
Abstract
Background
Diffusion-weighted magnetic resonance imaging (DWI) is increasingly used in the diagnosis of endometrial disease. No complete knowledge, however, exists yet of the influence of physiology on the endometrial apparent diffusion coefficient (ADC) values on which DWI is based.
Purpose
To establish whether the ADC values measured with DWI in the endometrium of healthy reproductive-aged women significantly vary from the early proliferative to the periovulatory phase of the menstrual cycle and between the fundus and the isthmus of the uterus.
Material and Methods
In 17 women the endometrial ADC values measured on the fifth menstrual day, both at the fundus and at the isthmus of the uterus, were compared to the values obtained on the 14th day before the subsequent cycle. In 81 women (menstrual day: fifth through 21st) the endometrial ADC values measured at the fundus were compared to the values obtained at the isthmus of the uterus. All examinations were performed with a 1.5 T magnet (b values: 0 and 800 mm/s2). The results were analyzed by means of Student's t-test per paired data.
Results
The endometrial ADC values measured on the fifth day of the menstrual cycle were lower than those obtained in the periovulatory phase both at the fundus (mean 0.923 vs. 1.256 × 10−3 mm2/s) and at the isthmus (mean 1.297 vs. 1.529 × 10−3 mm2/s) of the uterus. The endometrial ADC values measured at the fundus of the uterus were lower than those obtained at the isthmus (mean 1.132 vs. 1.420 × 10−3 mm2/s) through the menstrual cycle. All these differences were highly significant (P < 0.001) at statistical analysis.
Conclusion
Physiological variations occurring in endometrial ADC values of healthy women should be considered by the radiologists when interpreting DWI examinations in patients with endometrial disease.
In the last decade diffusion-weighted magnetic resonance imaging (DWI) has increasingly become part of the diagnostic workout in several types of cancer. Mostly because of the reduced volume of the interstitial space due to the high cellularity typical of many neoplasms, a slower speed of extracellular diffusion of water molecules is expected in malignancies than in benign lesions and in normal tissue. This difference can be quantified by DWI as apparent diffusion coefficient (ADC) and is significant enough to allow identification, characterization, staging, and monitoring of therapy of cancer (1, 2).
According to several published papers, gynecological malignancies have to be considered among the most successful applications of DWI. In particular, endometrial adenocarcinoma has been demonstrated to benefit from DWI in regard to characterization, identification of additional tumoral foci missed with the routine MRI sequences, assessment of the depth of myometrial invasion, and evaluation of the outcome after non-surgical treatments such as chemo- or radiation therapy (3, 4). In the diagnosis of endometrial cancer DWI has been reported to be 84.6–95.8% sensitive, 94.6–100% specific, and 92–94.9% accurate (3–9).
Two individual characteristics, however, point out the difference of the endometrium of healthy reproductive-age women from the other organs and tissues in which DWI has proven useful. The endometrium is known to undergo major cyclic macroscopic, histological, and chemical changes through the menstrual phases under the action of the continuously varying hormonal environment (10); in addition, some anatomical and physiological differences distinguish the uterine fundus from the isthmus. Both the cycle-related changes and the regional differences observed in the normal endometrium are likely to determine variations in the viscosity of the interstitial space and in the ratio of the volume occupied by cells to the volume of the interstitial space. Since these two factors influence the speed of the extracellular diffusion of water (1, 2), both temporal (over the phases of the menstrual cycle) and spatial (in the different regions of the uterus) significant changes might be expected in the range of the endometrial ADC values to be considered normal.
Despite a few recently published papers warning radiologists to check the physiological status of patients before interpreting MR studies of the female reproductive system (11, 12), only one study, to our knowledge, has addressed the topic of the possible relationship between the endometrial ADC values and the phases of the menstrual cycle in normal women (13). On the other hand, no data at all are available concerning possible physiological regional variations in the endometrial ADC values.
The aim of this study is therefore to ascertain whether, in healthy reproductive-age women, the endometrial ADC values significantly vary with the phases of the menstrual cycle and with the uterine regions.
