
Abstract
Background
CT radiation dose reduction results in increased noise or graininess of images which affects the diagnostic information. One of the approaches to lower radiation exposure to patients is to reduce image noise with the use of image processing software in low radiation dose images.
Purpose
To assess image quality and accuracy of non-linear adaptive filters (NLAF) at low dose chest CT.
Material and Methods
In an IRB approved prospective study, 24 patients (mean age, 63±7.3 years; M:F ratio, 11:13) gave informed consent for acquisition of four additional chest CT image series at 150, 110, 75, and 40 mAs (baseline image series) on a 64-slice MDCT over an identical 10-cm length. NLAF was used to process three low dose (110, 75, and 40 mAs) image series (postprocessed image series). Two radiologists reviewed baseline and postprocessed images in a blinded manner for image quality. Objective noise, CT attenuation values, patient weight, transverse diameters, CTDIvol, and DLP were recorded. Statistical analysis was performed using parametric and non-parametric tests for comparing postprocessed and baseline images.
Results
No lesions were missed on baseline or postprocessed CT images (n = 80 lesions, 73 lesions <1 cm). At 40 mAs, subjective noise in mediastinal window settings were graded as unacceptable in baseline images and acceptable in postprocessed images. Visibility of smaller structures improved from suboptimal visibility in baseline images at 40 mAs to excellent in postprocessed images at 40 mAs. No major artifacts were seen due to NLAF postprocessing, except for minor beam hardening artifacts not affecting diagnostic decision-making (14/22) in both baseline and postprocessed image series. Diagnostic confidence for chest CT was improved to fully confident in postprocessed images at 40 mAs. Compared to baseline images, postprocessing reduced objective noise by 26% (14.2±4.7/19.2±6.4), 31.5% (15.2±4.7/22.2±5.7), and 41.5% (16.9±6/28.9±10.2) at 110 mAs, 75 mAs, and 40 mAs tube current-time product levels.
Conclusion
Applications of NLAF can help reduce tube current down to 40 mAs for chest CT while maintaining lesion conspicuity and image quality.
Keywords
There is fundamental trade-off between computed tomography (CT) radiation dose and image quality. Lowering the radiation dose results in higher image noise or speckled appearance of images and sometimes more artifacts, this can compromise the diagnostic information in the CT images.
However, prior studies have shown a potential of radiation dose reduction in chest CT by optimizing scan parameters, such as lowering tube current (1–5) or reducing the peak kilo voltage (6–8). An alternate approach to limit radiation dose is reduction in image noise with the use of image processing software in low radiation dose images. Prior studies with use of noise reduction filters for reducing radiation dose have revealed mixed results (9–14). Furthermore, most prior radiation dose studies with filters used just one level of dose reduction to assess benefits (15–19). Effects of noise reduction filters on lesion characteristics following postprocessing have also not been described.
Therefore, the purpose of our prospective clinical study was to assess image quality and accuracy of non-linear adaptive filters (NLAF) at low dose chest CT.
Material and Methods
Patients
This prospective clinical study was approved by Human Research Committee of our Institutional Review Board (IRB) and was conducted in compliance with Health Insurance Portability and Accountability Act (HIPAA) guidelines. All 24 patients (mean age, 63 ± 7.3 years; age range, 55.7–70.3 years; male: female ratio, 11:13) gave written informed consent for the acquisition of four additional sets of research images, in addition to their standard of care, clinically indicated chest CT examinations.
Only patients scheduled for clinically indicated chest CT examinations were recruited if they were >50 years and were able to provide written informed consent, hold breath for a duration of at least 10 s, follow verbal commands for breath-holding, remain still for the scanning duration, and be hemodynamically stable (conscious, oriented, regular respiration rate of 12–40/min, pulse rate of 60–90 without dysrhythmia, systolic blood pressure of 100–140). Unconscious, unstable, or uncooperative patients not able to give informed consent were excluded from the study.
