
Abstract
Introduction
A rehabilitation group intervention has been an established treatment programme for patients with complex hand injuries requiring intensive therapy input.
Methods
A prospective audit of 20 patients was carried out to evaluate the outcomes of those attending the group with regard to improving hand function. The Disabilities of the Arm, Shoulder and Hand assessment was employed as a before and after measure of outcome.
Results
Nineteen out of 20 patients demonstrated an improvement in their hand function following group intervention. Patients with injuries uncomplicated by complex regional pain syndrome (CRPS) demonstrated the highest level of improvement. Patients with CRPS demonstrated the lowest level of improvement.
Discussion
Group therapy programmes are a valuable tool in delivering intensive therapy intervention to patients with complex hand injuries. Patients with injuries complicated by CRPS may benefit more from individualized therapy intervention.
Introduction
The Hand Therapy Department at St George's Hospital has been running a rehabilitation group for several years. The group is designed to provide flexible, tailor-made rehabilitation with each patient provided with a specifically designed programme to be undertaken within a supported group environment. As an intervention, group therapy has many potential practical and psychological advantages. Exponents of the use of therapeutic groups have identified positive benefits to members including: universality, cohesion, altruism and instillation of hope. 1 Active engagement in group activities can also facilitate a reflective and adaptive process through the participation in specific tasks. 2 This in turn, provides an opportunity for personal synthesis and growth, providing an individual with new knowledge, challenges, experiences and goals. 2
At St George's Hospital it was observed by therapists that the patients attending the rehabilitation group appeared to benefit from working on their therapy programmes within a group environment, providing each other with support and encouragement. In particular it was noted that group patients who were reaching the end of their therapy intervention gave hope and motivation to those at the early stages of their recovery.
The group comprises 6–8 patients with complex hand injuries and is facilitated by two therapists. Patients attend the group for a 1.5-hour session twice weekly, initially for a period of six weeks which is then extended at the discretion of the treating therapist. This format allows the team to deliver three hours of therapy intervention each week, a level of intensity that it would not be possible to provide on a one-to-one basis due to caseload pressures. Each patient follows an individualized therapy programme designed to address functional goals. Remedial and simulated tasks that address specific deficits are undertaken by the patient. Grading of activity and monitoring of patient progress is undertaken by the group therapists session by session.
The rehabilitation group was considered to be a valuable intervention; however, patient outcomes had not previously been evaluated and hence the belief in the value of the group was based on therapist observations of individual patients. Discussions among the therapists within the Hand Therapy team regarding experiences of managing patients with complex regional pain syndrome (CRPS) attending the group had highlighted a concern that this group of patients was not demonstrating the same level of benefit.
It is recognized that patients with CRPS will often require psychological intervention and support to deal with the condition, which in turn will affect an individual's ability to participate in activities, particularly in a group setting. 3 Therapists working in a group environment need to be responsive and sensitive to the emotional support these patients require. This may result in activities within a rehabilitation programme needing to be graded and adapted more regularly to accommodate changes in symptoms and pain levels, commonly seen in CRPS. As a result, this may affect the patients’ perceived benefits and outcomes of attending a rehabilitation group.
A prospective audit was therefore undertaken to measure the outcomes for the group in order to evaluate the current service and assess any need for development. The audit also aimed to address the question as to whether the group might be more effective in treating patients with certain diagnoses than others.
Patient outcomes were evaluated using the patient reported outcome measure Disabilities of the Arm, Shoulder and Hand (DASH). 4 The DASH was developed as an outcome measure to provide an evaluation of disability and symptoms for an individual with single or multiple disorders of the upper limb.4, 5 The DASH allows for monitoring of patient changes at a single point or at many points in time and covers a broad spectrum of performance areas encompassing functional activity, physical symptoms and the psychosocial impact of disability.4–6 The DASH was originally utilized for patients with specific upper extremity disorders such as carpal tunnel syndrome, and there is little literature available on the use of the DASH in patients who have sustained a traumatic hand injury. 7 However, the DASH shows potential for use in a trauma population as it is one of the most validated measures of upper extremity function in disorders of the upper limb. 8 In a study undertaken by Wong et al. 7 the authors identified significant changes in DASH scores between admission and discharge of patients with hand trauma, suggesting that it can be used to assess improvements in patients who have sustained a hand injury due to trauma. In the case of this audit of patients within a hand rehabilitation group, the majority of patients had sustained upper limb trauma.
