
Abstract
Cisgender men (CM) who report transgender women (TW) as sexual partners are an understudied population in the HIV epidemic in Latin America. The current study sought to characterize this group in a 2012 cross-sectional online survey of Latin American CM who were members of a sexual networking website for men who have sex with men (N = 11,847). Multivariable logistic regression models were fit to estimate demographic, behavioral, and psychosocial correlates of having a TW sexual partner and engaging in condomless sex. Overall, 0.9% (n = 106) reported a TW sexual partner in the last 12 months; of these, 76.4% (n = 81) reported condomless sex in the last three months. Identifying as bisexual or heterosexual compared to gay, and specifying a versatile sexual role preference compared to insertive were associated with reporting a recent TW sex partner (all p < 0.05). HIV-negative serostatus, lifetime STI history, and alcohol dependence were associated with recent condomless sex (all p < 0.05). CM with TW sexual partners have distinct HIV-related vulnerabilities. Future research is needed to understand CM who report TW sexual partners, including their sexual preferences and practices, sexual networks, exposure to stigma, biomedical prevention interest and uptake, and acceptability of integrating alcohol abuse screening into sexual health services.
Introduction
Cisgender men (CM) (whose gender identity is congruent with their sex assigned at birth) who have sex with transgender women (TW) (individuals assigned a male sex at birth who identify as women, female, trans women, male-to-female, travesti, or another diverse trans feminine gender identity or expression) are at risk of HIV acquisition and transmission. This is due to the concentration of the HIV epidemic globally in TW populations. 1 For example, in Peru HIV prevalence estimates have been shown to be as high as 33% among TW.2,3 One survey in Peru found that nearly one-third of TW (30% out of 142) reported condomless anal sex with their last male partner, and the majority (78%) of cases reported that their male partner’s HIV status was unknown. 4 CM who have sex with TW may contribute to general population HIV epidemics through varied sexual partnerships, including with cisgender women, CM, and TW.5,6 With few exceptions,4,6 little research has attended to the social and behavioral correlates of sexual behavior risk among CM who have sex with TW.
Multilevel structural, interpersonal, individual, and biological determinants shape HIV risk and resiliency for TW, 7 but biological risk for HIV infection is primarily attributed to condomless sex. 3 Studies suggest that TW most frequently engage in sexual behaviors that may confer risk for HIV infection with CM.8–11 Prior research suggests that men who have sex with TW are heterogeneous in sexual orientation identities, sexual behaviors, sexual roles, and masculine gender role conformity.9,12–14 Additional research is needed to characterize this group, including identifying subgroups at highest risk of HIV acquisition or transmission, potential psychosocial vulnerabilities such as depression and alcohol use,4,15,16 and awareness and acceptability of biomedical HIV prevention technologies, such as pre-exposure prophylaxis (PrEP) and home HIV testing, all of which have implications for design and implementation of sexual health interventions.17,18
The Internet has proven to be an important way of reaching difficult-to-sample populations, such as men who have sex with men (MSM). 19 Addressing the potential challenges in conducting research with these populations, internet and online dating applications have continued to play an increasing role in facilitating sexual partnerships and ‘hook-ups’ for MSM, with over six million active users globally. 20 These sites provide an opportunity to recruit members of a group potentially at high risk for HIV acquisition or transmission with relative ease where conventional methods may not be feasible. Especially relevant to Latin America, emerging literature provides support for the use of online surveying as a low-cost and novel method to access often stigmatized members of a study population at high risk for HIV.21–23
The purpose of this article is to (1) describe the demographic, behavioral, and psychosocial characteristics of Latin American CM seeking sex online who report TW as sexual partners, and assess HIV biobehavioral prevention awareness and acceptability in this group, to identify a potentially key population in need of prevention services; (2) characterize the behavioral profiles of those men with a TW sex partner who report condomless sex to identify individuals at highest risk of acquiring or transmitting HIV infection to guide future intervention efforts.
Method
Study design, participants, and procedures
A secondary analysis was conducted of data from an anonymous online survey of members of a sexual networking site for MSM in 2012, who reported currently living in Latin America, and who were CM as determined by the two-step method 24 (i.e. they reported a current male gender identity and a male assigned sex at birth). To recruit participants, an email message was sent to all current users that had indicated their residence was in Latin America and ages 18 years or older. Individuals agreeing to participate first completed consent form and then study questionnaire, which took approximately 30 min to complete (64% response rate). Study procedures have been described in detail elsewhere. 24 All study procedures were approved by the Fenway Health IRB.
