
Abstract
Background
Intracranial chondromas are rare benign tumors. To date, few data are available on their neuroradiological features.
Purpose
To describe a series of patients with intracranial chondroma and to analyze and discuss the computed tomography (CT) and magnetic resonance imaging (MRI) features that may distinguish chondromas from other intracranial neoplasms.
Material and Methods
We retrospectively analyzed clinical and medical imaging data of six patients who had pathologically confirmed intracranial chondromas in our two institutions between July 2006 and September 2011. Both CT and MRI scanning were performed in all six cases.
Results
Five tumors were located at the skull base and one originated from the falx. CT images revealed well-demarcated, irregular lobulated and variable density masses with obvious calcification (6/6), no or slight enhancement, without peritumoral edema, and frequently accompanied by erosion and destruction of surrounding bone (5/6). Tumor parenchyma appeared heterogeneously hypointense on T1WI, and hyperintense or mixed hyperintense and hypointense on T2WI, while the calcification appeared hypointense on T1WI and T2WI in five cases, demonstrating significant inhomogeneous enhancement on postcontrast MRI, which revealed the typical “punica granatum seeds” sign. Only one case showed homogeneous low signal intensity on T1WI and high signal intensity on T2WI, and relatively uniform obvious enhancement on postcontrast scans.
Conclusion
These characteristic CT and MR findings, combined with the location of the lesions and the history of a long duration of clinical symptoms, may prove helpful in differentiating intracranial chondromas from other more common tumors.
Chondromas are slow-growing, benign bone tumors of cartilaginous origin. They can be found in any part of the body that contains cartilaginous bone, and frequently occur in short tubular bones, especially the metacarpals and the phalanges (1). Their intracranial occurrence is extremely rare and represents approximately 0.2–0.3% of all intracranial primary tumors (2). They usually arise from the skull base synchondroses, and are particularly prevalent in the middle cranial fossa (3). However, cases of intracranial chondromas originating from the convexity dura, the falx, the posterior fossa dura, the choroid plexus, or the brain parenchyma have also been reported (3–7). The first reported case of intracranial chondroma was by Hirschfield in 1851 (4). To date, there have been few reports of the characteristic imaging appearances of intracranial chondromas, and these have mostly been case reports. As the incidence of intracranial chondromas is extremely low, and their clinical symptoms and radiographic appearance are usually non-specific, they can easily be misdiagnosed as other tumors, which affect both the treatment and prognosis. The current paper presents a series of cases, as well as an analysis and discussion, of the clinical manifestations, imaging features and pathological characteristics of intracranial chondromas, thereby aiming to reduce the frequency of misdiagnosis.
Material and Methods
Patients
Following approval from our institutional hospital review board, we reviewed cross-referenced records between July 2006 and September 2011 in the departments of radiology, neurosurgery, and pathology of our two hospitals. We identified six patients with pathologically confirmed intra-cranial chondromas. The six patients included three men and three women, aged between 15 and 69 years, with a mean age of 33.3 years. Most patients had complained of non-specific symptoms, including headache (n = 5) and vomiting (n = 2). Other presenting symptoms were diplopia (n = 3), impaired vision (n = 2), blurred vision (n = 2), visual field defects (n = 1), blepharoptosis (n = 1), anosphrasia (n = 1), ocular motility disorder (n = 1), facial paralysis (n = 2), and limb weakness with unsteady gait (n = 2). The duration of clinical symptoms ranged from 6 months to 96 months, with an average duration of 33.5 months. The final diagnoses were confirmed by surgical pathology. The CT and MR findings of the six patients, together with their clinical data, are detailed in Table 1.
