
Abstract
Introduction
Patient-rated outcome measures (PROMs) to measure upper limb activity and participation exist but there is little evidence to support their responsiveness in Dupuytren's surgery.
Methods
A literature review was conducted to evaluate the relative responsiveness of PROMs used in patients treated surgically for Dupuytren's contracture. A prospective observational pilot study was performed to test feasibility and clarify procedures in advance of a larger study to compare the relative responsiveness of different PROMs. The Quick Disabilities of the Arm, Shoulder and Hand (QuickDASH), the Patient Outcomes of Surgery-Hand/Arm (POS-Hand/Arm) and the Patient Evaluation Measure (PEM) were administered to eight patients before and 12 weeks after a fasciectomy.
Results
The literature review identified seven studies using PROMs before and after surgery for a Dupuytren's contracture. The PROMs were the Michigan Hand Questionnaire (MHQ), the DASH and the QuickDASH. All three had moderate-to-large effect sizes and standardized response means with the MHQ showing higher responsiveness than the DASH. In the pilot study the PEM demonstrated a higher responsiveness than the POS-Hand/Arm followed by the QuickDASH. No evidence was found to support responsiveness in terms of what is clinically relevant in relation to a patient-rated external criterion.
Discussion
The literature review and pilot study findings justify the need and feasibility to conduct a larger study to investigate the relative responsiveness of PROMs in patients undergoing Dupuytren's surgery.
Introduction
The International Classification of Functioning (ICF), Disability and Health requires that health outcomes include a measure of activity and participation ideally from the patient's perspective. 1 In addition, the UK National Health Service considers outcome measurement from the patient's perspective a major indicator of the quality of health care and is essential in guiding service provision. 2 This guidance has encouraged the development of global, region-specific and disease-specific patient-rated outcome measures (PROMs) now used widely in clinical research and practice. 3 However, in order for a PROM to provide useful information it must be reliable, valid and responsive. Each of these psychometric properties is specific to the population and setting in which it has been evaluated and efforts to determine these properties in different situations are ongoing. 4
This paper examines the responsiveness of region-specific upper limb PROMs with patients undergoing surgery for Dupuytren's contracture. Dupuytren's disease is a fibroproliferative disorder of the hand resulting in the affected digit(s) becoming fixed into the palm. 5 Interventions such as needle aponeurectomy, fasciectomy, dermofasciectomy and collagenase are available but research is ongoing to determine which treatment is most effective. 6 Several upper limb and hand specific PROMs have been used in this research but their responsiveness to intervention for Dupuytren's contracture is yet to be determined. 7 Targeted evaluation is required to establish if the PROMs used in Dupuytren's research are providing meaningful data.
A literature review was carried out to identify studies using a PROM in research investigating surgical treatment for Dupuytren's contracture and to determine if responsiveness could be calculated from the available data. A pilot study conducted in 2007 investigating the responsiveness of three PROMs administered before and three months after a fasciectomy and dermofasciectomy is then presented. The findings of the 2007 pilot study and the recent literature review are discussed with the aim of informing a definitive study.
