
Abstract
Summary:
High-risk human papillomavirus (HPV) in a lesion is related to an increased chance of neoplasic transformation, especially when with immunosuppression, as in HIV infection. We investigated HPV frequency in cutaneous and mucosal lesions of HIV-seropositive male patients. The frequency of malignancy, its association with the HPV type detected and some clinical variables were also assessed. A total of 38 lesions from 27 patients were studied in a period of 18 months. The biopsied fragment was submitted to HPV detection and typification, through polymerase chain reaction with generic (MY09/11) and specific (types 6, 11, 16 and 18) primers. HPV frequency was 63.2%, with detection of HPV types 6, 11 or 16 in 18 lesions and with multi-infection in three. There was low detection of high-risk HPV (type 16, 18.4%) and no HPV type 18. Of the lesions, 36.8% were already premalignant or malignant, and the frequency of moderate or severe dysplasia was higher in the study patients than that described in the HIV-seronegative population. High-risk HPV (type 16) was detected in four benign lesions and low-risk HPV (type 6) in three premalignant genital lesions. There was no significant association between the clinical variables and an increase in the prevalence of premalignant or malignant lesions.
Keywords
Introduction
The human papillomavirus (HPV) is significantly disseminated among the world population, being responsible for several clinical entities. It is estimated that genital HPV attacks between 30 and 50% of sexually active adults, presenting itself clinically in only 1% of the cases.1,2 There are over 35 types that infect the genital tract. Of these, types 16 and 18 cause approximately 70% of the cervical cancers and cervical intraepithelial neoplasia (CIN) of high grade (grades II and III); whereas types 6 and 11 cause 90% of the genital warts. 3
Its clinical importance lies in the capacity of some genotypes to induce oncogenic transformation in the infected epithelium. Presence of a high-risk HPV type (such as types 16, 18, 31, 33 and 35) in a lesion is associated with an increased chance of evolution to neoplasia, mainly when immunodepression is prevalent. 4 6 The association between infection by HPV and cancer in the uterine cervix, vulva, vagina, anus and penis is well established, with those cancers being preceded by progressive grades of intraepithelial neoplasia (IN). 7 9 Other neoplasms where HPV was detected, are squamous cell carcinoma associated to epidermodysplasia verruciformis (EV) and oral (mainly tonsillar), oesophagus and non-melanoma cutaneous cancers and cancer of the head and neck.10,11
The infection by HIV, besides facilitating the primary infection by HPV, may lead to persistence of the virus, reactivation of the latent infection or increase of HPV replication. 12 These factors, together with reduction of immunological surveillance, contribute to a neoplasic progression.8,13-15 It seems that in those patients an increase of the integration between viral DNA and the host's DNA occurs, which is an important stage in carcinogenesis. 16 The presence of HPV may also facilitate the infection by high-risk types or multiple infection (more than one type in the same lesions).8,17,18
Studies showed that genital lesions of HIV-positive patients present dysplasic alterations with greater frequency than HIV-negative patients.8,19, Immunodepression caused by HIV is associated to CIN and anal intraepithelial neoplasia, with a multifold increase of the risk of cervical infection by HPV and CIN in women infected by HIV.9,20 Severity of the cervical disease is associated with an increase of immune system degrading, mainly when the CD4 count is ≤200 cells/mm3, with possible response to the use of antiretroviral therapy (ARVT). 21 Other studies indicate that homosexual men, seropositive for HIV, present a high prevalence of anal HPV infection and anal IN.22,23 The relative risk of anal cancer in HIV-positive men is 38 and that in HIV-positive women is 6.8, compared with the general population. 24 HIV-positive patients with bowenoid papulosis also present an increased risk of invasive cancer development. 25
The expanded knowledge of the behaviour of HPV infection in an HIV-seropositive population is of extreme relevance due to the possibility of malignant transformation of the lesion in the presence of high-risk HPV types. Other variables of that population may also be involved in the process of malignant transformation, such as low CD4 count. The presence of HIV would also facilitate multiple infections and detection of genital HPV types in cutaneous lesions. Therefore, the alterations caused by HPV in prevalence of HIV infection can present a different behaviour from that observed in the general population, and should be the objective of further studies.
Objectives
General objective
The general objective was to investigate the frequency of HPV in verruca vulgaris, flat wart, EV, condyloma acuminatum, IN, bowenoid papulosis and squamous cell carcinoma in male HIV-seropositive patients.
