
Abstract
Introduction
Mallet injury is a commonly treated hand injury in acute hospitals. While there is much literature regarding the various treatment options and outcomes, no studies were found that describe the management of this injury across a national health service. This study describes how mallet injury is managed within the acute hospital system in Ireland. An understanding of the current system of service provision is essential for future service development in this area.
Method
Emergency and occupational therapy departments in the 29 acute case-mix hospitals in Ireland were contacted by telephone and postal questionnaire with 47 respondents participating in the study. Descriptive statistics are used to present the results.
Results
Results indicate that accessing acute hospital-based services for the conservative management of mallet injury typically follows a predictable pathway, but can result in delays and disruption to treatment for the patient. There is little evidence of direct referral from the emergency department to the occupational therapist which, when compared with published literature, would represent the most efficient and optimum care pathway for the patient. The choice of splint used by both the emergency and occupational therapy departments differs, but treatment provided is in line with available evidence-based practice.
Conclusions
This preliminary study provides a basis for future service development in the acute management of mallet injury, by describing how treatment is currently provided nationally. Recommendations for further investigation have been made, and the need for audit and outcome measurement has been highlighted. The development of therapy-led services in Ireland is proposed, to improve efficiency and quality of service provision in the conservative management of mallet injury.
Introduction
One of the priorities outlined in the Irish HSE (Health Service Executive) national service plan 2011 is the implementation of the ‘emergency medicine clinical programme’. The HSE state that ‘the focus will be on standardizing care and implementing proven solutions to save lives, prevent complications, remove waiting lists and save money’ (p. 3). 1
Acute care, for the management of injuries such as mallet finger, is provided in Ireland through a network of acute case-mix hospitals, which falls within the remit of this clinical programme. At the time of this study, there were 29 such hospitals in Ireland, as categorized by the HSE. Patients access acute services by presenting to an emergency department in an acute hospital, where emergency care is provided. Ongoing management of the injury is then arranged by emergency department staff, who refer the patient to the most appropriate follow-up service.
Mallet finger and management
Mallet injury occurs when there is a disruption of the extensor tendon mechanism in the hand, at the level of the distal interphalangeal (DIP) joint caused by an extensor tendon rupture or an avulsion fracture. It is typically caused by a sudden flexion force to the actively extended fingertip but can also result from laceration, crush injury or forced hyperextension. 2 Reported mechanisms of injury are varied and include skiing, 3 rugby, 4 bed-making 5 and donning socks. 6 Following their Cochrane review, Handoll and Vaghela 7 recommended conservative treatment with splinting for the majority of patients with acute closed soft tissue or bony mallet finger injury. Geyman et al. (1998) 5 also concluded, from a pooled quantitative analysis, that initial conservative management should be widely adopted; a recommendation that has also been supported by clinical opinion. 8
Treatment contexts for this diagnosis have not been previously described. The literature indicates that mallet injury can be managed in the emergency department, 9 general practice, 10,11 consultant-led clinics 12 and therapy-led clinics. 13–15 In an Irish context, emergency departments are most likely to provide the first point of contact for many of these patients. While appropriate diagnosis and treatment in the emergency department is critical to the ultimate outcome, ‘closed tendon injuries of the hand are unfortunately often not treated with the same respect as other hand injuries’ (p. 76), 9 thereby adding to the risk of long-term disability or deformity. No studies have compared the effectiveness of treatment in the emergency department to treatment in another setting.