Methods
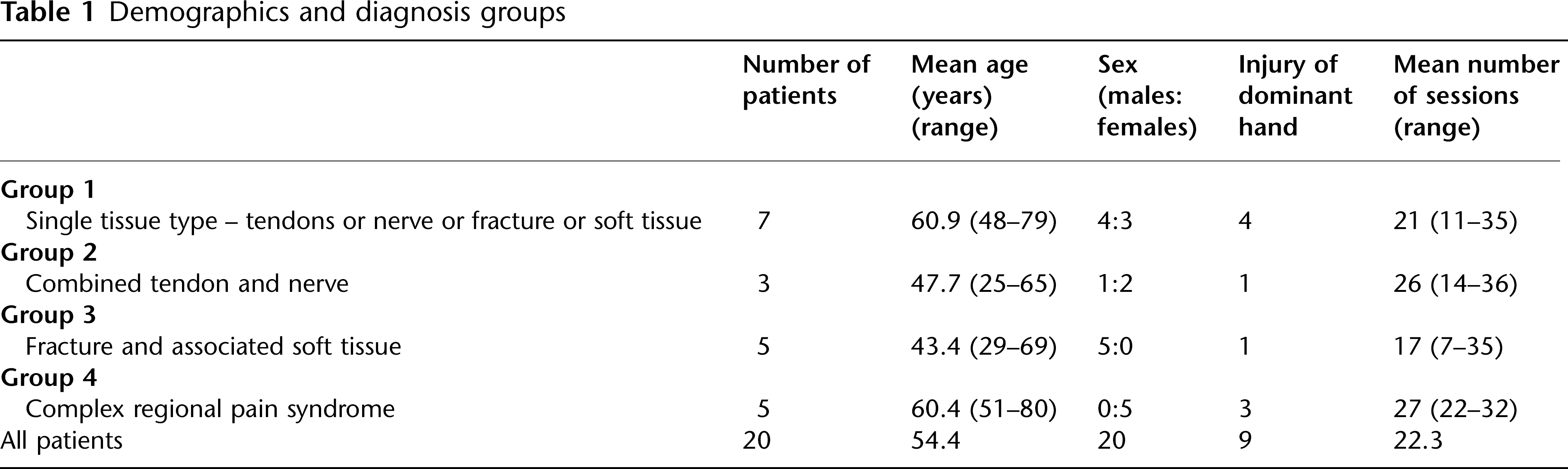
Twenty patients (10 men) attending the group between April 2009 and May 2010 were included in this audit. All patients attending the group during the audit period were included. A DASH questionnaire was completed by each patient before starting in the group and at the end of their last group session. In order to address the audit question the results were first divided into four patient groups depending on diagnosis. The diagnosis categories represent the range of complexity of the patients referred into the rehabilitation group. Demographics and diagnosis groups are detailed in Table 1.
Demographics and diagnosis groups
The DASH is a self-reported questionnaire. It comprises 30 questions each of which are rated on a 1–5 Likert scale (with 5 demonstrating the most severe disability). The developers of the DASH decided that a five-point response scale would allow sufficient room for an individual to describe the degree of change they were experiencing with a task which is needed if an assessment is to monitor change over a period of time.4–6 A lower score on each item demonstrates little or no difficulty undertaking the task in question. Scores are totalled and a scoring equation applied, producing a percentage that describes an individual's level of functional ability. 9 The DASH was selected to evaluate the group data as it provided a widely used and validated patient reported outcome measure that was easy to administer, available within the department, familiar to the team and applicable to a variety of diagnoses.
Analysis
The audit standard was set as an expected 15 point improvement. Test–re-test reliability studies for the DASH suggest that a change in a score which exceeds 15 points is the most accurate change score for discriminating between improved and unimproved patients. Therefore when a patient achieves such a change therapists can be confident that this represents a true change in function and symptoms.5, 9 Before and after analysis of DASH scores (calculated using the standard formula) was undertaken for individual group members and within the group categories.
A secondary analysis of the results was also undertaken by measuring the percentage of scores moving from a rating of 3–5 to a rating of 1–2 following completion of the group programme. We acknowledge that evaluation of the DASH in this way has not been validated; however, it was recognized by the therapists that a movement of score on any item from 3–5 (moderate difficulty, severe difficulty and unable) to 1–2 (no difficulty and mild difficulty) represented an improvement in outcome. This was felt to be useful from a therapist perspective in developing goal-specific treatment programmes and identifying areas of functional limitation. Completion of the group programme was anticipated to achieve a score of 1–2 in 75% of items previously rated 3–5. This additional standard was set following discussion within the Hand Therapy team and based on therapist's perceptions of previous patient improvement.