CT and MR findings and clinical data of six patients with intracranial chondromas
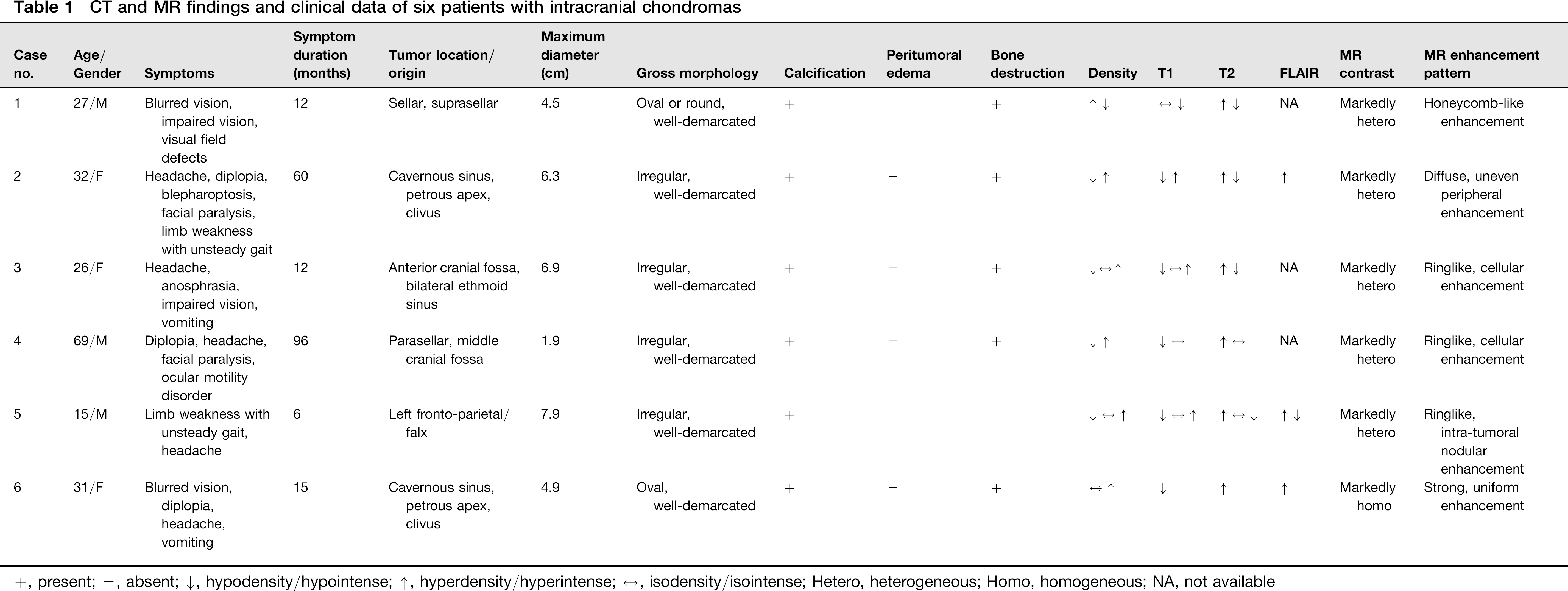
+, present; -, absent; 4↓, hypodensity/hypointense; ↑. hyperdensity/hyperintense; ↔, isodensity/isointense; Hetero, heterogeneous; Homo, homogeneous; NA, not available
Imaging techniques
All six patients underwent CT and MR imaging. All MR imaging was performed on a 1.5T (Magnetom Vison plus 1.5T, Siemens, Erlangen, Germany) scanner. Pregadolinium T1-weighted spin-echo images (TR, 450 – 600 ms; TE, 14 –20 ms), T2-weighted spin-echo images (TR, 4500–5500 ms; TE, 100–120 ms), and gadolinium-enhanced (Magnevist; Bayer Schering Pharma, Berlin, Germany; 0.1–0.2 mmol/kg [body weight]), T1-weighted images were acquired in the axial, coronal, and sagittal planes. All clinical CT examinations were obtained with a Somatom Plus 4 scanner (Siemens, Erlangen, Germany). All axial CT scans were obtained from the vertex to the skull base using a 3 mm section thickness, 120 kV, and 150–200 mAs before and after the intravenous administration of contrast agent (Omnipaque 300 mg I/mL; 1.5–2.0 ml/kg [body weight]; injection rate, 2.0–3.0 mL/s).
Image analysis
Each MR and CT image was retrospectively reviewed by two experienced neuroradiologists who had no knowledge of the histology. Where there was disagreement, a consensus decision was agreed upon. The MR images and CT scan characteristics were analyzed, with particular attention focusing on the location and size of the lesion, as well as local extension, shape, margin, cerebral edema, internal architecture such as the presence of calcification, density, signal intensity, enhancement pattern, and destruction of surrounding bone.
