
Abstract
Background
No report has appeared on the histologic characteristics as influencing factors associated with clinical outcomes and survival of patients who underwent percutaneous biliary interventions to treat malignant biliary obstruction caused by metastatic gastric cancer.
Purpose
To investigate the clinical outcomes after percutaneous biliary interventions in patients with malignant biliary obstruction caused by metastatic gastric cancer and to identify prognostic factors associated with clinical outcomes.
Material and Methods
We retrospectively assessed 117 patients who underwent percutaneous transhepatic biliary drainage (PTBD) between January 2005 and December 2009, for treatment of malignant biliary obstructions caused by metastatic gastric cancer. Of these 117 patients, 54 subsequently underwent metallic stent placement.
Results
The technical success rates of PTBD and metallic stent placement were 100% and 100%, respectively. Self-limiting hemobilia after PTBD occurred in eight (7%) patients, and self-limiting hemobilia (n = 4) and acute pancreatitis (n = 3) after stent placement occurred in seven (13%) patients. Successful drainage was achieved in 105 (90%) of the 117 patients who underwent PTBD and in 49 (91%) of 54 patients who underwent metallic stent placement. Multiple Cox's regression analysis showed that the histology of primary gastric cancer (P = 0.011), serum bilirubin after PTBD (P = 0.002) and stenting (P = 0.017), and chemotherapy after PTBD (P < 0.001) and stenting (P = 0.033) were independent predictors of survival.
Conclusion
PTBD and subsequent metallic stent placement were safe and effective methods for palliative treatment in patients with malignant biliary obstruction caused by metastatic gastric cancer. Patients with a differentiated histology of primary gastric cancer and serum bilirubin level ≤2 mg/dl after PTBD are probably the best candidates for treatment with a combination of metallic stent placement and chemotherapy.
Keywords
Malignant biliary obstruction is frequently caused by metastases from stomach, colon, lung, uterine, and breast cancers (1, 2). The incidence of malignant biliary obstruction in patients with metastatic gastric cancer has been reported to range from 1.3% to 2.3% (3–5). Several studies have described radiologic findings of malignant biliary obstruction caused by metastatic gastric cancer (2, 6).
Percutaneous or endoscopic placement of self-expandable metallic stents has become an established palliative treatment in the relief of malignant biliary obstructions (7–9). However, the endoscopic approach is usually difficult in patients who have previously undergone a gastric operation. To the best of our knowledge, reports on the clinical outcomes of patients who underwent percutaneous transhepatic biliary drainage (PTBD) and metallic stent placement to treat malignant biliary obstruction caused by metastatic gastric cancer are both few in number and limited in scope (5, 10–12). Moreover, no report on the histologic characteristics as influencing factors associated with clinical outcomes and survival has appeared. We therefore investigated the clinical outcomes after PTBD and metallic stent placement in 117 patients with malignant biliary obstruction caused by metastatic gastric cancer and to identify prognostic factors associated with clinical outcomes.
Material and Methods
Patient population
Between January 2005 and December 2009, we retrospectively identified 117 consecutive patients with malignant biliary obstructions caused by metastatic gastric cancer. Demographic, clinical, and laboratory data were collected from medical records or from our electronic patient information database. The study protocol was approved by the Institutional Review Board of our institution, which waived any need for informed consent. All patients had histologically proven primary gastric cancer. World Health Organization criteria were use for histological typing of all gastric tumors; signet ring cell carcinoma was considered present when >50% of the tumor consisted of isolated or small groups of malignant cells containing intracytoplasmic mucin (13). The characteristics of the primary gastric cancers in all 117 patients are presented in Table 1 (14).
Demographic and clinical characteristics of 117 patients with primary gastric cancer
*Macroscopic features of gastric cancer were categorized according to the Borrmann classification (14)
Imaging diagnosis
Contrast-enhanced computed tomography (CT) obtained in the portal venous phase and the direct cholangiogram obtained via percutaneous transhepatic biliary drainage catheter for the level and pattern of biliary obstruction were reviewed by the consensus of two radiologists blinded to the histologic results of primary gastric cancer. The levels at which biliary obstruction occurred, as determined by CT and cholangiography, were classified as biliary hilum and biliary non-hilum in nature. Hilar lesions were subclassified according to the Bismuth classification, and non-hilar lesions were divided into those of three segments: the common hepatic duct (CHD) (thus from the biliary hilum to the level of the cystic duct); the upper half of the common bile duct (CBD); and the lower half of the CBD. The cause of biliary obstruction as determined by CT was classified into five types: intraductal metastasis (enhanced ductal wall thickening or mass); periductal lymph node enlargement; periductal seeding mass; extrinsic compression by a metastatic liver mass; and direct invasion by a primary or recurrent cancer.