Scanning techniques
All 24 recruited patients underwent a clinically indicated standard of care chest CT examination on a commercial 64-channel multidetector row CT (Discovery CT750 HD, GE Healthcare, Waukesha, WI, USA) with administration of an intravenous contrast medium (80 mL of Iopamidol 370 mg% Bracco Diagnostics, Princeton, NJ, USA). Immediately after the acquisition of standard of care CT images, four additional sets of research images were acquired in each patient through an identical 10 cm scan length. Location of the acquisition of these additional image data-sets was selected based on one of the co-author's (SS) review of the patient's prior (available and reviewed in 22/24 patients) and current standard of care (reviewed in 2/ 24 patients) chest CT images. If multiple lesions were seen throughout the chest during review of prior CT or present standard of care images, preference was given the most subtle (first preference) or smallest (second preference) lesion detected in the chest CT. The maximum time period between the standard of care chest CT and the research images acquisition was <20 s.
To avoid contrast enhancement bias due to the delay in scanning from start of injection, the acquisition sequence of the four research CT datasets was randomized. Since it is not feasible to inject contrast media four times to a patient for acquiring images at identical contrast enhancement phase, no additional intravenous contrast medium was administered for acquisition of these research image series.
Fixed tube current-time products of 150, 110, 75, and 40 mAs were used for acquiring four sets of baseline images. The remaining scanning parameters with the exception of tube current were held constant and included: 120 kVp; pitch, 0.984:1; table speed per gantry rotation, 39.37 mm; helical acquisition mode, detector configuration; 64 × 0.625 mm; gantry rotation time, 0.5 s. The chest CT images were reconstructed at 2.5 mm section thickness, 2.5 mm section interval, and using a detail reconstruction kernel.
Image postprocessing
The non-linear adaptive filters (NLAF, ContextVision, Linkoping, Sweden) uses an algorithm which is based on the concept that CT image contain anatomical structures of various sizes and that image can be resolved into various frequency bands containing similar size structures. The algorithm is centered on the GOP (General Operator Processor) technology (20). The algorithm first divides image into various frequency bands and then individually process them to finally merge the information to produce the resultant image.
