
Abstract
Summary
Treatment for human papillomavirus (HPV)-associated anal canal disease has been unsatisfactory. The objective of our study was to determine the treatment outcome in our cohort with anal HPV disease. Overall, 181 patients were evaluated over a median period of 19.1 months (range = 2.8–125.5). Eighty-eight patients (48.6%) with high-grade anal intraepithelial neoplasia (AIN) and 82 patients (45.3%) with low-grade AIN underwent treatment. One hundred and forty-one patients (77.9%) received laser ablative treatment as an outpatient procedure. The treatment yielded cure, defined as a disease-free state at 12 months after treatment, in 63.0% (114/181). Median time to cure for the cohort was 31.5 months (95% confidence interval: 23.0–40.0). Treatment outcome showed no evidence of being affected by age, sexual preference, history of smoking or presence of high-grade disease. Median time to cure was significantly affected by a positive HIV status (P = 0.02) and the extent (volume) of the disease (P = 0.01). Contrary to the current view that treatment of HPV-related anal disease is difficult, unrewarding due to recurrences and may lead to substantial morbidity, we demonstrate that effective treatment is possible for both low- and high-grade AIN. These findings should help with the general desire to introduce screening for AIN for at-risk groups.
INTRODUCTION
Epidemiological studies have noted an increase in the incidence of anal cancer during 1943–1987 and 1940–1989 in Denmark and the USA, respectively. 1,2 More recently, a global increase in anal cancer in men in California has been demonstrated. 3 In London, an increasing incidence in anal cancer has been identified in those attending a large HIV unit. 4 Anal squamous carcinoma is associated with the presence of high-risk human papillomavirus (HPV). 5,6 The risk factors for anal HPV infection, anal intraepithelial neoplasia (AIN) and anal squamous carcinoma are similar. 7–11 In addition to a number of risk factors such as receptive anal intercourse, anogenital warts has been identified as a risk factor for anal cancer. 10,11 In a study looking at the incidence of AIN in patients with anal condylomata, subclinical AIN was found in 51% of HIV-positive men and 17% of HIV-negative men. 12 A recent study that followed up patients with anal condylomata showed that anal cancer developed in some cases after a median follow-up of 23 months. 13
Our high-resolution anoscopy (HRA) clinic was set-up in 1996 to provide clinical care for an increasing number of people identified by local physicians in their HIV or sexual health clinics. Currently, it provides a referral service for the north-east sector of London. We set out to treat all grades of anal HPV disease in our HRA clinic, as patients and their physicians clamoured for treatment. A retrospective analysis of all cases treated during the period January 1996–December 2006 was undertaken. There are no substantial studies looking at the treatment outcome of all grades of anal HPV disease in the published literature. Recently, Goldstone et al., 14 looking at treatment of 68 patients with high-grade disease, found a satisfactory outcome in their cohort. However, they considered that further treatment studies were needed of those with low- and high-grade disease and with a longer duration of follow-up. We believe that our data fill this gap in the literature.
METHODS
All patients were referred by medical practitioners who had suspected or identified anal canal disease. Some patients had their AIN diagnosed through their prior anorectal surgery and were referred for further management. Patients were examined in the lithotomy position, using a microscope (colposcope). A metal proctoscope was introduced with minimal lubrication. At 6 cm into the anal canal, a 5% acetic acid moistened cotton ball was applied to all of the mucosa. After visualization, the proctoscope was gradually withdrawn and the process repeated until the anal verge and the perianal skin had been examined. The proctoscope was reintroduced, and under local anaesthesia, biopsies were obtained using Eppendorf biopsy forceps. Several biopsies were taken if the disease involved more than one quadrant of the epithelial surface. A ferric subsulphate solution was applied for haemostasis.
During the treatment visit, patients were re-examined as above, and local anaesthesia was injected submucosally to all of the lesions. Using a diode laser delivered through a fibre secured through a handpiece, laser ablative treatment was performed. The handpiece had dual channels, with the second channel being connected to a suction unit, for smoke evacuation. All personnel, including the patient, wore eye protection and masks were worn by the operator and assistant. The duration of treatment varied from 10 to 90 minutes depending on the amount of disease (volume). Patients were given oral analgesics, topical anaesthesia and lactulose, in every case. If the extent of treatment was three or four quadrants, they were also prescribed antibiotics. All patients received treatment as outpatients. Generally, patients were reviewed after six months (5–7 months) and if any recurrent disease was found, further treatment was offered. Some patients had either excision or topical application of 5% imiquimod as treatment. Generally, these patients had low volume disease (one quadrant) or had expressed a preference for topical treatment. All patients were reviewed annually, if free of disease.