PTBD and stent placement
No patient underwent endoscopic drainage because of the difficulty associated with this procedure in patients who have undergone gastric operations. Therefore, PTBD and metallic stent placement served as the first-line treatments for patients with malignant biliary obstruction caused by metastatic gastric cancer. The indication for PTBD was malignant biliary obstruction caused by metastatic gastric cancer based on combinations of clinical symptoms such as jaundice, cholangitis, and itching, biochemical data, and the results of CT.
PTBD and metallic stent placement were performed under anesthesia induced by intravenous pethidine hydrochloride (Demerol, Keukdong Pharmaceutics, Seoul, Korea) and intramuscular lidocaine (Jeil Pharmaceuticals, Taegu, Korea). Antibiotics were administered intravenously 24 h before each procedure and for at least 48 h afterwards. The intrahepatic bile duct was punctured using a 21-gauge Chiba needle (Cook, Bloomington, IN, USA), under the guidance of fluoroscopy or ultrasound. Based on standard biliary drainage procedures, an 8.5–10-F biliary drainage catheter (Cook) was initially placed in the intra- or extra-hepatic bile duct. After PTBD, 60 (52%) patients received chemotherapy with various agents. The remaining 57 (48%) patients were not further treated because of advanced age (>76 years), impaired hepatic function (serum total bilirubin >4 mg/dl), poor general condition (Eastern Cooperative Oncology Group [ECOG] performance status grade 3–4), or patient refusal.
Fifty-four patients received a total of 66 metallic stents, of four types, 0–39 days after PTBD (median 10 days). The remaining 63 patients did not undergo biliary stent placement because of unsuccessful drainage after PTBD, poor general health status (ECOG performance status grade 3–4), or the presence of extensive extrabiliary metastases. We used commercially available uncovered stents (Zilver, Cook; Sentinol, Boston Scientific, Galway, Ireland) or polytetrafluoroethylene-covered (Hercules, S&G Biotech, Seongnam, Gyunggi, Korea; GD stent, TaeWoong Medical, Kimpo, Korea) metallic stents; stent choice was made by individual physicians according to availability and personal preference. Covered stents were used in 30 patients, and uncovered stents in 24. Patients with non-hilar biliary obstructions underwent unilateral stenting via a single percutaneous site employing single stent insertion, whereas patients with hilar biliary obstructions underwent bilateral stenting via a single percutaneous site employing stent-in-stent deployment in a T configuration.
After stent placement, an 8.5–10-F temporary drainage catheter was left in place for 3–5 days to flush and maintain access to the biliary system. Stent position, expansion, and function were confirmed by cholangiography performed through the catheter. Following documentation of free contrast flow through the stent into the duodenum and a decrease or normalization of serum bilirubin level, the temporary catheter was removed.
Endpoints of PTBD and stent placement
Technical success of stent placement was defined as successful stent deployment in the appropriate position resulting in drainage of the stented bile duct. Complications were classified as major or minor according to the guidelines of the Society of Interventional Radiology Standards of Practice Committee (15). Major complications were defined as those necessitating major therapy, an unplanned increase in the level of care or prolonged hospitalization (>48 h), or permanent adverse sequelae or death. Minor complications were defined as those requiring no or nominal therapy, including overnight admission for observation only. Successful drainage after PTBD was defined as a ≥20% decrease in serum bilirubin level relative to baseline within 1 week (12). Successful internal drainage after stent placement was defined as a decrease in serum bilirubin level to <75% of the pretreatment value within 1 month (16). Patients with stents that remained patent were assumed to experience no increase in serum bilirubin levels and no dilatation of the intrahepatic bile ducts, as shown by ultrasonography or CT during follow-up. Stent patency was defined as the time interval between initial stent placement and recurrence of obstruction. If obstruction was not evident during a patient's life, stent patency was considered equivalent to patient survival. A stent was assumed to be patent at the time of patient death if serial serum bilirubin levels were normal or only mildly increased (<3 mg/dl). If the patient was obviously jaundiced or had higher bilirubin levels, the stent was assumed to be obstructed. Patient survival was defined as the time interval between initial stent placement and patient death or last follow-up. If the patient was alive at the last follow-up, survival was considered equal to follow-up duration.
