
Abstract
Background
Unilateral biliary metallic stent placement in the lobe with patent portal vein seemed to be a safe and effective palliative treatment of patients with contralateral portal vein occlusion caused by advanced hilar malignancy, obviating bilateral stent placement in these patients, because the hepatic lobe with portal vein occlusion ceases to produce bile due to interruption of enterohepatic circulation.
Purpose
To investigate the safety and efficacy of percutaneous unilateral expanded polytetrafluoroethylene (ePTFE)-covered stent placement in malignant hilar biliary obstruction with contralateral portal vein occlusion.
Material and Methods
From February 2008 to March 2011, 24 consecutive patients with malignant hilar biliary obstruction and unilobar portal vein occlusion were enrolled in this prospective study. All patients were treated by percutaneous placement of ePTFE-covered stents.
Results
Stent deployment was technically successful in all patients. Two (8%) patients experienced minor self-limiting hemobilia. No major complication was noted. Successful internal drainage was achieved in 22 (91.6%) patients. Mean serum bilirubin level, which was 12.5 mg/dl ± 8.4 before drainage, decreased significantly to 2.7 mg/dl ± 3.4, 1 month after stent placement (P < 0.001). Median survival was 191 days (95% CI, 94–288 days) and cumulative stent patency rates at 1, 3, 6, 9, and 12 months were 100%, 95%, 95%, 95%, and 71%, respectively. Two (8%) patients presented with stent occlusion due to sludge incrustation. Aside from two patients who had died within 30 days after stent placement, the other 22 patients demonstrated slight decrease in diameter of undrained lobe and did not experience cholangitis nor jaundice.
Conclusion
Unilateral placement of ePTFE-covered stent in the lobe with patent portal vein seems to be a safe and effective method for palliative treatment of patients with contralateral portal vein occlusion. In addition, ePTFE-covered stent placement can prevent tumor ingrowth without functional occlusion of segmental bile ducts.
Transhepatic or endoscopic placement of self-expanding metallic stents has been an established method of palliative treatment to relieve malignant hilar obstructions (1–13). There have been conflicting opinions as to whether stent placement should be unilateral or bilateral (9–13). Some investigators have preferred bilateral stenting not only because unilateral stenting alone may not completely relieve jaundice (11) but also because stent patency may be longer than unilateral stenting (10). On the other hand, others have advocated unilateral drainage not only because the risk of complications is lower than multiple stent deployment (7) but also because adequate palliation can be achieved by the drainage of only 25% of the liver (8). In a report by De Palma et al. (12), patients with bilateral drainage had a significantly lower rate of successful stent insertion and a significantly higher rate of early cholangitis than patients with unilateral drainage. However, these previous reports have usually focused on technical or clinical outcomes of unilateral or bilateral drainage in advanced hilar obstruction according to Bismuth-Corlette classification.
To date, there has been only one comparative study of unilateral and bilateral stenting in patients with hilar biliary obstruction with unilobar portal vein occlusion caused by advanced malignancies (14). That study showed that unilateral biliary metallic stent placement in the lobe with patent portal vein seemed to be a safe and effective palliative treatment of patients with contralateral portal vein occlusion caused by advanced hilar malignancy, obviating bilateral stent placement in these patients, because the hepatic lobe with portal vein occlusion caused by advanced hilar malignancies ceases to produce bile due to interruption of enterohepatic circulation (14, 15).
Although the use of expanded polytetrafluoroethylene (ePTFE)-covered stents has proven to be feasible for the treatment of malignant biliary obstruction (16–23), less is known about the outcomes of covered stent placement in patients with malignant hilar biliary obstruction (16, 18, 23). Only one study reported that T-configured ePTFE-covered stents for palliative treatment of malignant hilar biliary obstruction were technically safe and clinically effective (23).
We therefore investigated the safety and efficacy of percutaneous unilateral ePTFE-covered biliary stent placement in 24 patients with hilar biliary obstruction with contralateral portal vein occlusion.
