
Abstract
Background
Plasma D-dimer measurement is used in the assessment of the clinical probability of pulmonary embolism (PE), in order to minimize the requirement for pulmonary computed tomography angiography (CTA).
Purpose
To evaluate whether doubling the threshold value of serum D-dimer from 500 μg/L to 1000 μg/L could safely reduce utilization of pulmonary CTA to exclude PE in our emergency department patient population.
Material and Methods
Emergency department patients evaluated for PE with a quantitative D-dimer assay and pulmonary CTA were eligible for inclusion. D-dimer values were retrospectively collected in all included patients. Pulmonary CT angiograms were reviewed and scored as positive or negative for PE. Receiver-operating characteristic (ROC) analysis was used to determine the accuracy of quantitative D-dimer measurements in differentiating between positive and negative PE patients as per CTA.
Results
A total of 237 consecutive patients underwent pulmonary CTA and had a D-dimer measurement performed. Median D-dimer level was 1007 μg/L and in 11 (5%) patients the pulmonary CT CTA was positive for PE. The ROC curve showed an area under the curve (AUC) of 0.91 (P < 0.0001). Increasing the D-dimer threshold value of 500 μg/L to 1000 μg/L increased the specificity from 8% to 52% without changing the sensitivity.
Conclusion
Adjusting the D-dimer cut-off value for the emergency department community population and patient age increases the yield and specificity of the ELISA D-dimer assay for the exclusion of PE without reducing sensitivity.
Keywords
The diagnosis of thromboembolic disorders including deep vein thrombosis (DVT) and acute pulmonary embolism (PE) continues to be a major diagnostic challenge. The mortality rate of untreated PE is reported to be as high as 30% (1, 2). Unfortunately, the clinical manifestations of PE are variable and lack specificity to reliably diagnose or exclude clinically significant PE.
Plasma D-dimer, a degradation product of cross-linked fibrin, has been studied extensively as a first-line test to rule out PE (3). In the outpatient population presenting with dyspnea or pleuritic chest pain, different diagnostic algorithms, combining assessment of clinical probability and serum D-dimer testing, have been developed to improve the clinical accuracy for the diagnosis of PE (4, 5). In patients classified to be at high risk for PE based upon diagnostic algorithms, the diagnosis of PE can be confirmed using pulmonary computed tomography angiography (CTA).
Overall, there has been a significant increase in the use of pulmonary CTA by emergency physicians even in the low-risk population (6, 7). Unfortunately, pulmonary CTA is associated with significant radiation exposure and thereby carries the potential for increased cancer risk (8, 9). PE positivity rates for pulmonary CTA have been declining and are now less than 10% in many observational studies (10, 11).
Conventionally, a serum D-dimer level of 500 μg/L is used as the cut-off value, below which the diagnosis of PE can be ruled out in most patients (3, 12). In recent studies, raising this cut-off value increased the proportion of patients in whom PE could be safely excluded and thereby eliminated the need for pulmonary CT angiograms in a greater number of patients (13, 14). In this study, we retrospectively analyzed if doubling the cut-off serum D-dimer value to 1000 μg/L could effectively and safely reduce the use of CTA in our emergency department patient population.
Material and Methods
Study design
This was a retrospective review study of physician use of the D-dimer value and pulmonary CTA for ruling out PE. The Institutional Review Board of our hospital granted permission for this study.
Study setting and population
This study was conducted from January 1, 2010 to October 15, 2010 in the emergency department of a community hospital. All patients aged over 17 years that underwent pulmonary CTA and had a quantitative D-dimer performed were identified from the electronic radiology system.
Study protocol
Pulmonary CTA procedures were performed on a multi-detector row helical CT scanner (Lightspeed QX/I; GE Healthcare, Milwaukee, WI, USA) with 1.25-mm collimation and a pitch of 1.5:1. A volume of 150 mL of low-osmolar iodinated contrast material (64% iohexol; Omnipaque 300; GE Healthcare, Princeton, NJ, USA) was injected at a rate of 4.0 mL/s via a power injector.