Responsiveness
Responsiveness is the ability of an instrument to detect change over time; however, a further operational definition of responsiveness is needed to give it meaning within the context of this study.3, 8 The following are the two operational definitions of responsiveness that will guide this investigation:
Responsiveness as an indicator of treatment effect regardless of the significance of the effect, normally expressed as the effect size (ES) or standardized response mean (SRM).3,8,9 An ES or SRM <0.5 is small, >0.5 moderate and >0.8 large. 10 A moderate or large ES or SRM indicates good responsiveness for a PROM. 11 An ES and SRM provide a unit-free value from which the responsiveness of different PROMs can be compared. 12
The responsiveness of a measure with regards to what is clinically relevant in relation to an external criterion.4,9,13–15
As the aim of the study is to evaluate outcomes from the patient's perspective it would be prudent for the external criterion to consider the patient's opinion of change. 3 The standard method of measuring the patient's opinion of change is in the form of a transition question asking what their status is now compared with before treatment.9,13,15–17 Response is given in the form of a Likert scale (e.g. much better; somewhat better; no change; somewhat worse and much worse). 17 Patients indicating they are much or somewhat better are defined as clinically improved.9,13,15–17 The mean change in score for those patients indicating improvement is defined as the minimal clinically important difference (MCID). 15 The MCID attributes meaningfulness to the PROM by providing a value associated with a patient's sense of improvement. 18 Transition questions have also been shown to correlate with patient satisfaction levels thus attributing further value to their use.19, 20
Literature review of PROM use in Dupuytren's research
A literature review was conducted to investigate the responsiveness of PROMs in patients with Dupuytren's disease treated by fasciectomy or dermofasciectomy. A PROM applied to a surgical population would need to demonstrate a clinically worthwhile treatment effect despite postsurgical recovery and potential complications that would not be as prevalent in a non-surgical population. Therefore, non-surgical interventions such as needle aponeurectomy and collagenase were excluded as they are less invasive with shorter recovery times and therefore not comparable to surgical intervention.21, 22 Studies with less than a three-month follow-up were also excluded as prior to this period of recovery there is still a degree of postsurgical healing that could mask the effect of surgical intervention.23, 24 Only studies with preoperative and postoperative PROM data were included to allow for evaluation of responsiveness. Finally, the search was limited to publications from 2000 to date as measurement of activity and participation is a recent phenomenon and it is unlikely that earlier articles included a PROM. 1