Material and Methods
Patient population
We evaluated 24 consecutive patients with malignant hilar biliary obstruction and contralateral portal vein occlusion who underwent unilateral ePTFE-covered stent placement between February 2008 and March 2011. Portal vein occlusion caused by underlying malignancies was diagnosed when there was encasement of the portal vein with no demonstrable flow or an intraluminal filling defect. Atrophy was defined as approximately 50% loss of expected volume in two or more hepatic segments with crowding of the bile ducts and hepatic vasculature (24). Two independent radiologists (RY and DIG) reached 100% concordance for the diagnosis of bile duct obstruction, portal vein occlusion, and atrophy.
Patients were included if they had malignant hilar biliary obstruction and unilobar portal vein occlusion that could not be treated surgically as a result of unresectability, late-stage tumor, advanced age, or co-morbid condition, and if an endoscopic attempt to drain the obstructed bile ducts was unsuccessful. Exclusion criteria included an abnormal coagulation status (INR value ≥1.5 and platelet count ≤50,000) or poor general health status (Eastern Cooperative Oncology Group performance status grade 3–4). This prospective study was approved by the institutional review board of out institution and written informed consent was obtained from all the patients.
Technique
All percutaneous transhepatic biliary drainage (PTBD) procedures and stent insertion were performed under conscious sedation using intravenous pethidine hydrochloride (Demerol, Keukdong Pharmaceuticals, Seoul, Korea) and intramuscular lidocaine (Jeil Pharmaceuticals, Taegu, Korea). All unilateral PTBD procedures were performed at the peripheral intrahepatic bile duct of the lobe without portal vein occlusion. The intrahepatic bile duct was punctured with a 21-gauge Chiba needle (Cook, Bloomington, IN, USA) under fluoroscopic or ultrasonographic guidance, and an 8.5-F drainage catheter (Cook) was inserted to relieve jaundice or cholangitis. Stents were placed for less than 2 weeks after PTBD, allowing cholangitis if any, to be treated. Antibiotics were administered intravenously 2 h before the procedures and for at least 48 h afterwards.
All stent deployments were performed with double stent (Gwon stent; TaeWoong Medical, Kimpo, Korea) (Fig. 1) composed of the outer self-expanding uncovered stent (Niti-D stent, TaeWoong Medical) and the inner conical-configured covered stent (22). The inner covered stent was composed of an outer ePTFE membrane and inner supporting self-expanding uncovered stent (Niti-S stent, TaeWoong Medical). Stents were available in diameters of 10 mm and in lengths of 7, 8, 9, and 10 cm. In addition, 2 or 3 cm proximal uncovered metal extensions were available for intrahepatic overstenting to prevent tumor overgrowth, stent migration, and intrahepatic side branch occlusion (21–23). Radiopaque markers were incorporated into the ends of both the inner and outer stents to increase visibility during placement under fluoroscopic guidance. The stent delivery system was a standard push-rod assembly consisting of a 9-F sheath and an inner catheter. After deployment, stents became shortened by 15%.
Standard form of Gwon stent (10 mm × 9 cm and 2 cm proximal uncovered extension) used in this study
Before inserting the stent, the stricture was dilated using a balloon catheter 6–8 mm in diameter (Synergy; Boston Scientific, Galway, Ireland). The diameter and length of each covered stent was decided by the physician operators according to the degree of intrahepatic bile duct dilatation and the extent of malignant stricture. The covered stent deployment system was introduced over a 0.035-inch, 150-cm long stiff hydrophilic guide wire (Terumo, Tokyo, Japan) or over an extra stiff Amplatz guide wire (Cook) and then deployed across the hilar stricture to the common bile duct to cover the bile duct approximately 1–2 cm proximal and 2–3 cm distal to the stricture to prevent tumor overgrowth. Post-stenting balloon dilation was not performed in any patient. After stent placement, an 8.5-F temporary drainage catheter (Cook) was placed just proximal to the stent. For 1–2 days after stent placement, external drainage catheter was frequently irrigated to remove blood clots or sludge. The temporary drainage catheter was removed after 2–3 days of catheter clamping, without further intervention if free contrast flow through the stent into the common bile duct and the duodenum was documented.