All examinations included routine 2.5 mm thick axial and 1.3 mm thick coronal reformatted images. Additionally, thin slab maximum intensity projection (MIP) images (1.0-mm slab thickness) in a coronal and sagittal oblique projection were also reviewed. Cases were interpreted at the time of image acquisition by board-certified radiologists in the emergency setting with 5–30 years of experience. Secondary blind review of all images was performed by a board-certified radiologist specialized in chest imaging with >15 years of experience. In cases of discrepancy, consensus was negotiated. The findings of the pulmonary CT angiograms were interpreted as positive or negative. A positive finding resulted if a filling defect was present in one or more pulmonary arteries. A negative finding resulted if there was no filling defect and if there was normal enhancement of the pulmonary arteries.
The serum D-dimer value was determined using the Vidas® D-dimer Exclusion™ Assay (BioMérieux, Durham, NC, USA) and a mini-VIDAS® immunoassay system. Assays were performed according to the manufacturers' specifications. The manufacturer reports that a serum D-dimer level less than 500 μg/L fibrinogen-equivalent units should be considered normal.
Data analysis
Statistical analysis was performed with the statistical package SPSS for Windows (Version 15.0; SPSS, Chicago, IL, USA). Mean D-dimer values of PE positive vs. PE negative CTA studies were compared with an unpaired t test. Receiver-operating characteristic (ROC) curve analysis was performed to summarize the trade-off between sensitivity and specificity of different threshold D-dimer values that may be chosen to exclude