The electronic bibliographic databases CINAHL, EMBASE and MEDLINE were searched in 2007 and again in March 2012 for English language publications using the terms Dupuytren's, fasciectomy or dermofasciectomy. Six hundred and seven papers were identified. The title and abstract were screened and PROM use was identified by reviewing the abstracts. When it was not clear if a PROM was used, the full text article was obtained and reviewed. The reference lists of papers using a PROM were also searched.
The literature review identified seven papers using three PROMs while investigating Dupuytren's surgery or postoperative management.7,25–30 The three PROMs used were the Disabilities of the Arm, Shoulder and Hand (DASH), QuickDASH and Michigan Hand Questionnaire (MHQ).23,31,32 Table 1 gives a description of these PROMs.
Full text articles were obtained for all seven studies utilizing PROMs to determine if sufficient raw data were available to evaluate responsiveness in accordance with the operational definition. All the studies provided the mean change score or sufficient raw data to calculate the mean change score of the PROM (Table 2). The Skoff and Zyluk and Jaglielski studies present the DASH raw score, however, this can be converted into a final DASH score by using the recommended scoring method.26,27,33 An assumption was made that all the items in the DASH were completed. Although, a mean change score in itself is not part of the operational definition of responsiveness for this study, it is required in order to calculate an ES and SRM. A mean change score in itself can be considered evidence of responsiveness when it is in the direction expected following an intervention that is known to be effective; however, it does not allow for comparison between PROMs to determine relative responsiveness in a given situation. 33 All of the studies show a mean change of PROM score in the direction of improvement.
A summary of PROMs evaluated
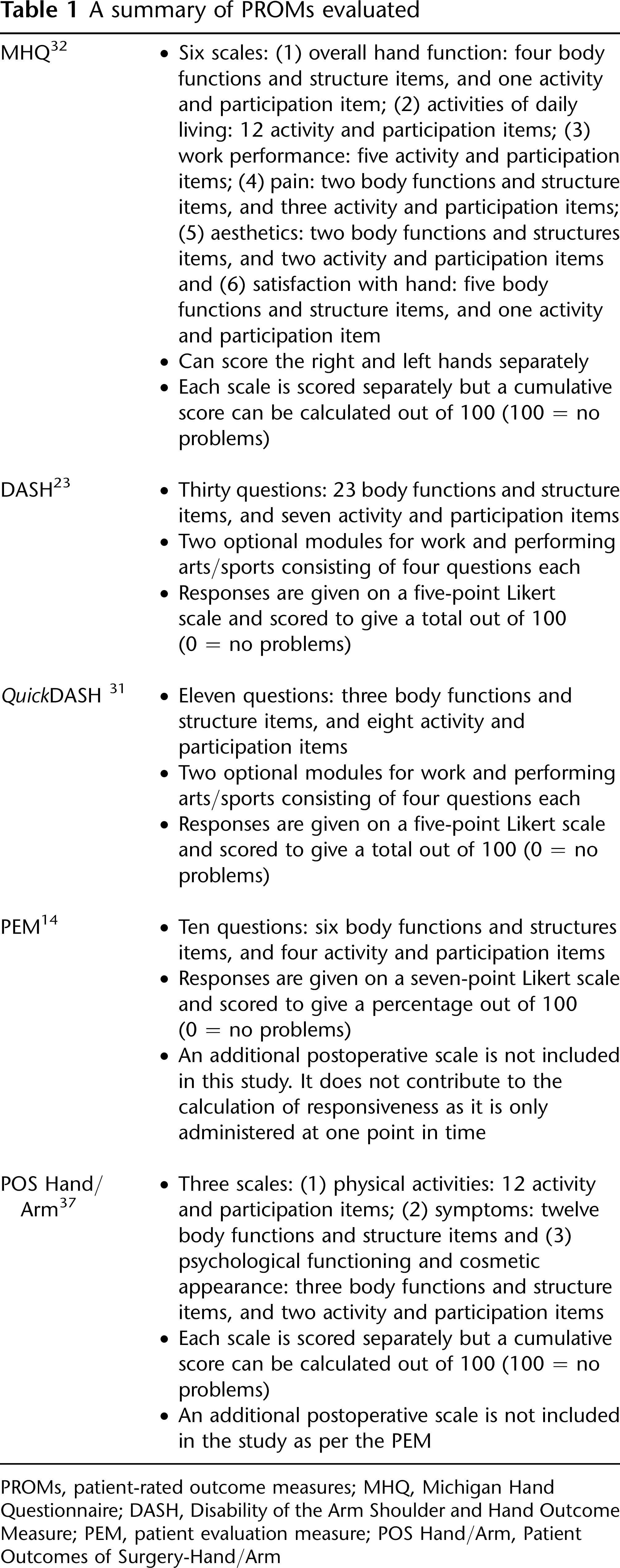
PROMs, patient-rated outcome measures; MHQ, Michigan Hand Questionnaire; DASH, Disability of the Arm Shoulder and Hand Outcome Measure; PEM, patient evaluation measure; POS Hand/Arm, Patient Outcomes of Surgery-Hand/Arm
Summary of responsiveness data from Dupuytren's studies using PROMs
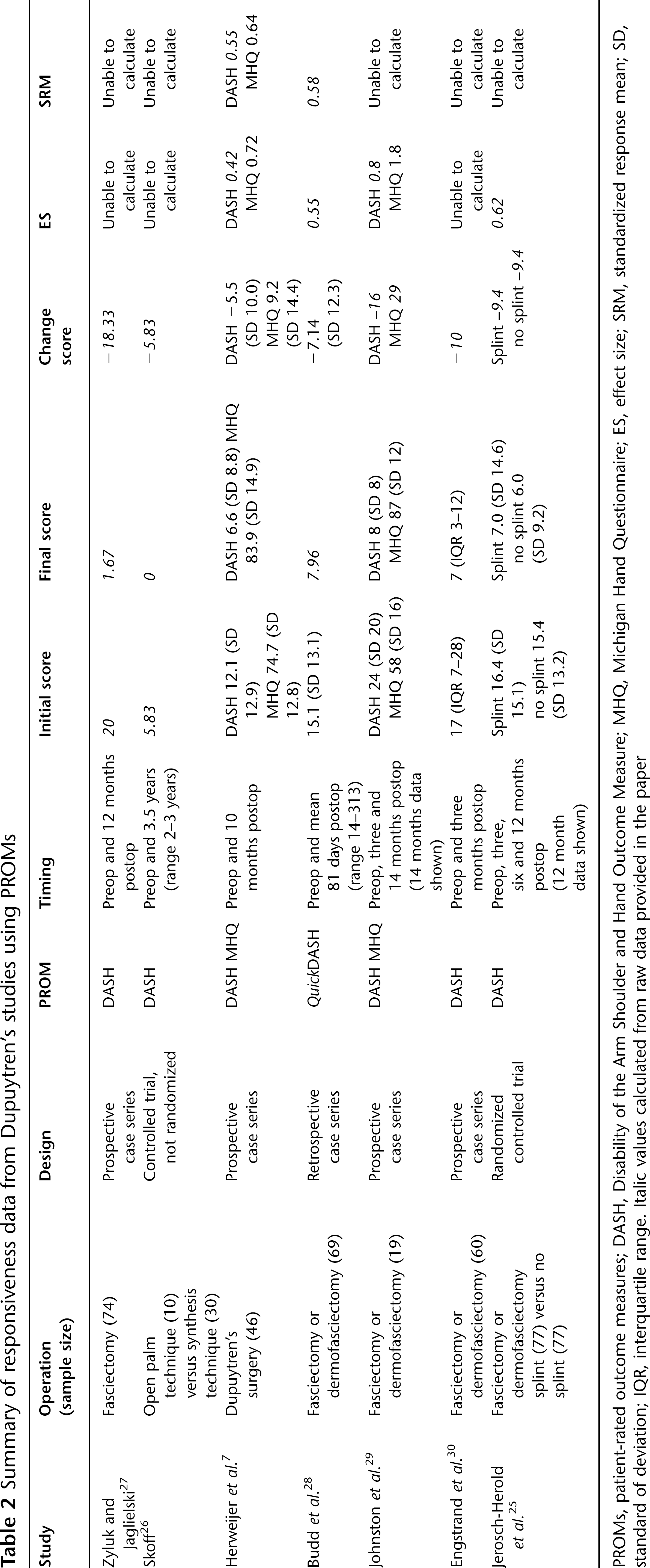