Results
Imaging findings
The tumor was located in the anterior cranial fossa and the bilateral ethmoid sinus and intruding upwards into the bilateral frontal lobe in one patient (Fig. 1); in the sellar and suprasellar regions in one patient (Fig. 2); in the parasellar area and middle cranial fossa in one patient; in the falx region in one patient (Fig. 3); and at the cavernous sinus – petrous apex – clivus region and crossing the middle cranial fossa and posterior fossa in two patients (Fig. 4). The tumors ranged in size from 1.9 to 7.9 cm in maximum diameter, with a mean diameter of 5.4 cm. Two lesions were oval or round, and the remaining four lesions were irregular masses. All six tumors had a distinct margin without peritumoral edema.
Case 3: Intracranial chondroma in a 26-year-old woman. MR and CT images demonstrate that the tumor is multi-lobulated and well demarcated, and is located in the anterior cranial fossa and bilateral ethmoid sinus extending into the bilateral frontal lobe. Axial T2-weighted image (a) shows a mass with both hyperintense and scattered hypointense areas (arrow). Axial T1-weighted image (b) shows an inhomogeneous hypointense mass with hyperintense foci in the center and isointense intratumor separation. Axial (c), coronal (d), and sagittal (e) postcontrast T1-weighted images demonstrate the mass with significant heterogeneous ringlike, cellular enhancement. Precontrast axial routine CT image (f) and bone window image (g) display a mixed density mass with hypoattenuation and a large amount of sheet, punctate and irregular calcifications, accompanied by erosion of the anterior cranial fossa bone, ethmoid labyrinth, and cribriform plate. In addition, an irregular mass can be identified in the bilateral ethmoid and sphenoid sinus infiltrating into the bilateral fossa orbitalis and the left frontal lobe, with similar signal characteristics to the primary lesion on coronal (h) and sagittal (i) contrast-enhanced T1-weighted images 18 months after subtotal resection of the tumor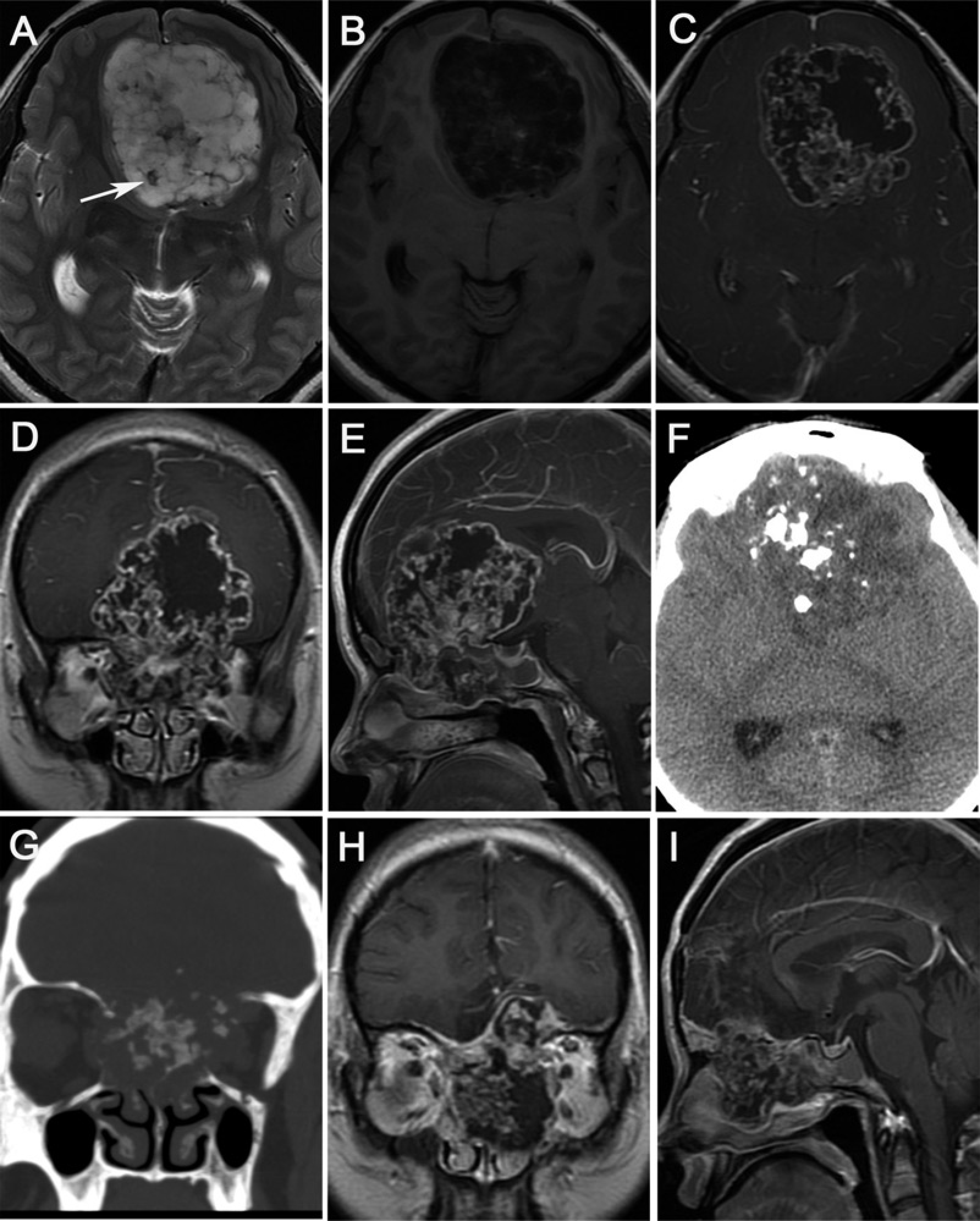