Two studies have reported treatment outcomes for mallet injury managed in hand therapist-led clinics in the UK. Richards et al. 14 prospectively examined 34 cases of mallet injury treated with a custom-made thermoplastic splint. All patients were referred directly from the emergency department to the hand therapist, were seen within one week and none required referral to the orthopaedic clinic. They reported a successful outcome in 88% of cases (i.e. less than 5° extension loss, no stiffness and full flexion). Katsoulis et al. 13 reported that 51% of 39 soft tissue mallet cases, and 73% of 15 bony mallet cases treated with a dorsal aluminium splint, achieved an excellent outcome (i.e. less than 10° extension loss, no pain and full flexion). Both studies provide evidence to support the management of mallet injuries by hand therapist-led clinics, indicating that a hand therapist can treat mallet injuries independently 14 and as effectively as a surgeon. 13 A group of 25 international hand therapy experts have also recommended that patients be treated by a hand therapist in the initial splinting phase of management. 8
This model of therapy-led service delivery has been widely reported in the UK in the treatment of other upper limb conditions, the experience of which could inform the development of management of mallet injury in Ireland. Reported benefits include a shortened patient pathway and timely detection of missed diagnoses in the case of wrist injuries; 16 greater patient turnover, increased patient satisfaction and improved continuity of care in the case of hand trauma; 17 and reduced waiting times and costs in the case of carpal tunnel syndrome. 18
The importance of early treatment of mallet injury has been advocated in the past, 6,19 but as there is no clear definition of what constitutes delayed presentation, comparison of outcomes of early versus delayed conservative management is difficult. Brzezienski and Schneider 20 state that ‘the period of time after injury that this non-operative treatment can be delayed and still be effective is being extended and the absolute outside time limit is not known’ (p. 385). 20
Abouna and Brown 19 and Lester et al. 12 report less favourable outcomes in cases of delayed presentation, defined as greater than four weeks and greater than two months respectively. But the literature also provides evidence of favourable outcomes with splinting in cases of delayed presentation. Outcomes for 10 patients with chronic (>4 weeks) mallet injury were reported by Patel et al., 21 where nine patients achieved positive outcomes (i.e. less than 10° extension lag, full flexion, no pain). Garberman et al. 22 compared outcomes for what they described as early (<2 weeks) and delayed (>4 weeks) treatment groups, with statistical analysis indicating no difference in outcomes. Similar conclusions were drawn in several other studies; 23–25 however, unclear reporting of results was noted in the latter two studies.
A review of the literature reveals widespread use of the Stack splint 26 as a treatment option for mallet injury. However, many problems with its use have also been reported, including skin maceration, 13,15,27 difficulty achieving adequate fit 15,28 and issues regarding oedema. 11 Reported treatment failure rates associated with use of the Stack splint range from 23.8% to 48%. 15,27–29 An earlier retrospective review of 151 injuries treated with the Stack splint suggested that poor technique in splint application may be responsible for some complications, and presented guidelines for its correct application and management. 30
Many studies 15,27–29 have compared the Stack splint to other splint designs including a custom-made perforated splint, 27 a padded aluminium splint 28 and the Abouna splint. 29 All concluded that the outcomes were similar with both splints, but reported some advantages of the alternative splints regarding comfort and fit. A Cochrane review, which included the latter three studies concluded that due to methodological flaws and poor outcome reporting, there was insufficient evidence to recommend any of these splints above another. 7
Various other methods of splint immobilization have been reported including elastic bandage splints, 31 custom-made thermoplastic splints, 32,33 tape splints 34 and plaster casting, 2,35 the latter described only in situations where both the proximal and the DIP joints were immobilized. In a blinded, prospective, randomized clinical trial involving 87 participants, Pike et al. 32 compared volar aluminium, dorsal aluminium and custom-made thermoplastic splints and found no significant difference in their effectiveness. They reported a trend suggesting superiority of the custom-made thermoplastic splint; however, this finding must be considered with caution, due to lack of statistical significance. A recent prospective randomized controlled trial demonstrated that a custom thermoplastic splint was significantly less likely to result in treatment failure when compared with a Stack splint and dorsal aluminium splint. 15 There is also evidence that clinical opinion supports custom splinting with international experts recommending that ‘an accurately fitted custom-made splint is preferable to a factory-made splint’ (p. 2). 8
There is not enough evidence to inform the best way to treat mallet finger injuries, 8 including the required period of immobilization and the subsequent period of night splinting, if recommended at all. Eight weeks of immobilization, followed by two weeks of night splinting was recommended in a treatment algorithm for mallet finger. 36 Geyman et al. 5 conducted a pooled quantitative literature analysis, and concluded that six to eight weeks of immobilization followed by two weeks of night splinting should be employed. In a UK study, Pratt 37 critically reviewed the literature to examine if eight weeks of immobilization was sufficient, and found the evidence to be inconclusive. In a review of treatment options for mallet finger, six weeks of immobilization was the most commonly reported period, based on tendon healing timelines. 38 Pike et al. 32 treated 87 Canadian patients with six weeks of splinting. Follow-up night splinting was only employed if there was more than 20° extension lag or if the patient deemed the lag unacceptable, which occurred in nine cases. They noted that extension at the DIP joint disimproved between week seven and week 12, and therefore concluded that six weeks of splinting may be insufficient. Cadaveric studies support the theory that only the DIP joint requires immobilization, 39 with inclusion of the proximal interphalangeal (PIP) joint recommended where a risk of swan-neck deformity exists. 33
Examination of, and reflection on, current practice is an essential part of implementing future service development as prioritized by the HSE. In the case of mallet injury, no studies were found which examine or even describe the current system of service delivery. The aim of this study was to describe how mallet injury is currently treated in Ireland and to review this in light of international literature.