Statistical analysis
The Mann-Whitney U test was used to compare pairs of independent, continuous variables between the groups. Student's t test was used to compare categorical variables between the groups. Paired-sample t test was used to compare the pre- and post-biliary intervention (PTBD and stenting) serum bilirubin levels. Patient survival after PTBD, stent patency, and patient survival rates after stent placement were calculated according to the Kaplan-Meier method, and differences between curves were analyzed by the log-rank test. The following variables were included in analysis: age; gender; histology; serosal invasion; lymph node metastasis of primary gastric cancer; history of previous gastrectomy; type of metastasis; level of biliary obstruction; serum bilirubin levels after PTBD; metallic stenting after PTBD; and chemotherapy after PTBD. Serum bilirubin levels after PTBD were dichotomized a cut-off point based on statistical significance (a decrease to 0.5–2 mg/dl post-PTBD versus a decrease to ≥4.1 mg/dl). Variables found to be significant by univariate log rank analysis (P < 0.2) were considered candidate variables for multiple analysis, which was performed using the Cox's proportional hazard model. Variables were selected in a stepwise forward selection manner. All statistical analyses were performed using SPSS (version 14.0; SPSS, Chicago, IL, USA). A two-sided P value less than 0.05 was considered statistically significant.
Results
Biliary obstruction: characteristics
Imaging characteristics are summarized in Table 2. Of the 117 patients, 78 (67%) had previously undergone gastrectomy for primary gastric cancer. In such patients, the median interval between previous gastrectomy and onset of biliary obstruction was 26 months (range 1–126 months). The remaining 39 (33%) patients did not undergo gastrectomy because of advanced tumor stage and the presence of extragastric metastases. In such patients, the median interval between diagnosis of primary gastric cancer and onset of biliary obstruction was 6.2 months (range 0.5–28.5 months). The level of biliary obstruction was non-hilar in 78 (67%) patients and hilar in 39 (33%). Of the 78 non-hilar lesions, 39 (33%) were in the upper CBD, 21 (18%) in the entire CBD, 13 (11%) in the lower CBD, and five (4%) in the CHD (Bismuth type 1). Biliary obstructions were caused by intraductal metastases indistinguishable from primary biliary malignancies in 67 (57%) patients and by metastatic lymph nodes in 25 (21%) (Fig. 1). The intraductal metastases of the 67 patients manifested as pure enhanced wall thickening (n = 64) or presence of an intraductal mass (n = 3). The enhanced wall thickening was concentric in 62 patients and eccentric in two patients. Of the 67 patients with intraductal metastases, 41 (61%) had cystic ductal lesions contiguous with the intraductal lesions. In one of these 67 patients, the obstructive process of an intraductal metastasis from recurrent gastric cancer was pathologically confirmed.

A 51-year-old man who underwent subtotal gastrectomy 38 months earlier because of advanced gastric cancer with poorly differentiated adenocarcinoma histology. (a) Contrast-enhanced axial CT image at the level of the upper CBD, showing partially necrotic low-attenuation lymph node in the portocaval space (asterisk); (b) Contrast-enhanced coronal CT image, showing bile duct dilatation proximal to the lymph node (asterisk); (c) Cholangiography after right PTBD, showing the upper CBD obstruction; (d) Cholangiography showing successful placement of a metallic stent (arrows) across the lesion
Imaging characteristics of 117 patients with malignant biliary obstructions caused by metastatic gastric cancer
CBD = common bile duct, CHD = common hepatic duct
PTBD: technical outcomes
The technical success rate of PTBD was 100%. Mean serum bilirubin levels were 10.1 ± 7.1 mg/dl before PTBD and 5.1 ± 4.9 mg/dl 1 week after PTBD (P < 0.001). Successful drainage was achieved in 105 (90%) of the 117 patients. Among the 12 patients for whom internal drainage was unsuccessful, seven showed increases in serum bilirubin levels and five minimal decreases. Successful internal drainage was not associated with patient age, gender, histology of primary gastric cancer, type of metastasis, level of obstruction, or serum bilirubin levels before stenting.