PROMs, patient-rated outcome measures; DASH, Disability of the Arm Shoulder and Hand Outcome Measure; MHQ, Michigan Hand Questionnaire; ES, effect size; SRM, standardized response mean; SD, standard of deviation; IQR, interquartile range. Italic values calculated from raw data provided in the paper
Four of the studies provide sufficient data to calculate either an ES or SRM and allow for evaluation of responsiveness as an indicator of treatment effect regardless of the significance of the effect.7,25,28,29 ES is calculated as mean change in score divided by the standard deviation of baseline score. SRM is calculated as mean change in score divided by the standard deviation of change score (Table 2). The MHQ and QuickDASH ES and SRM values calculated from the Herweijer et al. and Budd et al. studies exceed the 0.5 threshold set as acceptable for PROM responsiveness.7,11,28 The ES for the DASH exceeds 0.5 in the Johnston et al. 29 and the Jerosch-Herold et al. 25 studies but not in the Herweijer et al. 7 paper. Only the Herweijer et al. 7 and the Johnston et al. 29 papers utilized two PROMs, the DASH and the MHQ, in the same population and circumstances and thus allow an evaluation of their relative responsiveness. In both studies, the MHQ fared better than the DASH in terms of ES and SRM values.
This literature review has provided useful initial data regarding the responsiveness of the QuickDASH, DASH and MHQ with Dupuytren's surgery in terms of responsiveness as an indicator of treatment effect regardless of the significance of the effect. Unfortunately, a patient-rated external criterion indicating global change was not used in any of the studies making it impossible to attach clinical meaning to the change in score. In addition, only the MHQ and the DASH have been used in the same cohort to allow for the evaluation of the relative responsiveness of the PROMs. Further investigation is needed regarding the responsiveness of the PROMs in Dupuytren's surgery in order to meet the need for accurate and effective outcome measurement from the patient's perspective.
Pilot study
A pilot study was conducted by the author in 2007 to test the feasibility of conducting a larger scale study and clarify procedures in anticipation of a larger trial. 8 In a pilot study it is inappropriate to draw statistical conclusions due to the small sample size; 34 therefore, the aims of this pilot study were to:
Obtain data on the eligibility and recruitment rates
Evaluate if cost and time implications of conducting the study were acceptable
To obtain initial estimates of the relative responsiveness of the PROM
To obtain initial estimates of acceptability of the PROMs to patients.