Measures
Five broad domains were assessed. (1) Demographics: Country (All Latin American Countries excluding Honduras, Panama, and Paraguay because no TW partners were reported), age (continuous in years), socioeconomic status assessed as income (no income, low income, middle income, high income), educational attainment (university or above versus less than university). (2) Sexual orientation, preferred sexual role, and masculine gender conformity: Participants were asked their sexual orientation identity (gay/homosexual, bisexual, heterosexual, unsure/questioning) and preferred sexual role (top, bottom, versatile). A two-item scale assessed socially-assigned gender conformity 25 by asking participants to rate their ‘appearance, style, or dress’ and ‘mannerisms (such as the way they walk or talk)’ on a scale ranging from 1 = very feminine to 7 = very masculine. The two items were highly correlated (r = 0.79) and loaded onto a single factor (eigenvalue = 1.65; % variance explained = 82.7). The two items were summed so that higher scores reflected higher socially-assigned masculine gender conformity. (3) HIV infection, sexually transmitted infection (STI) history, and condomless sex: Participants self-reported their HIV serostatus, lifetime history of STI, and whether they had engaged in condomless anal or vaginal sex with a partner of any gender (male, female, transgender) in the last three months. (4) Psychosocial vulnerabilities: Current alcohol dependence as assessed via the 4-item validated CAGE scale (a score of 2 or greater is suggestive of hazardous alcohol use).26,27 Depressive symptoms were assessed using the CES-D 10-item measure and were scored on a 4-point Likert scale from 0 to 3, with a score of 10 or greater suggestive of clinical depression. 28 (5) Awareness and acceptability of HIV biobehavioral prevention and HIV home testing: Awareness of PrEP was assessed by asking, ‘Have you ever heard of HIV-negative people taking HIV medicines before sex because they thought it would reduce their chances of getting HIV infection (also known as PrEP)?’ Acceptability of HIV home testing was asked via ‘If a home test for HIV was available, would you use it?’
Data analysis
Statistical analyses sought to (1) examine the proportion of CM who reported recent sexual contact with a TW in the last 12 months and compare those men reporting a TW sex partner to those who did not (outcome 1: transgender partner in last 12 months yes/no); (2) estimate the proportion of men with a TW sex partner who reported condomless sex in the last three months (outcome 2: condomless anal or vaginal sex with a partner of any gender in the last three months – male, female, transgender yes/no). Variables considered in multivariable models were selected a priori based on a review of the literature. A complete case analysis was conducted. Logistic regression models were fit with variances clustered on country of residence. Final multivariable model fit was implemented by finding the model with the lowest Akaike information criterion using a backwards stepwise algorithm. 29
Results
Comparing men with and without TW sex partner(s) – Table 1
Overall, 0.9% (n = 106) of the sample reported sex with a TW in the last 12 months. Table 1 presents comparisons of men with a transgender sex partner to those who did not report having a transgender sex partner. Statistically significant correlates of reporting a transgender sex partner in a multivariable model were older age (adjusted odds ratio [aOR]=1.03; 95% confidence interval [CI]: 1.01–1.04; p < 0.001), identifying as bisexual (aOR = 9.66; 95% CI: 5.76–16.21; p < 0.001) or heterosexual (aOR = 18.52; 95% CI:3.67–93.38; p < 0.001) compared to gay/homosexual, versatile sexual role preference (aOR = 1.87; 95% CI: 1.13–3.10; p = 0.02) compared to top (insertive) role, increased awareness of PrEP (aOR = 2.04; 95% CI: 1.51–2.77; p < 0.001), and decreased acceptability of HIV home testing as a prevention strategy (aOR = 0.59; 95%CI: 0.38–0.91; p = 0.02). High socially-assigned masculine gender nonconformity was significant in bivariate analyses (aOR = 2.19; 95% CI: 1.44–3.33; p < 0.001), but not statistically significant in multivariable models. Self-reported prevalence of HIV infection, STI history, and condomless sex were not statistically significant comparing men with a transgender sex partner and those without. There were also no significant differences in psychosocial characteristics (e.g. alcohol dependence and depression).
