
Abstract
Home delivery (HD) of medication is a goal of the Department of Health's Pharmacy in the Future; Implementing the NHS Plan. We evaluated the safety and effectiveness of an HD service for antiretroviral therapy (ART). Patients on ART with stable viral load (VL) <50 were identified. Comparison was made between patients using HD and those using the clinic-based pharmacy (CP). The primary endpoint was HIV virological failure (VF) (HIV VL >400 copies/mL on two consecutive occasions). Secondary endpoints included frequency of outpatient attendances (OPA) and an incidence of adverse events. Cumulative incidences (Culmln) for each outcome event were calculated. Incidence-rate ratios (IRR) were obtained using Poisson regression. Of 1663 patients identified; 450 received HD and 1213 used CP. Culmln of VF was =4% in those using HD and =7% in those using CP (IRR [95% confidence intervals, CI] =0.53, 0.32-0.90). HD patients had fewer OPA, less frequent blood test monitoring and less frequent abnormal liver function results (IRR [95% Cl]= 0.63 [0.59-0.67] and 0.59 [0.53-0.67], 0.68 [0.65-0.71] and 0.64 [0.53-0.78], respectively). Patients deemed stable enough on social, psychological and medical grounds to receive HD of ART had a lower risk of VF, fewer OPA and no increase in adverse events when compared with patients using CP.
Introduction
In 2000, the Department of Health published Pharmacy in the Future: Implementing the NHS Plan. In this document, home delivery (HD) of medication is cited as one of the goals. 1 Furthermore, provision of convenient access to prescription and other medicines is one of the chief pharmaceutical officer's 10 key roles for pharmacy services in the UK. 2 In 2005, the London Specialized Consortium Group for HIV implemented a London-wide framework agreement for HIV treatment centres to develop HD of HIV medication. 3 Implementation of HD schemes in other specialties such as haemophilia has already been shown to result in significant financial savings for the National Health Service (NHS). The Pan-Thames Haemophilia Consortium reported a saving of £3.2 million in 2005-2006 in an area which covers 76 primary care trusts (PCTs) and where annual expenditure for that period was £86 million. 3
Current NHS financial constraints have created incentives for HIV services to develop more cost-effective methods of delivering patient care. 4 A commercial service also reduces drug expenditure, as value added tax is not added to the cost of home-delivered medication. Once service charges are taken into consideration the outcome is an approximate 12% saving on drug costs.
There is little published data describing the experiences of HD of medication in other chronic diseases5–9, with no published data in patients with HIV infection. HIV is complicated by the need for sustained adherence to antiretroviral medication10–12 and multiple complex drug-drug interactions. 13 Clinical care may potentially be compromised in a home-delivered medication service as a result of reduced face-to-face consultation with medical and allied staff and opportunities for pharmacov-igilance. In February 2001, Camden PCT HIV service developed and piloted an HD of medications service. It subsequently undertook large-scale recruitment to this service after October 2004. This study aimed to investigate treatment and clinical-care outcomes in patients using the HD service for antiretroviral therapy (ART) and to compare these outcomes in patients utilizing the existing clinic-based pharmacy.
Methods
Camden PCT is one of two large providers of care for HIV-infected patients in North Central London. This NHS Trust provides outpatient care for patients with HV infection at two sites: The Mortimer Market Centre and Archway Sexual Health Clinic, which are geographically 2.5 miles apart. Approximately 2600 patients access their care from this service.
Patients attending our HIV service were offered HD of medication if they were ‘stable’ on ART (defined as a sustained virological response (viral load [VL] < 50 copies/mL) over a six months period), In addition, some patients were offered HD if this criteria was narrowly missed, such as VL <100. From the clinic and pharmacy databases, we identified all patients who were ‘stable’ on ART between October 2004 and January 2007. We performed a retrospective database search and case-note review of patients who received HD of antiretroviral medication and compared them with patients eligible for HD of medication using the strict criterion above, but who received standard care, i.e. clinic pharmacy dispensed medication. We recorded the date at which patients began using the HD service.
From case-note review, data were collected on demography, HIV VL, CD4 count, haemoglobin, serum creatinine and alanine aminotransferase (ALT) enzyme levels for patients receiving HD and conventional pharmacy services. Of patients who discontinued using the HD service, an assessment was made from individual patient's notes to ascertain the reason for this.
The primary outcome of the study was incidence of virological failure (VF), defined as an HIV VL >400 copies/mL on consecutive measurements. Secondary outcomes included the frequency of clinic attendance and rates of adverse events, including renal impairment (serum creatinine >100 |xmol/L), anaemia (haemoglobin <12 g/dL; men and <11 g/dL; women) and abnormal liver function (ALT >50 IU/L).
‘Baseline’ analysis was based on the time of first eligibility for HD (i.e. sustained VL measurements of <50 copies/mL recorded after October 2004). However, for those who commenced HD before meeting this criterion the baseline is defined as the start of HD. The chi-squared test was used to compare the study groups at baseline for categorical factors, the Mann-Whitney test for clinical measurements and the t-test for age.
The start of follow-up for analysis was considered to be the date of starting HD for the HD group and the date of first eligibility for HD for the comparison group. Analysis was performed on an ‘intention to treat’ basis, in that for the HD group all follow-up events are included after starting HD, irrespective of whether HD subsequently ceased. For the primary outcome, analysis was repeated excluding events experienced during a treatment interruption. Cumulative incidences (CulmIn) for outcome events such as VF were calculated. Median (interquartile range [IQR]) number of episodes were presented for outcomes such as attendances with potentially multiple occurrences in follow-up. Incidence-rate ratios (IRR) were calculated using Poisson regression to account for varying periods of follow-up. Follow-up data were collected until study close on 19 January 2007. All analyses were performed in Stata 9.