Selection of PROMs for evaluation of responsiveness
Eligible PROMs to be included in the pilot study were identified in 2007. Priority was given to the PROMs already used in Dupuytren's research in order to provide evidence to support or refute their use. The DASH and the Patient Evaluation Measure (PEM) had been used in Dupuytren's research at the time the PROMs were selected and were both considered appropriate for evaluation.26,27,35 Although Dias and Braybrooke's 35 study using the PEM to report outcomes following Dupuytren's surgery did not meet the inclusion criteria for the evaluation of responsiveness this did not exclude it from being appropriate for the pilot study. A further literature review was conducted in 2007 to identify if other PROMs existed that would also be suitable but had not yet been used in Dupuytren's research.
Medline (1966 to date), CINAHL (1982 to date) and EMBASE (1983 to date) were searched using the terms ‘outcome measurement’, ‘questionnaire’, ‘hand’ and ‘upper limb’. Several PROMs were identified that were potentially suitable for investigating responsiveness to Dupuytren's surgery. To minimize the burden to participants it was decided to limit the PROMs to three.
Important concepts such as acceptability, clinical feasibility and cultural relevance were considered in addition to relevance to patients with Dupuytren's disease.3, 36 The QuickDASH was selected instead of the DASH as it demonstrates comparable psychometric properties and is more acceptable to the patient and more feasible to use in a clinical setting. 31 It was also being used as an outcome measure in the local hospital and its routine preoperative administration allowed the investigator to unobtrusively determine if the patient could complete a PROM independently and thus be eligible for the study. The PEM and the Patient Outcomes of Surgery-Hand/Arm (POS-Hand/Arm) were also selected as both had been used either to report outcomes in Dupuytren's surgery or included Dupuytren's patients in the development of the questionnaire.35, 37 Both were developed with a British population thus supporting cultural relevance. 3 See Table 1 for a description of the PROMs.
Methods
The pilot study had a prospective observational design using consecutive sampling. Patients attending a routine preoperative assessment clinic prior to undergoing a fasciectomy or dermofasciectomy were eligible. Patients unable to read English were excluded as the PEM and POS-Hand/Arm had not been translated to other languages. Patients who had a visual or mental impairment were also excluded as reliability and validity tests on the PROMs had been performed with patients completing them independently with no evidence to support the examiner verbally administering the PROMs for patients with insufficient reading or comprehension skills.14,31,37
Completion of the QuickDASH in the preoperative assessment clinic is routine practice and adequate language, literacy, visual acuity and mental capacity were assessed by the patient's ability to complete it independently. If the patient was unable to complete the QuickDASH the hand therapist assisted as is normal practice but the patient was not invited to participate in the study. Eligible patients were given a package including the study information sheet, consent form, a checklist, the PEM, the POS-Hand/Arm and a stamped addressed envelope to take home. If they chose to participate they signed the consent form, completed the PROMs and posted the package back to the investigator. No reminders or prompts were given.
Upon receipt of the signed consent form and the completed PEM and POS-Hand/Arm the investigator accessed the participant's preoperative QuickDASH completed as standard practice. Demographic and operation details were obtained from the participant's medical records.
Participants progressed through the standard care pathway for Dupuytren's surgery at the local hospital. At 12 weeks after their operation, participants were posted the QuickDASH, PEM and POS-Hand/Arm, a checklist of what to do, a transition question and secondary outcome measures consisting of questions regarding length of time to complete and ease of understanding of each PROM. These secondary measures were designed to assess acceptability and feasibility. 3 The question examining ease of understanding was drawn from the Hand Clinic Questionnaire developed in Oswestry, UK and published by Sharma and Dias. 14 It simply asks the patient to rate if the PROM was ‘very easy to understand’, ‘difficult to understand but I managed’ or ‘impossible and I needed help’. The participants completed the forms and returned them in the stamped addressed envelope provided.