Minor complications occurred in eight (7%) patients, all of whom had self-limiting hemobilia that completely resolved 2–6 days after PTBD, without transfusion. One (1%) patient experienced a major complication, severe hemobilia secondary to a pseudoaneurysm of a right intrahepatic artery, which was successfully treated by selective transarterial embolization.
PTBD: survival analysis
The cut-off date for data analysis was December 31, 2010. During a median follow-up period of 185 days (range 7–1266 days), 110 patients died and seven patients remained alive. The causes of deaths were disease progression (n = 107) and sepsis (n = 3). Thirteen patients (11%) died within 30 days after PTBD. The median survival time after PTBD was 104 days (95% CI 84–123 days).
Univariate log rank analysis showed that the histology of primary gastric cancer (P = 0.119), the level of biliary obstruction (P = 0.074), metallic stenting after PTBD (P = 0.001), serum bilirubin level after PTBD (P < 0.001), and use of chemotherapy after PTBD (P < 0.001) were all associated with patient survival. Multiple Cox's proportional hazard regression analysis showed that the histology of primary gastric cancer (P = 0.011), serum bilirubin level after PTBD (P = 0.002), and use of chemotherapy after PTBD (P < 0.001) were independent predictors of patient survival (Table 3).
Multiple Cox's proportional hazard regression analysis of factors independently associated with survival after PTBD
PTBD = percutaneous transhepatic biliary drainage
Median survival was significantly longer in patients with differentiated histology (115 days; 95% CI 64–166 days) than in those with signet ring cell histology (80 days; 95% CI 44–116 days) (Fig. 2a); in patients with serum bilirubin levels ≤2 mg/dl (172 days; 95% CI 122–222 days) compared to >2 mg/dl (48 days; 95% CI 31–65 days) after PTBD (Fig. 2b); and in patients who received chemotherapy (172 days; 95% CI 111–233 days) compared to those who did not receive chemotherapy after PTBD (55 days; 95% CI 36–74 days) (Fig. 2c).

Multiple Cox's regression analysis of patient survival after PTBD. Kaplan-Meier curves showing patient survival according to (a) primary gastric cancer histology, (b) serum bilirubin level, and (c) use of chemotherapy
Metallic stent placement: outcomes and stent patency analysis
The technical success rate of stent placement was 100%. Mean serum bilirubin levels before and 1 week after stent placement were 5 ± 4.5 mg/dl and 1.8 ± 2.4 mg/dl, respectively (P < 0.001). Successful internal drainage was achieved in 49 (91%) of 54 patients. Among the five patients who did not experience successful internal drainage, one showed an increase and four minimal decreases in serum bilirubin levels. Seven patients (13%) experienced minor complications, including three with self-limiting hemobilia, which resolved completely within 3 days after stent placement and without transfusion, and four who presented with acute pancreatitis and were treated successfully by conservative management over 3–7 days (mean 4 days). However, no patient who underwent stenting experienced major complications.
Median stent patency time was 351 days (95% CI 219–483 days) and cumulative stent patency rates at 3, 6, 9, and 12 months were 95%, 77%, 70%, and 50%, respectively (Fig. 3). Stent occlusion was observed in 13 (24%) patients after a mean of 231 days. In the seven patients who underwent uncovered stent placement and experienced stent occlusion because of tumor ingrowth, six occlusions were caused by intraductal metastases and one patient had an occlusion caused by a periductal metastasis. In the six patients who underwent covered stent placement and experienced stent occlusions, four occlusions were attributable to tumor overgrowth caused by progression of lymph node metastasis, whereas two occlusions were caused by sludge incrustation. Four of the 13 patients with stent occlusion were managed by insertion of more than one additional stent, whereas nine were managed by placement of internal or external drainage catheters, because of rapidly progressing disease and poor general condition. Neither stent patency nor successful internal drainage was associated with any of patient age, gender, histology of primary gastric cancer, type of metastasis, level of obstruction, serum bilirubin level before stenting, use of chemotherapy after stenting, or stent type.