Methods
This study utilized purposive sampling with all 29 acute hospitals in Ireland (as categorized by the HSE ‘Healthstat’ system) being contacted, thus ensuring national representation.
For inclusion in this study, hospitals were required to have an emergency department and/or occupational therapy department that treated mallet injuries. Telephone contact was made to confirm this. Verbal communication also confirmed that physiotherapists were not routinely involved in provision of splints for mallet injury, with just one hospital reporting that the physiotherapist may be involved in this process.
Twenty-eight of these settings had an emergency department that managed mallet injuries. Twenty-six had an occupational therapy department; 19 of which treated mallet injuries. These 47 departments made up the study sample.
Ethical approval was obtained from the Research Ethics Committee of the Adelaide, Meath & National Children's Hospital and St James’ Hospital, Dublin. Consent from participants was assumed by voluntary return of the questionnaires.
Data collection
Two questionnaires were designed for the purpose of this study, one for each of the responding departments. They captured primarily quantitative data with some open-ended questions included. They were piloted by two clinical specialist occupational therapists and an advanced nurse practitioner.
The questionnaires were distributed by post and included a stamped-addressed envelope and a cover letter outlining the purpose of the study. A reminder letter was sent after the response date had passed.
In the case of the 28 emergency departments only one questionnaire was sent, where one representative was asked to answer on behalf of that department. This method was chosen because in all cases, a varied number of disciplines provided treatment within the same setting.
Within the 19 occupational therapy departments, all of the therapists treating mallet injury were given the opportunity to respond regarding intervention in their particular treatment area, for example, orthopaedics or plastics. This method was chosen to ensure that differences in patterns of patient presentation across treatment areas were examined. Therefore, multiple questionnaires were sent through a contact person for dissemination.
As this was a descriptive study, data gained from the questionnaires were organized and analysed using Microsoft Office Excel (2007), and descriptive statistics were used to present the data.
Results
Twenty-eight emergency departments were contacted and 16 questionnaires were returned, giving a response rate of 57%. Fourteen of the 19 occupational therapy departments contacted, responded with 24 individual questionnaires, giving a department response rate of 74%.
Emergency department respondents
The majority (63%; n = 10) of emergency department questionnaires were completed by an advanced nurse practitioner. Two respondents (12.5%) reported that they had an occupational therapy service in their emergency department that would accept referrals for mallet injury. In all other cases, respondents reported that multiple staff members were routinely responsible for the provision of splints. This included consultants, non-consultant doctors and nurses. No respondent reported that physiotherapists were involved at this stage. This indicates that splints for mallet injury were, in most cases, provided as part of the generic emergency department treatment by multiple professionals.
Occupational therapy respondents
The majority of respondents (75%; n = 18) were senior occupational therapists. The number of years working in hand therapy ranged from six months to 18 years, with a mean of 6.7 years experience. Forty-six percent (n = 11) of respondents had practised hand therapy in more than one setting.