Depending on the scanner type and the anatomy of the scanned region, CT image is divided into a defined number of bands. Each band usually contains similar size structures, which allows it to process anatomical structures by size. As shown in Fig. 1, the low-pass band on the left consists mainly of the amplitude of the 2D signal and low frequent variations, whereas the high-pass band contains predominantly small structures and noise. The remaining band cover structures of mid size and low frequent noise. The NLAF processes each frequency band separately and coalesce the enhanced bands to produce final enhanced image.
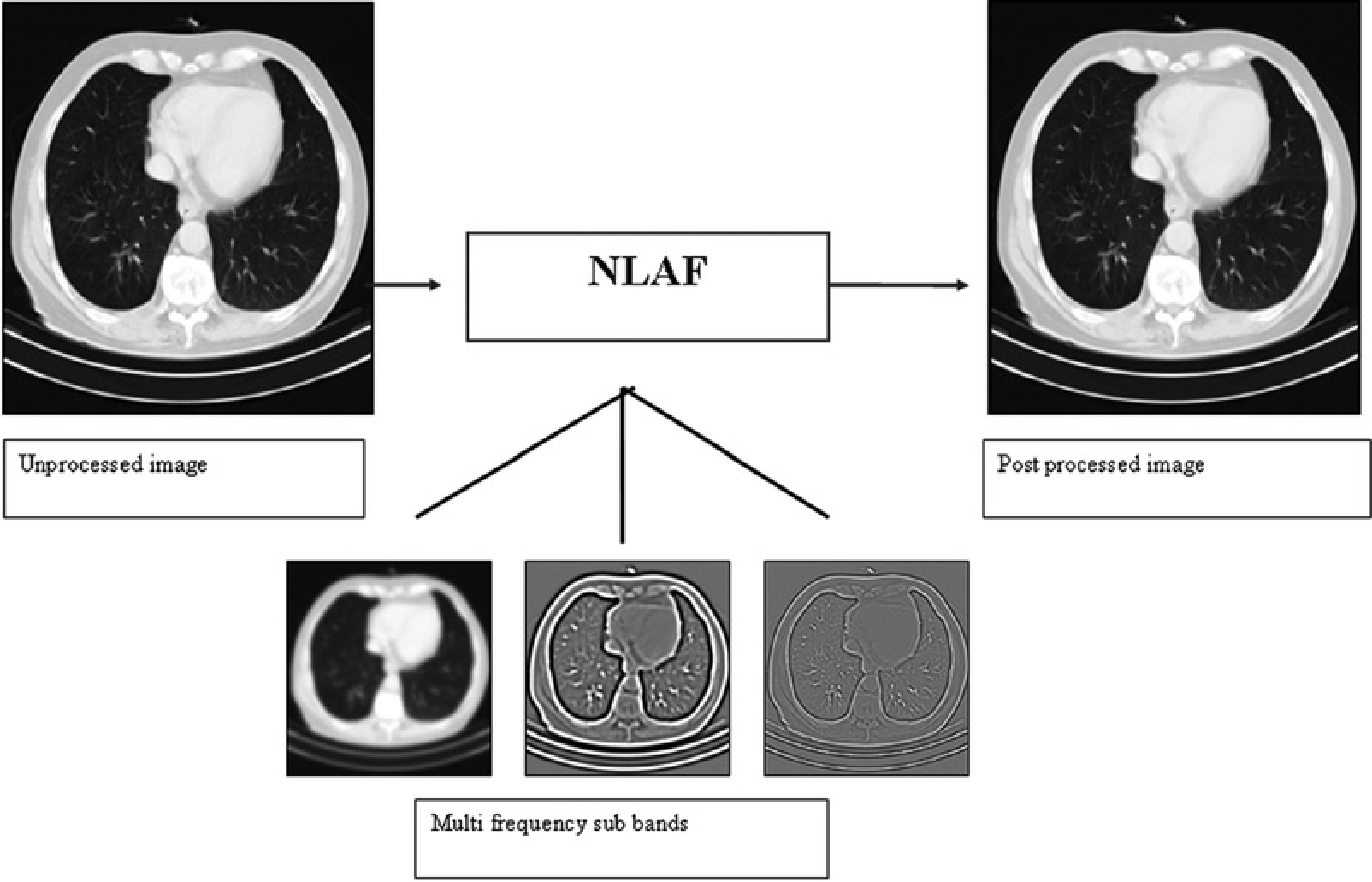
NLAF divides the original image into a number of frequency bands, which are processed separately and ultimately re-combined into a resultant final image
At the pixel level, NLAF examines each pixel in relation to its neighboring pixels. Subsets of filters are used to assess the predefined local features by running these subsets of filters in different directions. The filters are designed so that the combined filter response is completely rotational invariant. A number of features are estimated during the estimation of these subsets of filter responses including variance, orientation, phase, and energy. Feature estimation is performed on higher abstraction level, to produce more accurate and robust results. This information is used to decide whether the pixel is a part of same structure as its neighbors.
Finally based on the calculated set of these features, the contextual information for every location in the image is formed. This contextual information is merged to produce a specific filtering method, which adapts to image signal at every pixel location and individually optimizes it. The distinct quality of NLAF is the likelihood of adapting desired behavior to the image content and hence allowing both noise reduction as well as edge enhancement. For example, selectively noise reduction in soft tissue regions as well as edge enhancement in high frequencies areas such as lung and bones within a single image.
Lastly, the NLAF parameters noise reduction and edge enhancement can be optimized for the anatomy of the scanned region. The enhancement is performed in different intensity value ranges, corresponding to tissue-type-specific Hounsfield Units (HU). Also these parameters can be adjusted based on user preference as some radiologists prefer smooth images while others prefer a sharp, crispy image.