Material and Methods
Informed consent to this study, approved by the local institutional review board, was obtained from all included patients after the nature of the procedure had been fully explained.
Subject selection
Between March and September 2011 a series of healthy volunteers underwent pelvic MRI. They were women aged 18–40 years (mean 28.2 years) without contraindications to MRI examinations, all of them with normal menstrual cycles, without vaginal bleeding or any kind of discharge, who in the 6 months before the examination had not taken oral contraceptives nor had been pregnant. In no case was the examination performed during menstruation; a minimum endometrial thickness of 4 mm and the absence of fluid within the endometrial cavity at the reference T2-weighted scan were adopted as inclusion criteria.
To compare the ADC values in the different menstrual periods, 17 subjects were recruited in whom DWI was performed in the early proliferative phase (on the fifth day after the beginning of the menstruation) and, repeatedly, every day in the subsequent periovulatory phase. Among these latter examinations, the one was retrospectively selected which corresponded to the 14th day before the beginning of the next menstruation.
To compare the ADC values in the different regions of the uterus, 81 subjects were recruited whose menstrual day ranged from the fifth to the 21st.
DWI examination
All subjects were scanned in the supine position after lying supine for at least 10 min on the MR table in order to minimize the accumulation of any undetected endometrial fluid in the lower portion of the cavity, as it might happen had the subjects undergone MRI after prolonged standing.
All examinations were performed with a 1.5 T magnet (Signa HD Excite, GE Healthcare, Milwaukee, WI, USA) equipped with a phased-array 8-elements coil. After a preliminary T2-weighted 2D FRFSE (fast-recovery fast spin-echo) sagittal scan aimed to the assessment of the minimum endometrial thickness required for inclusion and of the absence of fluid into the uterine cavity, DWI was performed using a spin-echo EPI (echo-planar imaging) technique. 2D sagittal scans (slice thickness: 4 mm; interval: 0) were obtained (TR/TE, 5700/84.9 msec; FOV, 36 × 36 cm; matrix, 128 × 128; NEX, 8; phase FOV, 1); the duration of the acquisition was 3 min and 2 s. Through linear regression analysis of the natural logarithm of the signal intensity versus the diffusion gradient (b) used (0 and 800 s/mm2) inside an operator-defined region of interest (ROI), the software quantified the extent of diffusion and produced an ADC value expressed in mm2/s.
In the comparison between the different phases of the cycle, the ADC values were calculated, in each of the two examinations considered in the 17 women selected, both at the fundus of the uterine cavity (as high as possible within the endometrium, Fig. 1a–c) and in the isthmic portion of the uterine body, 2–3 cm cranial to the internal cervical os (Fig. 1b and d). These same anatomical landmarks were adopted to compare the fundal to the isthmic ADC values in 81 women at any phase (fifth through 21st day) of the menstrual cycle.