Ethics
The hand rehabilitation group is an integral component of service delivery within the Hand Therapy team at St George's Hospital. The outcomes of the group were evaluated and audited as part of the ongoing need for proper practice and clinical governance. Patient information was not stored on a computer database of any sort. Therefore Ethics Committee approval was not required.
Results
Results showed that 16 out of the 20 patients achieved a 15-point improvement on the DASH (Table 2). Of those patients who did not achieve this level of improvement three out of the four were from group 4 (CRPS group). Only one of the patients demonstrated deterioration in function as reported by DASH scores. This patient, who was from the CRPS group, went on to have further surgery including amputation of the affected digits.
Before and after DASH scores, percentage of patients achieving audit standards by diagnosis group
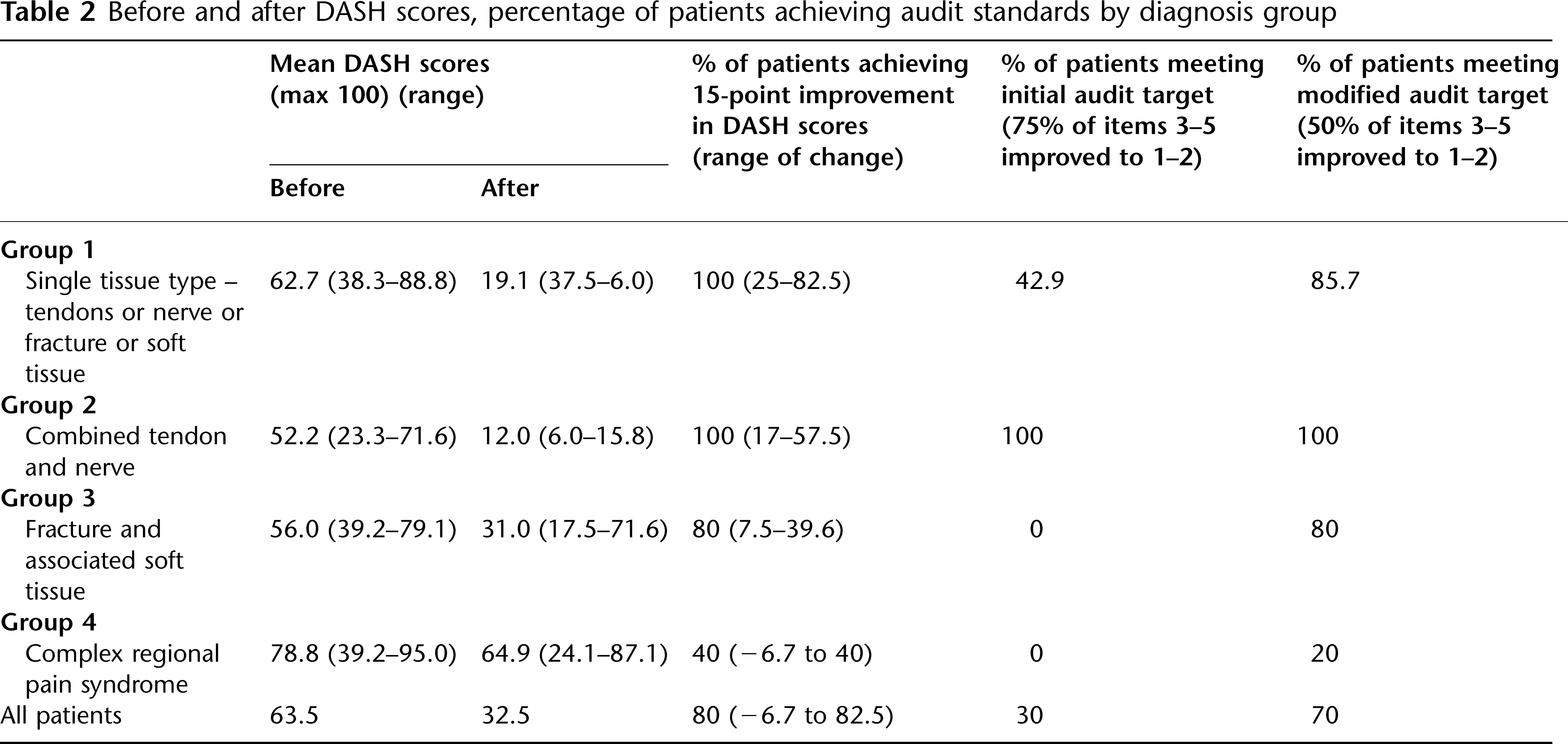
There was an improvement in DASH scores after completion of the rehabilitation group for all patients combined (Table 2); however, only six of the 20 patients achieved the 75% improvement rate (DASH scores graded as 3–5 severity moving to 1–2 postgroup intervention) that was set as the secondary audit standard (Figure 1). The patients achieving this level of improvement were all from groups 1 and 2 with no patients with a combination of fracture/soft tissue injury (group 3) or CRPS (group 4) achieving this standard.