Three low dose baseline image series were processed with NLAF to obtain three sets of postprocessed images at 110, 75, and 40 mAs. Thus, seven image series were available for evaluation for chest CT (baseline 150, 110, 75, and 40 mAs and postprocessed 110, 75, and 40 mAs) in each patient.
Each image data-set was coded, de-identified, and randomized in Microsoft EXCEL 2003 (
Subjective image quality
All baseline and processed image series were reviewed on a Picture Archiving and Communication Systems (PACS) diagnostic workstation (AGFA Impax ES, AGFA Technical Imaging Systems, Ridgefield Park, NJ, USA) by two experienced thoracic radiologists (JBA and MG with 13 and 11 years of experience, respectively) for evaluation of image quality. Prior to the actual readout of image quality and lesion detection, both radiologists were trained on two image data-sets for the grading of different aspects of subjective image quality and as well as lesion assessment in order to understand the evaluation system as well as to improve inter-observer agreement. All images were reviewed on DICOM calibrated monitors with minimum resolution of 1920 × 1080.
Subjective image quality was assessed in terms of subjective image noise on a five-point scale (1, very little noise; 2, less than average noise; 3, average noise; 4, above average noise; and 5, unacceptably high noise) in the med-iastinal soft tissue window (window width 350 and window level 40). Artifacts were graded on a four-point scale (1, none; 2, minor artifacts not interfering with diagnostic decision-making; 3, major artifacts affecting visualization of major structures, but diagnosis still possible; and 4, artifacts affecting diagnostic information). In addition, radiologists also commented upon type of artifacts such as helical or windmill artifacts, streak artifacts due to metals and leads, beam hardening artifacts due to arms by body side, rarely, large body size and truncation due large body size or off centering and blotchy pixilated appearance. Visibility of smaller structures (such as blood vessels in the peripheral 2 cm of the lungs was assessed in lung window (window width 1500 HU and window level -600 HU) on a five-point scale (1, excellent; 2, above average; 3, acceptable; 4, suboptimal; and 5, unacceptable). Lesion size was measured on a four-point scale (1, focal and <1 cm; 2, focal and 1–5 cm; 3, focal and >5 cm; 4, diffuse lesion), lesion conspicuity of the smallest or most subtle lesion was assessed on a five-point scale (5, well-seen lesion with well-visualized margins; 4, well-seen lesion with poorly visualized margins; 3, subtle lesions; 2, probably an artifact mimicking a lesion; and 1, definitely an artifact mimicking a lesion) and diagnostic confidence (1, completely confident; 2, probably confident; 3, confident only for limited clinical situations; and 4, poor confidence). Image quality attributes assessed in our study have been described in the European Guidelines on Quality Criteria for Computerized Tomography (EUR 16262 www.drs.dk/guidelines/ct/quality/index.htm) and other chest CT studies pertaining to radiation dose reductions (21).
Assessment of subjective noise was performed prior lesion detection for each of the four dose levels from the lowest dose to the highest dose level in order to avoid potential bias.
Objective measurements
All participating subjects were weighed prior to their chest CT examinations. Circular region of interests (2–3 cm) to measure objective image noise (standard deviation) and CT numbers (HU) were drawn in descending thoracic aorta without touching the lumen walls, to cover at least two-thirds of its lumen, of all seven baseline and post-processed CT image series. The skin-to-skin maximum transverse diameter of chest was measured from localizer radiographs as transverse images are often reconstructed with a smaller field of view and may not include the skin.
CT dose index volume – CTDIvol (mGy) and dose length product – DLP (mGy.cm) were recorded for all dose levels.