The gold standard for diagnosis was biopsy histology. All biopsies taken were retrospectively reviewed by NS, an experienced histocytopathologist.
A database of all attendees of the HRA service is maintained. Using this database, we identified all patients who had attended for treatment and received at least one follow-up visit. The data was analysed using SPSS V 14.0 (SPSS Inc. Chicago, IL, USA) and confidence interval analysis. Analysis of survival times was undertaken using the Kaplan–Meier method. This takes account of the censoring in the data and allows times for the patients who have not been followed to cure to be accounted for in the analysis.
RESULTS
Of a total of 254 patient entries on the database, we identified 181 complete records (71.2%). Thirty-one patients (12.2%) did not have any disease. Twenty-three (9.0%) were lost for follow-up after their treatment. Seventeen (6.7%) did not complete their treatment and two (0.8%) did not have HRA examination findings recorded. Baseline characteristics are given in Table 1. Overall, 181 patients were evaluated over a median period of 19.1 months (range = 2.8–125.5, interquartile range = 10.3–37.5). Patients predominantly consisted of men who have sex with men (MSM) of white ethnicity (59.7%, 108/181). Eighty-four patients (46.4%) were known to be HIV-positive. Others were either negative (42.5%) or of unknown status (11.0%). Of the 84 HIV-positive patients, 35 (41.7%) had a CD4 count of 400 or above at the time of treatment, while 26 had a CD4 count between 200 and 400 (31.0%). Only 13 patients (15.5%) had a CD4 count of less than 200 at the start of treatment. Fifty-one HIV-positive patients (60.7%) were on antiretroviral medication at the start of treatment. Ninety-three (51.4%) had high-volume disease involving three or four quadrants of the epithelial surfaces. Of 176 cases (96.7%) with histology, 88 (48.6%) had high-grade disease (AIN2 or AIN3).
Base line patient characteristics
ARVT = antiretroviral therapy; AIN = anal intraepithelial neoplasia; HPV = human papillomavirus; Bx = biopsy
One hundred and forty-one patients (77.9%) had laser ablative treatment. Treatment yielded cure, defined as a disease-free state at 12 months after treatment, in 63.0% (114/181). Figure 1 shows the treatment outcome for the whole group. Median time to cure for the whole cohort was 31.5 months (95% confidence interval [CI]: 23.0–40.0). Table 2 shows median time to cure by patient and treatment characteristics and the results of the log rank test. Using Cox regression analysis, there was no evidence of an effect of age on time to cure (hazard ratio = 1.00 [95 CI: 0.98–1.03] per year of age). Median time to cure shows no evidence of being affected by ethnicity, sexual preference, history of smoking, current smoking and presence of high-grade disease. However, median time to cure was significantly affected by positive HIV status (P = 0.02) and the extent (volume) of disease (P = 0.01). A number of treatment combinations occurred in the course of treatment. The numbers in each group were too small for analysis to determine the best treatment option.