PE. The non-parametric (trapezoidal rule) area under the ROC curve was calculated to represent the overall accuracy. Probability values <0.05 were considered significant. The McNemar chi-square test was used to estimate the statistical significance of the differences in specificity when utilizing different threshold D-dimer values.
Results
During a 10-month study period, a total of 237 consecutive emergency department patients underwent pulmonary CTA and had a D-dimer measurement performed as part of their evaluation of PE. The mean age of the patients was 56 years (range, 17–96 years) and 77% (183/237) were women. Median D-dimer level on admission was 1007 μg/L (range, 66–10,000). A total of 11 (5%) pulmonary CT angiograms were positive for PE and 226 (95%) were negative. The plasma D-dimer level was significantly higher in patients who demonstrated PE on CT scan compared with those who did not (P < 0.005) (Fig. 1).
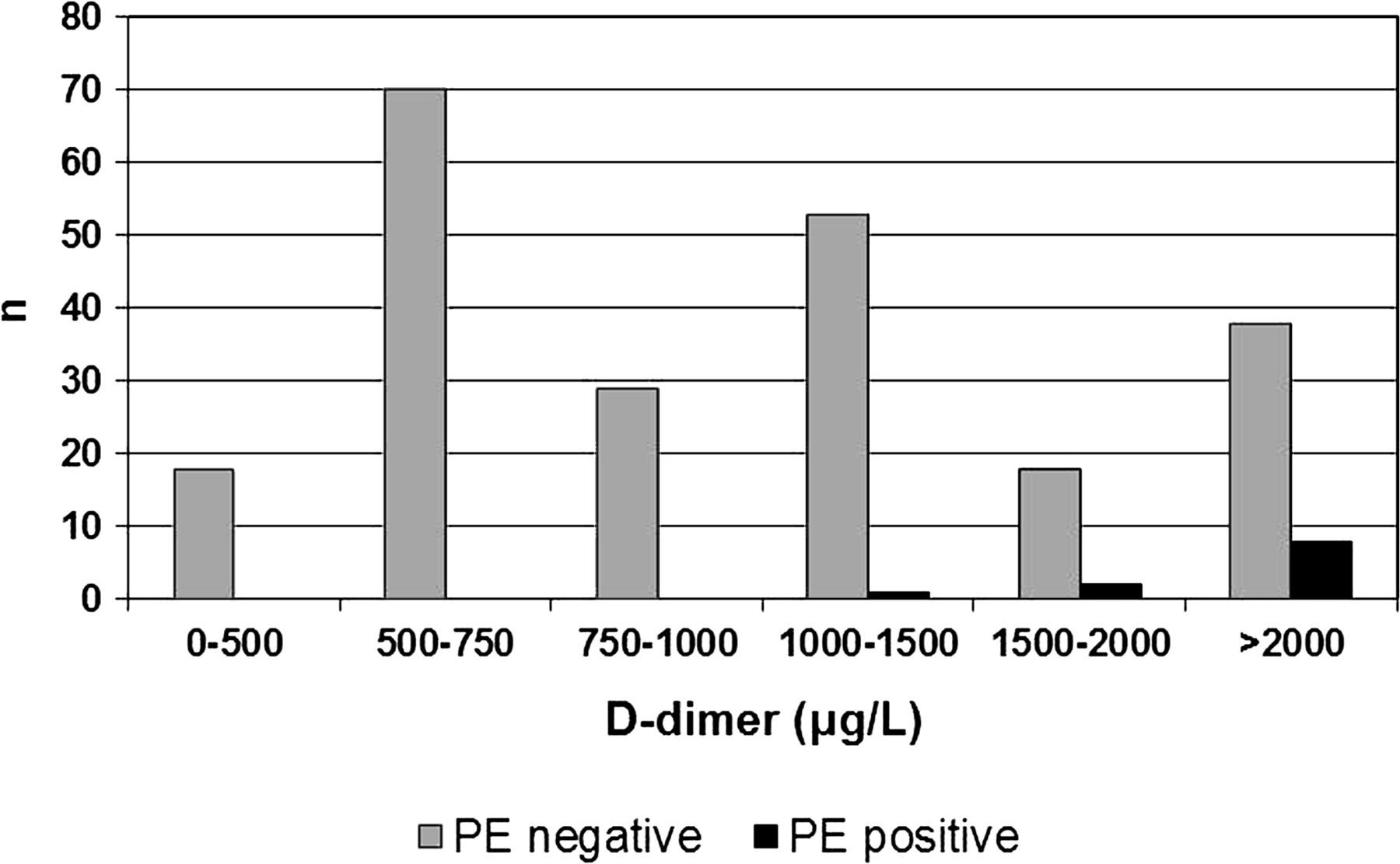
Bar graph showing the distribution of PE positive and PE negative patients (as per CTA results) for subsequent D-dimer values
The ROC curve was plotted with an area under the curve (AUC) of 0.91 (P < 0.0001, 95% confidence interval [CI] 0.867–0.944) (Fig. 2). D-dimer value was very sensitive when the standard threshold value of 500 μg/L was used, correctly categorizing 11 (100%) of 11 positive PEs with a sensitivity of 100% (95% CI, 67–100%), a specificity of 8% (95% CI, 5–12%), a positive predictive value (PPV) of 5% (95% CI, 3–9%), and a negative predictive value (NPV) of 100% (95% CI, 78–100%).
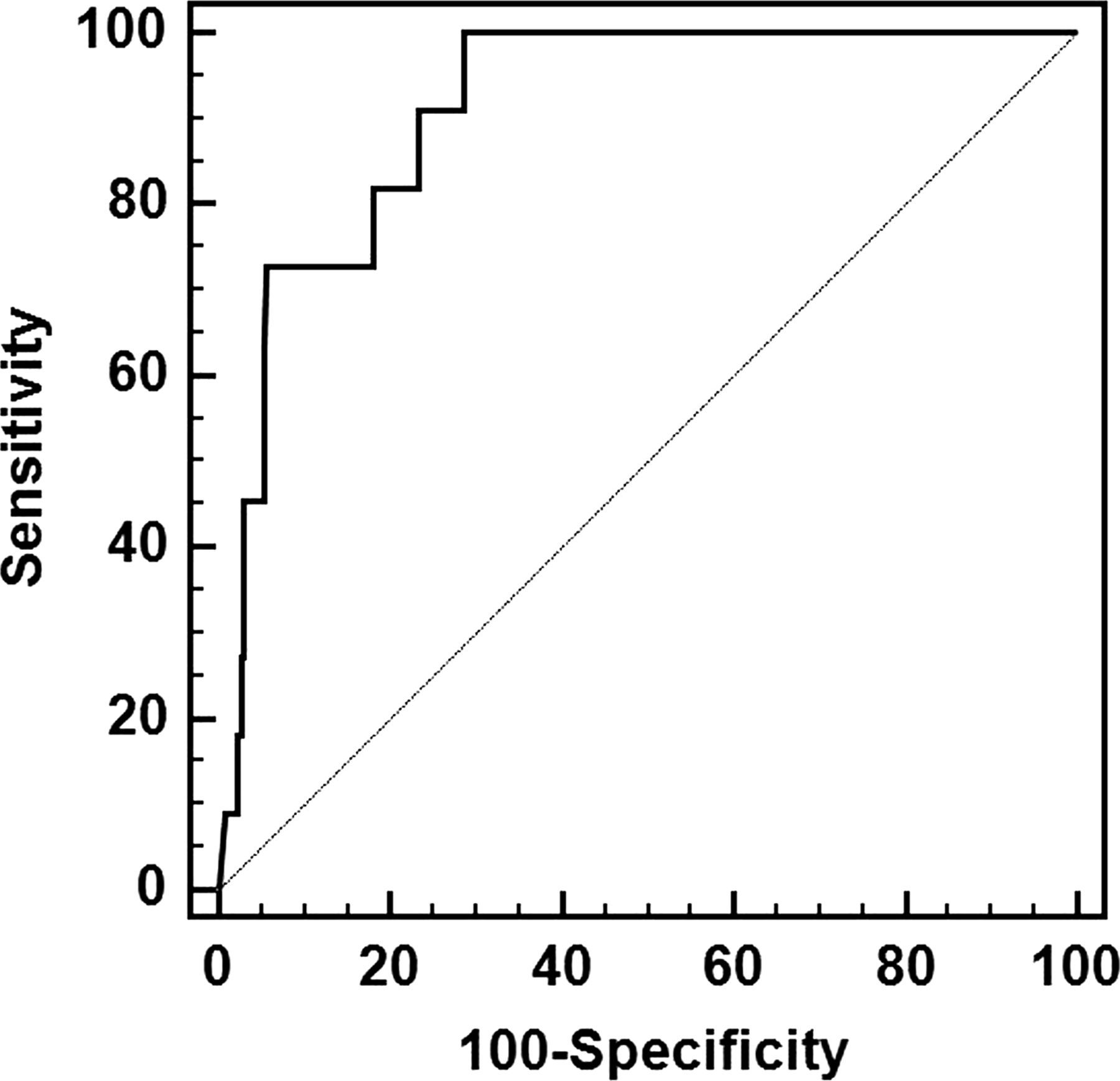