The study was peer reviewed and approved by the investigator's educational institution and the local hospital's research and development committee. Participants were informed that this was a pilot study as part of a student project. Ethics approval was obtained from the local research ethics service. Patient information and questionnaires were reviewed by representatives from a local senior's advocacy group. Confidentiality was protected at all times in accordance with the Framework for Research Ethics and Data Protection Act (1998).38, 39
Results
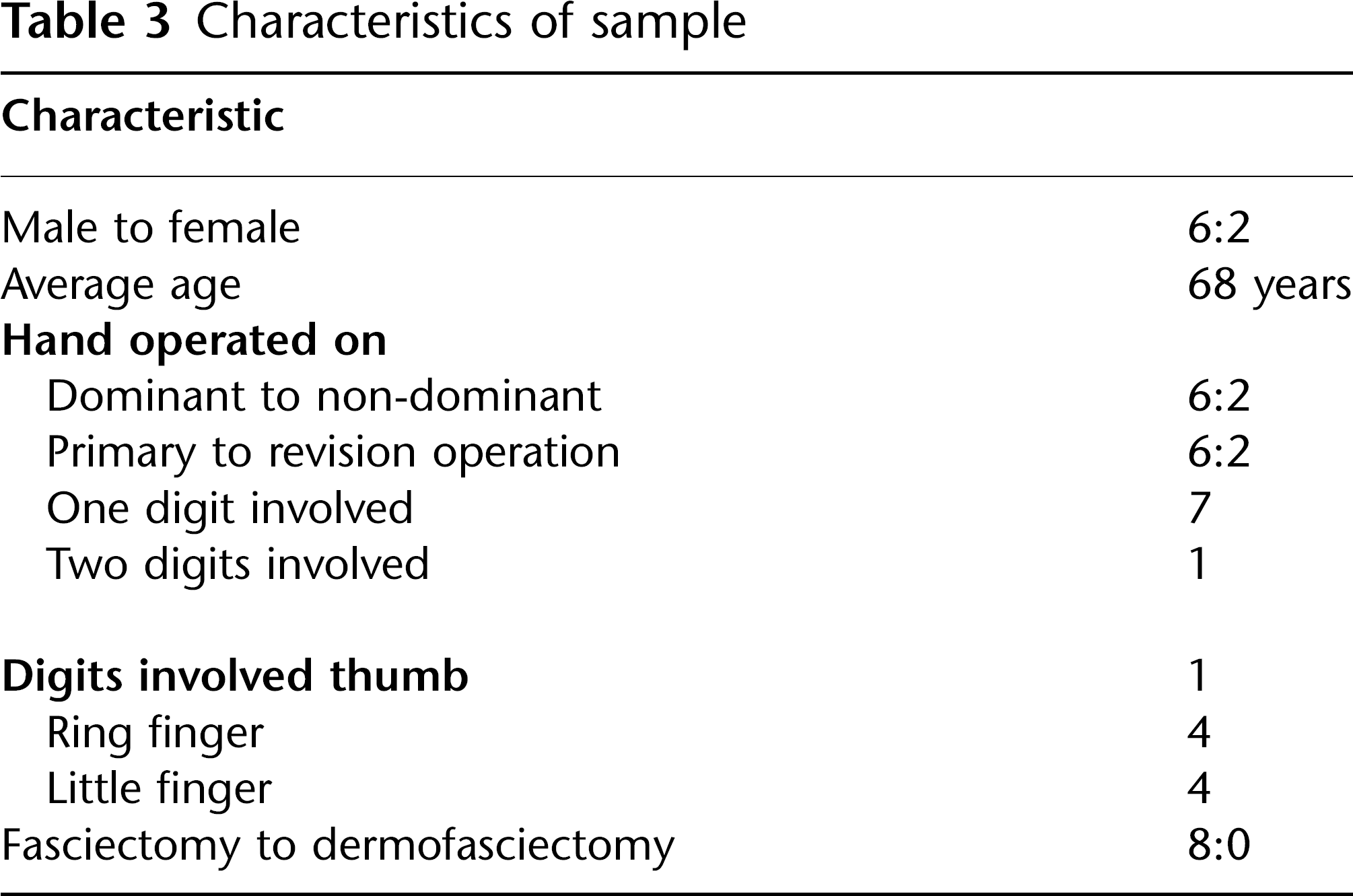
Fifteen consecutive patients attending the orthopaedic upper limb preoperative assessment clinic for Dupuytren's surgery met the inclusion criteria during the six-week recruitment period in 2007. One was excluded due to an inability to complete the routine QuickDASH independently. Fourteen patients were invited to participate. Nine patients returned the completed PROMs with a signed consent form. One participant later opted to have a needle aponeurectomy and was subsequently excluded. Characteristics of the sample are presented in Table 3.