DASH scores 3–5 before and after rehabilitation group intervention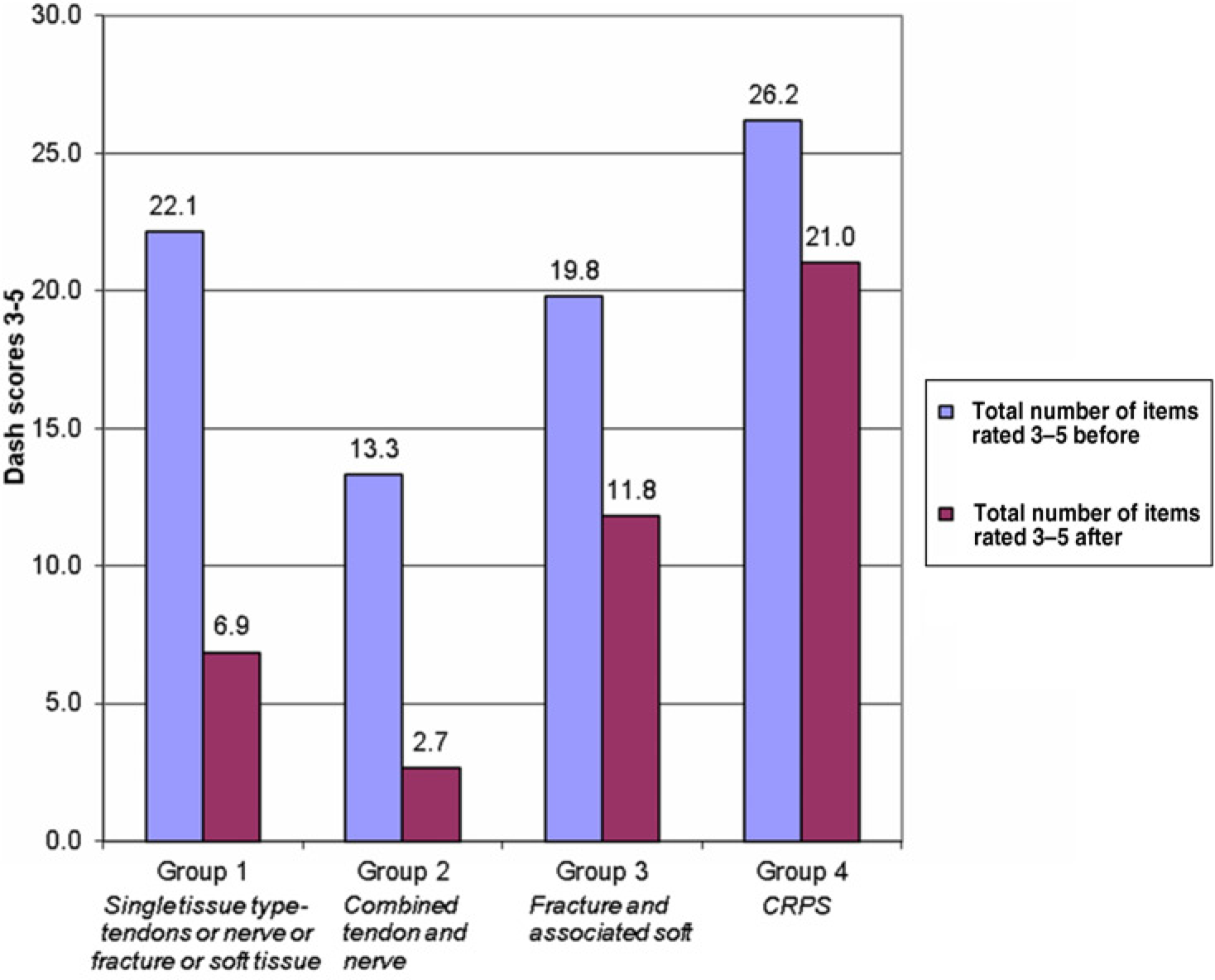
As a 75% improvement was demonstrated in a minority of patients the results were then re-examined applying a 50% improvement rate to determine if this would aid analysis of the intervention. With this modification 14/20 patients achieved this level of change. Groups 1, 2 and 3 all demonstrated a high proportion of patients achieving this 50% improvement rate (6/7 group 1, 3/3 group 2 and 4/5 group 3) while group 4 (CRPS) showed the lowest level of positive change (1/5).