Receiver-operator characteristic curve (ROC) to predict the possibility of PE by measuring the level of D-dimer. Area under ROC curve by Wilcoxon estimate was 0.90 (95% CI, 0.856–0.936)
Increasing the threshold to 1000 μg/L included 11 (100%) of the 11 positive PE studies and increased the specificity; demonstrating a sensitivity of 100% (95% CI, 67–100%), a specificity of 52% (95% CI, 45–58%), a PPV of 9% (95% CI, 5–16%), and a NPV of 100% (95% CI, 96–100%). This is a significant difference in specificity when compared to the standard threshold value of 500 μg/L (McNemar test, P < 0.0001). The use of this increased cut-off value resulted in a 42% (99/237) absolute increase in the number of patients in whom D-dimer levels were considered normal. When the D-dimer cut-off level was set at 1500 μg/L, the sensitivity was 91% (95% CI, 57–99%), the specificity further improved to 75% (95% CI, 69–81%), and the PPV and the NPV were 15% (95% CI, 8–27%) and 99% (95% CI, 96–100%), respectively.
Subsequently we stratified the patients by age (Fig. 3) and examined the effects of an age adjusted D-dimer cut-off value for patients older than 50 years (n = 131). In this age group, the use of the standard threshold value of 500 μg/L showed a sensitivity of 100% (95% CI, 31–100%), a specificity of 5% (95% CI, 2–10%), a PPV of 2% (95% CI, 1–7%), and a NPV of 100% (95% CI, 52–100%). Increasing the threshold to 2000 μg/L resulted in a sensitivity of 100% (95% CI, 31–100%), a specificity of 81% (95% CI, 73–87%), a PPV of 11% (95% CI, 3–30%), and a NPV of 100% (95% CI, 96–100%). The use of the age-adjusted cut-off value resulted in a 75% (98/131) absolute increase in the number of patients in whom D-dimer levels were considered normal.