Case 1: Intracranial chondroma of the sellar and suprasellar region in a 27-year-old man. Axial T2-weighted image (a) shows a mass with uneven hyper-intense and punctate and linear hypointense areas. Coronal (b) and sagittal (c) T1-weighted images show a hypointense mass, interspersed with punctate and linear isointense. In addition, compression and displacement of the optic chiasm and the pituitary can be seen. Coronal (d) and sagittal (e) postcontrast T1-weighted images exhibit obvious non-uniform honeycomb-like enhancement. An axial routine CT image (f) reveals a well-defined mass with multiple calcified plaques and hypodense areas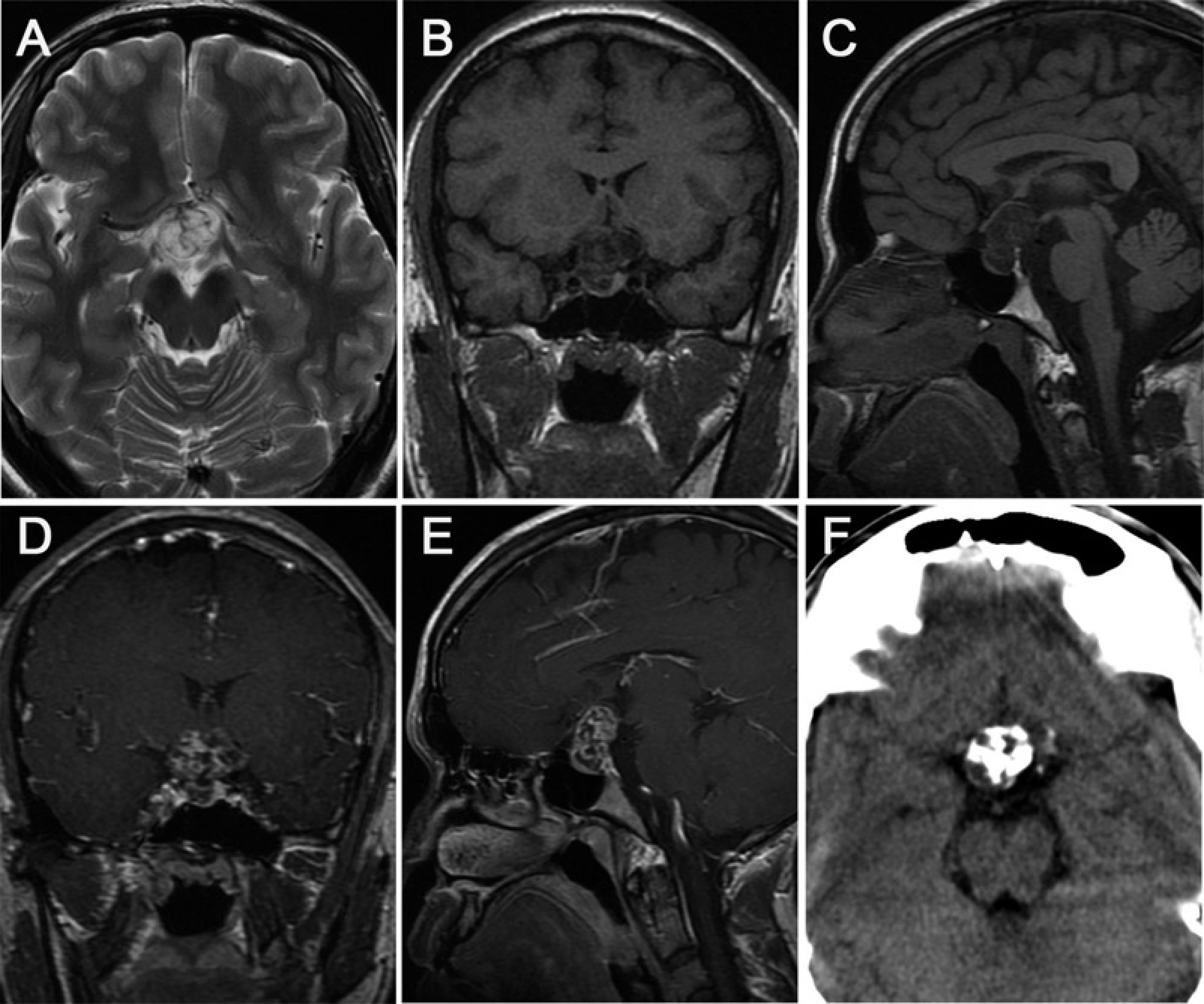
Case 5: Intracranial falcine chondroma in a 15-year-old boy. MR images show a huge space occupying lesion located in the left frontal and parietal lobes with clear contours. The tumor is connected to the falx cerebri and the left cranial vault dura with a broader base. The tumor parenchyma appears as heterogeneously hyperintense on T2-weighted image (a), hypointense on T1-weighted image (b), and slightly hyperintense on FLAIR image (c). Multiple strip and spot hypointense areas along the intracranial tumor margin (arrows) and within the tumor are portrayed clearly on the T1-weighted image, T2-weighted image, and FLAIR image. In addition, hyperintense foci scattered in the tumor can also be identified on the above sequences. Axial (d), coronal (e), and sagittal (f) postcontrast T1-weighted images reveal marked ringlike and intratumoral nodular enhancement, and no enhancement of the hypointense areas are seen on the T1-weighted image, T2-weighted image and FLAIR image (arrows). Furthermore, the “dural tail” sign can be found on contrast-enhanced T1-weighted MRI (arrowheads)