Statistical analysis
Data were analyzed using parametric and non-parametric statistics. Analysis of variance (ANOVA) was performed to compare objective image noise and CT numbers. Wilcoxon signed rank tests were used to compare the subjective image quality for both baseline and postprocessed image series. Inter-observer variability was estimated using percentage agreement between the two radiologists for each of the assessed subjective image quality and lesion assessment parameters.
Results
The percentage agreement between the two radiologists ranged from 77.2% (17/22 scores with agreement for visibility of small structures) to 100% (22/22 scores in perfect agreement for criteria such as image noise, lesion conspicuity, and diagnostic confidence) in baseline and post-processed CT image series.
Subjective assessment
Detailed subjective lesion detection and image quality scores are summarized in Table 1. No lesions were missed on low dose processed or unprocessed chest CT image series. A total of 80 lesions were detected in 22 patients in all seven image series data-sets. Seventy-three lesions (73/80, 91%) were <1 cm in maximum dimension, while six (6/80, 7%) lesions measured 1–5 cm in maximum dimension. These lesions included 70 solid or subsolid lung nodules, pleural thickening or trace pleural effusion (n = 4), patchy ground-glass opacities (n = 2), fissural thickening (n = 1), diffuse bronchial wall thickening (n = 1), and complete unilateral collapsed lung (n = 1). All lesions were well seen with well visualized margins in both unprocessed and processed image series irrespective of the tube current-time product levels (P < 0.05).