Specific objectives
Analyse the frequency of premalignant and malignant lesions in the patients;
Determine the presence of HPV types 6, 11, 16 and 18 in the lesions;
Investigate if there is a relationship between malignancy of the lesion and presence of high-risk HPV;
Evaluate the association between lesion malignancy and the patient's age, date of first positive HIV test, lesion evolution time, HIV viral load, use of ARVT, high grade of immunodepression (CD4 ≤ 200 cells/mm3) and presence of HPV in the lesion.
Methodology
Study design
This is a cross-sectional, observational study of the male HIV-seropositive patients seen between March 2003 and August 2004 (18 months) at the Sector of Dermatology of the University Hospital of the Federal University of Rio de Janeiro (HUCFF/UFRJ).
Population studied
Criteria for inclusion in the study
Presence of verruca vulgaris, flat wart, EV, condyloma acuminatum, IN, bowenoid papulosis and/or squamous cell carcinoma;
HIV seropositivity;
Males;
Age ≥18 years.
There were no criteria for exclusion from the study.
Study procedures
The studied lesions were biopsied with scissors, scalpel or punch, under local anaesthesia with 2% lidocaine, without vasoconstrictor. A part of the collected material was preserved in formalin (for histopathological analysis) and another was stored and dried in a freezer at -20°C (for polymerase chain reaction [PCR] examination).
Variables collected in the questionnaire
Age, skin colour, marital status, education, profession, family income, place of birth, time of HIV disease, use of ARVT, time of ARVT use, types of antiretroviral medication used, previous diseases related to HIV, lesion evolution time and clinical diagnosis.
Histopathological examination
The following were considered as benign lesions: condyloma acuminatum, grade I IN, flat wart and verruca vulgaris; premalignant: EV, grades II and III IN and bowenoid papulosis and malignant: squamous cell carcinoma.
Detection and typification of HPV
The method used was PCR, comprising the following steps:
DNA extraction, for which samples were incubated in digestion buffer containing proteinase K following extraction by phenol-chloroform-isoamilic alcohol, DNA precipitation with sodium acetate and ethanol and verification of DNA presence; (2) PCR reaction, for which, in the first phase, regarding HPV detection, generic My09-My11 primers were used; 26 (3) Detection of PCR products (amplicons) on agarose gels and (4) HPV typification - HPV typing was performed using primers targeting DNA sequences of HPV 6 which presented an estimated molecular weight of 230 bp; for HPV 11, 89 bp; for HPV 16, 134 bp; for HPV 18, 119 bp; for HPV 31, 97 bp; for HPV 33, 132 bp and for HPV 35, 186 bp.
Statistical analysis
The EPIINFO 6.05 (Centers for Disease Control and Prevention, Atlanda, GA, USA) and SPSS 13.0 (SPSS Inc, Brazle) programs were used for data input and analysis. For description of the distribution of continuous variables, average values were used, with their respective reliability intervals; and for categorical variables, proportions were used.
HPV prevalence in the lesions as a whole and in the presence or not of malignity was estimated. The differences between the characteristics of the group with premalignant or malignant lesions and of the group with benign lesions were evaluated using the Mann-Whitney test for averages and χ 2 -test for proportions. An alpha value ≤5% was considered statistically significant.
The prevalence proportions and the respective reliability intervals were estimated by comparing the categories of the different variables with the classification of malignancy of the lesions.
Results
During the 18 months of the study, 129 HIV-positive men were seen and 38 muco-cutaneous lesions of 27 patients were biopsied.
Description of patients regarding their socioeconomic and cultural characteristics
The population studied presented as most frequent characteristics: age - between 31 and 50 years (63%), with an average of 39 years; skin colour - white; marital status - single, without companion; education - high school (51.8%); profession - retired; and family income - up to two minimum salaries.
Data related to the HIV disease
Date of first positive HIV test
The average was five-and-a-half years (varying from two months to 20 years), standard deviation of 71 months.
Use of ARVT
Of all patients 21 (77.8%) were on ARVT at the time of biopsy.
Data related to the lesions studied
Frequency of premalignant or malignant lesions
Frequency of premalignant or malignant lesions was 36.8% (14 lesions), with half of them presenting moderate or severe dysplasia (18.4% - CIN grade II or bowenoid papulosis). The descriptions of the lesions studied are listed in Table 1.