Case 6: Intracranial chondroma in a 31-year-old woman. MR and CT images demonstrate an oval well-circumscribed space occupying mass located at the left cavernous sinus- petrous apex- clivus region and crossing the middle cranial fossa and the posterior fossa with a broad basilar part attached to the skull base (long arrows). The tumor parenchyma is homogeneously hyperintense on T2-weighted image (a), hypointense on T1-weighted image (b) and slightly hyper-intense on FLAIR image (c), with strong and relatively uniform enhancement on postcontrast T1-weighted images (d-f), suggesting rich blood supply of the tumor. The left cavernous sinus is surrounded and the adjacent brain stem is clearly shifted and deformed. A plain axial routine CT image (g) depicts an isodense or slightly low density mass with a blurred boundary and a little punctate calcification. In addition, erosion of the left petrous apex and dorsum sellae is clearly demonstrated on the CT bone window image (short arrow, h). A photomicrograph (i) shows that the tumor consists of mature hyaline cartilage, with absence of nuclear atypia or pathological mitoses of the chondrocyte. There is abundant uniform mucus in the cartilage matrix (H&E stain, original magnification × 200)
On plain CT images, the density of all six lesions varied, as they contained multiple or scattered patchy, striplike, sheet, punctate, and irregular calcifications (Figs. 1 and 2). Postcontrast CT scans detected slight and uneven enhancement in five cases, and lack of early enhancement in one case. In addition, the adjacent bone was affected in five patients (Figs. 1g and 4h).