Lesion detection and subjective image quality scores for chest CT examinations for NLAF processed and unprocessed image groups at four different radiation dose levels. Image noise was lowered and visibility of small structures was enhanced with NLAF processing. Since, discrete values cannot be averaged; the table presents the lowest or similar scores (median, interquartile range) for lesion conspicuity, image noise, contrast, and diagnostic confidence given by radiologists
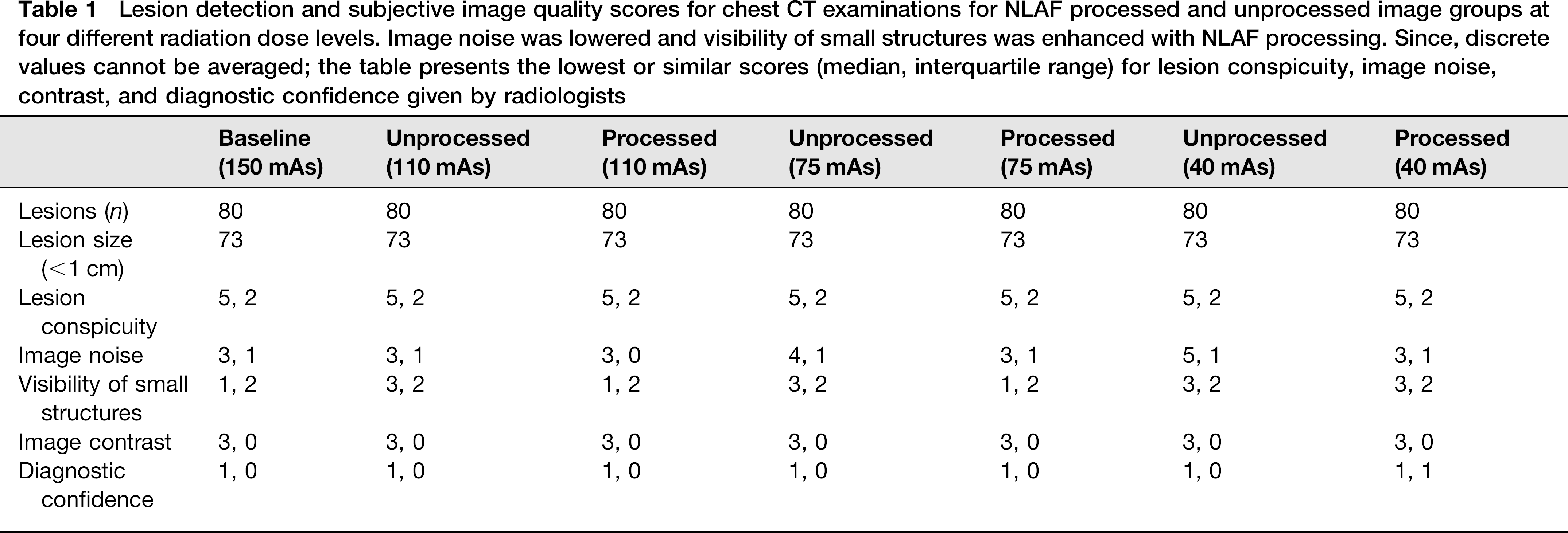
Both thoracic radiologists ranked subjective image noise as unacceptable in unprocessed images at 40 mAs, while noise was acceptable with NLAF processing at respective dose level (P < 0.0001) (Fig. 2). Visibility of smaller structures, such as peripheral blood vessels in the lungs, was found to be acceptable in both unprocessed and processed image series at 40 mAs (P < 0.05) and improved from acceptable to excellent at 110 and 75 mAs (P < 0.001). No major artifacts were seen on any of NLAF processed image series. Minor beam hardening or photon starvation artifacts were noted in both unprocessed and processed image series in 20 out of 22 image series at lowest dose level. These artifacts were rated as minor and did not interfere in diagnostic decision-making. Image contrast was found to be acceptable in all unprocessed and processed images.
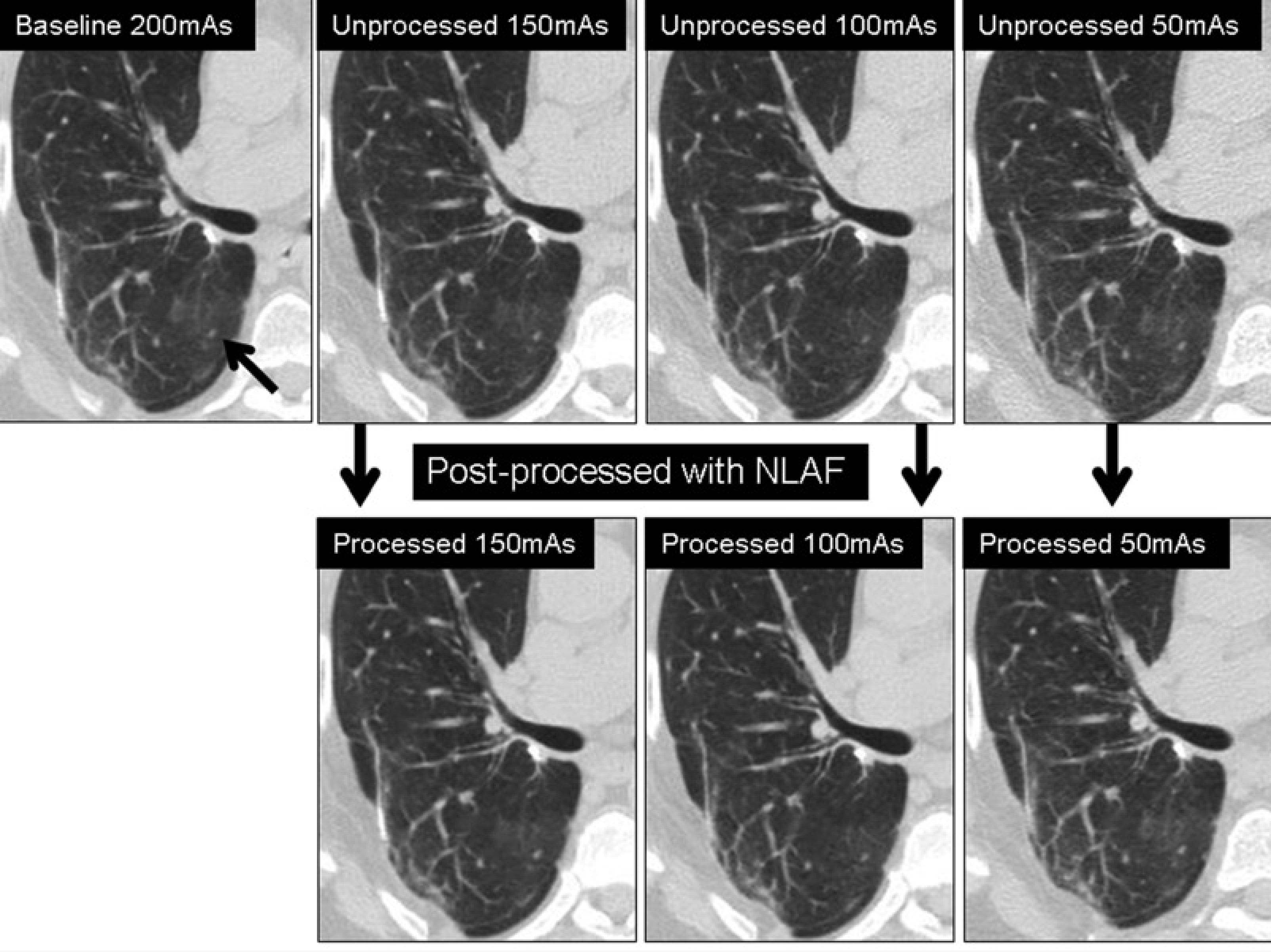