Characteristics of sample
The participants rated all the PROMs as very easy to understand. The PEM was the quickest to complete followed by the POS-Hand/Arm then QuickDASH. The PEM was also the quickest to score followed by the QuickDASH then the POS-Hand/Arm. The QuickDASH had the fewest items left blank followed by the PEM then the POS-Hand/Arm (see Table 4).
Ease of use of PROMs
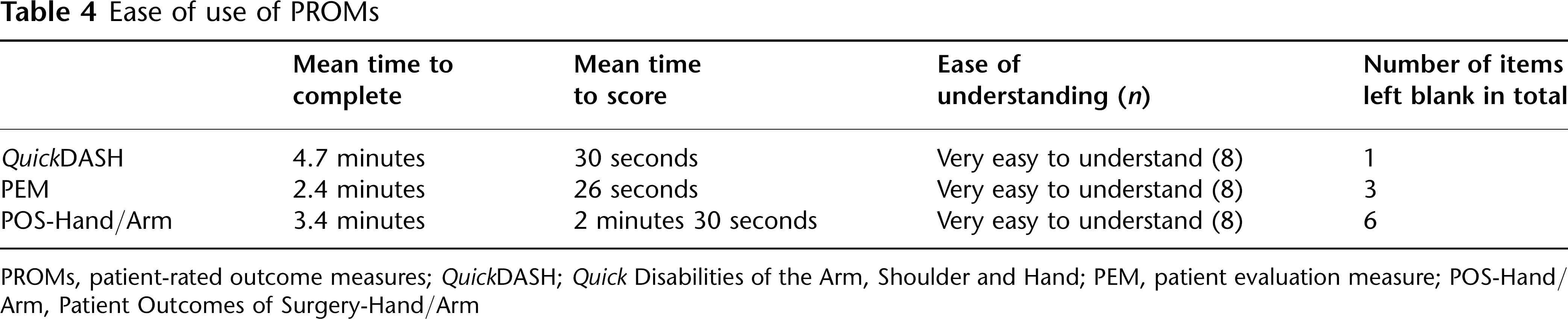
PROMs, patient-rated outcome measures; QuickDASH; Quick Disabilities of the Arm, Shoulder and Hand; PEM, patient evaluation measure; POS-Hand/Arm, Patient Outcomes of Surgery-Hand/Arm
In response to the transition question ‘how would you rate the change in the status of your hand from the way it was before the operation to now?’ five patients responded ‘much better’ and three indicated ‘somewhat better’.
The PEM showed the greatest ES and SRM followed by the POS-Hand/Arm then the QuickDASH (Table 5).
Responsiveness of PROMs

PROMs, patient-rated outcome measures; QuickDASH; Quick Disabilities of the Arm, Shoulder and Hand; ES, effect size; PEM, patient evaluation measure; POS, patient outcomes of surgery; SRM, standardized response mean
Discussion
This literature review and pilot study have examined the responsiveness of the PROMs used for Dupuytren's surgery in terms of (1) being an indicator of treatment effect regardless of the significance of the effect and (2) being able to reflect change that is clinically relevant by anchoring it to a patient-rated external criterion.4,9,13–15 For treatment effect the literature review demonstrated that the MHQ and QuickDASH exhibit an acceptable ES and/or SRM in the studies for which they could be calculated.7,25,32,33 However the variation of the ES and SRM values for the same PROM in different papers reflects the difficulty in comparing the treatment effect of PROM's across studies. Factors such as time of follow-up, sample size and technique, surgical skill and therapeutic intervention will influence change in PROM scores and thus make it impossible to determine their relative responsiveness.40, 41 Relative responsiveness can only be accurately judged when the PROMs are applied in the same circumstances, as in the Herweijer et al. and Johnston et al. studies where the MHQ was evaluated to be superior to the DASH in terms of treatment effect.7,29,33
The pilot study was designed to allow for evaluation of the relative responsiveness of PROMs in Dupuytren's surgery as they are administered to the same population in the same circumstances. A limitation of this pilot study is its small sample size limiting conclusions to be made about the ES and the relative responsiveness of each PROM. The PEM demonstrated the largest ES followed by the POS-Hand/Arm followed by the QuickDASH. The DASH and QuickDASH have shown comparable responsiveness when applied to the same population in other conditions and it is reasonable to assume that they would behave in a similar fashion when applied to the same patients undergoing Dupuytren's surgery.31, 42 The DASH has been widely used in Dupuytren's research and it is significant to note that both this literature review and pilot study have found that the DASH/QuickDASH are not as responsive as other PROMs. 43
The literature review and the pilot study were not able to provide evidence for the second operational definition of responsiveness for any of the PROMs used in Dupuytren's research. None of the studies in the literature review asked the patients if they had improved from their preoperative status and the pilot study did not have a sufficient sample size to provide a meaningful calculation of an MCID. An MCID value is a useful responsiveness statistic because it allows for interpretability of change in the PROM score at an individual level as opposed to treatment effect, which is more useful for comparison of PROMs at group level. 33 However, an MCID has greatest value in terms of responsiveness if it exceeds the minimal detectable change (MDC), defined as the minimum change in score beyond that of measurement error.33, 44 If the MCID is greater than the MDC then this gives greater confidence that the change in score is due to a clinical change and not due to day-to-day variability in score. 33