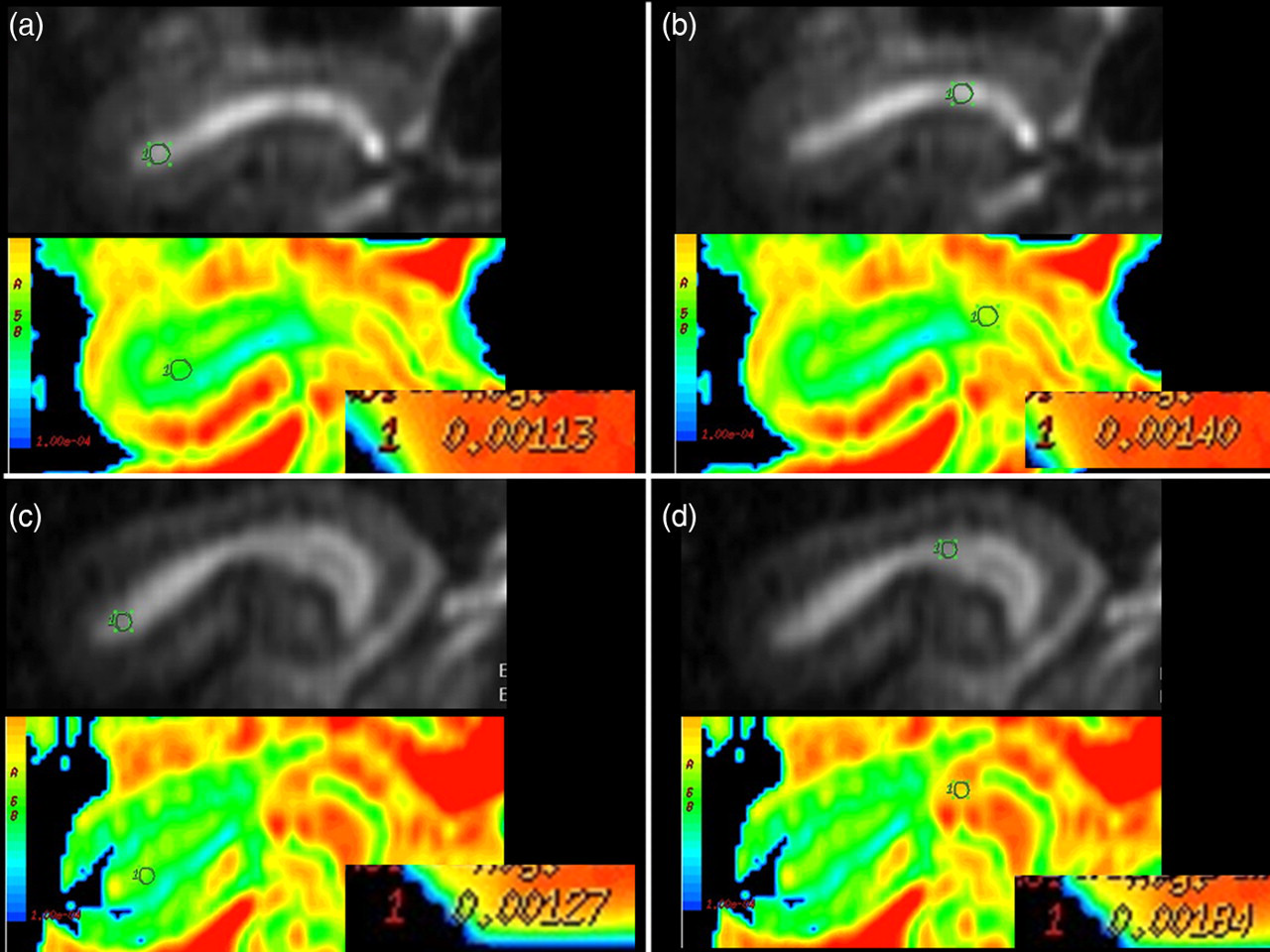
Endometrial DWI in one healthy subject (gray-scale and colour ADC maps). The ADC values measured at the fifth menstrual day (a and b) are lower than those measured in the periovulatory phase (c and d); the fundal values (a and c) are lower than the isthmic ones (b and d)
The ROIs (circular-shaped with 4–5-mm diameter) were drawn by one radiologist on the gray-scale ADC images (if necessary using the corresponding T2-weighted images for visual matching) and automatically transferred by the software to the color ADC maps for quantification. To reduce random variability in the measurements and to minimize the effects of possible partial volume artifacts, each ADC value considered in this study was calculated through the average of three different measurements, obtained in the same session slightly moving the position of the ROIs. One reader, with 8 years of experience in body MRI, performed all examinations.
Analysis of the results
The statistical significance of each of the differences in the ADC values obtained in each subject (early proliferative vs. periovulatory phase, both at the fundus and at the isthmus of the uterus; fundus vs. isthmus, independent of the menstrual phase) was measured by means of Student's t-test per paired data. P values <0.01 were considered statistically significant.