Transverse chest CT images in a 67-year-old woman weighing 77 kg with known history of carcinoid tumor of lung showing ground-glass opacity at four different tube current-time product levels (150, 110, 75, and 40 mAs). Three lower tube current-time product levels (110, 75, and 40 mAs) when processed with 2D-NLAF showed lower image noise and enhanced visibility of smaller structures, hence making 40 mAs low dose images diagnostically acceptable
Objective image quality
Detailed objective image quality scores for chest CT have been summarized in Table 2. Average objective noise (± standard deviation) for chest CT was decreased by 26% (14.2 ± 4.7/19.2 ± 6.4) in 110 mAs, 32% (15.2 ± 4.7/ 22.2 ± 5.7) in 75 mAs and 41% (16.9 ± 6/28.9 ± 10.2) in 40 mAs processed images compared to the corresponding mAs unprocessed image series (P < 0.0001). There was no significant change in the mean CT numbers in unprocessed and processed chest CT image series at four different radiation dose levels (P > 0.08–0.36).
Average objective image noise and HU values in chest CT examinations for NLAF processed and unprocessed image series at four different radiation dose levels. Objective image noise was decreased in NLAF processed image as opposed to unprocessed image series with no significant change in average HU values (P > 0.08–0.36)
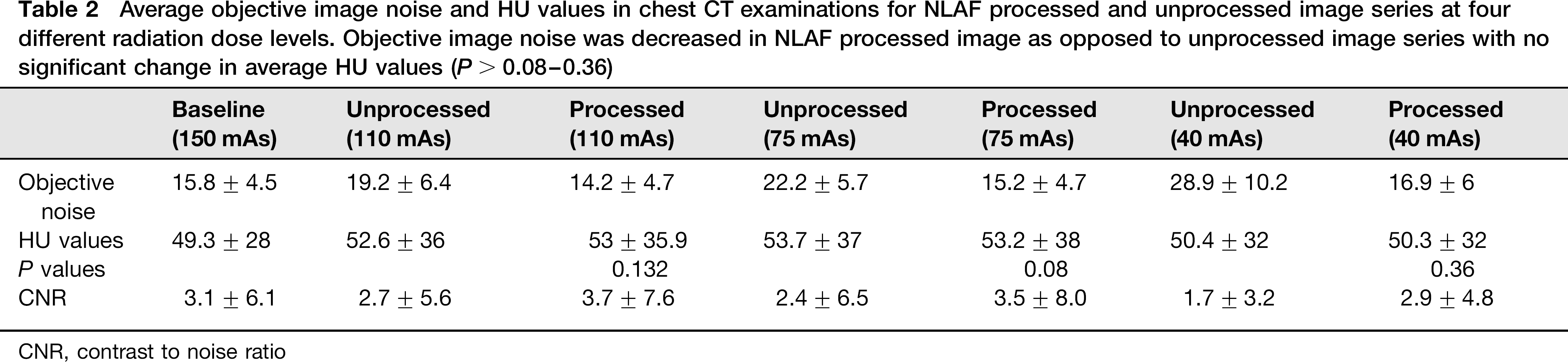
CNR, contrast to noise ratio
Radiation doses
CTDIvol for chest CT image series at 150, 110, 75, and 402 mAs were 12.6, 9.2, 6.3, and 3.2 mGy, respectively. DLP and estimated effective radiation doses for 150, 110, 75, and 40 mAs were 109.3, 71.8, 50.7, and 30.72 mGy-cm, and 1.5, 1, 0.7, and 0.42 mSv respectively.