Scatter plot showing the correlation between D-dimer value and patient age
Discussion
Diagnostic algorithms involving clinicians' assessments of pretest probability and D-dimer testing have been shown to be useful in stratifying patients into those who do and do not require further testing (4, 5). Recently, there has been an increase in D-dimer tests ordered in the emergency department patient population presenting with chest pain or shortness of breath. Using current guidelines, an increased D-dimer value (>500 μg/L) often supports the argument for further work-up, resulting in an increase in the total number of patients examined with pulmonary CTA. One of the major disadvantages of pulmonary CTA is radiation exposure (6, 7, 15). Studies have shown an estimated effective dose per scan of 10–20 mSv, adding to an increased overall life-time cancer risk for the patient (8, 16, 17). At the same time, several investigators have shown that the prevalence of PE among patients being evaluated with CTA is less than 10% in many observational studies (10, 11).
A guiding paradigm in medicine is that the benefit to the patient from any procedure should outweigh any incurred risks. Proper clinical testing can avoid possible exposure to ionizing radiation, intravenous contrast material, and unnecessary treatment for false-positive diagnoses (7, 12, 15). Although the sensitivity of the D-dimer assay using standard cut-points is high, excluding PE with 90–95% accuracy, this examination is not specific since several other conditions such as surgery, malignancy, inflammation, pregnancy, and trauma can produce a falsely elevated D-dimer. By adjusting the cut-off points in specific patient populations, test specificity can be improved and thereby the number of patients undergoing unnecessary pulmonary CTA can be decreased.
The emergency department patient population represents a relatively healthy patient group when compared to the inpatient population. Righini et al. showed that in a subgroup of patients with a low clinical risk for PE, increasing the D-dimer threshold to 1000 μg/L would have excluded PE in 69% instead of 45% of the patients, with a minimal decrease in the negative predictive value (from 100% to 98%) (18). In our study, we showed that in emergency department patient population doubling of the standard D-dimer threshold value of 500 μg/L to 1000 μg/L resulted in a 42% absolute increase in the number of patients in whom D-dimer levels were considered normal. There was an increase in the specificity from 8% to 52% and an increase in the positive predictive value from 5% to 9%, without a compromise in the sensitivity.
Baseline D-dimer concentration increases with age, likely due to co-morbid conditions (19). Therefore, the specificity of D-dimer tests decreases and the number of false-positive results increases in elderly (20). Recent studies showed that age adjusted D-dimer cut-off points can increase the proportion of older patients in whom PE can be safely excluded (13, 14, 21). Douma et al. proposed the use of an adjusted D-dimer cut-off value in patients aged >50 years, calculated as (patient's age ×10) μg/L. The use of this age-adjusted cut-off value resulted in a 6.3% absolute increase in the number of patients in whom D-dimer levels were considered normal (13). In line with these findings, we showed that in older emergency department patient (>50 years) an increase in threshold value from 500 μg/L to 2000 μg/L significantly improved the specificity (from 5% to 81%) without lowering the sensitivity. The use of the age-adjusted cut-off value resulted in a 75% (98/131) absolute increase in the number of patients in whom D-dimer levels were considered normal.
Our analysis has limitations. Although D-dimer results were collected prospectively, this study was a retrospective analysis and only included those patients that underwent pulmonary CTA and had a quantitative D-dimer performed. The retrospectively nature of the study limited the collection of data regarding pre-test probability and alternative diagnosis to explain the patient's symptoms and elevated D-dimer levels. Physician participation in careful clinical assessment should be prioritized in order to avoid inappropriate use of D-dimer testing. Second, this study was performed in a community hospital emergency department, and the results may not be applicable to academic health centers or hospitalized patients. Furthermore, this study showed a relatively small number of positive pulmonary CT angiograms. Therefore, our results should be interpreted carefully and the results should be validated prospectively in a multicenter study.
In conclusion, a D-dimer cut-off value adjusted for the emergency department patient population and patient age increased the yield and specificity of the ELISA D-dimer assay for the exclusion of PE without reducing sensitivity. This new cut-off value could reduce utilization of pulmonary CTA.