Follow-up
All patients were clinically evaluated, including measurements of total serum bilirubin level, at the interventional radiology outpatient clinic at 1, 3, 6, 9, and 12 months after their procedures. Patients who experienced unexpected symptoms or signs, such as jaundice, pain, or fever, were evaluated on an urgent basis. Beginning 12 months after stent placement, patients were interviewed by telephone at monthly intervals. Patients were followed up until recurrence of obstructive jaundice or death, and evaluated by computed tomography (CT) of the liver at 1 and 6 months after stent placement. Complications were diagnosed by clinical and laboratory examinations and when indicated by imaging modalities. Patients with recurrent jaundice were evaluated by CT or percutaneous transhepatic cholangiography. If stent occlusion was detected, the stent was revised percutaneously by inserting a biliary drainage catheter with/without metallic stent.
Study endpoints and definitions
The study endpoints were the rates of technical success, complications, successful internal drainage, stent patency and patient survival times, as well as the assessment of the undrained lobe with portal vein occlusion after stent placement. Technical success was defined as stent deployment in an adequate position across the stricture with good contrast passage through the stent. Complications were classified as major and minor according to the guidelines of the Society of Interventional Radiology Standards of Practice Committee (25). Minor complications were defined as those requiring no therapy or nominal therapy, including overnight admission for observation only. Major complications were defined as those necessitating major therapy, those necessitating an unplanned increase in the level of care or prolonged hospitalization (>48 h), and those resulting in permanent adverse sequelae or death. Successful internal drainage was defined as successful removal of temporary drainage catheter and a decrease in serum bilirubin level to less than 75% of the pretreatment value within the first month following stent placement.
Because one limitation in using a covered stent for treatment of malignant hilar biliary obstruction is a risk of occlusion of intrahepatic segment ducts at the drained lobe (16–23), we assessed the change in diameter of the blocked segmental duct at the drained lobe by CT of the liver. A blocked segmental duct was defined as an intrahepatic bile duct that was covered by the covered portion of the stent.
To evaluate anatomical and functional changes of the undrained lobe with portal vein occlusion after stent placement, we assessed several factors such as liver volume, bile duct diameter, and serum total bilirubin level. However, comparison of liver volume change after stent placement was determined to be unsuitable for evaluation of an undrained lobe because of the following reasons: The degree of volume change was not clear because nearly half of the patients already had atrophic change of the lobe with portal vein occlusion at initial admission. In addition, during the follow-up period after stent placement, volume change was variable due to progression of underlying malignancy and intrahepatic metastases. Therefore, to evaluate follow-up change of the undrained lobe, diameter of the intrahepatic bile duct of the undrained lobe, and serum total bilirubin level were chosen because they could be less affected by these possible factors than the liver volume. Measurement of bile duct diameter was performed by two independent radiologists (RY and DIG) using a CT analysis system (Petavision for Diagnosis; Asan Medical Center, Seoul, Korea). The intrahepatic duct dilated most in the undrained lobe with portal vein occlusion was chosen, to compare its diameter before, and 1 and 6 months after stent placement.
A stent that remained patent was assumed to have no increase in serum bilirubin levels and no dilatation of the stented intrahepatic bile ducts depicted on CT during the follow-up period. Stent occlusion was defined as a radiologically confirmed biliary obstruction plus serum bilirubin levels higher than 3 mg/dl, or any condition requiring reintervention to improve biliary drainage. Sludge formation was defined as sludge occluding the stent lumen that could be cleared by biliary balloon sweeping. Tumor ingrowth was defined as tissue occluding the stent lumen that could not be cleared by biliary balloon sweeping. Stent patency was defined as the time interval between initial stent placement and stent occlusion. If there was no evidence of obstruction during a patient's life, the patency period was considered to be equal to the patient survival time. Patient survival time was defined as the time interval between initial stent placement and death.
Statistical analysis
Paired-sample t-test was used to compare the pre- and post-stenting serum bilirubin levels and diameters of the blocked segmental duct at the drained lobe and the intrahepatic bile duct at the undrained lobe. Stent patency and patient survival were calculated according to the Kaplan-Meier method. All statistical analyses were performed using SPSS software (version 14.0. SPSS, Chicago, IL, USA), with P values < 0.05 considered to be statistically significant.