Factors associated with Latin American cisgender males who report transgender sexual partners in the last 12 months (N = 11,847).
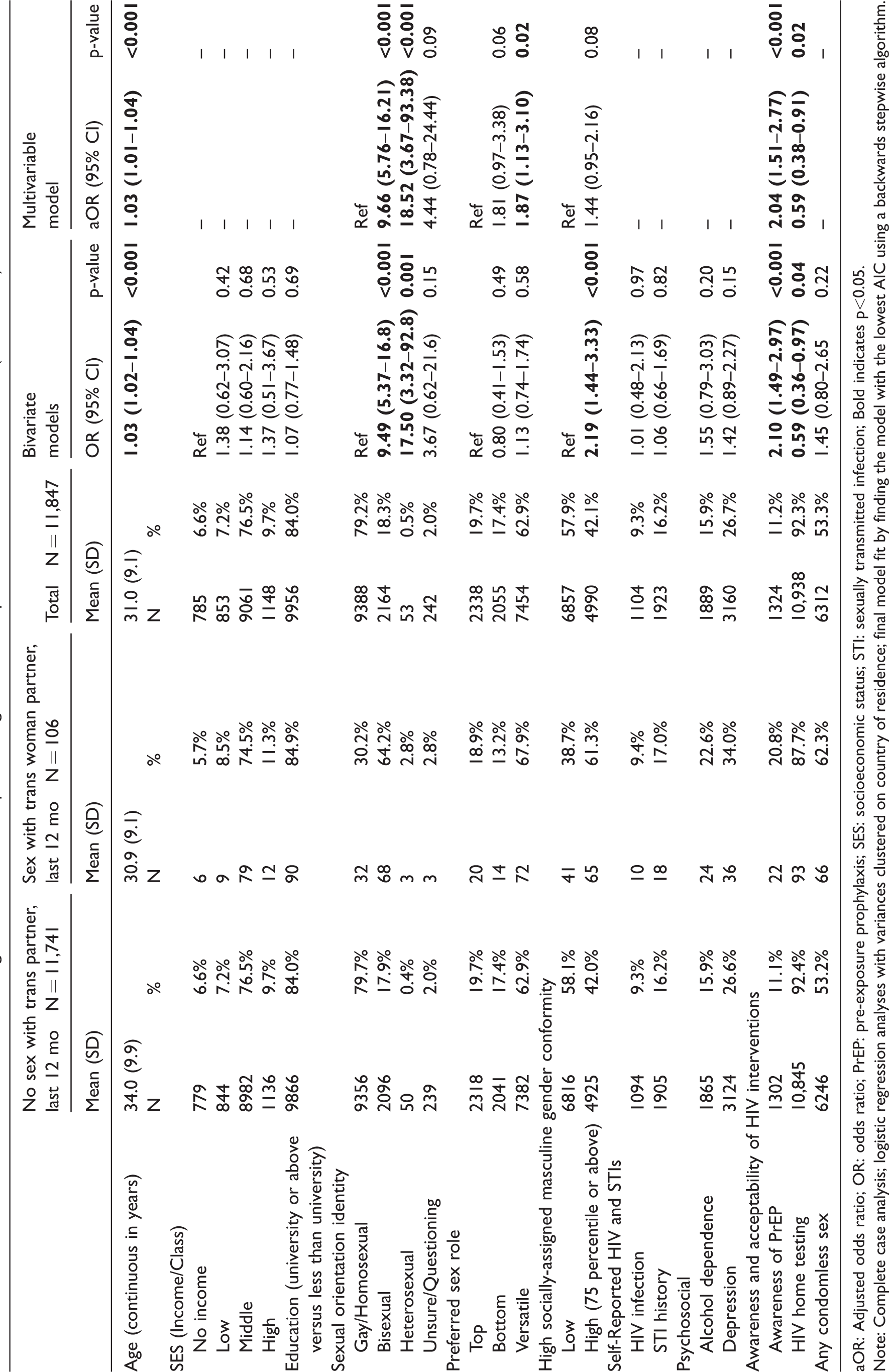
aOR: Adjusted odds ratio; OR: odds ratio; PrEP: pre-exposure prophylaxis; SES: socioeconomic status; STI: sexually transmitted infection; Bold indicates p<0.05.
Note: Complete case analysis; logistic regression analyses with variances clustered on country of residence; final model fit by finding the model with the lowest AIC using a backwards stepwise algorithm.
