
Abstract
Background
The presence of muscularis propria invasion by bladder cancer is a key factor in prognosis and treatment decisions, although may be missed by biopsy due to sampling error. MRI has shown potential for detection of muscle invasion but has not specifically been evaluated for this purpose in the setting of bladder cancer patients without evidence of muscle invasion on initial biopsy.
Purpose
To evaluate the role of MRI in detection of muscularis propria invasion by bladder cancer following a pathologic diagnosis of non-invasive tumor.
Material and Methods
This retrospective study included 23 patients who underwent pelvic MRI following a pathologic diagnosis of bladder cancer without muscularis propria invasion and in whom additional histologic evaluation was performed following MRI. Two radiologists in consensus reviewed T2-weighted images to identify those cases suspicious for muscle invasion on MRI. The radiologists identified whether cases suspicious for invasion demonstrated disruption of the T2-hypointense muscularis layer of the bladder wall, peri-vesical fat stranding, and peri-vesical soft tissue nodularity. Findings were compared with pathologic results obtained after MRI.
Results
Suspicion was raised for muscle invasion in eight of 23 cases, four of which exhibited invasion on follow-up pathology. No case without suspicion on MRI exhibited invasion on follow-up pathology. Therefore, sensitivity and specificity were 100% and 79%, respectively. Among individual findings, muscularis disruption on T2WI exhibited sensitivity of 100% and specificity of 79%, peri-vesical fat stranding exhibited sensitivity and specificity of 50% and 84%, and peri-vesical soft tissue nodularity exhibited sensitivity and specificity of 25% and 100%.
Conclusion
MRI demonstrated high sensitivity for detection of muscle invasion in cases of bladder cancer without invasion on initial histologic assessment. Muscularis disruption on T2WI appeared to exhibit a better combination of sensitivity and specificity than did peri-vesical changes.
Preoperative staging of bladder cancer plays a central role in establishing patient prognosis and guiding management decisions. Specifically, it is critical to be able to reliably distinguish between tumors without invasion of the muscularis propria and those with muscle invasion (1). Non-muscle-invasive tumors are unlikely to be associated with metastatic disease and are thus treated via transurethral resection with or without intravesical therapy. On the contrary, localized muscle-invasive tumors have an increased potential for metastatic disease and are frequently treated with radical cystectomy or radiation therapy as well as systemic therapy.
Both CT and MRI have been explored for staging of bladder cancer (2). Of these, MRI has generally shown higher accuracies, attributed to its superior soft tissue contrast and ability to depict the muscularis propria as a distinct layer within the bladder wall (3–6). However, MRI is still not used in most clinical practices as a routine test in bladder cancer management. This may in part be attributable to the central role of pathologic determinations of stage in treatment selection. Tissue is necessarily obtained early in the course of disease and, if demonstrating muscle invasion, prompts aggressive therapy, whether or not this invasion is identified on imaging. Alternatively, if imaging suggests the presence of muscle-invasive tumor, this suspicion most often must be confirmed histologically prior to cystectomy given the enormous impact of this surgery on the patient.
One clinical setting in which there is potential for an increased role for imaging for primary tumor assessment is following an initial pathologic diagnosis of non-invasive bladder cancer. Biopsy has been documented to under-stage a significant fraction of tumors due to sampling error (7). Therefore, for patients with non-muscle-invasive tumors, repeat biopsy has been advocated for patients with either high grade disease or with invasion of the sub-epithelial connective tissue (stage T1 disease), as well as in cases in which there is an absence of muscle within the specimen (8). Unfortunately, adherence to such recommendations remains low due to both physician- and patient-related factors (9, 10). Suspicion for muscle invasion on imaging in these patients may facilitate earlier repeat tissue sampling. However, to our knowledge, no previous study has assessed the role of MRI specifically in this context. Therefore, the purpose of this study was to retrospectively evaluate the role of MRI in detection of muscle invasion that is not identified on initial histologic assessment.
Material and Methods
This retrospective study was approved by our institutional review board and compliant with HIPAA. Requirement for written informed consent was waived. Institutional databases were searched to identify patients who underwent MRI of the bladder following a biopsy that was positive for bladder cancer but without definitive evidence of muscle invasion and who also had a second histologic evaluation of the tumor following the MRI. A total of 23 patients (18 men, 5 women; mean age 72 ± 9 years, range 56–90 years) were identified.