Results
Patient characteristics
Patient characteristics
Technical outcomes
Stent deployment was technically successful in all 24 patients, with correct positioning was verified in all (Figs. 2 and 3). The 24 patients received 24 covered stents of different sizes, i.e. 10 mm × 7 cm (n = 2), 10 mm × 8 cm (n = 11), 10 mm × 9 cm (n = 8), and 10 mm × 10 cm (n = 3). Sixteen patients had one or two segmental duct blockages by the covered portion; nine of these patients showed no contrast filling, whereas seven showed contrast filling, of the blocked segmental ducts on pre-stenting cholangiography. Control cholangiography immediate after stent placement confirmed the correct positioning of the stent and showed that the lesion was completely covered by the covered portion of the stent. Two (8%) patients experienced minor procedure-related complications of self-limiting hemobilia that completely resolved 2–3 days after stent placement without transfusion. No major complication directly related to the stent placement procedure was noted. Follow-up cholangiography 3–5 days after stent placement showed adequate decompression of the treated biliary ducts in all patients. Temporary drainage catheters were removed from all patients after confirmation of good stent patency.
An 83-year-old man with intrahepatic cholangiocarcinoma (Bismuth type III) and right portal vein occlusion. (a) Contrast-enhanced CT image shows intrahepatic bile duct dilatation and right portal vein occlusion caused by tumor encasement. (b) Cholangiogram via the left-sided drainage catheter shows stricture of the left intrahepatic bile duct and upper CBD. Right intrahepatic bile duct is not opacified by contrast media. (c) Cholangiogram 3 days after ePTFE-covered stent placement shows good passage of contrast media via the stent (arrowheads). (d) Contrast-enhanced CT scan obtained 1 month after stent placement shows decompressed left intrahepatic bile duct A 66-year-old man with bile duct carcinoma (Bismuth type III) and right portal vein occlusion caused by preoperative portal vein embolization. (a) Cholangiogram shows stricture from the left intrahepatic bile duct to lower CBD. This patient underwent right portal vein embolization using coils (arrow) and vascular plug (arrowhead) 4 weeks before stent placement. (b) Cholangiogram 4 days after stent placement shows good passage of contrast media via the stent

Clinical outcomes
One month follow-up evaluation of serum bilirubin level and CT scan were available in 22 patients; the remaining two patients died before 1-month follow-up. Successful internal drainage was achieved in 22 (91.6%) of 24 patients. Mean serum bilirubin level, which was 12.5 mg/dl ± 8.4 before drainage, decreased significantly, to 2.7 mg/dl ± 3.4, 1 month after stent placement (P < 0.001). Although the degree of decrease in the diameter of the intrahepatic bile duct in the undrained lobe did not reach statistical significance (P = 0.092), the 22 patients demonstrated a slight decrease in diameter (mean diameter, 6.7 mm ± 2.9 before drainage, to 6.5 mm ± 2.8) 1 month after stent placement (Fig. 4). The 16 patients with segment duct blockage by the covered portion (mean, 7.2 mm ± 4.1) demonstrated a significant decrease in mean diameter of the blocked segment duct to 5.4 mm ± 2.1, 1 month after stent placement (P < 0.001). Aside from the two patients with stent malfunctions, the remaining 20 patients did not experience cholangitis or jaundice until death or until the end of the study.
A 72-year-old man with intrahepatic cholangiocarcinoma (Bismuth type IV) and right portal vein occlusion caused by tumor encasement. CT images obtained before percutaneous transhepatic biliary drainage and 1 month after stent placement show little change in diameter of right intrahepatic bile duct after stent placement
Patient survival
All patients were clinically followed up until death or until the end of the study on August 31, 2011. The mean follow-up period was 207 days (range, 13–460 days) after stent placement. At the time of this analysis, six patients remained alive. Two patients died within 30 days after stent placement due to rapid progression of underlying malignancies, with their deaths not directly related to the procedures. Kaplan-Meier analysis showed that median patient survival was 191 days (95% CI, 94–288 days) (Fig. 5).
Kaplan-Meier curve of the survival rate of the study patients
Stent patency
Stent occlusion occurred in two (8%) patients after 79 and 325 days each. The cause of covered stent occlusion was sludge incrustation. No tumor ingrowth occurred. The two patients with stent occlusion underwent biliary drainage procedures via percutaneous route such as only PTBD (n = 1) or additional metallic stent insertion (n = 1). Kaplan-Meier analysis showed that cumulative stent patency rates at 1, 3, 6, 9, and 12 months were 100%, 95%, 95%, 95%, and 71%, respectively (Fig. 6).