On MR imaging, only one case showed homogeneous low signal intensity on T1WI and high signal intensity on T2WI, and displayed relatively uniform obvious enhancement on postcontrast scans (Fig. 4). The other five lesions appeared heterogeneously hypointense on T1-weighted images (n = 5), unevenly hyperintense (n = 2), or mixed hyperintense and hypointense (n = 3) on T2-weighted images, and surrounded by an arc-shaped short-T2 signal intensity rim (n = 4), in which patchy areas of longer T1 and longer T2 signal intensities were observed (n = 2) (Fig. 3). Contrast-enhanced MR images revealed significant inhomogeneous, ringlike, and intratumoral honeycomb-like enhancement (n = 5) (Figs. 1–3). The multiple strip, spot, and irregular calcifications within the tumors were hypointense on T1WI and T2WI without enhancement in five cases (Fig. 3). Furthermore, due to tumor expansion or invasion, compression and displacement of the middle cerebral artery was observed in two cases; the adjacent brain parenchyma, ventricle, and cistern were shifted and deformed in five cases (Figs. 1, 3, and 4); and the cavernous sinus was surrounded in three cases (Fig. 4). One lesion in the anterior cranial fossa and the bilateral ethmoid sinus, which had undergone a subtotal resection, recurred and transformed into a chondrosarcoma 18 months after surgery. A new mass appeared in the bilateral ethmoid and sphenoid sinus, and its signal characteristics looked similar to those of the primary lesion on plain and enhanced MRI scans (Fig. 1h, i).
Pathology findings
All lesions were surgically resected and the diagnosis was confirmed by histopathologic examination. During the surgical procedure, a lobulated, well-demarcated, gray red or off-white mass with a capsule and smooth surface was revealed. The majority of the chondromas had a rich blood supply and was not easily separated from the adjoining skull attachment (n = 4). The lesions felt hard in one case, fragile in two cases, and the texture was uneven in three. Microscopic examination confirmed that the tumors consisted of mature hyaline cartilage of varying sizes with partial calcification. The tumor cells situated within the lacunar spaces were unevenly distributed and of varying size. Nuclear atypia or any pathological mitoses of the cells were not found in any of the tumors. There was abundant uniform mucus and a small amount of fiber in the cartilage matrix (Fig. 4i). In all six cases, immunohistochemical staining demonstrated that the tumors were positive for vimentin and S-100 protein and negative for epithelial membrane antigen (EMA).
Discussion
Intracranial chondromas are extremely rare and benign neoplasms that characteristically form mature cartilage, accounting for approximately 0.2% to 0.3% of all intracranial primary tumors (1,2). These tumors usually occur in young adults with a peak incidence in the third decade (5,6). The age of patients reported in the literature ranges from 15 months to 60 years (7). Several publications have reported a slight female preponderance (3). In the present study, patients’ age ranged from 15 years to 69 years, with a mean age of 33.3 years, and a male-to-female ratio of 3:3.
The vast majority of the tumors are extramedullary (70–80%), and the predominant site is the skull base, especially the middle cranial fossa, the parasella, petrous apex, spheno-petrosal, spheno-occipital, and petro-occipital synchondroses (8,9). However, intracranial chondromas originating from less common sites such as the convexity dura, the falx, the tentorium, the choroid plexus, and the brain parenchyma have also been reported (1, 3, 10–14). In our study, the tumor was located in the skull base in five patients and in the falx region in one patient. Our findings are therefore consistent with previous observations. Intracranial chondromas can occur as solitary lesions or as part of Maffucci's syndrome (multiple enchondromatosis associated with soft tissue angiomas) or Ollier's disease (multiple polysystemic enchondromatosis) (15,16). Intracranial chondromas differ from chondromas in other locations in the body as a result of their expansile and irregular growth patterns.
Endochondral bone formation in the base of the skull occurs during the embryonic stage, and there are often some residual embryonic chondrocytes at the basilar synchondroses, which is why most intracranial chondromas occur in this region. The exact pathogenic mechanism implicated in the development of chondromas in the convexity dura, the falx, and the brain parenchyma remains unknown. Several hypotheses have been suggested, including chondroma development from heterotopic chondrocytes (1,17), and tumor development secondary to metaplasia of perivascular mesenchymal tissue or meningeal fibroblasts (18). Therefore, we believe an understanding of the histological origin is important for the identification of tumors that occur in unusual locations.