Referrals
Number of new referrals received per week
Of the 16 emergency department respondents, all reported that patients with mallet injury typically presented to them, less than one week post-injury. In 94% (n = 15) of cases, typical management on the day of presentation was described as ‘provision of a splint or cast’.
Occupational therapy respondents described the source of their referrals and the frequency with which they were received. Figure 1 indicates that referrals were most frequently received from the orthopaedic clinic. As referrals were rarely received from inpatient wards and ‘other’ sources, these were excluded from further analysis in this study.
Source and frequency of referrals to occupational therapy for the management of mallet injury (n = 24)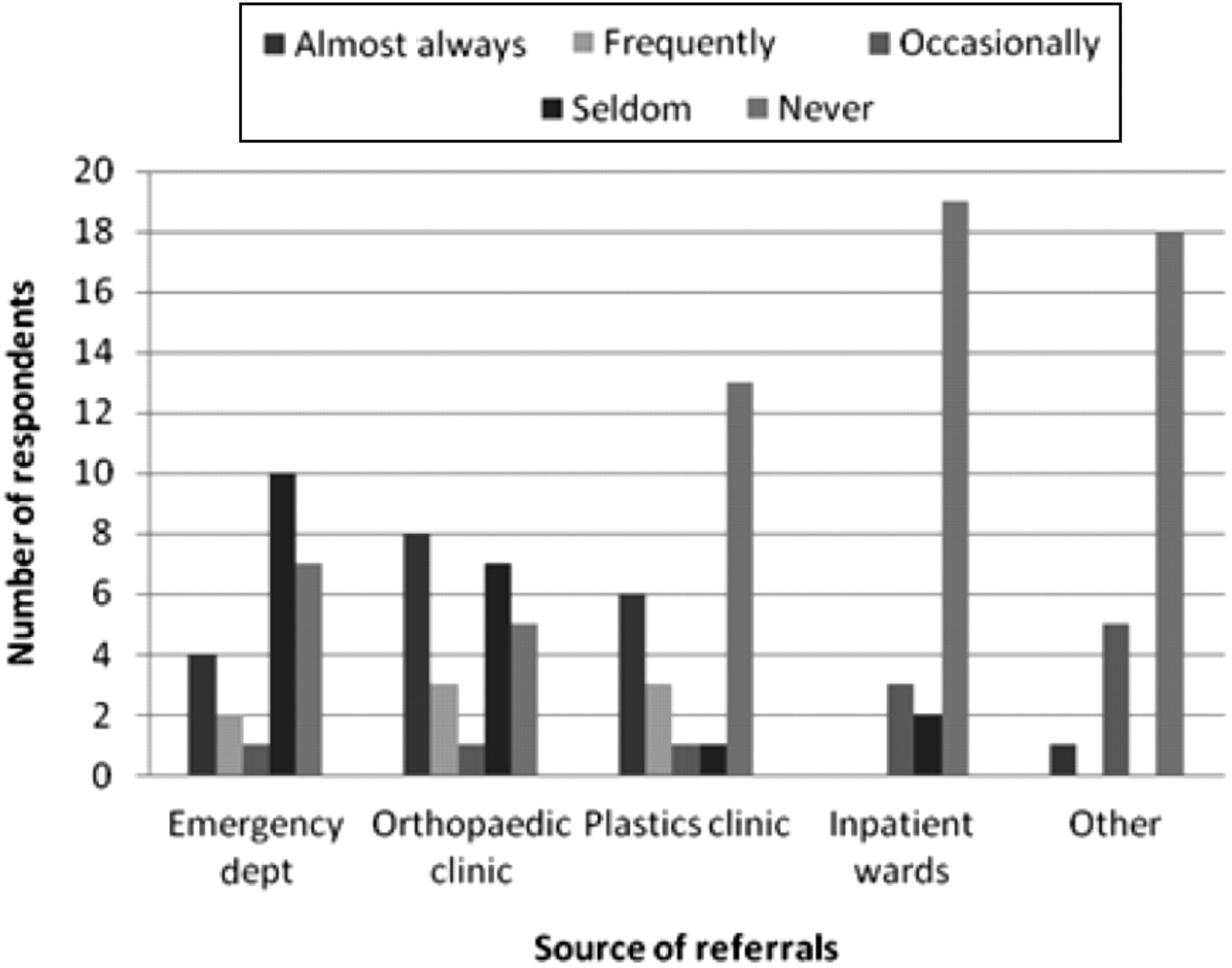
Frequency of ‘early’ and ‘delayed’ presentation of patients with mallet injury to occupational therapy
ED, emergency department; OPD, outpatient department
Mobility status of affected digit on presentation to occupational therapy
ED, emergency department; OPD, outpatient department
In cases where patients presented to occupational therapy with a splint in place, respondents described the type of splint, with some giving multiple responses. The splint was most frequently a Stack splint (59%; n = 20), followed by an aluminium/foam splint in 35% of cases (n = 12).