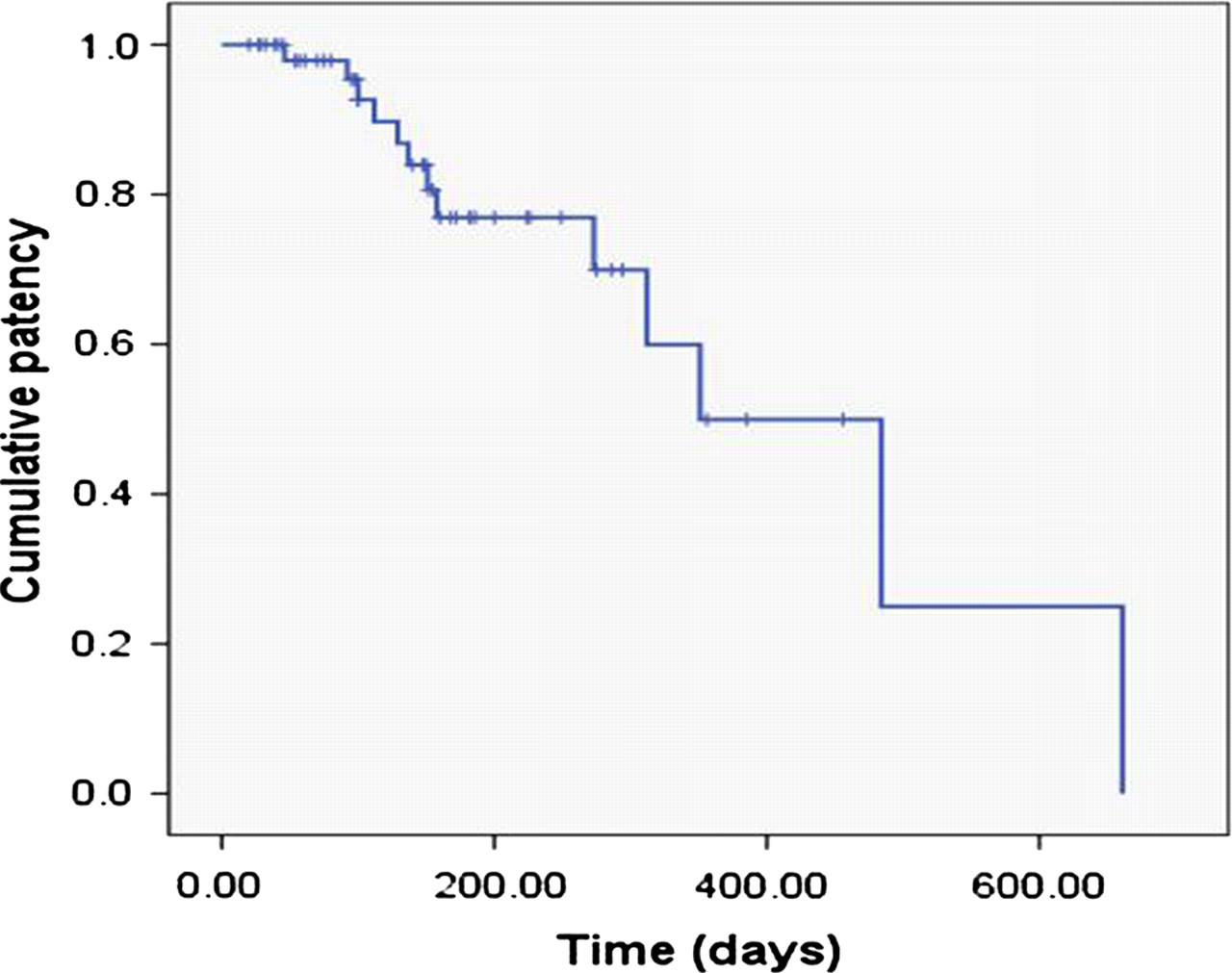
Cumulative stent patency rates by Kaplan-Meier analysis
Metallic stent placement: survival analysis
Univariate log rank analysis showed that serum bilirubin level after stenting (P < 0.001) and use of chemotherapy after stenting (P = 0.001) were significantly associated with patient survival. Multiple Cox's proportional hazard regression analysis showed that both serum bilirubin level after stenting (P = 0.017) and use of chemotherapy after stenting (P = 0.033) were independent predictors of patient survival (Table 4).