In general, the clinical presentation of intracranial chondromas is non-specific and depends on the tumor size and site. The slow-growing nature of these tumors means that they can be clinically silent for relatively long periods prior to diagnosis. The most common presenting symptoms include headache due to raised intracranial pressure, and multiple cranial nerve lesion involvement, which may result in diplopia, impaired vision, blurred vision, visual field defects, blepharoptosis, deafness, tinnitus, hearing loss, anosphrasia, ocular motility disorders, facial paralysis, and limb weakness with unsteady gait.
Surgical removal is the treatment of choice, as complete removal with careful resection of all dural attachments can result in an excellent long-term outcome (19,20). There has been a report of a patient who underwent total or subtotal tumor resection who remained disease-free for more than 40 years (21). Occasionally, cranial base chondromas are closely correlated with structures in that region. In these cases, subtotal or partial resection may be performed in order to avoid injury to nearby cranial nerves or major blood vessels and other important structures (22), resulting in the possibility of tumor recurrence and rarely, malignant transformation. In our series, five patients had complete excision and showed no obvious signs of tumor recurrence on postoperative MRI assessment during the 5- to 62-month follow-up period. One patient underwent subtotal resection and subsequently presented with tumor recurrence, which was confirmed as a well-differentiated chondrosarcoma, 18 months after the original operation. This patient received further surgery followed by radiation therapy. However, the long-term outcome is as yet unknown as the follow-up period to date has been relatively short. Previous reports have demonstrated that postoperative radiation therapy is not advised for residual tumor or non-operative patients, as chondromas do not respond well to irradiation and can potentially undergo malignant transformation (23,24).
Imaging features aid the pretreatment diagnosis when an intracranial chondroma is clinically suspected. However, the published literature on this to date mainly consists of case reports. According to these, intracranial teratoma is frequently seen as a lobular well-circumscribed mass with calcification (60–90%), accompanied by erosion and destruction of surrounding bone (50–60%), hyperostosis of the inner table of the skull, with no or minimal peritumoral edema, variable tumor density on CT (due to variable degrees of calcification and possible cystic degeneration), and exhibiting no or mild early enhancement and characteristic delayed enhancement after contrast administration, which is due to relatively slow blood flow within the tumor (3, 4, 9, 25–28). Lacerte et al. (29) classified the tumor into two distinct types based on imaging findings: Type I tumors are considered the classic and more common type, and these lesions appear uniformly isodense and homogenous on CT. On the other hand, type II tumors appear hypodense in the central area.
The CT findings in our six patients with intracranial chondromas were similar to those previously reported. The presence of calcification and the destruction of neighboring bone are usually the dominant features of intracranial chondromas. In our study, multiple punctate, striplike, sheet, round, irregular, or characteristic ring calcifications were observed in all patients. The incidence of calcification and bone destruction was 100% and 83.3%, respectively, in our group, which was higher than that previously reported (23,27).
MR imaging can offer invaluable information on localization, the extent of the tumor, as well as the anatomic relationship between the tumor and adjacent structures, all of which are of vital importance for treatment planning and assessment. In published literature to date, the tumor has been described as low or isointense lesions on T1WI and with a mixed hyperintense and hypointense appearance on T2WI, with a broader basilar part linking with the skull base. Tumoral calcification mostly demonstrates low signal intensity on T1WI and T2WI, and intratumoral cysts display low SI on T1W1 and high SI on T2WI, similar to the water signal. Slight ring-like enhancement after the administration of contrast agent has been reported (4,7). Some angiographic studies have found that these tumors are characteristically avascular (4, 6, 7, 9, 13, 20, 23, 29). Our results partly confirmed these findings.