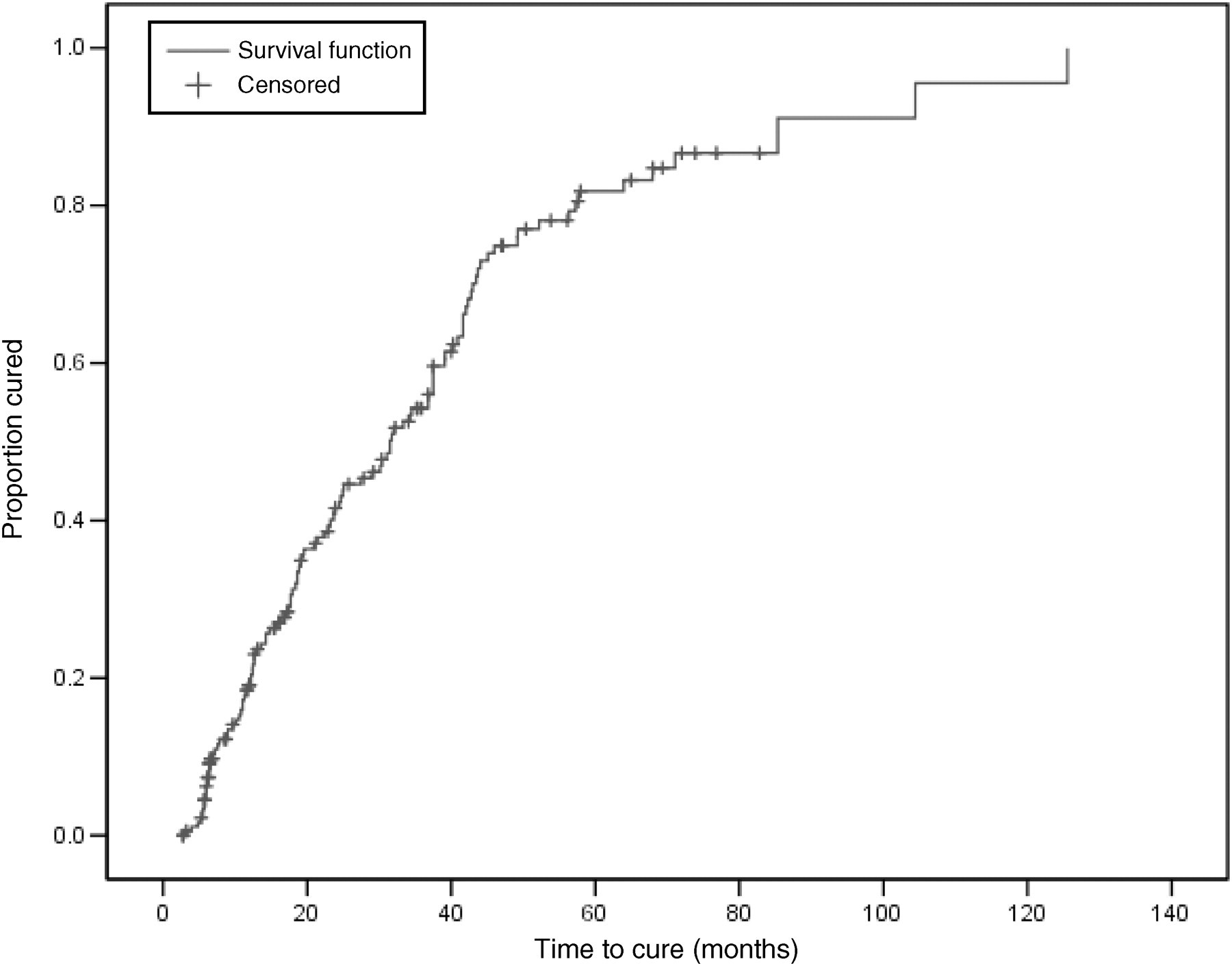
Kaplan-Meier plot showing treatment outcome for the whole group
Median time to cure by patient and treatment characteristics
AIN = anal intraepithelial neoplasia; HPV = human papillomavirus; CI = confidence interval; LR = log rank; Bx = biopsy
Anal cytology was performed during follow-up after treatment. Of 88 smears, 46 were obtained from those who were free of disease on examination, while 42 were from those showing signs of disease. Of the 46 with no disease, 40 smears (86.9%) were negative. The other six smears showed mild dyskaryosis (four) or borderline or HPV changes. Of the 42 smears from patients with disease, 27 (64.3%) showed some abnormality. Sixteen smears showed dyskaryosis, 11 showed minor abnormalities. The kappa value for agreement between HRA findings and anal cytology was 0.60 (95% CI: 0.38–0.81) based on 61 patients.