Multiple Cox's proportional hazard regression analysis of factors independently associated with survival after metallic stent placement
Median survival time was significantly longer in patients with serum bilirubin levels ≤2 mg/dl (182 days; 95% CI 122–242 days) compared to in >2 mg/dl (54 days; 95% CI 20–88 days) after stenting (Fig. 4a), and in patients who did (224 days; 95% CI 138–310 days) rather than did not (148 days; 95% CI 133–163 days) receive chemotherapy after stenting (Fig. 4b).
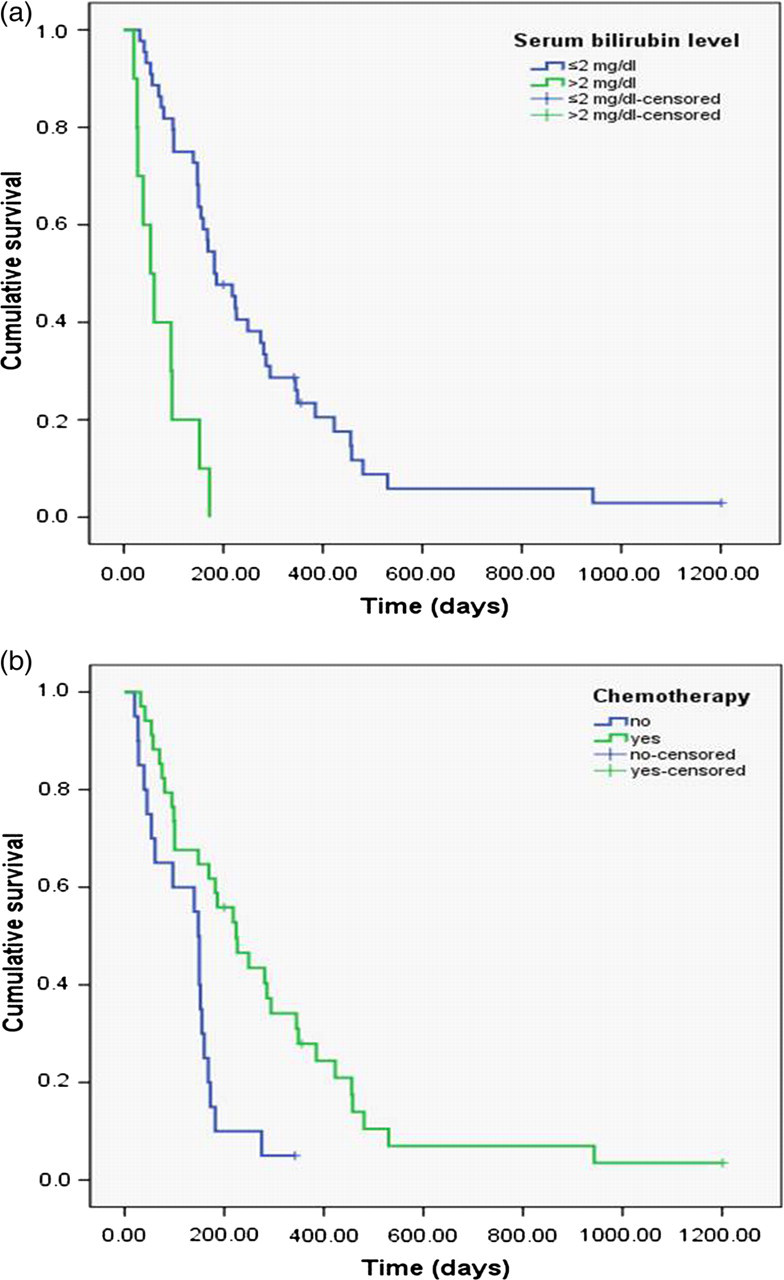
Multiple Cox's regression analysis of patient survival after stenting. Kaplan-Meier curves showing patient survival according to (a) serum bilirubin level, and (b) use of chemotherapy
Discussion
We have shown here that the upper CBD (33%) and hilum (33%) were the most frequent levels at which biliary obstruction occurred. We also found all 25 patients with lymph node metastasis had non-hilar bile duct (upper CBD and whole CBD) obstructions. Although lymph node metastasis in the hepatoduodenal ligament has been reported to be the primary cause of biliary obstruction (4, 6, 12), we found rather that intraductal metastasis (57%) was the most frequent cause. We also found that intraductal metastases could involve the intra- or extrahepatic bile duct as well as the cystic duct, and that all hilar obstructions were associated with intraductal metastasis or hepatic metastases. These findings indicate that lymph node metastases tend to be located in the extrahepatic area along the hepatoduodenal ligament, whereas intraductal metastases spread into the intrahepatic or cystic ductal system.