Discussion
Our study shows that image noise can be lowered in chest CT images when processed by non-linear adaptive filters (NLAF) as opposed to unprocessed CT images. Indeed, subjective noise was acceptable in processed CT images at 40 mAs compared to unacceptable in unprocessed CT images at this dose level. Although NLAF reduced noise, postprocessing of CT images did not affect the image contrast or the lesion conspicuity. This trend was confirmed with objective noise measurements in chest CT images.
We also found that visibility of smaller structures, especially blood vessels in peripheral 2 cm of lungs, improved with NLAF. Due to the ability of the NLAF algorithms to separate image structures into different frequency components and process them separately, image noise in the thoracic soft tissue noise (mediastinum and chest wall) and visibility of smaller structures improved from selective edge enhancement in the lungs. This resulted in improvement of edge detection or improved conspicuity of smaller structures of lungs. Paradoxically, prior studies with some other non-linear filters have reported loss of visibility of small structures and decreased lesion conspicuity (12–14). Although we did not observe substantial improvement in lesion detection with the application of NLAF compared to baseline images in our study, it is conceivable that a larger sample size study with greater number of lesions and higher radiation dose reduction might have led to different observation with the application of NLAF.
Limitations of our study include small sample size of patients, which was primarily due to difficulty in recruiting patients, who are more aware of concerns associated with radiation induced hazards. Second, we did not use automatic exposure technique for dose modulation to assess the effect of NLAF, even though automatic exposure technique is used for routine clinical care. Fixed tube current settings was selected for the following reasons, foremost, it is required to adjust noise index (desired image noise for adjusting tube current), minimum and maximum tube current for each dose levels as well as for different patient size as automatic exposure control would have increased radiation dose to larger subjects and decreased the radiation dose for slimmer subjects. In addition, change in radiation dose with automatic exposure control is non-linear to the body size in order to avoid inadvertent use of high tube currents in larger subjects and too low tube currents in slimmer subjects.
Another limitation of our study is the fact that CT images were acquired in non-dynamic phase of contrast enhancement or without contrast enhancement. To decrease bias for lesion detection with repetitive review of four different dose levels with and without NLAF, radiologists were asked to assess the lesion conspicuity in images with highest noise and then evaluate the other dose levels.
Implications of our study include potential 75% radiation dose reduction for chest CT with NLAF used in our study. NLAF can enable acquisition of chest CT at 40 mAs, and perhaps at even lower mAs for evaluation of lung tissue window settings. Exact extent of dose reduction potential of NLAF may require further studies with acquisition of images at <40 mAs. Future studies may also be needed to assess advantages or disadvantages of NLAF approach for CT radiation dose reduction compared to hybrid or fully iterative reconstruction of CT images acquired at fractional dose levels.
In conclusion, 2D non-linear adaptive filters can allow reduction of tube current to 40 mAs for chest CT examinations while maintaining diagnostic confidence.