
Abstract
Introduction
Gliding without adhesion is imperative to regain full range of motion after flexor tendon repair. The purpose of this study was to find assessment tools that represent these outcomes and to explore their relationship with hand function.
Methods
Ninety-six flexor tendon injuries in 24 patients were assessed at 12 weeks after flexor tendon repair. Total active motion (TAM) and total passive motion (TPM) were recorded with a goniometer. For patient-reported upper extremity function, the Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire was used.
Results
A moderate negative correlation was found between total active motion and DASH score (r = −0.3809 to −0.5815, P < 0.0001). While TAM and TPM improved over the 12-week period, mean values did not reach those of the uninjured hand. Mean DASH scores improved from 46.05 points at four weeks to 23.5 points at 12 weeks.
Conclusion
Despite early flexor tendon rehabilitation in this sample, after 12 weeks, some degree of dysfunction and loss of active ability for finger flexion still persisted. The DASH appears to be an appropriate outcome tool after flexor tendon repair. The combination of patient-reported questionnaire and measures of impairment such as TAM and TMP give a more comprehensive picture of functional outcome.
Introduction
Tendon injuries are among the most severe injuries of the upper extremity. These lesions occur almost exclusively in young workers and usually result in disability. The tendon injury typically requires 3–4 months of rehabilitation before return to work. Failure to repair or poor residual function after surgery can reach 20–30% of cases. 1
Assessment instruments and accurate rehabilitation techniques allow surgeons and therapists to identify dysfunctions, analysing the development of a treatment and also providing communication among professionals. 2,3 Hand therapy is still a young adjunct to surgical repair. So, many technical details of the therapeutic intervention have yet to be determined. 4 Therefore, rehabilitation regimens through immobilization or active/passive early motion exercises after tendon repair are chosen mainly by the preferences and observations of surgeons and therapists, according to the suture technique applied, the patient's ability to actively participate in the rehabilitation process and the therapist's experience. 5,6
Kleinert et al. 7 and Duran et al. 8 were pioneers in this field and many modifications of their protocols have been presented and used in different rehabilitation units.
Outcome measurement needs to be accurate but also inexpensive and requires assessment tools that are easy to use. 9 Outcome assessment of flexor tendon repair must capture the integrity of the flexor tendon. However, an isolated measurement of the finger joints is probably not enough to analyse dysfunction. The total flexion of the finger, subtracted from any lack of extension, needs to be measured. There are many methods for evaluating outcome after flexor tendon repair 10 of which total active motion (TAM) and total passive motion (TPM) have been standardized by the American Society for Surgery of the Hand (ASSH). Any differences between TAM and TPM can be used to identify tendon adhesion. 2,11
Strickland and Glogovac's qualitative criteria are a well described method that shows by percentage the finger flexion capability after tendon repair. They include only interphalangeal joints in the analysis and thus focus on zones I and II only. The ASSH criteria for TAM and TPM incorporate metacarpophalangeal joint for most complex lesions involving tendon and nerves in zones IV and V, where impairment of intrinsic muscles is included. 10
Hand therapy for flexor tendon injury is primarily focused on physical impairment. However outcomes should not be focused solely on measures of impairment such as motion but the additional use of measures of activity and participation is advocated. 12 Evidence-based health care demands the integration of best available research with professional skill experience and patient preferences. 13,14
The use of region-specific measures of activity and participation allows therapists and surgeons to capture the patients' perspective of the consequences of traumatic hand injury but also enables comparisons between outcomes from different groups of patients and diagnoses. 15,16
The Disabilities of the Arm, Shoulder and Hand (DASH) questionnaire is one of the most widely used instruments for assessing functional capability and physical symptoms in upper extremity dysfunctions. 17 It is one of the most translated and validated instruments cited in literature. 18–22
The combined use of objective clinical evaluation and self-reported scales in hand therapy practice ensures that rehabilitation focuses on individual needs. 23
The objective of this study was to explore the correlation between active range of motion and self-reported disability and function in patients treated through early mobilization after flexor tendon repair.
Methods
A consecutive sample of adult patients, referred to early rehabilitation, were diagnosed with traumatic flexor tendon injury in any Verdan's flexor tendon zone and submitted to primary tendon repair in a tertiary hospital with a modified Kessler suture. All patients were treated with an early passive mobilization protocol at a hand therapy unit of the public rehabilitation centre. Patients with associated lesions such as peripheral nerves and vessels were included. Those with fractures or other major trauma were excluded. All patients were recruited between 2010 and 2011.
