
Abstract
Objective
To determine the validity of a self-diagnostic questionnaire for Dupuytren's disease among rock climbers.
Methods
A simple, self-diagnostic questionnaire for Dupuytren's disease was freely distributed to climbers in Austria and Germany. None of the subjects were medically prescreened. The questionnaire consisted of four questions with pictures concerning their present diagnosis and the differential diagnosis for Dupuytren's disease. Medical experts then clinically examined those climbers who completed the questionnaire for Dupuytren's disease.
Results
Sixty-one climbers (46 men, 15 women; mean age 32 [13] years; climbing for 10 [11] years) participated in the survey; 16 participants were competition climbers. Clinical diagnosis of Dupuytren's disease was confirmed in five cases (8.2%). The questionnaire produced no false-negatives, but there were three (4.8%) false-positive results in this sample. The correlation between the self-diagnostic tool and the clinical examination was r = 0.62 (P = 0.005). No significant difference (P = 0.250) was found between the self-diagnostic tool and the clinical examination. The sensitivity of the self-diagnostic tool in a sample of rock climbers was 100%, and its specificity 94.9%.
Conclusions
The questionnaire is an accurate and precise self-diagnostic tool for rock climbers to determine the diagnosis of Dupuytren's disease.
Introduction
Dupuytren's disease is a fibroproliferative disorder of the palmar fascia that can result in contractures of one or more fingers. The aetiology of Dupuytren's disease is not completely clear and many predisposing factors have been discussed. 1–3 Depending on the selected population, their geographic origin, gender and age, the prevalence of Dupuytren's disease varies widely from 4% to 19%. 2,4 Prevalence increases with age and is higher in men. 2,5
The diagnosis of Dupuytren's disease includes inspection and palpation of the palms and fingers during physical examination. 3,6 Dupuytren's disease occurs when palpable nodules (small growths or lumps of tissue) appear in the connective tissue of the palm, under the skin. These typical nodules are a definite sign of Dupuytren's disease. 2,7 Isolated palmar nodules do not impair manual abilities or cause pain. Over time, these nodules can grow into cords of contracted tissue. 8 Once the tissue has contracted, it becomes difficult to fully extend the finger. Over time this contracture can become fixed in a permanently flexed position. One or more fingers may be affected. 9 It is at this advanced stage that medical advice is typically sought. 10
A self-diagnostic tool could help affected persons to identify early signs of Dupuytren's disease and seek medical advice before contractures develop. Once a contracture becomes permanent, surgery is the only option available.
Rock climbers use diverse grip techniques with high torque movements of the upper limb which transmit extremely large forces onto the hands and fingers. 11,12 These forces put heavy stress especially on the palmar fascia, which is usually the primary affected tissue in Dupuytren's disease. 13 Logan et al. 13 suggested that the repetitive trauma to the palmar fascia in rock climbers may predispose them to the development of Dupuytren's disease. Their postal questionnaire to 1100 climbers had a response rate of 51% (almost exclusively men). Dupuytren's disease was found in 19.5% of the respondents (mean age 58.4 years). Years of climbing and its intensity were higher in affected climbers. This postal questionnaire was not followed up by a physical examination by medical experts to verify the results.
Therefore the purpose of this study was to determine whether rock climbers could accurately and precisely self-diagnose the presence of Dupuytren's disease using the proposed questionnaire. Medical experts verified the results once the questionnaire was completed by physical examination. This data acquisition is part of a larger study concerning the prevalence of Dupuytren's disease in rock climbers based in Central Europe.
Methods
Data collection was carried out between April and October 2007 in Austria and Germany. This observational study comprised two parts: self-completion of the questionnaire immediately followed by an examination by a physiotherapist or by an orthopaedic surgeon, both with a special interest in hand injuries. The self-diagnostic part of the questionnaire contained four questions (see Figure 1). An explanation of the questionnaire, including detailed information about Dupuytren's disease and its clinical signs, formed part of the introduction of the questionnaire. The study was approved by the Centre of Sport Sciences and University Sports, University of Vienna and participants gave fully informed consent.
