our CTC images was excellent although optic colonoscopy and CTC were performed on the same day. We carried out total optic colonoscopy before CTC and suctioned residual liquid in the colon during colonoscopy, the conditions for CTC were therefore optimal as the effects of residual liquid were markedly reduced.
In most previous studies on the detection of polyps at CTC (5, 7, 18–21), the polyps were classified into three categories based on their size: ≤5 mm, 6–9 mm, and ≥10 mm. Johnson et al. (6) excluded polyps <5 mm from their assessment. Lieberman et al. (20) reported that 1.7%, 6.6%, and 30.6% of polyps measuring 1–5 mm, 6–9 mm, and ≥10 mm, respectively, were associated with advanced neoplasia. Our search of the literature found no studies in which polyps measuring ≤5 mm were stratified based on their size for evaluation. These lesions may be very small screening targets and their natural history remains to be elucidated (20). We subclassified small polyps to determine whether lesions ≤5 mm can be detected by CTC. We found that sensitivity was 46.5% and 74.5% for polyps measuring 2–3 mm and 4–5 mm, respectively. Due to the thin-slice collimation of 64-row multidetector CT systems and the establishment of optimal conditions by careful bowel preparation, 56.6% of all lesions ≤5 mm were detected. Consequently, we consider the sensitivity of CTC for such small lesions acceptable. Our results document that 91.3% of polyps measuring ≥6 mm, the targets for treatment and detailed examination, can be detected at CTC screening.
The adenoma-carcinoma pathway is thought to be involved in approximately two-thirds of all colorectal cancers (11, 22, 23). Another growth pattern of de novo cancers, in which superficial flat tumors progress to infiltrating cancers, is encountered in clinical practice (24, 25). Among superficial flat tumors, depressed tumors account for approximately 15.5% of all infiltrating cancers. As polyps measuring ≤5 mm tend to infiltrate the submucosal layer and most polyps measuring ≥10 mm infiltrate this layer massively, depressed tumors have drawn interest (11). We found that by CTC it may be possible to detect small and flat lesions although their identification continues to present challenges. To improve their detection rate, the spatial resolution and the performance of fecal tagging and electric cleansing must be improved. In addition, the development of high-precision computer-aided detection methods that facilitate the detection of small height differences and of tylosis of the intestinal wall is desirable.
Our study has some limitations. First, not all polyps were examined histopathologically. Second, we did not record the time needed for image interpretation. The interpretation of CTC images are usually time-consuming, and it should be clarified which mode of CTC image reconstruction is most time-effective in the future studies. Third, since CTC was performed immediately after colonoscopy, the conditions were optimal as there was almost no residual liquid or solid matter in the colon. When only CTC images are acquired, their interpretation will be performed under less favorable conditions due to the presence of larger amounts of residual liquid and solid matter in the colon. This may lower the detection rate. Nonetheless, lesions measuring at least 6 mm, the targets for treatment and detailed examination, can be detected by CTC, rendering this method useful for colon cancer screening. Improvements in the spatial resolution of CTC images and detailed evaluation will facilitate the detection of smaller lesions. Efforts are underway in our laboratory to improve the detection of superficial flat tumors with small height differences.
In conclusion, CTC using 64-row multidetector CT is useful for colon cancer screening to detect lesions measuring 6 mm or more although small, flat lesions are still difficult to detect. The optimization of imaging conditions at CTC may make it possible to detect small, flat lesions.