MRI studies were performed between January 2003 and June 2011, and the MRI protocol at our institution varied given this long study period. However, all examinations were performed on a 1.5T system (Magnetom Avanto, Sonata, or Symphony; Siemens Healthcare; Erlangen, Germany) and included sagittal and axial turbo spin-echo T2-weighted imaging (T2WI) with typical parameters as follows: TR/TE 6000/116 ms, slice thickness 4 mm, field-of-view (FOV) 200-275 × 275 mm, matrix size 192–256 × 512, receiver bandwidth 200 MHz/voxel, 2 signal averages, parallel imaging factor of 2 for sagittal T2WI. All cases were retrospectively reviewed by two radiologists in consensus who knew that all examinations were performed following an initial pathologic result indicating non-invasive tumor, but unaware of subsequent pathologic findings. The radiologists classified each case in terms of presence or absence of findings suspicious for muscle invasion on multi-planar T2WI. For cases that were considered suspicious for invasion, the radiologists classified each of the following three factors as present or absent: disruption of the T2-hypointense muscularis propria layer of the bladder wall, peri-vesical fat stranding, and peri-vesical soft tissue infiltration. Between one and three factors could be classified as positive for each suspicious case.
Findings were correlated with evidence of muscle invasion on the pathologic specimen obtained after the MRI. The sensitivity and specificity for muscle invasion on the repeat biopsy based on suspicion for tumor on MRI were calculated. The three specific imaging findings assessed for all suspicious cases were all compared with the repeat pathology in summary fashion, and the sensitivity and specificity for these were calculated as well. In performing these calculations, the three imaging findings were considered to be absent in those cases in which there was no suspicion for muscle invasion.
Results
Pathologic findings
Among the 23 patients included in the study, the tumor grade on the initial pathologic assessment was reported using the WHO 2004 classification system in 20 cases (11), and was low-grade in seven patients and high-grade in 13 patients. The pathology report from the initial biopsy indicated an absence of muscle invasion in 16 patients, a lack of muscularis propria in the specimen in four patients, equivocal muscle invasion in two patients, and no comment regarding muscle invasion in one patient.
All 23 patients had repeat tissue analysis following the MRI. The repeat tissue was obtained via repeat biopsy in 16 patients and via cystectomy in seven patients. Four patients had muscle invasion on repeat tissue sampling. Of these four patients, the follow-up pathology was obtained via cystectomy in three patients and via biopsy in one patient. In addition, all four of these patients had high-grade tumor on the initial biopsy.
MRI findings
The two radiologists identified suspicion for muscle-invasion in eight patients, which included all four patients with muscle invasion on repeat tissue sampling. No patient without suspicion for muscle invasion on MRI exhibited muscle invasion on repeat pathologic analysis. Therefore, among the entire cohort of 23 subjects, MRI exhibited a sensitivity of 100% (4/4) and specificity of 79% (15/19) for detection of muscle invasion on repeat pathology.
Findings regarding presence of specific imaging findings are summarized in Table 1. Among the eight patients with suspicion for muscle invasion on MRI, all eight exhibited disruption of the muscularis propria, five exhibited peri-vesical fat stranding, and one exhibited peri-vesical soft tissue infiltration. Among the four patients with muscle invasion, all four exhibited muscularis disruption, two exhibited peri-vesical fat stranding, and one exhibited peri-vesical soft tissue infiltration. Among the four patients without muscle invasion, all four exhibited muscularis disruption, three exhibited peri-vesical fat stranding, and none exhibited peri-vesical soft tissue nodularity. Therefore, among the cohort of 23 patients, muscularis disruption exhibited a sensitivity of 100% (4/4) and specificity of 79% (15/19); peri-vesical fat stranding exhibited a sensitivity of 50% (2/4) and specificity of 84% (16/19); and peri-vesical soft tissue infiltration exhibited a sensitivity of 25% (1/4) and specificity of 100% (19/19). Figs. 1–5 show cases of MRI exhibiting either the presence of absence of these various findings.