Kaplan-Meier curve of the stent patency rate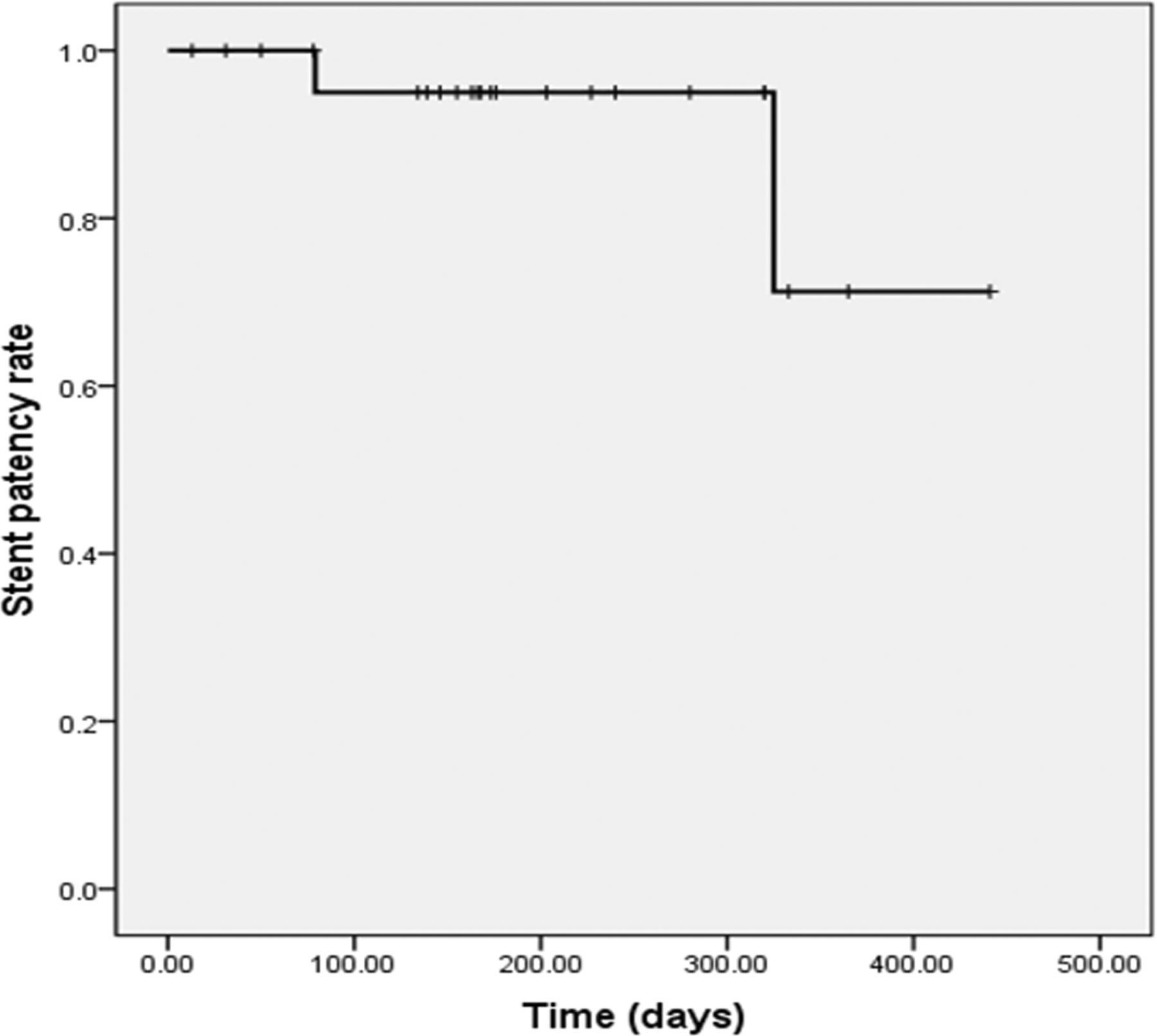
Discussion
In this study, we found that the technical success rate (100%), complication rate (8%), successful internal drainage rate (91.6%), and median patient survival time (191 days) were in good agreement with the results of previous studies of percutaneous or endoscopic metallic stent placement of various configurations (1–14, 23). In those studies, the technical success rate ranged from 93% to 100%, the overall complication rate ranged from 17% to 33%, the successful internal drainage rate ranged from 89% to 92%, and the median patient survival time ranged from 176 to 239 days.