Initial management
Respondents were asked to describe the type of splint(s) they provided for mallet injury, and whether they were provided ‘almost always’, ‘frequently’, ‘occasionally’, ‘seldom’ or ‘never’. The responses of ‘almost always’ and ‘frequently’ are presented in Figure 2, which reflects the most frequently provided splints by both departments.
Splint type which is ‘almost always’ provided (i.e. 75–100% of the time) by both emergency and occupational therapy departments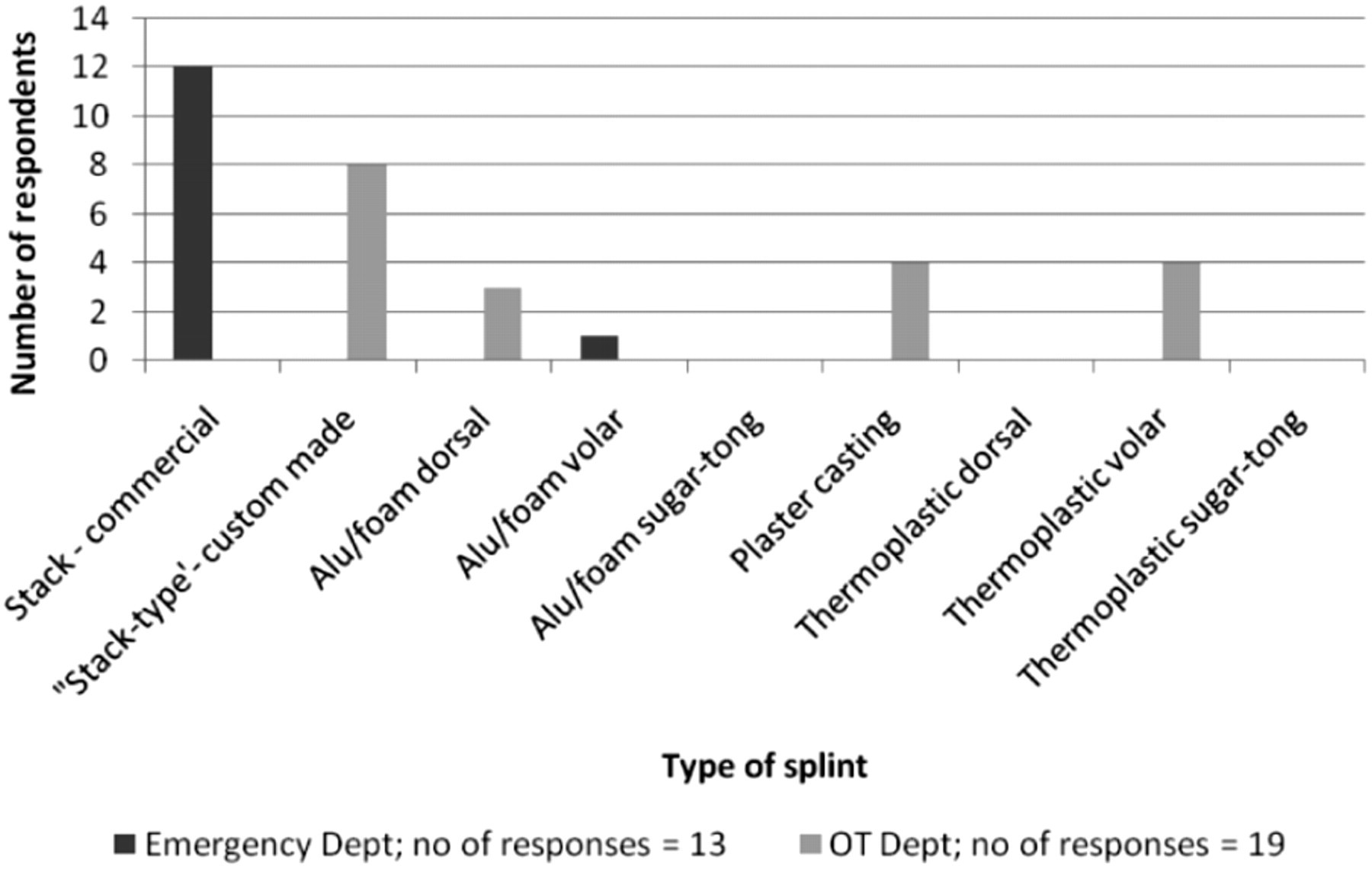
To further clarify the type of splint provided, respondents were asked to outline which joints were included and thus immobilized in the splint used. Fourteen of the 16 emergency department respondents (88%) indicated that they include only the DIP joint, while two (12%) also immobilize the PIP joint. Twenty of the 24 occupational therapy department respondents (83%) indicated that they include only the DIP joint, with three (13%) indicating they include the PIP joint only if a swan-neck deformity is noted.
Reasons why an alternative to the practitioners ‘first choice’ of splint would be considered
OT, occupational therapy
Ongoing management
This section describes what happened for a patient following their initial intervention. The 16 emergency department respondents described the process following their initial intervention with 20 responses received. The majority of responses (n = 13) indicated that patients were referred to an orthopaedic clinic. One respondent indicated that patients were referred directly to occupational therapy, while no respondent reported referral to physiotherapy. Only two respondents reported that they (i.e. the emergency department staff) provided ongoing management to the point of discharge. The ongoing management of these injuries was not further analysed, as the sample of two departments was deemed insufficent.
All of the occupational therapy respondents reported that they provided ongoing management of mallet injury within their department. The period of 24 hour immobilization reported, ranged from four to eight weeks, with the majority of respondents (48%; n = 11) reporting six weeks of immobilization (Figure 3). This was followed by a period of night splinting in 92% of cases (n = 22) (Figure 4). One respondent failed to answer both questions.