In general, patients with metastatic disease causing biliary obstruction experienced poorer overall survival, because many also had widespread metastases. The median survival time of patients with malignant biliary obstruction caused by metastatic gastric cancer was 104 days, comparable to the intervals reported in previous studies (70–79 days) (10, 12). In patients who underwent PTBD, all of tumor histology, serum bilirubin level after PTBD, and chemotherapy after PTBD, were independent predictors of survival. Previous studies suggested that chemotherapy after biliary drainage offers a survival benefit to patients with malignant biliary obstruction caused by metastatic gastric cancer (10, 12). Our results also suggest that chemotherapy after PTBD may prolong patient survival. However, patients who received chemotherapy had lower serum bilirubin level and were in better general condition than were those who did not receive chemotherapy. Such imbalances in clinical background may have affected the survival difference noted between patients who did and did not receive chemotherapy. We found that patients with post-PTBD serum bilirubin level >2 mg/dl were at a 2.014-fold greater risk of death than were those with ≤2 mg/dl, suggesting that serum bilirubin level after PTBD is a predictor of patient survival. Patients with primary cancers in different organs and serum bilirubin levels <4 mg/dl had a survival advantage over those with higher bilirubin levels (17, 18), as did patients with malignant biliary obstruction caused by metastatic gastric cancer and those with serum bilirubin levels < 2 mg/dl (12). We also found that median survival time was significantly longer in patients with differentiated rather than signet ring cell histology of primary gastric cancer, the histology of the primary tumor thus may be an independent predictor of patient survival. A previous study suggested that signet ring cell histology is a major and independent predictor of poor prognosis due to specific characteristics such as more infiltrating tumors showing affinity for lymphatic tissue accompanied by a hilar rate of peritoneal carcinomatosis (19).
We found that both serum bilirubin level and use of chemotherapy after stenting were independent predictors of survival in patients who underwent metallic stent placement. In contrast to what was noted upon survival analysis of patients who underwent PTBD, the histologic type of the primary tumor was not an independent predictor of survival in patients who underwent metallic stent placement. However, many patients with signet ring cell histology did not undergo metallic stent placement because of contraindications such as poor general health status and the presence of extensive extrabiliary metastases. We found that the overall stent occlusion rate was 24% and the median stent patency time 351 days, but there were no significant differences in stent patency or patient survival between patients with the intraductal and lymph node metastases. We also found no significant association between patency rate and any of patient age, gender, histology of primary gastric cancer, level of obstruction, serum bilirubin level before stenting, use of chemotherapy after stenting, or stent type.
This study had several limitations, including a retrospective design and inclusion of a relatively small number of stent patients. Moreover, because differences among the four types of stents used may have influenced stent patency, further prospective, randomized comparisons according to type of metastasis are necessary. Another limitation was that a histologic diagnosis of intraductal metastasis was made in only one (1.5%) of 67 patients. However, histologic confirmation was clinically difficult and unnecessary because of the occurrence of extrabiliary metastases or poor general patient condition. Despite these limitations, imaging diagnosis of intraductal metastasis was successfully conducted.
In conclusion, PTBD and subsequent metallic stent placement were safe and effective methods for palliative treatment in patients with malignant biliary obstruction caused by metastatic gastric cancer. Patients with differentiated cancer histology and serum bilirubin level ≤2 mg/dl after PTBD are probably the best candidates for treatment with a combination of metallic stent placement and chemotherapy.