Results
Early proliferative vs. periovulatory phase
In the 17 subjects included, the endometrial ADC values measured at the fundus of the uterus on the fifth menstrual day (mean 0.923 × 10−3 mm2/s; standard deviation [SD] 0.134; range 0.68–1.16, Fig. 2a) were lower than those measured at the fundus in the periovulatory phase (mean 1.256 × 10−3 mm2/s; SD 0.170; range 1.10–1.80, Fig. 2b). The difference was highly significant (P < 0.001) at statistical analysis.

Endometrial diffusion through the phases of the menstrual cycle (“box-and-whisker” plot). The fundal ADC values measured during the early proliferative phase (a) are significantly lower (P < 0.001) than those measured in the periovulatory phase (b). The same difference, with faster speed of diffusion, is observed between the early proliferative (c) and periovulatory (d) values at the isthmus. The center of each box indicates the median ADC value, the upper and the lower ends of the box, respectively, the first and the third quartiles, and the upper and the lower ends of the whiskers, respectively, the highest and the lowest ADC values measured
The same statistical significance (P < 0.001) was obtained comparing in these subjects, in the two phases considered, the endometrial ADC values measured at the isthmus of the uterus: the mean fifth-day value was 1.297 × 10−3 mm2/s (SD 0.220; range 0.91–1.65, Fig. 2 c) vs. a mean periovulatory value of 1.529 × 10−3 mm2/s (SD 0.192; range 1.28–1.96, Fig. 2d).
Fundus vs. isthmus
In the 81 subjects included, the endometrial ADC values measured at the fundus of the uterus (mean 1.132 × 10−3 mm2/s; SD 0.240; range 0.68–1.80, Fig. 3a) were lower than those measured at the isthmus (mean 1.420 × 10−3 mm2/s; SD 0.239; range 0.83–1.96, Fig. 3b). The difference was highly significant (P < 0.001) at statistical analysis.
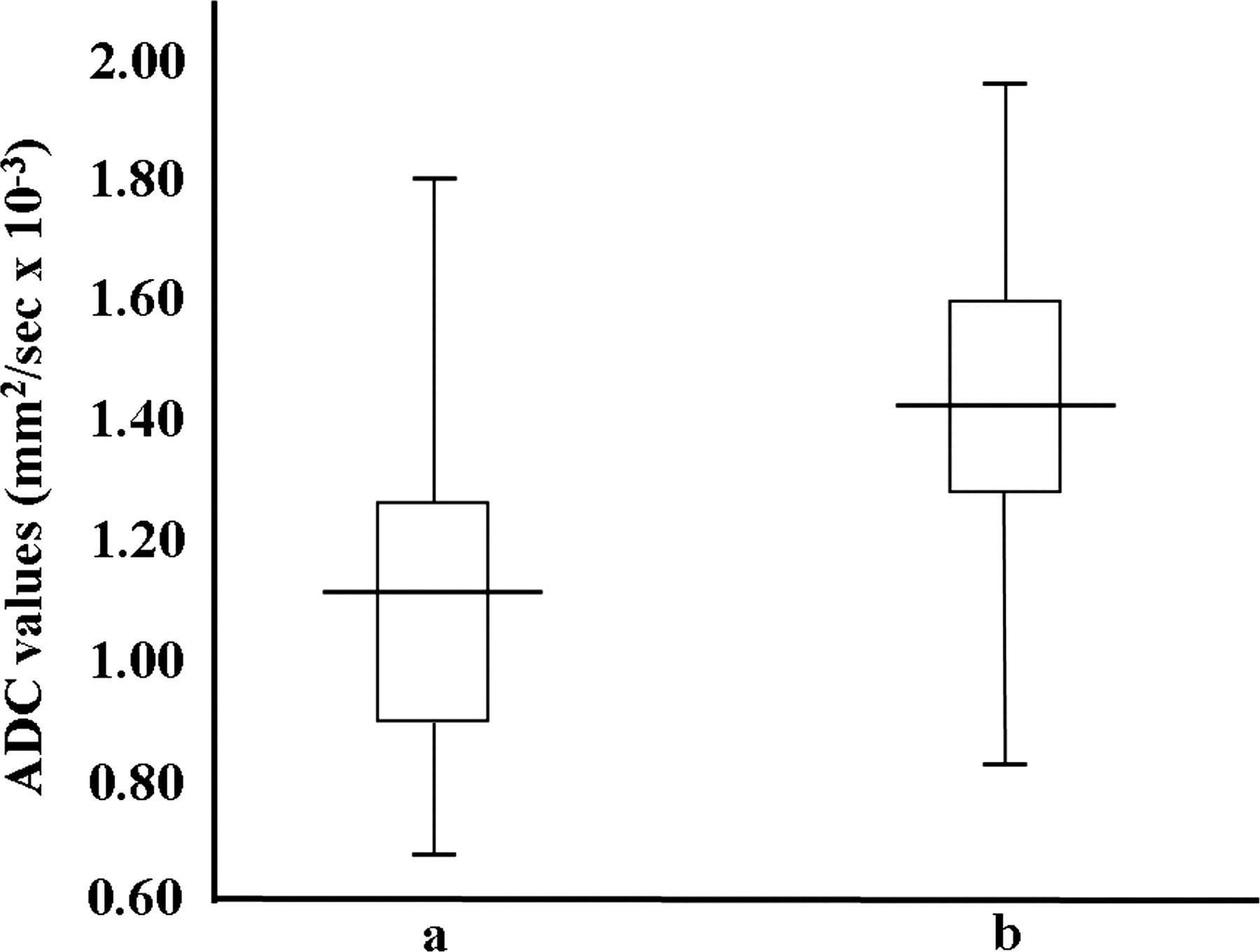