Period of 24-hour immobilization (number of respondents = 23) Period of subsequent night splinting (number of respondents = 23)

Treatment outcomes
Respondents were asked if their organizations had a written treatment protocol to guide the management of mallet injury. Thirteen (81%) of the emergency department respondents, and 20 (83%) of the occupational therapy respondents confirmed that their organization had such a protocol.
Respondents were subsequently asked if their department's routinely audited treatment outcomes. Both emergency departments providing ongoing management, and 22 (92%) of the occupational therapy respondents reported that they did not audit outcomes.
Discussion
This study describes the system patients encounter when they access acute hospital-based services for the treatment of mallet injury in Ireland. The results indicate that it typically follows a predictable pathway, but can result in treatment access delays and disruption for the patient.
The first point of contact for patients within the acute hospital system is the emergency department. After this initial contact, two emergency department respondents reported that they provided follow-up treatment, through to discharge for this condition. The majority of respondents indicated that patients were referred to an orthopaedic outpatient clinic. Only one emergency department respondent reported that mallet injury patients were referred directly to occupational therapy for treatment.
Management of this injury by a hand therapist is advocated, and it is suggested that after the initial diagnosis is confirmed, patients do not require management by a consultant or specialist registrar. 13,15 Richards et al. 14 compared outcomes for mallet injury from their therapy-led clinic to previous studies, and concluded that a purpose-made splint applied and monitored by a specialist hand therapist may be the preferable approach to treatment. As described above, this current study found little evidence to indicate that patients in this system have early access to occupational therapy, where specialist hand therapy input could be provided, as the majority of patients were sent directly from the emergency department to a consultant-led service.