Studied lesions description: location and histopathology
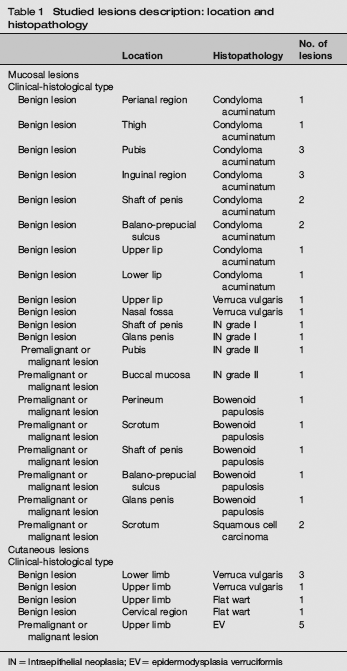
IN = Intraepithelial neoplasia; EV = epidermodysplasia verruciformis
Data related to HPV detection
HPV infection frequency
Virus frequency in the 38 lesions was 63.2% (24), with 70.8% (17) of the frequency in benign lesions and 50% (7) in premalignant or malignant lesions.
Data related to HPV typification
Of the 38 lesions studied, HPV types 6, 11 or 16 were found in 18 lesions (47.4%). HPV 16 frequency was 18.4% (7 lesions). Multi-infections (more than one type of HPV) occurred in three genital lesions histologically classified as condyloma acuminatam; being: types 11 and 16, types 6 and 16 and types 6 and 11. There was no detection of type 18. Types 31, 33 and 35 were also not detected in the samples that contained HPV of indeterminate type. The relationship between histopathological classification of the lesion and the type of detected HPV is shown in Table 2 and a detailed description of each patient is presented in Table 3.
Relationship between lesion malignancy and detected HPV type
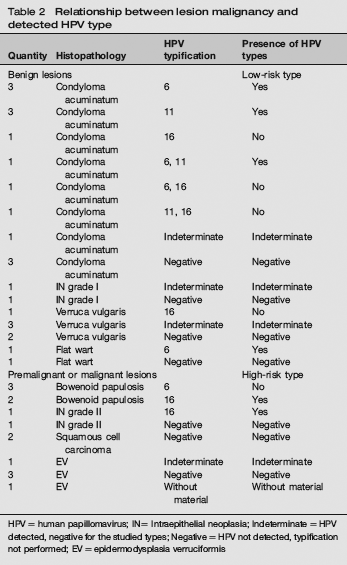
HPV = human papillomavirus; IN= Intraepithelial neoplasia; Indeterminate = HPV detected, negative for the studied types; Negative = HPV not detected, typification not performed; EV = epidermodysplasia verruciformis
General characteristics of patients – description of each patient's CD4 count, viral load, histopathological exam, HPV detection and typification
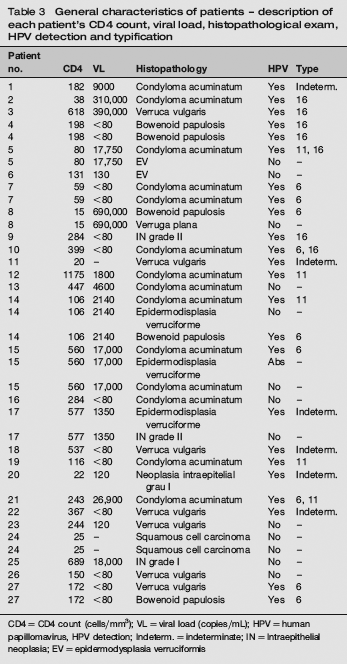
CD4 = CD4 count (cells/mm3); VL = viral load (copies/mL); HPV = human papillomavirus, HPV detection; Indeterm. = indeterminate; IN = Intraepithelial neoplasia; EV = epidermodysplasia verruciformis
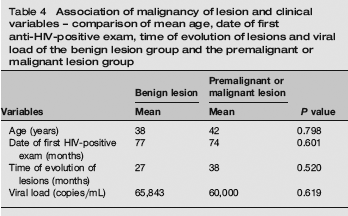
There was no statistically significant difference among the variable averages of the benign lesions group and premalignant or malignant lesions group (Table 4).