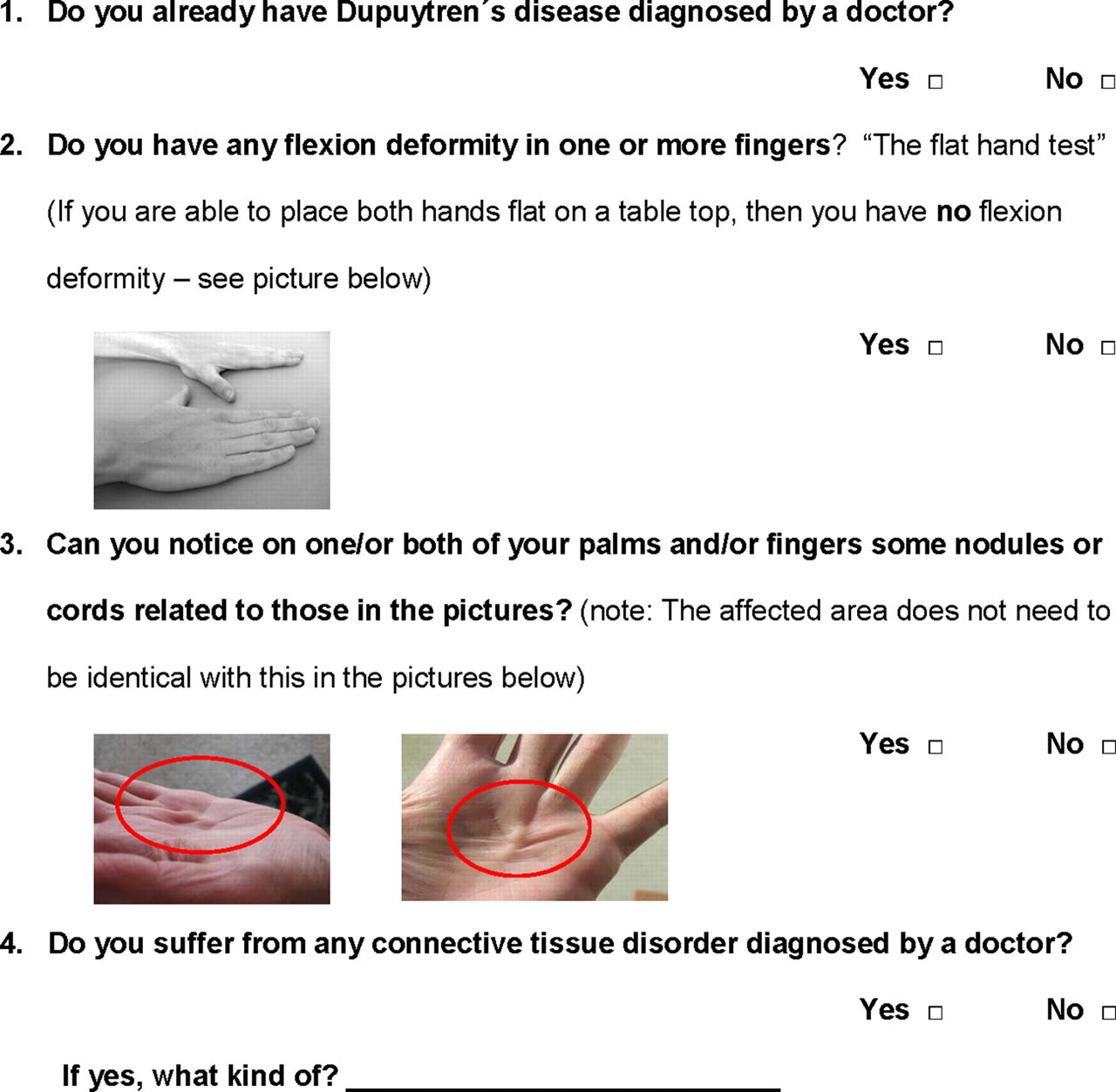
Self-diagnostic section of the questionnaire
To avoid any bias, none of the subjects were prescreened for Dupuytren's before completing the questionnaire. The venues chosen for data collection were known to attract dedicated and interested climbers, either as contestants or viewers at climbing competitions.
The questionnaire used the classification of Iselin and Dieckmann for Dupuytren's disease. 14 The appearance of an isolated palmar nodule of the palmar fascia without contracture corresponds to Stage 1 in the classification of Iselin and Dieckmann. This is the minimal sign of a positive diagnosis of Dupuytren's disease. A flexion deformity of one or more fingers alone without palpable nodules in the palmar fascia was insufficient for a positive diagnosis, as it is mainly the consequence of pulley injuries or joint capsular injuries in rock climbers. 11
Results from participants with already diagnosed Dupuytren's disease and/or a connective tissue disorder were excluded from this investigation. Incomplete questionnaires were omitted from the study.