Discussion
This audit aimed to address two questions in relation to the rehabilitation group as an intervention: (a) What are the outcomes for patients attending the group with regard to improving hand function after complex injury? (b) Do all patients regardless of complexity/diagnosis benefit similarly from the group intervention?
This audit demonstrated an improvement in function following hand trauma as represented by the DASH scores. However, the subcategory of patients with CRPS appeared to benefit least from attendance at the group.
It is acknowledged that a larger sample size would have achieved greater power to detect any significant differences between the subgroups, and we would suggest that a larger scale study is justified.
As previously outlined, there is little evidence specifically exploring the use of the DASH in upper-limb trauma populations. However, as the assessment allows for comparison of patients with differing pathology, and is the most widely validated measure of upper extremity the use of the DASH with this population is well supported.7, 8 Owing to the nature of trauma, it was generally acknowledged that an individual would present with a high DASH score at the time of admission to the rehabilitation group. It has been previously reported that patients who undergo trauma and subsequent surgery show large change in scores.7, 10 As the goal of the group and the interventions provided were focused on improving function, and the nature of trauma is that patients will, to a large extent, improve over a period of time, it was anticipated that improvements would be made in DASH scores post-therapy within the hand rehabilitation group.
The additional diagnosis of CRPS creates a different level of complexity and management within a group environment. It has been well reported that the clinical and emotional needs of patients with CRPS will fluctuate, and this may potentially impact the level of intensity required in treatment.3, 11 Anecdotally, therapists working within the rehabilitation group have reported that it may be experienced as disheartening to a patient with CRPS to have their programme altered or adapted within a group setting, while their peers are following a more upwards trajectory of improvement and recovery.
The pathophysiology of CRPS is unclear; however, symptoms including pain, sensory changes, temperature abnormalities and motor signs are all recognized as part of the clinical spectrum of the condition.3, 11 Current guidelines for the management of patients with CRPS are complex with a focus on rehabilitation (incorporating hand therapy, occupational and physiotherapy), pain management and psychological treatment and education.3, 11 CRPS presents many challenges to therapists working in the outpatient setting, and often environmental and clinical constraints do not allow for flexibility in treatment and service delivery.
In addition, the group environment itself presents some challenges for optimizing the treatment efficacy for CRPS. Sensory motor re-education techniques such as graded motor imagery and mirror box therapy can be employed to enhance rehabilitation programmes and have, at times, been incorporated into patient treatment programmes within the hand rehabilitation group. However, these techniques are best undertaken in a quiet environment free from distractions, in order to achieve an optimal outcome.12, 13 A group environment does not allow these techniques to be easily employed in such a setting, and as a result, patients may not get the full benefit from the activities. A 1:1 focus with a therapist may therefore be more appropriate for treating patients with CRPS.12, 13
The audit was completed using a patient-rated outcome measure (DASH). This standardized outcome measure has been demonstrated as a valid and reliable tool for use in this patient group and allows comparison of data from patients with a variety of diagnoses.4–6 It may be useful in future studies to supplement this outcome measure with a goal oriented outcome measure, for example the Canadian Occupational Performance Measure (COPM). 14 This measure would specifically capture patient achievements in personal goals, assist in the development of therapy programmes and supplement the DASH scores in assessing the effectiveness of our intervention.
Prior to the audit, the Hand Therapy team felt that a change in reported DASH scores rated 3–5, of 75% was the desired outcome. However, the majority of patients completing the group demonstrated only a 50% level of improvement. The suggested level of patient improvement may have been over optimistic and indicative of a desire to return patients to full functioning. Therapists’ expectations of patient outcome in hand rehabilitation is an area worthy of further investigation. 15
Undertaking this audit has been helpful in addressing questions regarding the rehabilitation group and has established a method of evaluating the outcomes. This audit indicates that group therapy is a valuable resource for efficient management of complex traumatic hand injuries. The results of this audit have also provided a starting point for further service development through the exploration of rehabilitation methods and care pathways for our CRPS patients.
Footnotes
Acknowledgement
We thank the Clinical Audit Department at St George's Hospital for their assistance.