Association of malignancy of lesion and clinical variables – comparison of mean age, date of first anti-HIV-positive exam, time of evolution of lesions and viral load of the benign lesion group and the premalignant or malignant lesion group
The use of ARVT was related with increase of prevalence of premalignant or malignant lesions (Attributable Risk Prevalence [ARP] of 23.6%), however this result was not statistically significant.
In spite of not being significant, the CD4 count ≤200 cells/mm3 was associated with an increase of the prevalence of premalignant or malignant lesions (ARP of 45%).
Likewise, the detection of HPV in the lesion was associated with the decrease of prevalence of premalignant or malignant lesions (ARP of 41.7%) however this result was not statistically significant (Table 5).
Comparison of the number of patients using ARVT with CD4 count of ≤200 who had HPV detected in their lesions of the benign lesion group and the premalignant or malignant lesion group
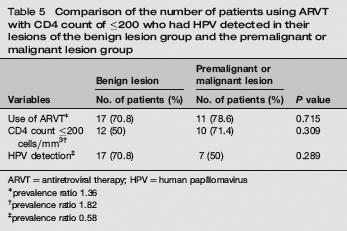
ARVT = antiretroviral therapy; HPV = human papillomavirus
prevalence ratio 1.36
prevalence ratio 1.82
prevalence ratio 0.58
Discussion
The immunodepression resulting from HIV-virus infection facilitates the oncogenic transformation caused by the HPV virus. The present study is justified by the association between these two viruses. Among the several types of HPV, it was opted to research types 6, 11, 16 and 18 as being more prevalent in genital lesions. The negative cases were also tested for types 31, 33 and 35, being types of high risk for malignant transformation, also prevalent in genital lesions. It was decided to include lesions of any location because the study will serve as the basis for future projects.
The absence of statistical correlation between the analysed variables may be explained by the homogeneity of the population studied and reduced number of samples.
Gomousa-Michael et al., 8 in 2000, evaluated HPV genital infection and IN in 70 men infected by HIV and found moderate or severe dysplasia in 33.3% of the HIV-positive patients, compared with 5% of HIV-negative patients. The study carried out by Aynaud, in 1998, 16 compared anogenital lesions caused by HPV in HIV-seropositive and -seronegative men and found high-degree dysplasia in 29.3% of the lesions of HIV-positive patients and 5% in HIV-negative patients. In the present study, the frequency of moderate or severe dysplasia (grade II IN or bowenoid papulosis) was 18.4%, being higher than in the HIV-negative-patient populations mentioned above. This corroborates the hypothesis that malignant transformation occurs more frequently in immunodepressed patients.
Another extremely relevant discovery in the study was the diagnosis of EV in five cutaneous lesions that clinically presented as flat warts, located in photo-exposed areas. Lesions resembling EV in HIV-positive patients have been increasingly frequently described. It is questioned whether this is the classic EV in genetically predisposed HIV-positive patients, or a new clinical entity, with less aggressive behaviour in those patients. 27 29
The lack of HPV detection in 36.8% of the samples may be justified by the pair of oligonucleotides used. In 1998, Surentheran et al. 30 studied three pairs of degenerate oligonucleotides and verified that the My09/11 pair was the most sensitive for mucosal types, but was only capable to detect cutaneous types in the presence of a high number of copies. Other causes could be the low number of DNA copies in the sample (old lesions, lesion periphery), lack of positive cells in small biopsies, presence of a new type of still not identified HPV, absence of HPV in the sample and excess of keratinization of the material, hindering DNA extraction (as occurred in one of the samples studied).
Gomousa-Michael et al. 8 in 2000 also found a high prevalence of high-risk HPV (16/18, 31/33/35) in the HIV-positive patients (50%), compared with HIV-negative patients (5%). Aynaud, 17 in 1998, found 35% of high-risk HPV in anogenital lesions of HIV-positive patients and 12% in lesions of HIV-negative patients. In the present investigation, the rate of high-risk HPV detection (type 16) was low (18.4%), being found only in seven lesions, without types 18, 31, 33 and 35 having been detected. Detection of type 18 would not be expected, since its prevalence in the general population is low (around 15%). It seems that the population of Rio de Janeiro presents a low incidence of infection by HPV 31, if compared with other states. An investigation accomplished in Niterói, Brazil, with 25 positive samples of cervical smears for HPV did not find any positive HPV 31 samples. 31
Multi-infection was present in three cases of condyloma acuminatum. There was no relation between multi-infection, severity of the lesion, CD4 count and viral load. Finding multi-infection has important social repercussions, suggesting that several types of HPV are being transmitted among the sexually active population. We should also not forget the presence of a sexually transmitted disease (STD) that can facilitate the acquisition of other STDs, including HIV.