An MCID value is published for the DASH, however, the authors caution against considering MCID as an absolute value and that it is more likely to vary in differing circumstances. 33 Work is ongoing to determine MCID values for the DASH but at the moment it is recommended to use an MCID of 15 points exceeding the MDC at a 95% confidence interval of 13 points. 33 As the initial scores of the DASH/QuickDASH in the literature review and the pilot study ranged from 5.83 to 24 with change in scores ranging from 5.5 to 18.33 it is possible that an MCID calculated from a Dupuytren's responsiveness study would not exceed the MDC of 13 points. Further research is needed to calculate an MCID for the DASH/QuickDASH with a Dupuytren's specific population to then compare with the MDC.
MCID values are published for the MHQ but are reported for each of the three domains and not the total score. 45 Unfortunately, neither the Herweijer et al. 7 nor the Johnston et al. 29 studies provided the raw data for each domain with which to compare the published MCID. MDC values have not been published for the MHQ and MDC and MCID values are not known for the PEM and POS-Hand/Arm. To fulfil the second operational definition of responsiveness further research with these PROMs would need to include calculations of the MDC with which to compare an MCID determined with a Dupuytren's specific population.
The literature review and pilot study have identified that the MHQ, PEM and POS-Hand/Arm and the DASH/QuickDASH warrant further investigation in a larger study investigating relative responsiveness in patients undergoing Dupuytren's surgery. In addition to these PROMs a Dupuytren's disease-specific PROM has recently been introduced. 46 The Unité Rhumatologique des Affections de la Main (URAM) was investigated with a population undergoing needle aponeurotomy, thus not meeting the inclusion criteria for the literature review and was published after the pilot study. The URAM has been shown to be reliable, valid and responsive with this population and has been translated into English. It warrants inclusion in future studies investigating responsiveness with a surgical population although the practicalities and patient burden of using multiple PROMs need to be considered.
The purpose of this pilot study was to test whether the procedures were ethical and feasible. The pilot study achieved a 57% recruitment rate and provides a realistic estimation of 38 weeks needed to recruit a target sample size of 50 if the same recruitment procedures are used. The 100% retention rate and the PROMs all being rated as very easy to understand suggest that completing the PROMs was not an onerous task for the participants. However, ease of use data such as items left blank and time to complete the PROMs are also indicators of acceptability to patients and will be useful in informing selection of PROMs for further investigation. 3 In ethical and practical terms it is felt that it would be feasible to continue this project as a full study with further consideration of the PROMs that will be included.
Conclusion
The use of PROMs is being promoted as an important driver that will influence health policy and consumer choice. It is crucial that the choice of PROMs is based on robust data. This literature review and pilot study are the preliminary steps for a larger study that will contribute to the evidence base on the responsiveness of PROMs with Dupuytren's surgery.
Footnotes
Acknowledgements
The author thanks JP and TF for approving this project and allowing study time. JD for advice and assistance with regard to R&D and ethics. PC and TR for supervising this project which was conducted as an independent study towards an MSc in Hand Therapy through Derby University.