Men with a TW sex partner who reported condomless sex versus those who did not – Table 2
Among men reporting sex with a TW in the last 12 months, 76.4% (n = 81) reported condomless sex in that past three months. Statistically significant correlates of engaging in condomless sex are shown in Table 2. Being older in age (aOR = 1.06; 95% CI: 1.01–1.11; p = 0.02), identifying as bisexual versus gay/homosexual (aOR = 0.48; 95% CI: 0.23–0.99; p = 0.05), self-reporting as HIV-uninfected (aOR = 0.17; 95% CI: 0.06–0.48; p < 0.001), self-reporting a lifetime STI history (aOR = 2.38; 95% CI: 1.11–5.12; p = 0.03), and meeting criteria for current alcohol dependence (aOR = 3.82; 95% CI: 1.23–11.88; p = 0.02) were each independently associated with an increased odds of engaging in condomless sex.
Factors associated with condomless sex with transgender partners in the last three months among cisgender males who report transgender partners (N = 81).
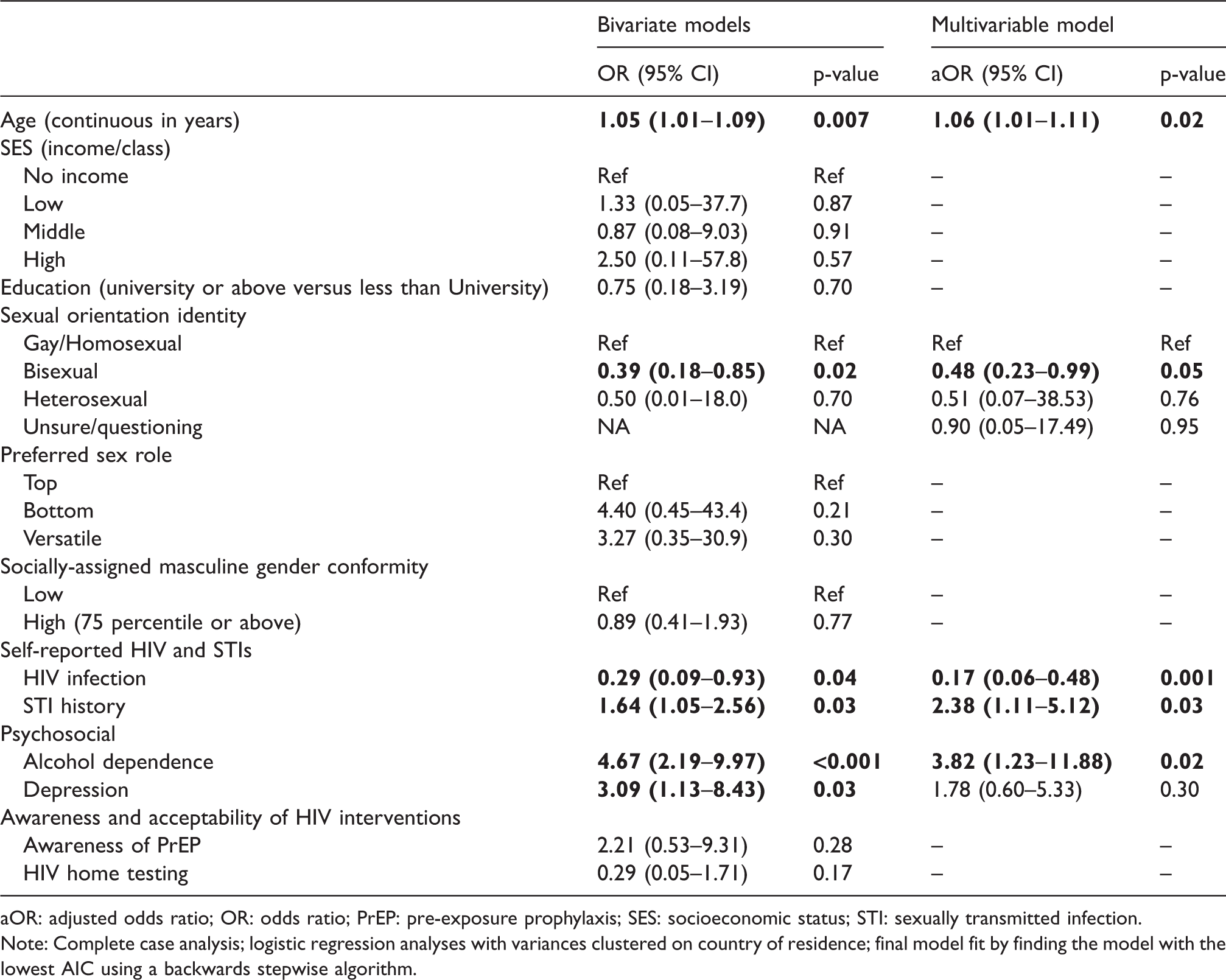
aOR: adjusted odds ratio; OR: odds ratio; PrEP: pre-exposure prophylaxis; SES: socioeconomic status; STI: sexually transmitted infection.