Occupational therapists receive their referrals from other disciplines (e.g. doctors), and results of this study indicate that the orthopaedic clinic was the largest referral source for occupational therapy. This correlates with responses from emergency department staff who indicated that most patients are referred, by them, to an orthopaedic clinic. Therefore, a consultant-led clinic acts as a ‘gate-keeper’ to occupational therapy/hand therapy access. A model of service delivery that allows direct access from the emergency department to hand therapy services after initial diagnosis, would eradicate the need for this unnecessary middle step in the process of service delivery. This would also serve to free up appointment slots at consultant-led clinics for more complex patients who require consultant or specialist registrar input, thereby reducing waiting times and costs incurred by the organization. 13,18
Delay and disruption in treatment
This study indicates that delayed presentation of patients to occupational therapy was most likely when referrals were received from the orthopaedic clinic, which suggests that the most typical referral route to occupational therapy was potentially also the slowest. As patients sometimes presented to occupational therapy at this point with no splint in place (Table 3), it is evident that in some cases a splint had either not been provided in the emergency department, or the patient had discontinued use of the splint that had been provided. Therefore, conservative treatment would have been commenced or re-commenced at this point.
Both of these scenarios indicate a disruption or delay in treatment. While delayed treatment for mallet finger is generally not associated with a significantly poorer outcome, 21,22 no studies have been found that examine the wider effects of delayed presentation. For example, the effect on the patient's subjective experience of their care or the impact of treatment duplication and delayed treatment access on the resources of the organization.
Again, development of therapy-led services would allow patients to gain more timely access to specialist hand therapy services, thereby promoting a system of service delivery where the patient receives the most appropriate care at the most appropriate time.
Splint choice
In a Cochrane review, Handoll and Vaghela 7 found no conclusive evidence to support the use of one splint over another and there is, therefore, no support for or against the different splint choices of the respondents in this study. Similarly, Pike et al. 32 (when comparing a commercial splint to a custom thermoplastic splint) and O'Brien and Bailey 15 (when comparing a dorsal aluminium and custom thermoplastic splint to a Stack splint) found no statistically significant difference in outcomes. However, O'Brien and Bailey 15 support the use of a custom thermoplastic splint as it is significantly less likely to result in treatment failure.
The commercial Stack splint is the most frequently supplied splint by the emergency departments in this study and custom-made splints are not typically supplied. Results showed that a wide variety of staff provided these ‘off the shelf’ splints in the emergency department, indicating that this was considered a generic skill for emergency department staff. In contrast the occupational therapy respondents most frequently supplied a custom-made ‘Stack-type’ splint, followed by other custom-moulded designs. This indicates that they offered a wider variety of treatment options, which is reflective of the hand therapy experience of the occupational therapy respondents. The benefits of therapy-led management of hand injuries requiring splinting is highlighted by Burke et al., 40 in their report on management of carpal tunnel syndrome in primary care. They state that for optimal effect, ‘splints should be chosen by experienced hand therapists from a range of available options, with the opportunity for a further visit to audit outcome and allow for additional adjustments’ (p. 434).
With the exception of the patients who were followed up in the emergency department (2 out of 16 respondents), this study suggests that patients were highly likely to have their splint changed from a commercial Stack splint to a type of custom-made splint at their first occupational therapy appointment. Katsoulis et al. 13 reported that in their therapy-led clinic, patients are changed from a Stack splint (as supplied by the emergency department) to a padded aluminium splint to minimize skin complications. This may be a possible reason for the splint change seen in this study also. The time and cost implications of this duplication of treatment warrants further examination to ensure maximum efficiency in provision of care, with the effect on the patient experience also considered.