The study was approved by the Clinical Hospital Ethical Committee of the University of São Paulo and all participants provided written informed consent.
Procedure
Early passive motion based on modified Duran protocol was initiated at the third postoperative day using a dorsal blocking Plaster of Paris orthosis (slab). Its position was approximately 20° of wrist flexion, 40–50° of flexion at the metacarpophalangeal and the fingers were bandaged with interphalangeal joints in extension when not exercising. 24 Patients performed isolated and combined passive flexion and extension and active associated extension exercises 10 repetitions, three times a day. At the intermediate stage (3–4 weeks postoperatively), after orthosis removal, protective active exercises were performed, initially using tenodesis effect, blocked active exercises and tendon gliding exercises. The exercise programme was progressively upgraded in the late phase (7–8 weeks postoperatively). In cases with poor tendon glide and adhesion presence, therapeutic ultrasound, stretching and strengthening exercises were incorporated, as well as serial casting when needed, based on the algorithm proposed by Sacoka et al. 25,26
Outcome measures
Demographic data on patients' gender, hand dominance, occupation, employment status, side of injury, flexor zone and associated lesions were recorded.
All goniometric measures were performed at three timepoints: at cast removal (3–4 weeks), at eight and 12 weeks after repair. A standard North Coast Medical goniometer™ (MN, São Paulo, Brazil) was used to assess active and passive range of motion, always by the same therapist. For analysis of TAM the standardized formula described by ASSH was used. 2,26 TAM is calculated as the sum of active motion of metacarpophalangeal, proximal and distal interphalangeal joints, subtracted by any extension deficit of the same joints.
In order to represent active range of motion in percentage, these values were divided by 260 and multiplied by 100. The same principle was applied for TPM calculation. The results were classified as excellent (100%), good (75–99%), regular (50–74%) and poor (<50%). 2,5
The DASH questionnaire was given to patients to complete at four weeks and 12 weeks postoperative and any complications were documented if present.
Correlation between DASH and TAM was calculated as Pearson co-efficient using SAS® 9.1/PROC CORR. P < 0.05 was accepted as significant.
Results
The patient sample was composed of 24 patients (16 women and 8 men) with a mean age of 25.8 years and different occupations (student, manicurist, mason, welder, among others). Twenty were right-handed and four were left-handed. Sixteen patients had injured their dominant hand. Zone V was affected in 20 cases (all associated with nerve injuries), three were in zone II and one in zone III.
Table 1 presents TAM results of all 96 included in the study, classified through the functional index of ASSH.
TAM results according to the American Society for Surgery of the Hand classification (ASSH)
TAM, total active motion; ROM, range of motion
Figures 1 and 2 show the progression of TAM and TPM in uninjured and injured hands at four, eight and 12 weeks after repair. Comparing DASH in the fourth and 12th week postoperative, a decrease of disability was observed. The mean values were respectively 46.05 points at four weeks and 23.50 points at 12 weeks.