Endometrial diffusion at the different uterine portions (“box-and-whisker” plot). The ADC values measured at the fundus (a) are significantly lower (P < 0.001) than those measured at the isthmus (b). The center of each box indicates the median ADC value, the upper and the lower ends of the box, respectively, the first and the third quartiles, and the upper and the lower ends of the whiskers, respectively, the highest and the lowest ADC values measured
Discussion
The mean ADC values reported in the papers affirming the reliability of DWI in the diagnosis of endometrial disease were in the range of 0.86–0.97 × 10−3 mm2/s for malignancies, 1.44–1.65 × 10−3 mm2/s for normal tissue, and 1.27–1.63 × 10−3 mm2/s for benign lesions (3–9). Given their relatively small magnitude, the differences in the endometrial ADC values reported between cancer and non-malignant conditions should have been further validated prior to their clinical utilization; in particular, a comparison to the physiological variations of the endometrial ADC values likely occurring in normal women both over the menstrual cycle and through the different uterine regions should have been obtained. To our knowledge, however, this question has not been thoroughly answered to date, and therefore the actual reliability of DWI in the diagnostic workout of endometrial cancer is far from having been fully ascertained.
Only one paper (13) tried to demonstrate cycle-related changes in endometrial ADC, observing lower values during the menstrual phase than in the periovulatory and secretory phases. However, only seven subjects were enrolled in this study, and both the definition of menstrual phases and the positioning of the ROIs seem to have been approximate; moreover, the authors themselves consider that the presence of blood in the uterine cavity affected the ADC values obtained during menstruation. All these factors might have limited the significance of this study in correlating the ADC values to the structural variations occurring within the endometrial mucosal layer.