Results
A total of 1663 patients were included in the study. This included 450 patients in the HD group and 1213 patients in the comparison group. Of the HD group, 104 (23%) initiated HD before meeting the strict eligibility criterion of stable VL <50. In the HD group median (IQR) months of potential follow-up until study close was 17 (12-23) months, and was 24 (16-26) months in the comparison group. There was no significant difference in the demographic or baseline characteristics between the HD and comparison groups (Table 1).
Baseline demographics among patients receiving home delivery (HD) of antiretroviral therapy and those eligible, but who received medication from the clinic pharmacy
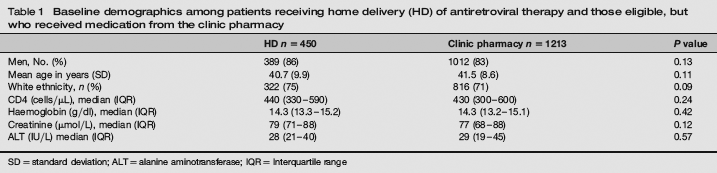
SD = standard deviation; ALT = alanine aminotransferase; IQR = Interquartile range
Primary outcome
The CulmIn of VF was lower for patients using HD (4% vs. 7% [IRR = 0.43, 95% confidence intervals, CI = 0.24, 0.78]) (Table 2).
Primary and secondary outcomes in patients receiving home delivery (HD) and in those collecting medication from the clinic pharmacy
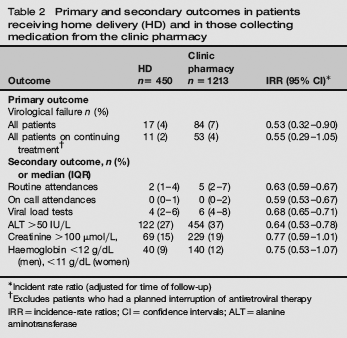
Incident rate ratio (adjusted for time of follow-up)
Excludes patients who had a planned interruption of antiretroviral therapy
IRR = incidence-rate ratios; CI = confidence intervals; ALT = alanine aminotransferase
Following exclusion of failure events associated with a treatment interruption, the CulmIn of VF remained lower in the HD group (2% vs. 4% [IRR = 0.55, 95% CI = 0.29, 1.05]) but the reduction was no longer significant.
Secondary outcomes
Patients in the HD group had significantly fewer clinic attendances for routine and emergency outpatient appointments and routine blood monitoring (IRR = 0.63, 0.59 and 0.68, respectively). There was some evidence of reduced incidence of anaemia and renal impairment in the HD group (IRR [95% CI]) =0.75 [0.53-1.07] and = 0.76 [0.53-1.07], respectively). There was a significantly lower incidence of abnormal liver function in the HD group, IRR (95% CI) = 0.64 (0.53-0.78).
Patients discontinuing use of the HD service
Seventy-eight (17%) of 450 patients stopped using the HD service (Table 3). The most common reason for discontinuation was patients preferring to return to the traditional method of collecting medication (28/78, 36%). Other reasons included moving out of the area (15%), change of HIV treatment regimen (13%), HIV VF (9%) and planned interruption of ART (8%).
Reasons for patients discontinuing the home delivery (HD) service

Discussion
In this study, we have shown that patients attending an inner London HIV treatment centre, who were receiving a system of HD of antiretroviral medication, had a lower risk of VF when compared with patients receiving standard clinic pharmacy dispensing of medication. This patient group also attended less frequently for both routine and emergency appointments, and for blood test monitoring. The only significant difference in laboratory adverse events was a lower risk of abnormal liver function in those using the HD service. These results suggest that patients receiving HD of antiretroviral medication had neither an inferior treatment response nor laboratory outcomes when compared with those who received their medications via the clinic pharmacy. Furthermore, the HD service was well accepted, with few patients stopping the service by choice.
This study has some limitations. First, patients were not randomized and thus, there may be confounders which might explain the outcome. There is potential for selection bias as not all patients starting HD met the criterion of two consecutive VLs <50 copies/mL required for the comparison group, and those starting HD will have been selected as being suitable for the service by their physician. Those receiving HD may also have had baseline prognostic factors favouring better ART outcomes, such as longer duration of virological response, better adherence records and less co-morbidity. However, these data are encouraging in terms of safety, and support the use of HD in selected patients stable on antiretroviral medication.
A further limitation of the study is that the outcomes were primarily focused on laboratory markers and on clinic attendance. We did not examine the impact of HD on other aspects of care such as psychological support, sexual and reproductive health, sexually transmitted infection screening and treatment and HIV-prevention advice. Additionally, we cannot exclude a small negative impact on outcome among those who received HD of antiretroviral medication.
This study is the first to describe the clinical impact of introducing HD of antiretroviral medication to patients with HIV infection. The study findings support further expansion of this potentially cost-effective and patient-friendly service. There is potential for significant financial savings without fear of compromise to patient's standard of care. Furthermore, the HD service adds to patient choice and eliminates time spent by patients waiting in the clinic pharmacy.
In conclusion, HD of ART to patients attending an inner London HIV treatment centre appears to be safe, to reduce per-patient treatment costs, is popular with patients and meets Department of Health guidelines.