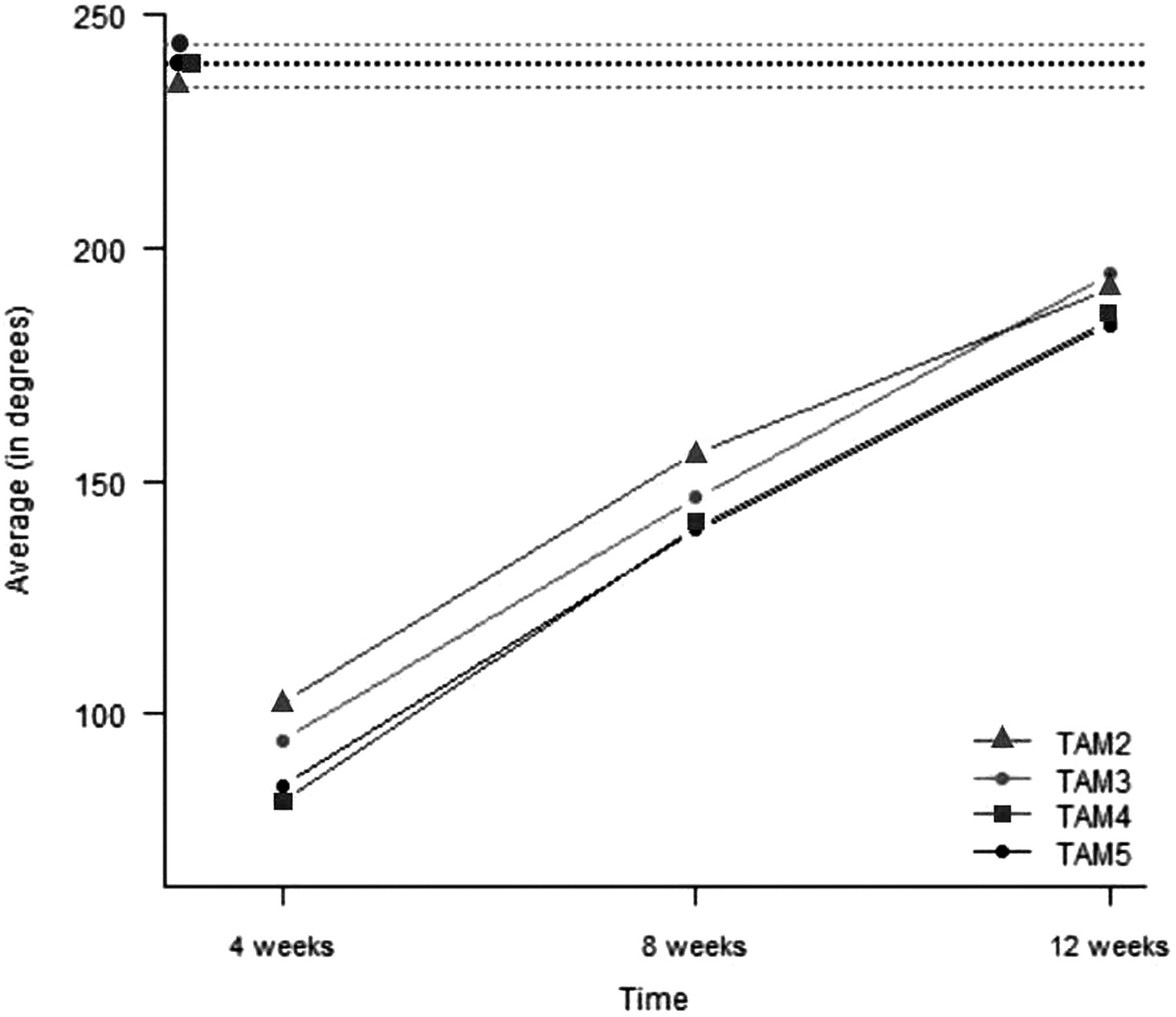
Linegraph of mean total active motion change over time
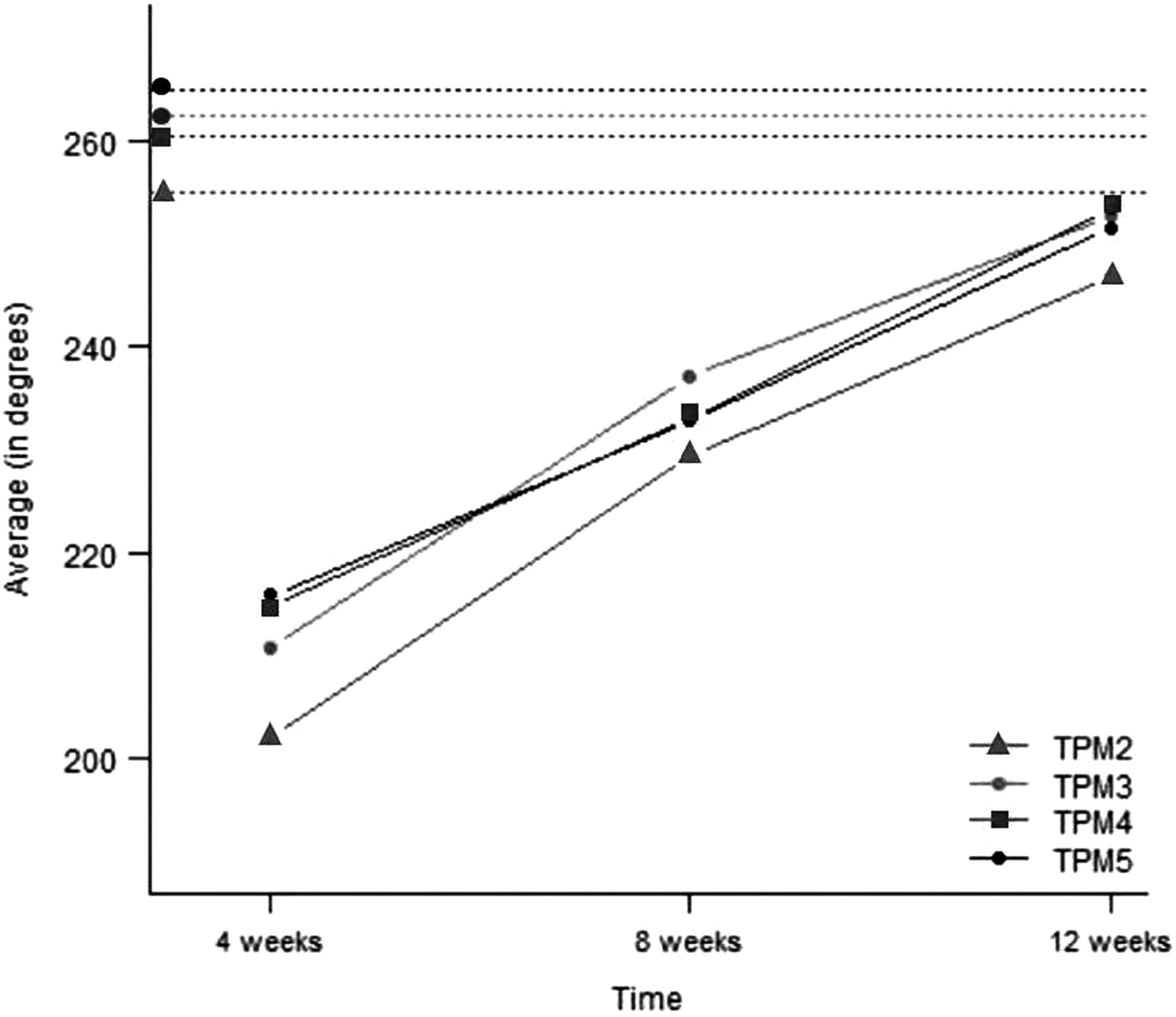
Linegraph of mean total passive motion change over time
There was a moderate correlation between TAM and DASH in each of the four digits ranging from (r = −0.3809 to −0.5815) (Figures 3–6).

Scattergraph of DASH and TAM2 – digit II. DASH, Disabilities of the Arm, Shoulder and Hand; TAM, total active motion
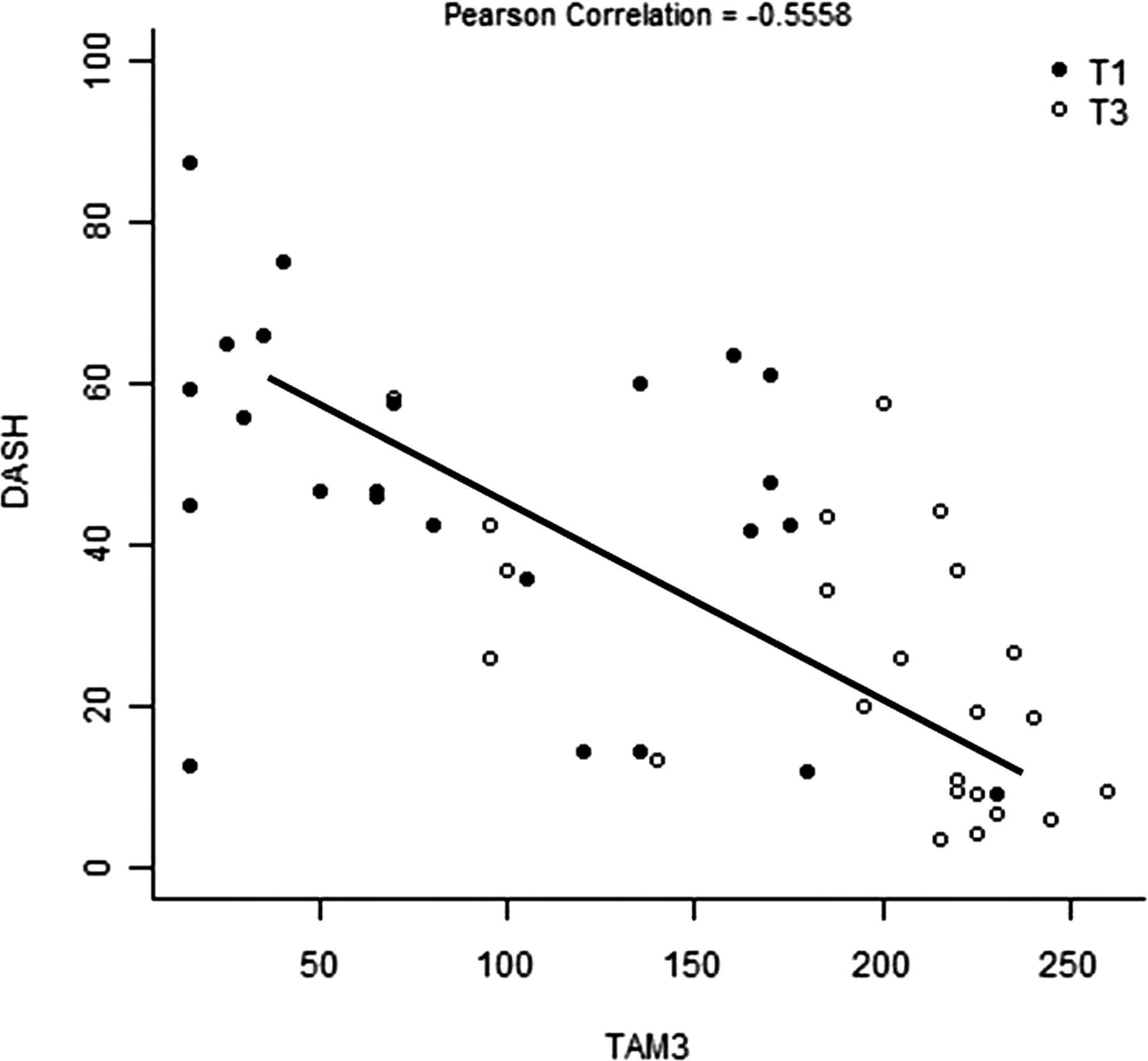
Scattergraph of DASH and TAM3 – digit III. DASH, Disabilities of the Arm, Shoulder and Hand; TAM, total active motion
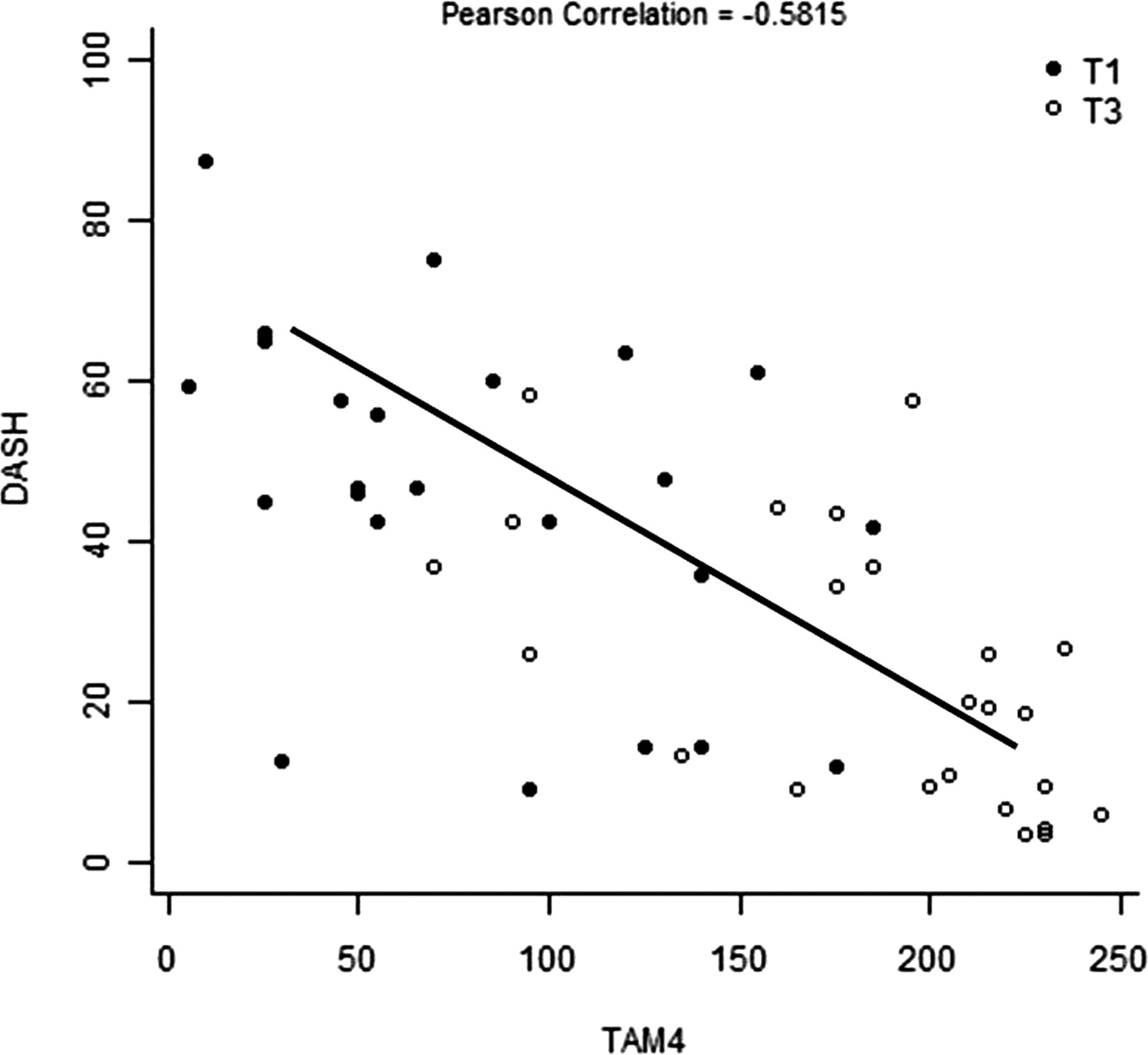
Scattergraph of DASH and TAM4 – digit IV. DASH, Disabilities of the Arm, Shoulder and Hand; TAM, total active motion

Scattergraph of DASH and TAM5 – digit V. DASH, Disabilities of the Arm, Shoulder and Hand; TAM, total active motion