In our study, the internal architecture was best represented on T2-weighted images, in which all lesions displayed inhomogeneous hypointensity and hyperintensity. Correlating MR imaging appearances and pathological findings, the lobulated high signal intensity on T2-weighted images may be related to a large amount of myxoid matrix contained within the tumor interstitium. The multiple striplike, punctate, sheet, or irregular hypointense signal intensities on T1WI and T2WI are probably due to large intratumoral calcified cartilage nodules. The arc-shaped short-T2 signal on the peripheral rim of the lesion may be attributed to the thin-walled fiber capsule covering the surface of the mass.
On postcontrast T1-weighted images, the obvious heterogeneous, ringlike, and intratumoral honeycomb-like enhancement was another feature seen in our series, demonstrating the “punica granatum seeds” sign. To our knowledge, this characteristic enhancement pattern has not been previously described, and is inconsistent with the majority of case reports in the literature. We believe that the degree of enhancement of the tumor on gadolinium-enhanced T1-weighted images depends on a variety of factors, including the number of tumor cells, the tumor blood supply, and the proportion of the cartilage matrix that is calcified. Obvious heterogeneous enhancement may be related to vascular proliferation within the lesion.
It is clear that an accurate diagnosis of intracranial chondroma is important in order to create a therapeutic plan and to assess prognosis. However, a preoperative diagnosis of chondroma can be very difficult. The differential diagnosis of a primary intracranial lesion in the skull base region includes, but is not limited to, craniopharyngioma, chordoma, and myxoma. Patient age and biochemical markers can be useful in differentiating craniopharyngioma from chondroma. In addition, craniopharyngiomas usually demonstrate typical “eggshell” calcification on CT and rarely cause bone destruction of the sellar region. As clinical prognosis is more favorable in patients with chondroma than those with a chordoma, it is important to be able to differentiate between these tumors. Chordomas may originate from an embryonic notochord residue and may contain both chondrogenic and mucus components. Chordomas commonly occur in the midline, in particular in the clivus bone, with aggressive growth and extensive destruction of bone. While chondromas are usually located in the upper clivus and parasellar regions, with more marked enhancement than chordomas as they grow, mainly towards the brainstem and barely reaching the clivus bone, bone erosion tends to be relatively less mild. When a chordoma is located at the middle cranial fossa and the parasellar region with multiple calcifications, preoperative differentiation from chondroma radiologically may be difficult. A shorter duration of clinical symptoms may be more suggestive of a chordoma than a chondroma (30,31). Myxomas originating from embryonic mesoblast cells may also contain components such as chondrogenic cells and mucus degeneration, with a predilection for similar sites. Thus, preoperative differentiation of myxoma from chondroma may be difficult radiologically. However, myxomas reveal relatively homogeneous long T1-weighted and long T2-weighted signals and mild rim enhancement. When intracranial calcified tumors are located in other regions, such as the convexity or falx areas, meningiomas, chondro-sarcomas, oligodendrogliomas, glioblastoma multiforme, hemangioblastomas, vascular malformations, and fungal infections should be considered in the differential diagnosis. The imaging characteristics that can distinguish chondromas from meningiomas are usually the lack of intense and homogenous enhancement and the absence of a “dural tail” sign (6). Angiography is the best method for differentiating the two tumors, with meningiomas demonstrating obvious tumor staining, and absence of tumor staining in chondromas. Intracranial chondrosarcomas are more common in the elderly and are widely invasive. In addition, they usually enhance more significantly on postcontrast scans due to the rich blood supply. Besides, intracranial teratomas with cartilage, chondromyxoid fibromas, and chondroblastomas are rare tumors, but they also need to be excluded. Pathological and immunohistochemical examination is critical for the accurate diagnosis of these tumors (7).
In conclusion, intracranial chondromas are benign, slow-growing tumors that usually occur in young adults. Although rare, our series of six patients revealed that intracranial chondromas have characteristic CT and MR imaging features, such as a lobular sharply demarcated mass with calcification, accompanied by adjacent bony involvement, without peritumoral edema, and exhibiting delayed enhancement on postcontrast CT scan. Contrast-enhanced T1-weighted images displayed marked heterogeneous, ringlike and intratumoral honeycomb-like enhancement, representing the typical “punica granatum seeds” sign. If a young patient presents with a long duration of clinical symptoms associated with a space-occupying lesion at the cranial base, or at uncommon sites such as the falx, the convexity region and the brain parenchyma, and imaging reveals features similar to those described above, the presence of an intracranial chondroma should be considered.