It is noteworthy that in this study, plaster of paris (POP) casting is one of the most frequently used splints by occupational therapists (Figure 2). References in the literature to management of mallet injury with POP, all refer to its use, only in cases where both of the interphalangeal joints are included. 2,6,12,35 Five of the six respondents in this study who report its use ‘almost always’ or ‘frequently’, report that they splint only the DIP joint. Further examination of the use of POP casting by Irish occupational therapists would provide an interesting opportunity for sharing of clinical experience, as no studies reporting DIP joint inclusion only, in POP casting for mallet finger were found.
To further investigate splint choice, an open-ended question was used to gather information on why a practitioner would deviate from their ‘first choice’ of splint (Table 4). The emergency department responses reflect a particular emphasis on resource considerations, such as availability of stock, indicating that this may be a priority for them. The occupational therapy responses include more patient-related considerations such as activities of daily living and digit shape, which is reflective of the occupational therapy core skills of activity analysis and splinting. A qualitative study to investigate clinical reasoning in splint choice would be beneficial to explore this issue.
Treatment protocol
This study found a variation in the duration of splinting from four to eight weeks, with the majority of respondents reporting a six-week splinting period. There was a wide variation in the period of follow-up night splinting reported, ranging from none to over four weeks. These timelines are consistent with that reported by Pratt 37 and Smit et al. 38 Cadaveric studies have confirmed that the PIP joint does not require immobilization 39 and this is reflected in the fact most respondents reported inclusion of the DIP joint only.
Irish evidence base
In contrast to the quantity of international literature, no Irish studies reporting treatment outcomes have been found. This paucity of information is reflected in this study, which found that only two respondents reported that their departments routinely audited outcomes of treatment for mallet injury. The routine collection of basic audit information is imperative for the efficient and evidence-based development of future services. Routine recording of the information gathered in this study is recommended (i.e. referral source, time elapsed since injury at time of presentation, splint(s) provided and treatment protocol followed, including the period of immobilization). In addition, recording of the subjective and objective outcome of treatment is essential to provide a basis on which we can recommend a management approach to improve the efficiency and quality of service provision in the management of mallet injury. The platform to allow this audit information to be gathered, has been shown to exist, as this injury is commonly seen across the acute hospital system with the majority (97%; n = 28) of the 29 acute hospitals reporting that they treated mallet injury. Also, a high proportion of respondents (over 80%) reported that their organization had a written protocol for the management of mallet injury, which offers a useful opportunity for sharing of information within, and across organizations.
Limitations
Although piloted, the use of an original questionnaire means that the measurement tool used was not validated. As multiple occupational therapists from each organization could respond, there may have been over-representation of a particular organization's treatment protocol, when multiple responses from one setting were received. The outcomes of this study are based on respondents’ description of their service and would ideally be supplemented with a national audit of these services to verify the accuracy of the respondents’ reports. Finally, the researcher, being an occupational therapist, brings more understanding of the management of mallet injury by hand therapy services, when compared with management in the emergency department. The pilot phase of the study aimed to address this possible bias, as did the initial telephone contact where emergency department respondents had the opportunity to describe their service to the researcher.
Conclusion
This study aimed to describe the management of mallet injury within Irish acute hospitals nationally. The information gained in this study will allow reflection on current management of mallet injury and will assist in future service development. This development should be in line with the priorities of HSE who state that ‘the focus will be on standardizing care and implementing proven solutions to save lives, prevent complications, remove waiting lists and save money’ (p. 3). 1 Many authors to date 13,14,16–18 have provided evidence of service delivery initiatives, which have indeed achieved these improvements sought by the HSE, and provide a template that is transferrable to the Irish health-care system. The widespread establishment of a model of service delivery, which facilitates direct referral from the emergency department to the occupational therapist would reduce delays and disruption in treatment access and provide the patient with the appropriate care at the appropriate time. The demand for appointments in consultant-led clinics would also be reduced, assisting with reduction in waiting lists and costs. This study highlights the potential that exists for improved efficiency and quality of service provision in the management of mallet injury in Irish acute hospitals.
Footnotes
Acknowledgements
Thanks to Simone Derham (BscOT; PgDipHT), Clinical Specialist Occupational Therapist, for clinical advice and guidance throughout the process of this research. A bursary of €200 was received from Irish Association of Hand Therapists.