In this study, the intrahepatic bile ducts of the undrained lobe with portal vein occlusion in patients who underwent unilateral ePTFE-covered stent placement showed no significant change in diameter on follow-up CT. Gwon et al. (14) proved the unilateral biliary metallic stent placement in the lobe with a patent portal vein was safe and effective palliative treatment of patients with contralateral portal vein occlusion caused by advanced hilar malignancy, obviating bilateral stent placement in these patients. In general, the most important factor in regulating the volume of bile flow is the rate of bile salt synthesis by hepatocytes, which is regulated by the return of bile salts to the liver through enterohepatic circulation. When the portal vein of one liver lobe is obstructed, portal vein obstruction interrupts the cycle of enterohepatic circulation in the obstructed lobe (14, 15). Previous investigators reported successful treatment of bile leakage by selective portal vein embolization, which induces cessation of bile production (26, 27). Thus, the liver lobe with portal vein occlusion caused by advanced hilar malignancies ceases to produce bile and becomes nonfunctional and atrophied. In addition, hepatic lobar atrophy is a frequent accompaniment of hilar cholangiocarcinoma and has been reported to occur in 20–30% of patients with the diagnosis (24, 28, 29). Previous studies (24, 29) have reported a significant correlation between hepatic lobar atrophy and ipsilateral portal vein occlusion and the fact that unilateral portal vein occlusion was present in 87–100% of atrophied lobes. Hadjis et al. (28) reported that biliary decompression of the lobe with portal vein occlusion neither reversed atrophy nor improved liver function. Other authors (24, 29) have recommended that biliary drainage should preferably be performed in the nonatrophic lobe. From these results, we postulated that unilateral stenting in the lobe with a patent portal vein may be preferable in patients with contralateral portal vein occlusion caused by advanced hilar malignancy or portal vein embolization because bile production in the undrained lobe may be functionally impaired or ceased by portal vein occlusion.
In this study, we found that stent patency rates at 1, 3, 6, 9, and 12 months were 100%, 95%, 95%, 95%, and 71%, respectively. We also found that stent occlusion rate was 8%, and important mechanisms causing stent occlusion was sludge incrustation. However, we did not observe stent occlusion resulting from tumor ingrowth. Stents covered with (e)PTFE or ePTFE/fluorinated ethylene propylene have been found to be effective in preventing tumor ingrowth, and have known to be associated with relatively low complication rates (16–23). To date, however, there has been only one comparative study of PTFE-covered and uncovered stent placement in palliative treatment of malignant extrahepatic biliary obstruction (21). That study showed that PTFE-covered stents were significantly superior in terms of stent patency compared with uncovered stents, without significant difference in complication rates.
In general, one important limitation in using covered stent for treatment of hilar malignancies is a risk of occlusion of branching bile duct. One study found that T-configured, ePTFE-covered stents for palliative treatment of malignant hilar biliary obstruction prevented tumor ingrowth without functional occlusion of the hepatic segmental bile ducts (23). We also found that the segmental ducts blocked by the covered portion of the stent showed a significant decrease in diameter, from 7.2 ± 4.1 mm before drainage to 5.4 ± 2.1 mm, 1 month after stent placement (P < 0.001). Moreover, patients with segment duct blockage by the covered stent did not show a significant increase in serum bilirubin level or cholangitis. Thus, unilateral placement of ePTFE-covered stent in the lobe with patent portal vein seems to be a safe method for palliative treatment of patients with contralateral portal vein occlusion caused by advanced hilar malignancies, not only preventing tumor ingrowth but also not compromising ipsilateral bile flow.
In conclusion, these preliminary results suggest that unilateral placement of ePTFE-covered stent in the lobe with patent portal vein seems to be a safe and effective method for palliative treatment of patients with contralateral portal vein occlusion caused by advanced hilar malignancies and portal vein embolization. In addition, use of ePTFE-covered stent can prevent tumor ingrowth without functional occlusion of hepatic segmental bile ducts. Additional studies in large number of patients with a longer follow-up period, as well as randomized, comparative trials, are required to determine the benefits of ePTFE-covered stent placement in these patients.