DISCUSSION
It appears that the presence of high-risk HPV in the anal canal leads on to the development of AIN lesions in high-risk groups such as HIV-positive MSM. A proportion of patients with AIN go on to develop anal squamous carcinoma. There are a number of studies that lends support to this view. Palefsky et al. 15 demonstrated that within two years, 20% of HIV-positive men and 8% of HIV-negative men in a cohort of 346 HIV-positive and 262 HIV-negative homosexual or bisexual men, respectively, developed incident high-grade squamous intraepithelial neoplasia. Recently, two studies of longer-term follow-up of cohorts with high-grade AIN demonstrated the development of anal squamous carcinoma in some cases. In the English study, where 35 patients with AIN3 were followed up for a median of 63 months, three patients who were immunosuppressed developed invasive anal carcinoma. 16 In a French study that followed 228 patients with anal condylomata, 38 (19%) showed high-grade AIN disease. Of those who had high-grade AIN, seven cases developed invasive anal carcinoma after a follow-up ranging from 13 to 108 months. 13 Thus, there seems to be an opportunity for us to prevent the development of anal cancer by treating or preventing the development of high-grade AIN. In a study looking at inter-observer agreement in the histological interpretation of anal intraepithelial neoplasia, the weighted kappa value for overall agreement was 0.59 (95% CI: 0.55–0.63). 17 It is therefore feasible that some high-grade disease may be downgraded as low-grade disease through sampling or through histological interpretation. We chose to treat all grades of disease as each patient wished. Laser treatment was generally acceptable, with the duration of moderate pain typically lasting 48 hours when patients took dihydrocodeine tartrate or diclofenac sodium. Patients who have had treatment for three- or four-quadrant disease also experienced pain after that period, when opening their bowels. Most patients prepared themselves with local anaesthetic cream and mild analgesia, thus minimizing the pain. Typically, the pain lasted between seven and 14 days, with patients resuming activities after the first 48 hours. The mode of application of 5% imiquimod therapy has been presented elsewhere. 18 Except two patients (2/61) who developed systemic side-effects and stopped their treatment, all tolerated treatment well. They titrated their applications to either twice or three times weekly based on local side-effects such as soreness or a burning sensation. Treatment typically lasted 12 weeks with some continuing to 16 weeks. The effectiveness of 5% imiquimod was recently demonstrated by a double-blind, placebo-controlled trial, where seven of 28 cases either became disease-free or downgraded their disease from high-grade AIN (AIN2/3) using 5% imiquimod compared with one of 25 cases on placebo (P = 0.038). 19
There is substantial evidence supporting the view that detection and treatment of high-grade cervical intraepithelial neoplasia reduces the incidence of cervical carcinoma. In the UK, about 1.5% of all women now younger than 50 years would have died of cervical cancer before age 85 if they had never been screened, and 3% would have developed disease. 20 The reduction in cervical cancer incidence and deaths has been made possible by the introduction of a national screening programme and by colposcopic examination and treatment of high-grade cervical intraepithelial neoplasia in those showing abnormal cervical cytology. There are several similarities between cervical squamous carcinoma and anal squamous carcinoma. 21 Treatment of high-grade AIN therefore may intercept the development of anal squamous carcinoma. A number of proponents have suggested the introduction of screening with anal cytology for those at high risk for anal cancer such as HIV-positive MSM. 22
Chang et al. 23 found surgical excision under general anaesthesia a successful mode of treatment for large volume high-grade disease in HIV-negative subjects compared with HIV-positive subjects (P = 0.03). However, their treated population consisted of eight HIV-negative and 29 HIV-positive subjects with a mean follow-up period of 32.3 ± 20.6 months and 28.6 ± 12.9 months, respectively. In a study by Goldstone et al. 14 24 out of 68 patients (35%) remained free of disease after treatment using infrared coagulation for high-grade AIN when followed up for a median of 413 days (range = 162–1313 days). Our study shows the largest cohort with a long follow-up period that underwent treatment for AIN. It also includes both low- and high-grade disease and HIV-positive and HIV-negative individuals in the same cohort. Further, we used an outpatient-based treatment procedure and employed laser ablation and, to a lesser extent, 5% imiquimod topical therapy and excision. All hospital-based treatment was carried out with HRA guidance. However, this is observational data, and the treatment selection has been influenced by many confounding factors such as size of the lesion, patient preference, previous treatment, etc. Further, preferably randomized, studies are needed to compare treatment types to verify the best approach to treatment.
Our data taken together with previous treatment data by Chang et al. and Goldstone et al. point to the possibility of successful treatment for both low- and high-grade AIN. The treatment success in our HIV-positive people might have been influenced by their relatively high CD4 counts at the start of the treatment. It is probable that antiretroviral therapy may also have an influence but was difficult to measure in this cohort. These findings should help with the general push to introduce screening for AIN in at-risk groups. A modelling study by Goldie et al. 24 demonstrated the clinical and cost effectiveness of screening for squamous AIN lesions with anal cytology. Anal cytology may need further evaluation before its use as a tool to assess cure. A recent study using minichromosome maintenance proteins detection as a means of identifying cervical neoplasia showed a higher sensitivity and 0% false-positivity when compared with the conventional cervical smear test. 25 Future studies are needed defining cure for AIN using a number of modalities such as HRA findings, anal cytology and immunocytochemistry.