Discussion
This study showed, as expected, that TAM and TPM scores of all fingers improved over time. However, some degree of active flexion dysfunction was still present at 12 weeks postoperatively. Many reasons may account for this including extrinsic and intrinsic muscle weakness, associated nerve lesions or tendon adhesion and early follow up. Considering that our sample was composed with 83.3% of zone V lesions at 12 to 14 weeks, this postoperative period is described as late phase, when unrestricted use of the hand would be allowed, in accordance with the literature. 24,27,28
Several studies have shown that DASH is a valid and reliable tool for upper limb musculokeletal disorders. 29,30 This questionnaire captures information about daily living activities, pain and function. The total score represents how much dysfunction is present in patients after treatment and a minimal detectable change was determined to be at least 12.7 points. 31 Even though we analysed a small sample (96 fingers), our findings are consistent with results reported by Bal et al. 32 They compared grip strength percentage and total active motion recovery with Quick DASH scores and found their results moderately correlated (r = −0.435; r = −0.541), similar to our results (r = −0.3809 – to −0.5815).
The limitations of our study are related to the short outcome time. Studies that analyse long-term outcomes may demonstrate greater improvement for flexor tendon repair. Rehabilitation aimed at preventing adhesions and maximizing function continues to be a challenge for therapists, despite refinement of surgical repair methods.
Conclusion
Despite early flexor tendon rehabilitation, in this patient group, after 12 weeks, some degree of dysfunction and loss of active ability for finger flexion still persisted. Our results suggest that the outcome from flexor tendon repair should not be based solely on range of motion but combined with a patient-reported instrument for a more comprehensive analysis, in a clinic setting. The therapist should use both instruments to ensure a more comprehensive assessment, focusing both on the patient's perception of his functional capacity and the recording of changes in the range of motion. Further long-term follow-up is required to confirm the correlation between self-report and total active motion.
Footnotes
Acknowledgements
This project was supported by São Paulo Research Foundation/grant 2008/00881-9 (Fundação de Amparo à Pesquisa do Estado de São Paulo – FAPESP), Brazil.