The finding of high-risk HPV, as HPV 16 that occurred in four benign lesions, should always indicate accomplishment of a more regular follow-up of the patient for precocious detection of malignant transformation.
The presence of HPV 6 in a lesion of bowenoid papulosis, three cases in the present casuistry, is infrequent, with few cases described in literature.32,33 The most common association is with HPV 16 and there are cases described with types 18, 31-34, 39, 42, 48, 51-54. 34 It should also be remembered that the low-risk HPV classification does not exclude involvement with malignant transformation. 11
There was no detection of HPV in six premalignant or malignant lesions, as already observed in other studies.7,35,36 For the malignant transformation to occur, the DNA of HPV becomes integrated to cellular DNA, causing genomic instability. During the integration, a rupture of a sequence of the L1 gene may occur, reducing the sensibility of the MY09/11 primer. 7
In cases of verruca vulgaris in oral mucosa, the types of HPV commonly found are 2, 4, 6, 11 and 57. 37 Finding HPV 16 in those cases is rare, and it occurred in a lesion located in the upper lip. Such fact could be justified by acquisition through the orogenital sexual contact.
The case of flat wart where HPV 6 was detected presented bowenoid papulosis lesion on the penis, where the same type of HPV was detected, which could justify the finding of a genital type in the cutaneous lesion through autocontamination. There are several reports in the literature of detection of HPV genital types in cutaneous lesions, especially in immunodepressed patients. 38 40 In clinical lesions similar to EV in HIV-seropositive patients, types 3, 5, 8, 10 and 20 have been found, all being EV-related types. 27 In most of the EV cases studied, there was no HPV detection, as expected, since specific primers were not used for EV-related types, but generic primer with low sensibility for cutaneous lesions.
Publications relating viral load and HPV are conflicting.18,41 In the present investigation, there was no difference between viral loads of the group with benign lesion and the group with premalignant or malignant lesion.
So far, highly active ARVT does not seem to be involved in improvement of the natural evolution of the diseases associated with HPV. 9 Most of the studies did not demonstrate its impact in the regression of the pre-neoplasic lesions, being the immune-system improvement insufficient to protect against HPV.21,24 It was also suggested that persistence of HPV and increase of the patients’ survival would act together, facilitating the progression to neoplasia.24,42 Another important factor in the beginning of ARVT is the syndrome of immunological reconstruction that can cause clinical worsening of infectious lesions, contributing to the progression of the disease. In the present study, the use of ARVT points to an increase of prevalence of premalignant or malignant lesions, suggesting that the increase of the survival would supply the time necessary for malignant transformation.
About the counting of CD4 T-cells in two studies, a low level of CD4 was a risk factor for anal cancer development.13,14,41 In the present investigation, the CD4 ≤200 cells/mm3 seems to be related to an increase of the prevalence of premalignant or malignant lesions, suggesting, likewise as found in literature, that the decrease of immunity would increase the prevalence of malignancy.
Conclusion
Our study showed that patient's age, date of first positive HIV test, lesions evolution time, HIV viral load, use of ARVT, high degree of immunodepression (CD4 ≤200 cells/mm3) and presence of HPV in the lesion have no relationship with increase of prevalence of premalignant or malignant lesions.
HPV had high prevalence with low HPV 16 rate and no HPV 18. Premalignant or malignant lesions were detected in less than 40%, and the frequency of moderate or severe dysplasia in the patients studied was higher than described in the seronegative HIV population. High-risk HPV (HPV 16) was also detected in benign lesions and low-risk HPV (HPV 6) in premalignant genital lesions, showing that in HIV patients low-risk HPV infection can also be associated to cancer progression.
Footnotes
Acknowledgements
The study was supported by the FAPERS-Fundafã Carlos Chagas Filho de Ampara à Pesquisa do Estado do Rio de Janeiro, Brazil; Sector of Dermatology and Post-Graduation Course, HUCFF-UFRJ and School of Medicine, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil; and the Sector of Virology Department of Microbiology and Parasitology, Universidade Federal Fluminense, Niterói, Brazil.