Note: Complete case analysis; logistic regression analyses with variances clustered on country of residence; final model fit by finding the model with the lowest AIC using a backwards stepwise algorithm.
Discussion
Although the proportion of this online sample of CM in Latin America seeking sex online who report sex with TW is small (nearly 1%), our results show that over three-quarters of these men reported condomless sex. Cisgender MSM and TW are distinct key populations at risk of HIV acquisition and transmission due to the concentration of the HIV epidemic globally. 23 It is important to consider the potential for concentrated and interrelated microepidemics among these groups. Findings highlight that primary HIV prevention efforts are needed for this group. Additional epidemiological research is recommended.
Latin American men reporting a transgender sex partner were more likely to be older in age, identify as bisexual or heterosexual rather than gay/homosexual, consistent with previous research. 12 They were also more likely to prefer a versatile (i.e. moderno) sexual role compared to a top (i.e. activo) sexual role, a finding which may have implications for HIV transmission risk. The high probability of HIV transmission through receptive anal intercourse has been shown to have a central role in explaining the HIV epidemic in MSM globally. 30 If men endorsing a versatile sexual role preference are more likely to engage in sex with TW than those with a top sexual role preference, then TW with male partners may have an elevated risk of HIV transmission since these men are already at a higher risk of contracting HIV given their sexual role preferences. 31 Meanwhile, if HIV prevalence is high among TW and if viral suppression rates are low, then bisexual or heterosexual men may be at risk of HIV acquisition given the relatively small TW partnership pool. Further research is needed, including collection of event-level data about sexual partnerships and episodes, to examine HIV transmission risk among men who have sex with TW, and their sexual partners. In particular, more nuanced data will allow examination as to whether any increased transmission risk may be due to bisexual and heterosexual men being more likely to be the receptive sex partner when having sex with a TW. Event-level data will also enable elucidation of sexual position preferences compared to enacted behaviors, potential seroadaptive positioning, and other risk reduction practices.
In this study population of men seeking sex online via a MSM website in Latin America who report sex with TW, having a history of one or more STIs and self-reporting as HIV uninfected were associated with condomless sex. Although data on current STIs were not available for this analysis, lifetime STI acquisition was associated with condomless sex. Previous research has shown that lifetime STI history is associated with increased probability of a currently active STI. 32 Currently active STIs can make HIV transmission more efficient and are a risk factor for HIV acquisition. 33 Future research is needed to assess currently active STIs among CM with transgender partners. Unlike STI history which was linked to condomless sex in this study, self-reporting as HIV uninfected was linked to not engaging in condomless sex. It is possible that CM with transgender partners are aware of the potential risks and change their behavior to avoid HIV acquisition. It may also be that TW, a priority population for HIV intervention globally, have agency and are responsive to prevention efforts. Additional mixed-methods research is needed on this topic to inform tailored HIV and STI prevention, testing, and treatment services for this population, including those which engage both TW and CM who have sex with TW.