Statistical analysis
To quantify the diagnostic ability of the self-diagnostic tool sensitivity and specificity were calculated. 15 A two-way contingency table analysis by χ 2 test was conducted to evaluate whether any association between the diagnostic tool and the clinical examination could be shown.
The continuity correction was applied and because of small expected frequencies Fisher's exact test was used. Additionally the McNemar's test was performed to determine equal frequencies in the variables. Two-sided significance was set at a 5%-level. Data are expressed using medians and interquartile ranges (IQRs). All statistical analyses were conducted using SPSS version 15.0 for Windows (SPSS Inc, Chicago, IL, USA).
Results
Sixty-three subjects completed the questionnaire and were examined by medical experts. Sixty-one, 46 men and 15 women, were included in this investigation. Two subjects were excluded because of already diagnosed Dupuytren's disease. All subjects were of Caucasian origin. Their median age was 32 (IQR = 13) years, ranging from 20 to 60 years. They had participated in rock climbing for 10 (IQR = 11) years. Sixteen of the included participants (26.2%) attended climbing competitions. Five persons (8.2%) reported an isolated palmar nodule of the palmar fascia without contracture, which corresponds to Stage 1 by Iselin and Dieckmann. One (1.6%) reported a flexion deformity without palmar nodule. Two subjects (3.3%) showed clinical signs of Dupuytren's disease verified by the clinical examination, in contrast to false self-diagnosis of Dupuytren's disease by three subjects. These three false-positive diagnoses were rectified by the medical experts during physical examination. Table 1 shows the results of the questionnaire and the clinical examination.
Contingency table: results of the self-diagnostic tool and the clinical examination (n = 61)
The sensitivity of the item isolated palmar nodule is 100% and its specificity 94.9%. The relationship between the item isolated palmar nodule and the clinical examination was r = 0.62 (χ 2 = 12.263, df = 1, P = 0.005). A difference (P = 0.250) between the results of the item isolated palmar nodule and the clinical examination could not be found.
Discussion
This self-diagnostic tool seems to be very valuable for detecting conditions at an early stage especially in a rock climbing community in which doctors are reportedly not often consulted. 16 A correlation (r = 0.62) between the self-diagnostic tool and the examination by medical experts was demonstrated. The self-evaluation protocol identified all participants with signs of Dupuytren's disease; none of the participants missed a positive diagnosis leading to a sensitivity of 100%. The false-positive diagnosis of three participants (specificity 94.9%) was rectified by medical experts during physical examination using a protocol including inspection and palpation of palms and fingers. Two of the rectified diagnosis had scars in the palm of their hands from previous injuries and the third climber showed some kind of callosity in his palm, but no Dupuytren's disease nodule. This method may be used as a valid tool for self-assessment. Negative health consequences would thus be avoided.
These findings raise the question if screening for Dupuytren's disease should be included in the health screening process by the national health system in its yearly preventive medical checkups. Townley et al. 10 specifically suggest that there would be no need for treatment in all cases whereas regular follow-up of Dupuytren's disease is indispensable for detecting early joint contractures and surgical intervention in case of indication. It is well established that the duration of untreated deformities leads to a higher risk of irreversible joint contracture. 2,4,17 An appropriately timed referral to a surgical specialist can prevent permanent loss of manual function. 17 To this end it is essential that patients suffering from this disease be made aware of the benefits and options of an early diagnosis.
Furthermore, successful non-surgical methods of treatment have been published in recent studies. 18–20 Injections with collagenase have shown early clinical promise for stages of mild disease 18,19 and a study by Betz et al. 20 concludes that radiotherapy effectively prevents disease progression for early stages of Dupuytren's contracture.
By means of a few carefully worded questions the self-diagnosis of Dupuytren's disease could be incorporated into health screening programmes.
Limitations
A clear limitation of this study is the small prevalence (3.3% [n = 2]) of Dupuytren's disease in our sample. The reason might be the young age of 32 (13) years compared with the mean age of 58.4 years in the study by Logan et al. 13 The bias of this study may be that participation attracts those climbers who are concerned about the health of their hands. This investigation should ideally be repeated with a larger sample size and therefore a higher number of positive findings.
Footnotes
Acknowledgements
Our special thanks go to Audry Birute Morrison and Anna Krumboeck for proofreading with helpful comments and criticism.