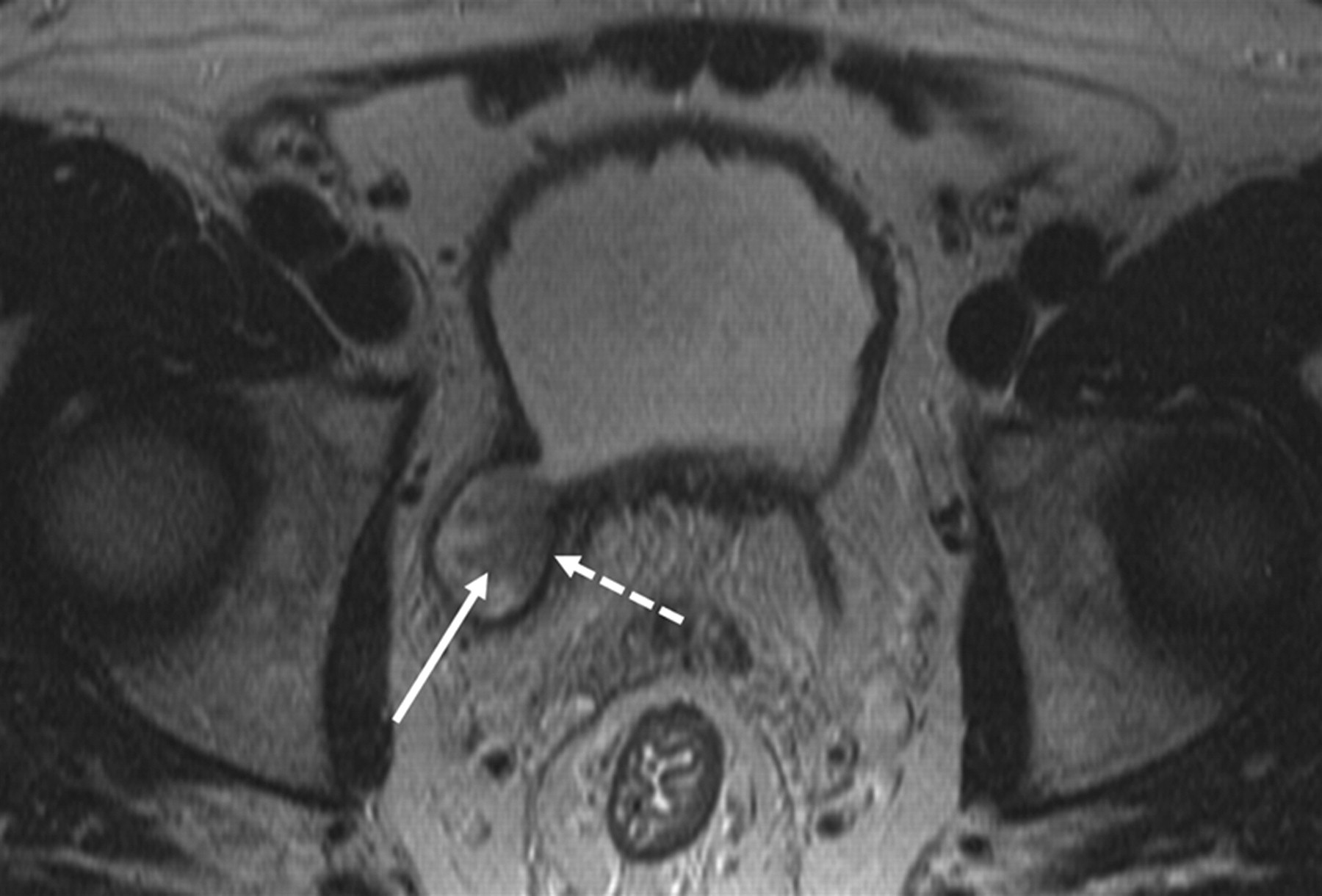
A 59-year-old man with prior biopsy of urothelial carcinoma within right-sided bladder pseudodiverticulum showing no evidence of muscle invasion. Axial T2-weighted MR image shows intermediate-signal mass within pseudodiverticulum (solid arrow) with intact overlying T2-hypointense muscularis layer (dashed arrow). The MRI was not considered suspicious for muscle invasion. On biopsy performed after the MRI, there was again no evidence of muscle invasion

A 56-year-old man with prior biopsy of urothelial carcinoma of the urinary bladder in which no muscularis was present. Axial T2-weighted MR image shows intermediate-signal mass within right posterolateral aspect of urinary bladder (solid arrow). There is disruption of the T2-hypointense muscularis layer (dashed arrow) by the tumor. Mild right hydroureter is also present (arrowhead). The MRI was considered suspicious for muscle invasion. On subsequent cystoprostatectomy, muscle invasion was observed
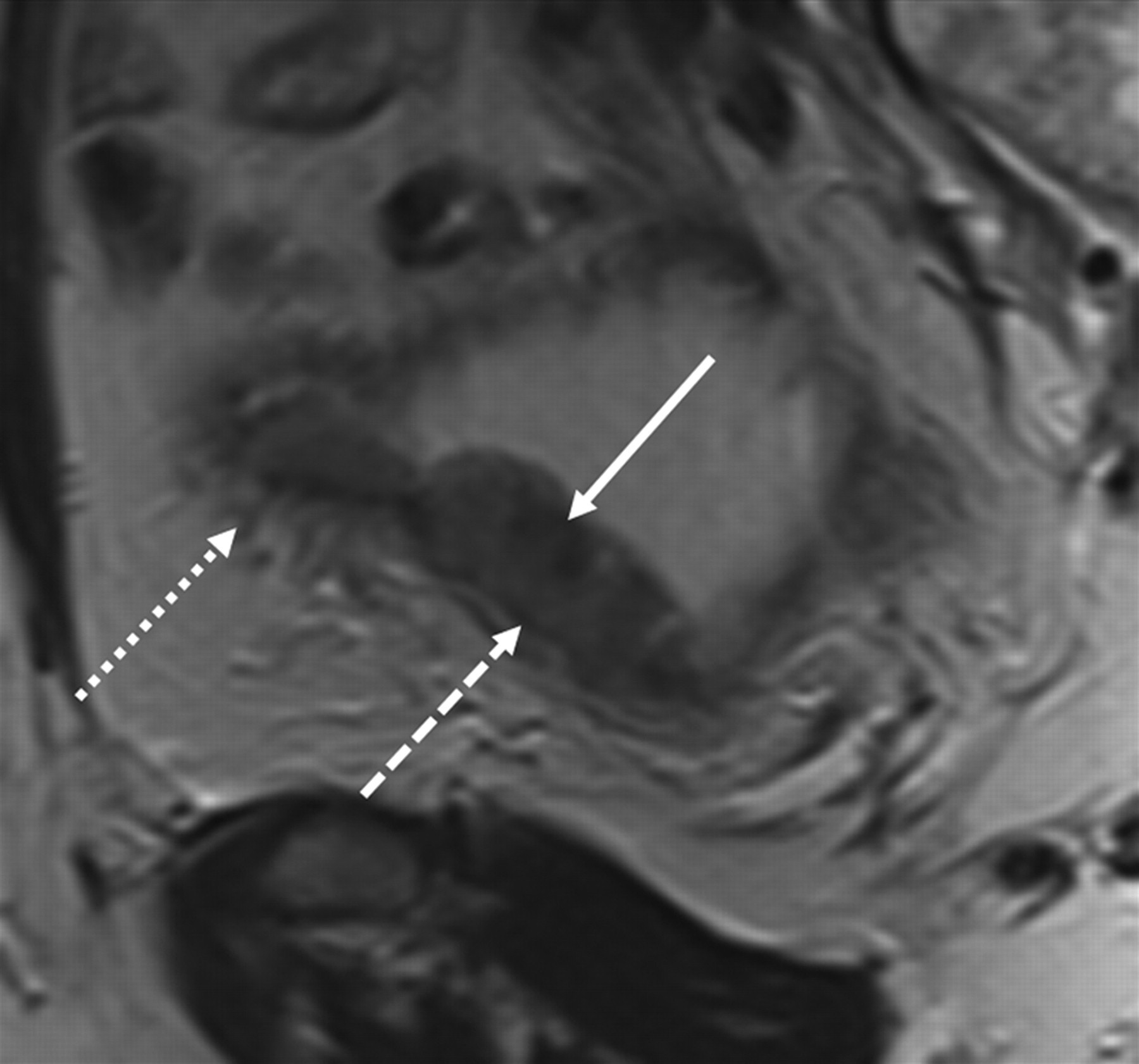
A 63-year-old woman with prior biopsy of urothelial carcinoma of the urinary bladder showing invasion of the lamina propria but no definite muscularis invasion. Sagittal T2-weighted MR image shows intermediate-signal mass within anterior aspect of urinary bladder (solid arrow). There is disruption of the T2-hypointense muscularis layer (dashed arrow) overlying the tumor as well as peri-vesical fat stranding (dotted arrow). The MRI was considered suspicious for muscle invasion. On subsequent cystectomy, muscle invasion was observed