Men reporting a transgender sex partner were more likely to be aware of PrEP than men without a transgender sex partner; however, they were also less likely to endorse HIV home testing as an acceptable prevention intervention relative to men who did not report a transgender sex partner. These differences in intervention acceptability indicate that additional efforts are needed to understand the HIV prevention and testing needs of this population. More research is warranted to understand perceived acceptability of PrEP as a prevention method, as well as to investigate actual access to and uptake of PrEP in Latin America. Gathering data on perceived barriers to home testing for HIV infection will also be important to inform future interventions for men who have TW sex partners, particularly those seeking to reach individuals in online contexts. 17
Meeting criteria for alcohol dependence was significantly associated with condomless sex among men who reported TW sex partners. Although data on concurrency between alcohol use and sexual risk behavior remain inconsistent, 34 heavy alcohol consumption 35 has been consistently associated with condomless sexual behaviors16,34 and suboptimal adherence to antiretroviral therapy.36,37 Further, a nationwide biobehavioral surveillance study in Peru found that 63% of MSM and TW met criteria for having an alcohol use disorder. 38 Taken together, these findings suggest that integrating alcohol screening along with in-depth HIV and STI counseling, testing, and treatment services that are more mindful of alcohol abuse may increase responsiveness of sexual health services for these men. 39 The current study cannot rule out potential confounding due to other variables not included in this analysis (e.g. mental health distress) which might contribute both to increased alcohol dependence and HIV risk.
Findings should be interpreted in the context of several limitations. Regions of Latin America where internet access is limited may be underrepresented in this online sample. Further, given this is an online sample recruited via a MSM website, it is not representative of all CM who report a TW sex partner. In particular, CM who would not be comfortable accessing a sex-seeking website tailored to MSM will not be captured in this study. The sample size of this study represents an important limitation; research is needed to enroll larger samples. Data were self-reported by participants and may be subject to bias, including social desirability bias. Specifically, with regard to reporting a TW sexual partner and HIV serostatus, participants may potentially underreport partnerships and/or diagnoses due to stigma. Reported knowledge of PrEP and HIV testing may not be indicative of overall knowledge when such resources do not exist in a region. These data were also collected before PrEP was commonly discussed as a prevention option and HIV home testing was widely available. Condomless sex is reported in aggregate in the last three months without information about partner gender or type, insertive or receptive sex, and/or other sero-positioning or sero-adaptive behaviors related to HIV serostatus. Despite limitations, information from this study of self-reported sexual risk behavior among men who have sex with TW highlights directions for future research, including the need for social network studies to engage this population and to understand the sociocultural contexts that drive HIV risk for this group.
Conclusions
Our findings highlight that men seeking sex online via an MSM website should not be conflated in one uniform category; rather, there is a continuum and heterogeneity between heterosexuality and homosexuality in terms of sexual identities, sexual practices, and gender of sexual partners. Future efforts should focus on understanding the psychosocial and behavioral epidemiology of HIV risk among men who have sex with TW in Latin America (e.g. sexual role preference, alcohol dependence) in order to develop and ensure availability of targeted, relevant, and maximally responsive HIV prevention, testing, and treatment interventions for this high risk, largely occult, and highly stigmatized subpopulation.9,10 Given previous research that CM who have sex with TW are exposed to stigma, marginalization, and exclusion specifically due to being in a sexual partnership with a TW,40,41 future research would benefit from examining the potential role of stigma in HIV risk behaviors and in uptake of biobehavioral prevention methods for this population. Gathering dyadic data from CM-TW partnerships may offer additional insights about the potential for concentrated HIV microepidemics in these key populations and elucidate the social inequities driving them.
Footnotes
Author’s contributions
SLR: Conceptualized the research and analyses, interpreted results, and finalized the manuscript.
AP-B: Conducted literature review, interpreted findings, contributed to the discussion, manuscript review.
CEO: Conducted data analyses and manuscript review.
KEG: Contribute to the literature review, discussion, and manuscript review.
JM: Conducted literature review, managed references, and manuscript review.
KL: Conducted literature review, managed references, and manuscript review.
MJM: Data collection, interpretation, and manuscript review.
JGR: Data collection, interpretation, and manuscript review.
KB: Data collection, interpretation, and manuscript review.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This publication was made possible with help from: (1) the Harvard University Center for AIDS Research (CFAR), an NIH funded program (P30 A1060354) which is supported by the following NIH Co-Funding and Participating Institutes and Centers: NIAID, NCI, NICHD, NHLBI, NIDA, NIMH, NIA, FIC, and OAR; (2) HU CFAR developmental grant awarded to Dr Sari Reisner (CFAR-FCHC-15–1); (3) the Harvard Global Health Institute (HGHI); (4) the National Institute of Mental Health (NIMH) of the National Institutes of Health under award number R34MH104072 (MPI: Clark, Mimiaga, Reisner). APB is supported by a National Institute of Child Health & Human Development T32 grant (T32HD049339; PI: Nathanson). The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.