Our study aimed to quantify the ADC values within the endometrial tissue and therefore refrained from performing any measurement during menstruation, demonstrating a significantly faster diffusion in the periovulatory than in the early proliferative phase. We cannot estimate which of the cycle-related variations known to occur in the histology of the endometrium is responsible for these results. The accumulation of interstitial fluid and mucoid matrix which makes the endometrial stroma become progressively looser after mid-cycle (10) might play a role, since the higher the amount of extracellular fluid the faster the diffusion is expected to be (1, 2). Less likely, in our opinion, is an influence on the ADC values of the variations observed in the cytoplasm (10) of the epithelial cells (ribosomes and rough endoplasmic reticulum are well represented in the proliferative phase, while in the secretory phase giant mitochondria develop, together with an abundant deposition of glycogen). Since we excluded those subjects in whom detectable amounts of fluid were present, we are sceptical about a possible role on the changes of ADC values of the varying composition of the endometrial fluid (10, 14). In addition, the lower viscosity of the uterine secretions in the proliferative phase due to the influence of estrogens (15) should have increased the speed of the diffusion (1, 2), which is opposite to our results. A limited evidence in support of the hypothesis that the ovarian endocrine activity induces cyclic changes in the speed of diffusion in hormone-sensitive tissues derives from two published papers: lower ADC values have been measured during the second week of the menstrual cycle in normal breast tissue, although the difference was not statistically significant (16), and higher ADC values have been demonstrated in the junctional uterine zone, even though not in the endometrium, in women taking oral contraceptives (17). In neither case, however, a correlation of the variations in the ADC values to a definite histological background is available.
In regard to the regional variations of endometrial ADC values, we could not find any satisfactory anatomical or endocrinological correlation in the literature. At the isthmus the endometrium is known to be less sensitive than at the fundus to cyclic hormonal variations (18) and a lower endometrial blood flow has been measured at the internal cervical os than at the fundus (19), but probably neither factor can explain the differences we observed. However, we aimed to minimize the gravitational effect of any undetected endometrial fluid by asking our volunteers to lay supine on the MR table before the examination, what leads us to suppose that the cause of the faster isthmic diffusion is once again histological.
The range of the absolute ADC values of the normal endometrium (1.44–1.65 × 10−3 mm2/s) reported in the published papers is less wide than ours (0.68–1.80 × 10−3 mm2/s at the fundus; 0.83–1.96 at the isthmus). However, both at the fundus (0.240 × 10−3 mm2/s) and at the isthmus (0.239 × 10−3 mm2/s) we observed standard deviations lower than those (0.33 and 0.246 × 10−3 mm2/s) measured by other authors (7, 9), despite these studies enrolled fewer subjects (50 and 30, respectively) than we did (81 subjects). The only remaining paper (8) in which the standard deviation of the normal endometrial ADCs is available reports a 0.10 × 10−3 mm2/s value, which however has been obtained in a very small cohort (12 patients). Moreover, within each homogeneous group of patients we measured lower standard deviations (down to 0.134 × 10−3 mm2/s in the fundal ADC values in the proliferative phase).
Whatever their origin, the temporal and spatial differences in the endometrial ADC values measured in our series (Figs. 2 and 3) are significant enough to deserve attention. In the only published paper concerning the correlation of ADC values to the menstrual cycle (13) the authors correctly stated that the magnitude of the mean intra-individual variation in ADC values over the different phases (0.40–0.60 × 10−3 mm2/s) is not very far from the difference (0.45–0.65 × 10−3 mm2/s) between malignancy and benign lesions or normal endometrium reported in the literature (3–9), this result making the diagnostic use of ADC values problematic, especially as a marker of response to antineoplastic treatment. Although both our methods and our results are largely different from those reported by these authors, we agree with their conclusion, strongly suggesting further analysis of the topic and an attempt to identify the histological causes of the varying ADC values. In the meanwhile, the radiologists should be cautious when directing the management of patients with endometrial disease on the basis of the results of DWI examinations.
This study has two limitations. The cohort of patients in whom the ADC values were correlated to the phases of the menstrual cycle was relatively small, and a definite DWI-histological correlation enhancing the significance of the results has not been obtained.
In conclusion, the magnitude of the physiological variations in the endometrial ADC values over the different phases of the menstrual cycle and among the different portions of the uterus should be taken into account when interpreting DWI examinations in patients with endometrial disease, especially if therapeutic choices are influenced by the ADC values measured.