A 73-year-old man with prior biopsy of urothelial carcinoma of the urinary bladder showing no evidence of muscle invasion. Axial T2-weighted MR image shows intermediate-signal mass within left lateral aspect of urinary bladder (solid arrow). The imaging was interpreted as demonstrating disruption of the T2-hypointense muscularis layer (dashed arrow) overlying the tumor. The MRI was considered suspicious for muscle invasion. However, on biopsy performed after the MRI, no muscle invasion was identified

A 67-year-old man with prior biopsy of urothelial carcinoma of the urinary bladder showing no evidence of muscle invasion. Sagittal T2-weighted MR image shows intermediate-signal mass within anterior aspect of urinary bladder (solid arrow). The imaging was interpreted as demonstrating disruption of the T2-hypointense muscularis layer (dashed arrow) overlying the tumor as well as peri-vesical fat stranding (dotted arrow). The MRI was considered suspicious for muscle invasion. However, on subsequent cystoprostatectomy, no muscle invasion was identified
Relationship between imaging findings relating to possible muscle invasion by bladder cancer and findings on pathology obtained after MRI. Note that in an additional 13 patients, none of the findings described below were identified, and pathology obtained after the MRI showed no evidence of muscle-invasive tumor
Discussion
In this study, we assessed the utility of MRI for detection of muscle invasion following an initial pathologic assessment that was either negative or indeterminate in this regard. Overall, MRI detected all cases with muscle invasion on subsequent pathology, with good specificity of 79%. We are unaware of previous data assessing the role of MRI in this precise setting.
The sensitivity and specificity for muscle invasion that we observed are similar to values reported in recent studies that did not specifically include only tumors that were non-invasive on initial histologic assessment. For instance, using a variety of MRI techniques, Takeuchi et al. reported sensitivities ranging from 88% to 94% and specificities ranging from 74% to 100% in differentiating non-invasive and invasive tumor (12). In addition, Tillou et al. reported a sensitivity and specificity of 80% and 90%, respectively (13). Furthermore, the greater sensitivity than specificity that we observed is consistent with at least four previous studies that reported overstaging of bladder cancer to be the most common error (5, 14–16). This overstaging has been attributed to poor contrast between the tumor and the bladder wall in some cases as well as to postprocedural inflammation (5, 12, 14).
The three specific imaging findings that were assessed for muscle invasion showed varying performance in comparison with the follow-up biopsy results. Past studies have evaluated imaging findings related to abnormalities of either the bladder wall or the peri-vesical fat. In this study, simple assessment of the integrity of the muscularis propria of the bladder wall on T2WI seemed to be the most useful sign for detection of muscle invasion given unacceptably low sensitivities for the other two findings. Indeed, this finding was observed in all cases that raised suspicion for invasive tumor. Peri-vesical fat stranding exhibited both several false-positives and false-negative interpretations in this small cohort and may have represented a reactive process given the previous intervention for all included tumors. Finally, peri-vesical soft tissue nodularity was observed in one patient in this study and ultimately was found to correspond with extra-vesical tumor on cystectomy; despite the specificity of this finding, it does not provide sufficient sensitivity to serve as a reasonable criterion for detection of invasive tumor.
Cross-sectional imaging of bladder cancer is largely utilized in patients with relatively advanced disease to assess for extra-vesical spread of tumor or for metastatic disease (17, 18). The clinical relevance of our work is in the suggestion of a potential role for incorporating MRI into the management of patients with lower risk features. This clinical role is particularly supported by the very high sensitivity that was observed. This sensitivity is of greater value than high specificity in this particular context given the importance of not missing a patient with potentially aggressive invasive tumor as well as the current standard to obtain a tissue diagnosis prior to radical surgery in most cases.
A number of strategies may be employed to try to further improve the accuracy of MRI for local staging of bladder cancer in comparison with what was observed in our study. First, two studies have suggested that diffusion-weighted imaging (DWI) may improve specificity of bladder cancer staging, possibly due to improved delineation between the tumor and the bladder wall on this sequence (12, 19). Because our study included patients dating back to 2003 prior to the routine use of DWI in body imaging, DWI was not performed for many of the subjects in our cohort, and this sequence was not included during our retrospective review. Second, two studies have reported improved local staging of bladder cancer using cross-sectional imaging following air insufflation of the bladder (20, 21). However, this approach is invasive and may not be practical in all patients. Finally, imaging the tumor prior to initial biopsy would be expected to improve specificity by reducing postprocedural inflammation that can result in over-staging (22). We feel that this approach, which generally is not part of current practice patterns, warrants prospective evaluation.
Our study has a number of limitations. First, the sample size was small, with only four cases of muscle-invasive tumor. In addition, the MRI protocol varied over the long time period of this study. Also, the pathologic specimens were not re-interpreted for the purposes of this study. Finally, given that two radiologists performed the assessment in consensus, inter-reader variability was not assessed.
In conclusion, we demonstrated a very high sensitivity of MRI for detection of muscle invasion in cases of bladder cancer without invasion identified on initial histologic assessment. The relatively weaker specificity that we observed is consistent with prior observations. Assessment for disruption of the muscularis on T2WI appeared to be a more useful imaging finding than assessment for peri-vesical changes in this determination. Future studies may attempt to further improve the accuracy of MRI in local bladder cancer staging as well as evaluate the role of bladder MRI in prospectively impacting patient management in this setting.